
Article Figures & Data
Figures
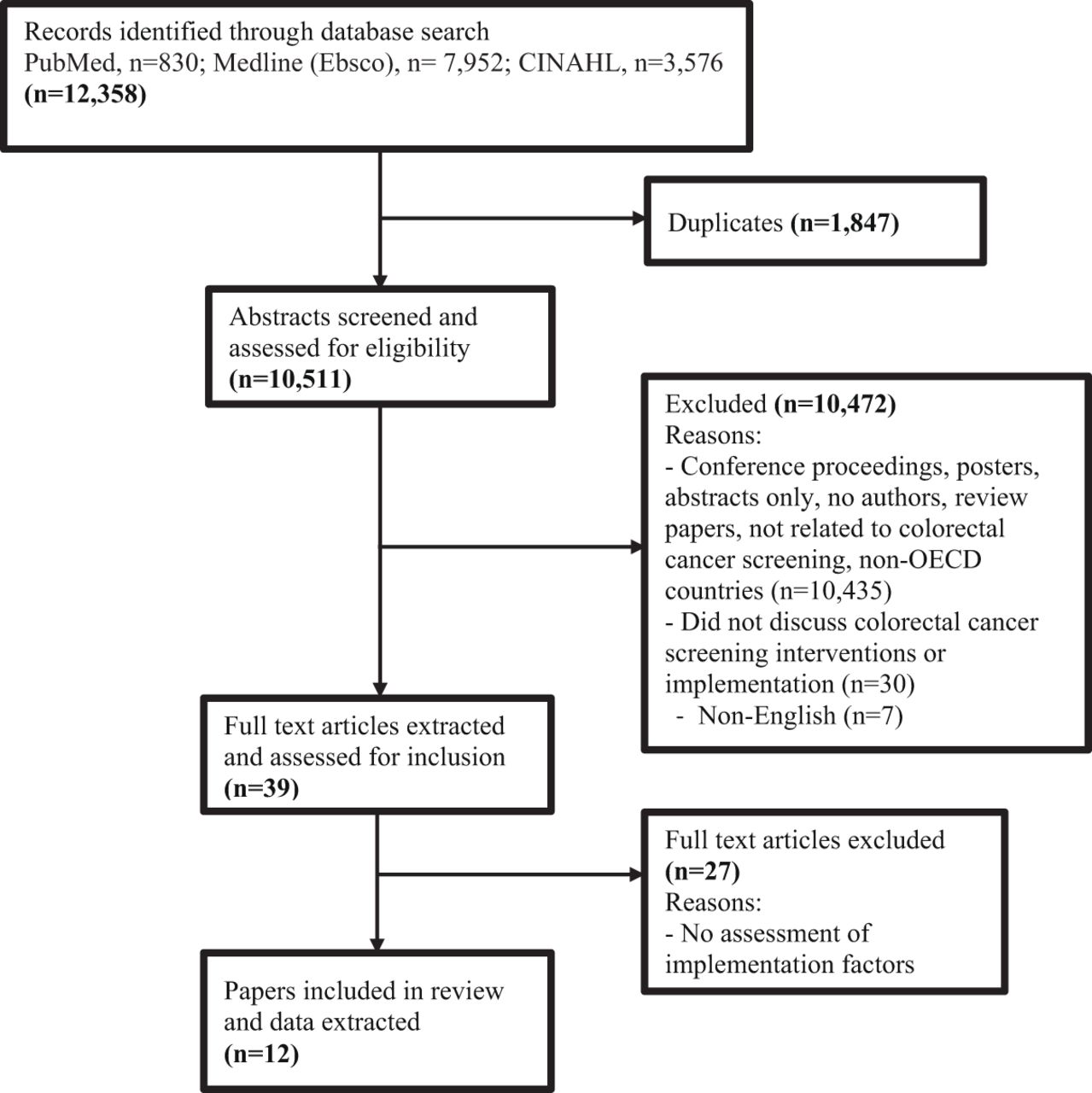
- Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram. Abbreviation: OECD, Organization for Economic Co-Operation and Development.

Tables
Author Objective Type of EBIs or intervention program to improve CRCS Study Setting Key Study Methods Green et al. 2017 USA To assess the change in CRCS rate and intervention implementation facilitators and challenges Mailed intervention, including mailing of FIT kit, patient education, and patient follow up.
- First mailing: pamphlet on CRCS choices, and statements saying they are due for CRCS, and will soon receive a FIT kit.
- Second mailing: FIT kit, pictographic instructions and a letter emphasizing the importance of completing screening.
- Third mailing: Reminder letter if the FIT kit is not received and processed by the lab within 3 weeks.Clinics - No mention of methods- data collection tools/techniques, samples in relation to barriers and facilitators assessment.
- Used CFIR to report the implementation factors.
- During implementationHannon et al. 2019 USA To evaluation whether grantees implemented andmaintained EBIs over the funding cycle (measured with quantitative survey items) and barriers and facilitators to implementing andmaintaining EBIs (measured with open-text survey responses) Implement one or more of these 5 interventions/EBI:
- Provider-centered: provider reminder, provider assessment and feedback
- patient-centered: small media (posters, postcards, brochures), client reminder
- Addressing structural barriers (to address the financial barriers of low income and unscreened people).CRCS program's grantee organizations (state department of health or tribal organization) - Qualitative (online open text survey responses)
- During implementationCole et al. 2015 USA To identify facilitators of and barriers to implementation of a proactive, mail-based colorectal cancer screening program in Federally Qualified Health Centers setting that draws on the published evidence from the evaluation of the SOS program - Patient education: mailing of patient information regarding CRCS
- Mailed return kit and patient reminder: mailing of FOBT kits with stamps and remindersFederally Qualified Health Centers comprising primary care clinics to provide primary care to low-income and uninsured patients - Qualitative (Semi structured interviews guide developed based on CFIR)
- During implementationBakhai et al. 2018 USA To increase CRCS and identify the materials/methods, physician and patient-related barriers to the acceptance of FIT and colonoscopy 1. Physician and staff reminder
2. In-clinic distribution of FIT
3. Patient education
4. FIT instruction
5. Patient reminderClinics - Root cause discussion and analysis (using a fishbone diagram)
- During implementationBaldwin et al. 2020 USA To explore implementation challenges and successes specific to two health insurance plans that serve enrollees in U.S. Medicaid and Medicare programs in implementing their mailed FIT programs in the first year - Sent introductory letters and FITs via mail
- Patient reminder (mailed postcard or live phone call)Clinics - Qualitative (telephone interviews using in-depth interview guide based on CFIR)
- After implementationCoronado, et al. 2017 USA To report on implementation challenges faced by eight community health centers that participated in STOP CRC, a large comparative effectiveness cluster-randomized trial to evaluate a direct- mail program to increase the rate of CRCS Mailed the introductory letter, the FIT kit, and the reminder postcard/letters. Clinics - Qualitative (telephone interviews using in-depth interview guide based on CFIR)
- Before implementation or baseline and post implementationCalanzani, et al. 2017, Scotland To test the feasibility and acceptability of an opportunistic intervention in general practice patient consultations, examining whether a brief conversation was a viable way to engage with non-responders and increase bowel screening participation Patient education: brief conversation between patient (non-responders) and providers about bowel screening. An opportunity to request a bowel screening kit, information leaflet, Freepost envelope were offered. Clinics - Qualitative (closed and open-ended questionnaire and semi-structured interviews
- After implementationDavis et al. 2019 USA To explore how Accountable Care Organizations work with clinics (the key facilitators that enhanced the organization and clinics collaboration) while implementing multicomponent interventions to improve CRCS. - Patient reminders
- Patient education
- Reducing structural barriers
- Provider assessment and feedback
- Patient and provider incentives
- Provider reminder and recallAccountable Care Organizational team - Qualitative (key informant interviews using semi-structured interview guide)
- During implementationCole et al. 2015 USA - To describe self-reported EHR system capabilities necessary for completing/delivering the CRC screening tasks and measuring colorectal cancer screening rates.
- To describe the ease in using EHR systems and the perceived accuracy of EHR data for measuring CRCS.CRCS reminders and provider reports Clinics (50 community health center clinics) - Quantitative (survey on EMR related barriers that can influence implementation)
- Before implementationWalsh et al. 2011 USA To assess the extent to which components of the FLU-FOBT intervention program were adopted, implemented and maintained 1 year after completion of the RCT. - Offering FOBT along with influenza vaccines
- Patient education materials
- Provided stamped mailing envelopes allowing patients to send completed sample to the labClinics - Qualitative (interview with clinic leaders using interview guide structured around the RE-AIM framework, after implementation Weiner et al. 2017 USA To describe facilitators of and barriers to implementing office systems in FQHCs (federally qualified health centers) clinics by using the practice facilitation and tool kit approach - Implantation of policies and practices or procedures for CRCS including reminder systems to cue providers and patients to take actions for CRCS. Clinics - Qualitative (semi-structured interviews)
- After implementationLeeman et al. 2019 USA To understand the process that Federally Qualified Health Center (FQHC) staff use to select and implement CRC screening interventions, and the factors influencing the intervention implementation Patient level: education (one-on-one education, small media, group education) and patient remindersProvider level: provider assessment and feedbackOrganizational level: Patient navigators, reminder and recall systems Other interventions: FluFIT and mailed FIT Clinics - Qualitative (interviews using a semi-structured interview guide across CFIR framework domains).
- During ImplementationAbbreviations: CRC, colorectal cancer; CRCS, colorectal cancer screening; FIT, fecal immunochemical test; CFIR, consolidated framework for implementation research; RE-AIM, reach, effectiveness, adoption, implementation, maintenance; EBI, evidence-based intervention; EHR, electronic health records; FBOT, Fecal Occult Blood Test; RCT, Randomized Controlled Trial; STOP CRC, Screening TO Prevent ColoRectal Cancer.
Qualitative studies (using the Critical Appraisal Skills Program checklist): Study Clear Statement of aims of the research Qualitative Methods Appropriate Research Design Appropriate Recruitment Strategy Appropriate Data Collection Addressed Research Issue Relationship Adequately Considered Ethical Issues Considered Data Analysis Rigorous Clear Statement of findings Results Help Locally Baldwin 2020 Yes Yes Yes Can't tell Yes Can't tell Can't tell Yes Yes Yes Calazani 2017 Yes Yes Yes Can't tell Yes No Yes Yes Yes Yes Cole 2015 Yes Yes Yes Yes Yes No Can't tell Yes Yes Yes Coronado 2017 Yes Yes Yes Yes Yes No Yes Yes Yes Yes Davis 2019 Yes Yes Yes Can't tell Yes No Can't tell Yes Yes Yes Hannon 2019 Yes Yes Yes Can't tell Yes No Can't tell Yes Yes Yes Leeman 2019 Yes Yes Yes Yes Yes No Yes Yes Yes Yes Walsh 2012 Yes Yes Yes Yes Yes No Can't tell Can't tell Yes Yes Weiner 2017 Yes Yes Yes Yes Yes No Can't tell Yes Yes Yes Quality improvement studies (using the Quality Improvement Minimum Criteria Set): Study Organizational Motivation Intervention Rationale Intervention Description Organizational Characteristics Implementation Study Design Comparator Data Source Timing Adherence/Fidelity Bhakhai 2018 Met Met Met Met Met Met Met Met Met Met Green 2019 Met Met Met Met Met Met Met Met Met Met Study Health Outcomes Organizational Readiness Penetration/Reach Sustainability Spread Limitation Bhakhai 2018 Met Met Met Met Met Met Green 2019 Met Met Met Met Met Met - Table 3.
Facilitators and Barriers of Implementation of Interventions to Improve Colorectal Cancer Screening (CRCS) Reported by Included Studies, Organized in Consolidated Framework for Implementation Research (CFIR) Domains
CFIR Domains Study Reference Facilitators Barriers 1. Intervention characteristics Evidence - - Not identified - Not identified Relative advantage Baldwin 2020, Leeman 2019, Cole 2015 - The new program/intervention is beneficial or impactful: helps to increase CRC screening and patient engagements and provides a roadmap for improving CRC screening program. - Not identified Adaptability Green, 2017, Calanzani 2017, Baldwin 2020 - Flexibility that clinics could make choices about some components of interventions while maintaining fidelity. - Not identified Simplicity vs complexity Green 2017 - Uncomplicated intervention; intervention could be put in place quickly. - Not identified Trialability Cole 2015 - Program can easily be implemented/tested on a small scale first before the widespread implementation. - Intervention significantly different than previous experience in the setting. Design quality and packaging Green 2017, Baldwin 2020 - Use of already existing CRCS-related materials and infrastructure for intervention (e.g., FIT kits, pre-stamped envelope, bulk ordering, lab).
- Materials were tested, packaged, and made them available to the general public and clinical team.
- Activities were able to be fit within clinicians' and staff's workflow (or work routines).- Amount of time required and complexity of setting up mailed FIT program e.g., determining accurate eligibility lists and establishing workflows and vendor expectations). Cost Green 2017 - Prior research evidence on low cost for intervention (mailing FITkit). - Not identified 2. Inner setting (clinic setting where the interventions were implemented) Networking and communication Cole 2015, Bakhai 2018, Leeman 2019, Baldwin 2020, Weiner 2017, Green 2017 - Leveraging existing meeting structure/communication strategies to introduce new programs. Staff meetings, where all staff members (practice manager and lead nurse) are involved to provide everyone with updated clinic information, policies, procedures, and also to gain insight on any suggestions or concerns.
- Communication by QI Committee about CRC screening improvement to staff via staff meetings, e-mail, newsletters and team huddles.- Communication challenges across organizations and within teams about mailed FIT program. Poor communication across disciplines. Organizational and professional teams have separate administrative and communication structures. - Communication of information about CRCS (status, improvement, efforts, process and plan) to providers and non-provider staff in separate meetings, limiting opportunities for interdisciplinary exchange. Culture Cole 2015, Green 2017 - Valuing prevention and population health.
- Individuals' and organizational commitment to improve CRCS rate.
- Viewing intervention as part of a broader preventive health agenda.
- Vision to care for the underserved population.
- Creation of quality improvement officer position that reports directly to CEO, which reflects importance of quality improvement works within the organization.
- A shared mission of organizational and professional team of providing health care.- Adoption and implementation of new interventions/programs at the discretion of administrative leadership without consultation of clinical or other staff about improvement priorities. Implementation climate Green 2017, Cole 2015 (quantitative study) - Clinics' autonomy to trying new things.
- Clinics' self-introduced adaptations.
- Organizational encouragement for healthcare innovations.
- Involvement of researchers with an experience of implementing the program.- Not utilizing data feedback and strategies to improve and sustain intervention/project.
- Staff not being able to generate specific information related CRCS using EMR functionality.
- Staff not being able to send reminder to patients (using EMR functionality) due for CRCS.Implementation climate: Tension for change Hannon 2019, Cole 2015 - Leadership with a strong motivation to improve CRCS. - Conflicting opinions of clinical staff on approaches to improving CRCS. Implementation climate: Compatibility Baldwin 2020, Davis 2019, Cole 2015 - Project's match with organization's mission and goal.
- Alignment of intervention with other similar initiatives/practices previously or currently experienced in the setting (cervical screening, alcohol brief intervention).
- Pieces of the intervention that fit within the current workflow.
- New roles and workflows consistent with leadership vision for organization.
- Organizational experience testing new program on a small scale before widespread implementation.- Needed to create a new role (care manager) for intervention implementation, leading to increased cost.
- Incompatible intervention or not the best approach (specifically direct mail approach) for special patient population (homeless, low literacy): incongruous with how organization likes to work (face to face conversations and directly handing kits to patients); too impersonal and thus inferior to face-face encounters.Implementation climate: Relative priority Leeman 2019, Cole 2015, Weiner 2017, Hannon 2019 - Provider's premature death due to CRC increased the importance of project.
- Leadership voiced strong support for CRCS as a priority and approach as a good fit for “where the organization is going”.
- Project housed within group that measures how clinic/providers are doing on quality metrics, including CRCS.
- Project/intervention selection based on what are going to be requirements in terms of resources, and then the overall value to patients from it.
- Organizations setting priorities that CRCS is in need of improvement and putting efforts to improve CRCS comparing to other areas.- Competing priorities for both providers and patients, that led to the limited frequency with which providers recommended screening and patients adhered to the recommendation.
- Change fatigue.
- Staff put preventive health issues lower on the priority list and sometimes forego offering them.Implementation climate: Organizational incentives Cole 2015 - New system for providing performance reports to clinical teams, which could create incentives.
- Implementation support to providers to implement the project (by providing implementation facilitator).- No financial incentives are tied to performance of providers or clinical teams. Implementation climate: Goal and feedback Cole 2015, Walsh 2012, Leeman 2019, Cole 2015 - Agenda set for each patient before his/her visit where they (Medical Assistants) check a lot of preventive activities and see whether or not they are up to date for CRC screening in the year.
- Monitoring of CRCS status every month and knowing the difference made or not made. Setting goal for few key indicators per years and providing monthly or quarterly performance feedback (clinic or provider specific).
- Creation of performance reports.
- The goal, key indicators, and current status/improvement presented via a graph, report, or scorecard, often during regularly scheduled meetings.- No systematic way for sharing performance reports on quality measures (e.g., screening rate). Implementation climate: Learning climate Cole 2015, Bakhai 2018, Walsh 2012 - Teaching environment to support learning new skills and implementation of new practices.
- Staff training regarding the project.
- Availability of technical support regarding the use of EMR for project implementation and evaluation.- Fast-paced clinic environment and financial pressures leading to most organizational resources devoted directly to clinical care.
- Not much time or structure for clinical staff to participate in skill development.
- Lack of peer mentoring or networking and support.Readiness for implementation Green 2017, Cole 2015 (quantitative study), Weiner 2017, Leeman 2019, Calanzani 2017, Hannon 2019, Cole 2015 - Robust data systems: EMR capturing accurate data related to CRCS history (identification of eligible patients, due or overdue for CRCS, high and average risks). Sharing EMR reports of eligible patients to attending providers. Building FIT workflow in EMR to document discussion with patients about FIT and to improve efficiency.
- Written protocol regarding the implementation plans/processes.- EMR: lack of EMR database; lack of EMR reminders/tools for physicians; lack of trackable documentation in EMR; lack of interpretable EMRs; lack of accurate EMR data for clinic patient member information; and time-consuming for modifying or establishing the EMR systems or functionalities/capabilities for changes.
- Lack of CRCS recommendation records in EMR.
- Recent rapid growth in organization and change in leadership structure.
- Large health centers with numerous clinic sites and providers.Readiness for implementation: leaders' and managers' engagement and commitment to implement) Baldwin 2020, Leeman 2019, Cole 2015, Green 2017, Hannon 2019, Bakhai 2018, Davis 2019, Hannon 2019, Walsh 2012 - Program sponsored by clinical operation chief and supervised by clinic operation manager.
- Project approval by grant funder.
- Clinic leaders worked hard to find ways to finance the FOBT kit mailing and returning process.
- Participation of leadership in pre-implementation interviews-demonstrating enthusiasm and willingness to involve and support.
- Engaged provider groups and their teams/staff: they were informed of program and knew what is happening regarding the program.
- Programmers work together in both delivery system and research.
- Previous QI experience and involved in projects related to FIT screening.
- Involving key staff and providers.
- Staff education and motivation regarding intervention/project.- Lack of involvement of high-level leadership such as CEO.
- Lack of leadership and organization's financially accountability for intervention success.
- High leadership/staff turnover or restructuring.
- Limited coordination between participating clinic sites.
- Undefined process for resourcing issues as they arise.
- Differing roles and involvement- GPs less engaged than the nurses.Readiness for implementation: Available resources (level of resources dedicated for implementation) Green 2017, Hannon 2019, Cole 2015, Calanzani 2017, Cole 2015 (quantitative study), Leeman 2019, Weiner 2017, Bakhai 2018, Baldwin 2020, Coronado 2017, Walsh 2012 - Dedicated staffing in place to do the project.
- Assigned responsibility of medical assistants and front desk staff for maintaining the CRCS tracking log and patient reminders/follow-up.
- Well-trained staff. Use of existing health information technology system.
- New staff (e.g., patient navigators), change to their EMR systems, and educational material for providers, staff and patients.
- Project funding to support clinic engagement and intervention implementation.- Limited staff time.
- Staff turnover- which caused clinics to redistribute staff rolesand train new staff in the clinic's office systems, and staffreluctance on the part of local gastroenterology practicesto perform free or low-cost diagnostic colonoscopies foruninsured or underinsured patients. Lack of staffing forpatient follow-up calls.
- Lower performance of staff due to staff turnover orlongstanding operation issues.
- Inadequate EMR staffingresources/technology support.
- Limited time of GP.-Limited time for new innovation in an already pressuredenvironment. No dedicated time to do FIT related tasks.
- Limited organizational resources for the scalability and sustainability of the program at the practice.
- Lack of clinical decision support tool for the physiciansto identify patients and order appropriate CRCS test.
- Unavailability of FIT test/kit in the clinics.Readiness for implementation: Access to information and knowledge (knowledge about intervention implementation) Walsh 2012, Coronado 2017, Leeman 2019, Cole 2015, Weiner 2017 - Participation of multiple clinical staff in pre-implementation interviews and interactions to understand the components of program and prepare for implementation.
- Creation of algorithm for CRCS and clinical workflow and making it available to clinical team.
- Clinic staff' access to wordless or pictorial information and instructions on CRC screening and beyond, developed by researchers.
- Clinic staff' learnings on how to assess CRCS eligibility, provide FOBT independently, and use patient education materials introduced by the study.
- Providing appropriate instructions for program in community clinics for test completion and return of kits to the laboratory using the new mailing envelope that was introduced by the study.
- Availability and use of EMR reports for sending information (reminders) to clients and for providers.
- Access to knowledge and information about interventions in an easy-to-understand format through patient information sheets, team huddles, and trainings.- Not fully trained staff in place or not trained in new work.
- Patient counseling script was too long.
- Patient decision aids were too time-consuming.
- Paper-based integrated summary was less useful as important information were lacking and inaccurate (such as patients due for CRCS and patients accessed interventions).
- Lack of knowledge and skill of staff and training/support on EMR system.
- Concerns about funding sustainability.3. Outer setting Patient needs and resources: Extent to which patient needs are accurately known and prioritized by organization Baldwin 2020, Leeman 2019, Calanzani 2017, Coronado 2017, Cole 2015 - Established “health access” program, which provides no cost or low-cost care to uninsured patients.
- Engaged patients and getting feedback on processes and promotion of screening options.
- Creation of awareness about CRCS to patients and family.
- Positive reactions from patients and expression of appreciation.
- Patients' receptivity of CRCS: patients called in to share they had their FIT or colonoscopy completed and appreciation of screening opportunities and support provided.- No organized program for providing specialty and/orhospital care to uninsured patients outside of the organization.
- Patients' knowledge gaps, fear of adverse effects, and concernsrelated to transportation/time away from work.
- Patient unable to understand FIT kit instructions.
- Difficulty in interacting on the topic of bowel screening with certain groups (e.g., males and minority ethnic groups).
- Some patient populations do not want to talk about poo or keeping the poo in kit.
- Low patient awareness about CRC and patients' confusion with a mailed program.
- Patients' lack of insurance coverage to pay for follow-updiagnostic testing.
- Patients' communication barriers such and not speakingEnglish, low health literacy, or difficulty hearing automatedcalls.
- Limited access to transportation, negative attitudestowards stool testing and low priority given to screeningrelative to other medical needs.Cosmopolitanism: degree to which organization is networked with other external organizations Cole 2015, Davis 2019, Leeman 2019 - Organization participated in Regional Patient Centered Medical Home initiative.
- Organizational alignment with other organizational initiatives on CRC screening and prevention.
- Organization is engaged in various types of networks and participated in network-related meetings and activities-noted value of networking is opportunity for staff and providers to lean about what was working well for others.External policy and incentives: External mandates, regulations and incentives Cole 2015, Hannon 2019, Coronado 2017 Externally funded research/project, where organizations are mandated to put greater emphasis on reporting and quality improvement. - Ending of funding.
- Shift in the partners' focus or priorities that led to thepartner no longer being interested in the program.
- No financial incentives to organization or staff for improving CRCS rates.
- Impact on colonoscopy access for higher number of positive FITs.
- Cumbersome process of EMR vendor to activate EMR toolscreating time delays for execution of work.
- Burdensome interface with outside labs processing FIT kitscreated delays/extra work.
- A lot of fatigue as wanting to do something different andshowing that everything is important.
- Influence of pay-for-performance incentives- staff andproviders being “overwhelmed” and experiencing “fatigue”related to all potential financial incentives.
- Grant funding often linked to specific, preselectedinterventions, which led unintended consequences such aslack of motivation and feeling of fatigue and overwhelmedin providers/staff.4. Characteristics of individual involved Knowledge and beliefs about the intervention: attitude toward and value placed on the intervention Hannon 2019, Green 2017, Cole 2015, Walsh 2012, Leeman 2019, Cole 2015 (quantitative study) - Clinical champions and investigator with interest in the project.
- Staff capacity to do the intervention related work.
- Leadership and clinical staff voiced understanding of how the intervention works and understanding of principles of which it is based.
- Providers value on preventive healthcare.
- The perceived professional role in educating patients and raising awareness.
- Motivation to adopt something new.
- Realization (of staff and providers) of importance of shifting from paper-based tracking to tracking in the EMR.
- Staff/providers valuing the importance of EMRs in intervention implementation and monitoring the quality and success of screening programs.
- Providers' interest and priorities for screening and interventions.
- The willingness of staff to see the importance of intervention/project, to say that this is relatively easy test for the clients to perform.
- Staff/providers knowledge on intervention/project and recognized its importance.- Some clinical staff (physicians and medical assistants) had incomplete knowledge about patient preferences in relation to CRC screening and effectiveness of different colorectal cancer screening tests.
- Providers' gap in knowledge about recommended CRCS guidelines.
- Providers desiring response rates for their patients/teams but information not available at the time of inquiry.
- Provider/health center resistance to FIT screening in some locations.
- Provider viewed project as adding pressurized work environment (project added greater workload as we are already struggling to provide our committed services).
- Providers believed that EMR-generated CRCS data are not accurate enough to guide the intervention implementation (somewhat accurate requiring verification or not at all accurate and could not be used for reporting).
- Reluctance of some clinic staff to adopt new roles and initial burden of participating in an RCT that required staff to shift up and back between intervention and control weeks during the RCT.
- Staff/providers' lack of confidence (i.e., self-efficacy) in their ability to translate their knowledge of CRCS and interventions into action.Other personal attributes Baldwin 2020, Leeman 2019 - Positive reactions from providers and health centers.
- Provider experienced minimum time and staff burden.
- Nurses spending more time on this project and doing more education with the patients.
- Ability to communicate with patients in a caring manner.- Desire to implement other EBIs and not being able to implement all EBIs at one time. 5. Implementation process Planning: Degree to which implementation is planned in advance Hannon 2019, Cole 2015, Green 2017 -Involving a multidisciplinary team and expertise in program planning and development.
- Minimal number of meetings.
- Detailed pre-implementation evaluation and implementation planning done by research team in collaboration with organizations.- Challenges in getting approvals or arranging contracts with partners agencies.
- Geographic distance between research team and organization making frequent in-person meeting difficult.
- More time-consuming to set up/start than anticipated.
- Some health centers/provider groups less interested as prefer to “do own thing” or had other CRCS strategies.
- Not assessing local factors that influence CRC screening rates and therefore, are not purposefully targeting the factors that influence screening rates in their settings or populations.
-Not assessing patient- and provider-level factors that contribute to low CRCS rates, leading to inappropriate intervention selection.
- No plan for the maintenance of the program/intervention implementation. As a result, improved screening participation outcome did not sustain.Engaging: Individuals from organization with responsibility for implementation or opinion leaders Baldwin 2020, Hannon 2019, Davis 2019, Weiner 2017, Cole 2015, Coronado 2017 - Leadership participation in pre-implementation evaluation and financial sustainment (of FIT kit mailing)
- Support and strong champion to lead program at leadership level.
- Engagement of providers, who lead CRCS program, clinical care, and education at the organization, as practice champions.
- Engaging IT staff to confirm the accuracy of EMR databases.
- Partnership approach that encourage health center participation by reducing staff burden and cost to implement CRCS on own (e.g., hiring implementation facilitator).
- Medical directors at health centers promoting FIT and idea of mailed FIT.
- Established workflows and strategies to address challenges as move into next year.
- Established relationships and building partnerships: history of prior relationship between key leadership and primary care stakeholders, physical proximity of the key leadership's infrastructure, and joint leadership roles of the key stakeholders and regional clinics.
- Involving organizational leaders and formally appointed implementation leaders to support planning and execution of CRCS intervention.
- Identifying and preparing implementation champions and leaders.- Multiple full-time responsibilities (teaching and clinical care) of practice champions.
- Lack of communication between key departments about mailed programs so less able to address patient questions.
- Lack of coordination between clinic staff and providers including “disconnect” between quality improvement coordinator and the clinicians who were directly responsible for recommending screening and distributing FOBT kits.
- Lack of clarity of clinic staff roles.Executing Davis 2019, Green 2017, Baldwin 2020, Weiner 2017, Walsh 2012, Davis 2019, Coronado 2017 -Timelines for activities in place.
- Materials/resources for activities in place, including established workflows for FIT kit mailing and returning process/returning of mailed kits, EMR.
- Assistance and use of a mailing vendor.
- Implementation coordination between team (recommending screening, ordering kit, offering kit, education, labs, scheduling colonoscopy).
- Appoint patient navigator or use nurse navigator or practice facilitator to support the implementation or improve existing practice, track FIT orders, FIT completion and urgent colonoscopy referrals (“glue of the program”).
- Encouraging health centers to scrub or clean/update screening eligibility lists.
- Providing information to providers on the FIT intervention program.
- Minimizing paperwork and integrating the intervention into existing information technology/EMR systems.
- Clinic-based staff support, learning collaboration, and change via facilitation.
- Use of tools including clinic self-assessment survey, the sample screening algorithm, the standing orders for CRCS, the tracking log, and the patient reminders.
- Flexibility in implementing process and tools.
- Start with small batch for testing and then the full-fledged mailed.- Complexity of working with vendors to get FIT kits ordered.
- Delay in obtaining kits from vendor, some kits are out of date.
- Delay in vendor mailing introductory letter and kits.
- Lack of sufficient oversight with vendor so difficult to know exactly how many reminder calls were being completed or if they are following script.
- Current lab vendor requires a two-sample test which may be barrier to FIT completion for patients.
- Returned FIT kits not always processed.
- Lack of workflow/process to ensure returned FIT kits were properly labeled before going to lab for processing.
- Delayed FIT kit mailing timeline, incorrect postage of kits.
- Wasted FIT samples because of no collection date labeled or mislabeling.
- CIinics are not being able to easily create a list of patient panels by providers and generate the eligible patient panel reports.
- CRCS history inconsistently documented in health records.
- Inability to accurately identify eligible patient for CRCS.Reflecting and evaluating Green 2017, Davis 2019, Calanzani 2017, Baldwin 2020, Leeman 2019 - Producing and sharing performance data: producing accurate, transparent and actionable reports (with results and interpretation); identifying area of improvement; report sharing to inform team including administrative leadership; use to prioritize actions, helping clinics to figuring out the solutions, and monitor improvement.
- Review of outcomes and implementation adjustments.
- Staff viewing more patients being returned the kit/screened than previously.
- Results intriguing enough to continue program.
- Requesting feedback from patients on their CRCS process.
- Monitoring and reviewing data and using data to improve CRC screening efforts.- Lack of timely or accessible data to show the worth of efforts.
- Assessment of kit return rate outcome hindered by delays and lag in claims data, hence, not being able to see the improvement.
- Staff fatigue due to metric focus associated tasks.
- Collecting data for the purpose of organizational reporting, but not for evaluation purpose or using data to improve CRCS intervention implementation processes and outcomes.
- Not using existing data sources available-asking new data collection, leading to fatigue and too busy.Bolded text signifies facilitators and barriers that are relatively more specific/targeted to CRCS intervention implementation whereas the nonbolded text are facilitators and barriers more general to implementation of change in primary care.
Table includes constructs for which relevant data existed in the reviewed literature; hence, other CFIR constructs such as innovation source and structural characteristics are not included in the table.
Abbreviations: CRC, colorectal cancer; CRCS, colorectal cancer screening; FIT, fecal immunochemical test; CFIR, consolidated framework for implementation research; EBI, evidence-based intervention; EMR, electronic medical records; QI, quality improvement; FBOT, Fecal Occult Blood Test.
- Table 4.
Summary of Commonly Discussed Facilitators and Barriers and the Number of Studies They Were Identified In
Facilitators of implementation [related CFIR domains (and constructs)] Number of studies Barriers of implementation [related CFIR domains (and constructs)] Number of studies Engagement of clinic team, leadership team and partners
[Implementation process (engaging) and internal setting (implementation readiness)]9 Limited time of clinic team to commit new project
[Internal setting (implementation readiness)]8 Priority or motivation to improve CRCS rates and recognizing benefits of new interventions
[Internal setting (culture and implementation climate) and characteristics of individuals involved (knowledge and beliefs about the intervention)]7 Challenges or unavailability of getting accurate and timely data to implement interventions and evaluate the progress or intervention
[Implementation process (reflection and evaluating)]6 Use of EMR system
[Internal setting (implementation readiness)]7 EMR-related challenges due to limited skills and supports and time-consuming
[Internal setting (implementation readiness)]5 Resources- staff's time, knowledge, skills, and training, availability of well-packaged materials in place
[Intervention characteristics (design quality and packaging), internal setting (implementation readiness), and implementation process (executing)]6 Communication challenges with clinics/organizations regarding FIT intervention program, disconnect between clinic team members, and lack of role clarity of clinic team
[Internal setting (networking and communication) and implementation process (engaging)]5 Continuous monitoring, feedback and reflection system of performance for improvement
[Implementation process (reflection and evaluating)]6 Patient-related barriers: includes cost, low health literacy, fear, not speaking English language, limited access (due to transportation), hesitancy of certain population to talk about or collect poo
[Outer setting (patients' needs and resources]5 Communication and coordination between clinic team
[Internal setting (networking and communication)]6 Process barriers due to lack of standard workflow, cumbersome workflow, or not following the process; delays from vendors
[Implementation process (planning and executing)]4 Clinics having autonomy to try new innovation and flexibility to adapt intervention/implementation process
[Intervention characteristics (adaptability), internal setting (implementation climate), and implementation process (executing)]5 Organizational structure changes, lack of leadership engagement, and leadership turnover
[Internal setting (implementation readiness)]4 Abbreviations: CRCS, colorectal cancer screening; CFIR, consolidated framework for implementation research; EMR, electronic medical records; FIT, Fecal Immunochemical Test.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Social Determinants of Health Influencing Colorectal Cancer Screening Behaviors Among Community Residents in China: A Scoping Review Protocol
- Evaluating the implementation of a multicomponent intervention to improve faecal immunochemical test-based (FIT) colorectal cancer screening in primary care
- Barriers and facilitators of implementing a multicomponent intervention to improve faecal immunochemical test (FIT) colorectal cancer screening in primary care clinics, Alberta
- Primary care provider interventions for addressing cancer screening participation with marginalised patients: a scoping review protocol
- Family Medicine Researchers Explore the Social Determinants of Health, COVID-19 Issues, and Cancer Survivor Care