
Abstract
Objective: We systematically reviewed and summarized previous studies that examined facilitators and barriers to implementing interventions to increase CRCS uptake in primary care practice.
Methods: We searched PubMed, Medline (EBSCO), and CINAHL databases, from the inception of these databases to April 2020. The search strategy combined a set of terms related to facilitators/barriers, intervention implementation, CRCS, and uptake/participation. A priori set inclusion and exclusion criteria were used during both title/abstract screening and full-text screening phases to identify the eligible studies. Quality of the included studies was appraised using quality assessment tools, and data were extracted using a predetermined data extraction tool. We classified facilitators and barriers according to the Consolidated Framework for Implementation Research domains and constructs and identified the common facilitators and barriers looking at how common they were across studies.
Results: A total of 12 studies were included in the review. Engagement of the clinic team, leadership team, and partners, clinics' motivation to improve CRCS rates, use of the EMR system, continuous monitoring and feedback system, and having a supportive environment for implementation were the most commonly reported implementation facilitators. Limited time for the clinic team to devote to a new project, challenges in getting accurate, timely data related to CRCS, limited capacity/support to use the EMR system, and disconnect between clinic team members were the most commonly reported implementation barriers.
Conclusions: The synthesized findings improve our understanding of facilitators of and barriers to the implementation of interventions to increase CRCS participation in primary care practice, and inform the customized implementation strategies. Many of the included studies had limited use of rigorous implementation science frameworks to guide their implementation and evaluation, which precludes a comprehensive understanding of the implementation factors specific to CRCS interventions in primary care. Future studies assessing the CRCS intervention implementation factors would benefit from the use of implementation science frameworks.
- Chronic Disease
- Community Medicine
- Faculty
- Family Medicine
- Health Promotion
- Infant Health
- Knowledge Translation
- Population Health
- Pregnancy
- Prenatal Care
- Primary Health Care
- Postpartum
- Social Determinants of Health
Background
Colorectal cancer (CRC) is the second most common cause of cancer death worldwide.1,2 CRC screening (CRCS) is highly effective at reducing the incidence and mortality of CRC.1,3⇓–5 Endoscopy-based (colonoscopy or sigmoidoscopy) and stool-based (Fecal Occult Blood Test (FOBT): Fecal Immunochemical Test (FIT) or Guaiac Fecal Occult Blood Test (gFOBT)) tests are the most commonly used effective screening modalities for CRC.1,6 CRCS program guideline recommendations such as age-group to screen and the choice of screening modalities vary by country.1 Nevertheless, high adherence to CRCS is essential for achieving the benefits, and yet screening rates remain suboptimal.
Strong evidence suggests that multicomponent interventions targeted at multiple levels (such as provider reminders, improved access, and patient education) can effectively increase the CRCS participation rate.7⇓⇓–10 However, the translation of interventions into routine primary care delivery, which often requires adaptation of existing care pathways and practices, can be difficult to achieve without a solid understanding of how to implement these interventions. Implementation can be influenced by a wide range of factors including those related to clinic context, intervention characteristics, providers' behavior, patient needs, and the implementation process.11 A comprehensive understanding of these factors can provide a foundation for planning strategies for implementation.11⇓–13
Several qualitative studies have reported on implementation factors pertinent to CRCS participation improvement interventions in primary care practice. However, to our understanding, there is no synthesis of these research findings; thus, a significant evidence gap exists in identifying effective implementation strategies. Our research objective was to systematically review and summarize previous studies that examined facilitators and barriers to implementing interventions to increase CRCS participation in primary care. Our review addressed the following research question: “What are the facilitators and barriers to implementing interventions to increase CRCS participation in primary care?”
Methods
Data Sources
We conducted a systematic review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement.14 We searched PubMed, Medline (EBSCO), and CINAHL, from the inception of these databases to April 2020. Search strategy was developed with the assistance of content experts and a research librarian as well as a preliminary review of the literature to identify potential terms. The search strategy combined a set of terms related to barriers/facilitators, interventions, CRCS/FIT, and participation (see Table 1 in the online Appendix).
Exclusion and Inclusion Criteria
The inclusion criteria for this review were (1) the study implemented a multicomponent intervention (must include at least 1: provider reminders, patient education, in-clinic FIT kit distribution or FIT kit mailing, patient reminders and follow up); (2) the study assessed implementation barriers and facilitators; (3) the study was conducted in OECD (Organization for Economic Co-Operation and Development) countries; (4) the study used an observational or experimental or qualitative study design and provided original and empirical evidence; (5) the article written in the English language.
Study Identification
Two authors (JL and MB) performed title and abstract review, followed by full text review for inclusion using those criteria. KA independently reviewed 20% of a random sample of articles at both phases to ensure reliability. Discrepancies between authors were settled by consensus.
Quality Assessment
Quality of the included studies were appraised in duplicates by 2 authors (KA and KM) using quality assessment tools as appropriate to study designs: the Critical Appraisal Skills Program for qualitative studies,15 the Mixed Methods Appraisal Tool for quantitative studies,16 and the Quality Improvement Minimum Criteria Set for quality improvement studies.17 Inconsistencies between authors were resolved by consensus.
Data Extraction
We constructed, pilot-tested, and refined a structured data extraction tool (see Table 2 in the online Appendix). JL and KA extracted data. Data extraction on 20% of the included articles was done by both data extractors to check consistency.
Data Analysis
All studies identified and excluded were summarized using a PRISMA flow diagram.14 We summarized individual study characteristics and their key findings on barriers and facilitators using narrative synthesis.18 We synthesized reported barriers and facilitators into distinct categories for the purpose of practical application and documented the frequency of these categories. Then, we classified the categories of facilitators and barriers according to the Consolidated Framework for Implementation Research (CFIR) domains and their subdomains.
The CFIR organizes implementation factors into 5 major domains (intervention characteristics; inner setting; outer setting; characteristics of the individuals involved; and implementation process) and their constructs. We selected the CFIR as our guiding framework as it includes comprehensive factors affecting implementation at multiple levels, can be applied to both qualitative and quantitative articles, and serves as a standardized structure for aggregating findings across studies in a systematic manner.
Results
Characteristics of the Studies
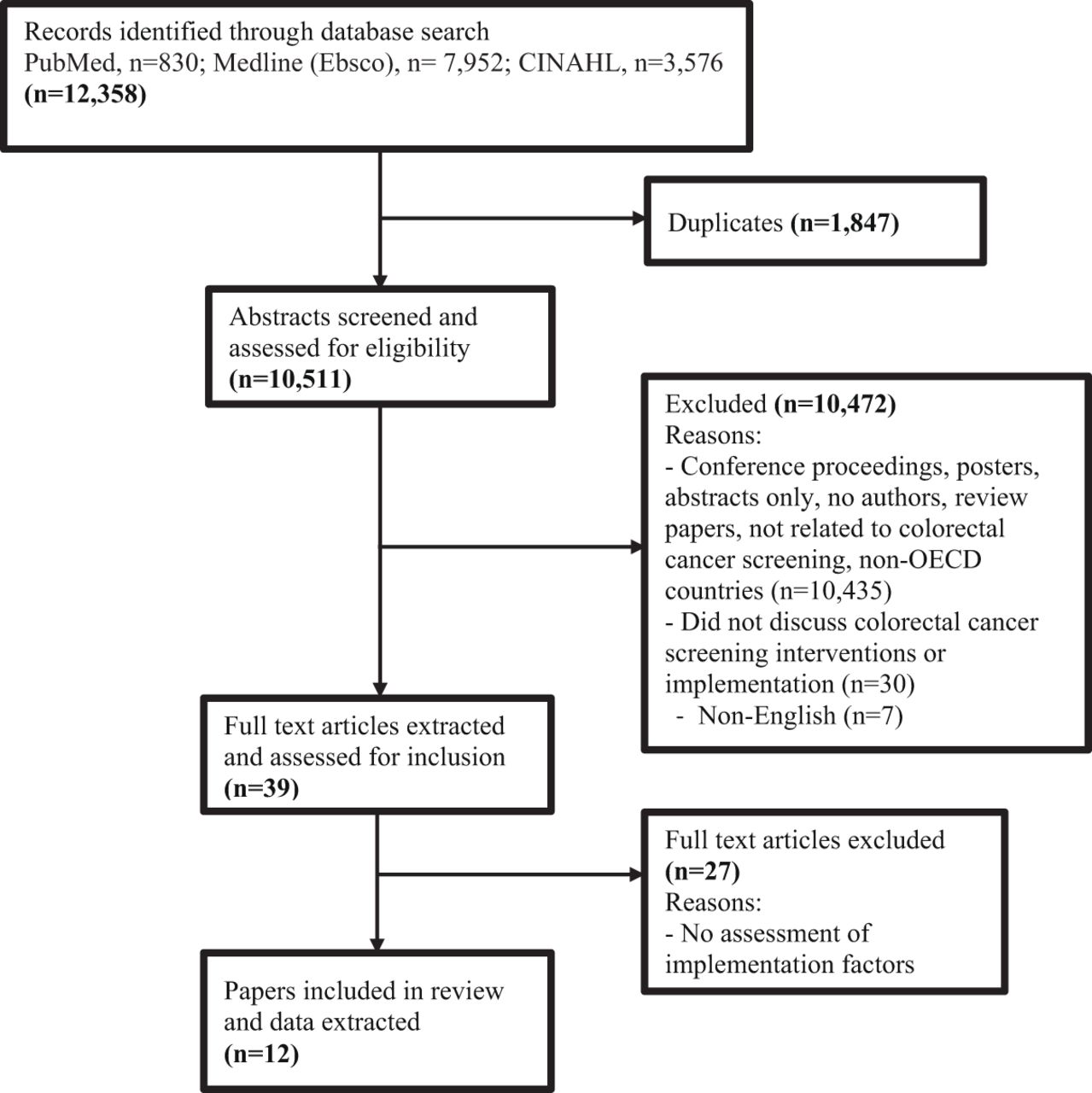
The initial search returned 10,511 deduplicated articles, of which 10,472 were excluded based on the title and abstract screening. We performed a full-text review on 39 articles. Of those, 12 studies were included in the review (Figure 1).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram. Abbreviation: OECD, Organization for Economic Co-Operation and Development.
Almost all included studies were from the United States. Nine studies used a qualitative study design, 2 used quality improvement, and 1 used a quantitative study design to obtain data pertaining to barriers and/or facilitators. Five studies used the CFIR framework (including all or some domains)11 and 1 study used the RE-AIM (reach, effectiveness, adoption, implementation, maintenance) framework19 to guide the assessment of barriers and facilitators. Most studies collected data using an interview method with a semistructured guide (n = 10) with data from clinic staff, providers, and clinicians, and few studies collected from organizational key leaders (including CEO, Medical Director, Nursing Directors) and the project team (Table 1).
Characteristics of Included Studies
Quality of the Included Studies
All qualitative studies20⇓⇓⇓⇓⇓⇓⇓–28 were judged to have a clear research aim, appropriate qualitative methodology and research design, data collection that addressed the research issue, a clear statement of findings, and results that would provide local benefit. However, none of the studies mentioned whether the relationship between the researcher and participants was adequately considered. The included quantitative study29 was judged as meeting 4 of the 5 quality criteria (relevant sampling strategy, representative sample, appropriate measurements, and appropriate statistical analysis), with the exception of risk for nonresponse bias. The quality improvement studies30,31 were judged as meeting all criteria on the checklist (Table 2).
Quality Assessment of Included Studies
Facilitators
Detailed facilitators and barriers are described in Table 3 and in Table 3 in the online Appendix. The following 7 factors were most commonly reported across studies as facilitators for the successful implementation of interventions aiming to improve CRCS participation rate (Table 4).
Facilitators and Barriers of Implementation of Interventions to Improve Colorectal Cancer Screening (CRCS) Reported by Included Studies, Organized in Consolidated Framework for Implementation Research (CFIR) Domains
Summary of Commonly Discussed Facilitators and Barriers and the Number of Studies They Were Identified In
Engagement was the most commonly reported facilitator, mapped to the CFIR constructs “readiness for implementation” and “implementation process” (engagement). Active engagement of clinic team members, clinic champions, leadership members, and stakeholders was important before and during implementation. Engagement included informing staff and leadership about the intervention, involving them in training and planning, and building relationships with primary care stakeholders. Priority or motivation to improve CRCS was also a key facilitator, mapped to the CFIR constructs “implementation culture and climate” and “individuals' knowledge and beliefs about the intervention.” This included providers and leaders valuing preventive health care, prioritizing screening programs, and recognizing benefits of CRCS interventions and the existence of organizational goals and activities on CRCS or quality improvement. Similarly, use of robust EMR systems, mapping to “readiness for implementation” on the CFIR, was seen as important for CRCS practice improvement work, tracking the practice, and for performance monitoring and evaluation. An ideal EMR would have FIT workflow built in and capture accurate data including identification of eligible patients for CRCS.
In addition, resources staff's time, knowledge, skills, and training, and availability of well-packaged materials were related to the CFIR constructs “design quality and packaging,” “implementation process (executing),” “knowledge and beliefs about the intervention,” and “readiness for implementation.” Implementation was facilitated by having dedicated and trained clinic staff to support the implementation, tested and well packaged educational materials, leveraging existing resources, and undisrupted clinic workflow. Continuous monitoring, feedback and reflection system of performance for improvement was mapped to the CFIR construct ‘reflection and evaluation’. Strong quality improvement processes allowed for producing accurate, transparent and actionable reports; sharing reports to inform the team including administrative leadership; using reports to identify and prioritize actions, and monitoring progress. Communication and coordination between clinic team and clinic's autonomy to try new innovations and adapt the intervention, mapping to the CFIR constructs ‘networking and communication’ and ‘implementation climate or process (execution),’ respectively also supported the implementation.
Barriers
The following 7 factors were most commonly reported as barriers to implementing interventions to improve CRCS (Table 4).
Limited time of clinic team for a new project was the most commonly reported barrier, mapped to the CFIR constructs “readiness for implementation' and ‘implementation process.” Challenges were related to limited staff time to commit to a new project, competing priorities, and a busy clinic environment due to existing activities or serving to acute health conditions. Challenges or unavailability of getting accurate and timely data, another commonly reported barrier, was mapped to the CFIR construct “implementation process (reflection and evaluation).” Challenges such as getting accurate and timely CRCS related data and inability to show the value of the implementation efforts impeded the implementation. EMR-related challenges, mapping to the CFIR construct “readiness for implementation,” included limited staff capability for using the EMR, time-consuming process to modify EMR functionalities for the CRCS intervention and lack of EMR supports. These resulted in challenges with: using the EMR database and tools/reminders, documentation, and extracting accurate data.
Communication and coordination barriers, mapped to the CFIR constructs ‘networking and communication’ and ‘implementation process (engaging)’ included disconnection between clinic team members and lack of role clarity on intervention implementation. Patient-related barriers were mapped to the CFIR construct p”atients' need and resources.” Studies reported a lack of insurance coverage for CRCS, low health literacy, limited access due to transportation problems, and hesitancy of certain minority ethnic groups to talk about or collect stool. In addition, the lack of leadership engagement and organizational changes and implementation process barriers, mapping to the CFIR constructs “readiness for implementation” and “implementation process (planning and executing),” respectively, negatively impacted the implementation. These included a lack of standard workflow, cumbersome workflow, delays from vendors in receiving FIT kits, a lack of involvement of high-level leadership, and organizational leadership structure changes.
Discussion
Interpretations
The multitude of identified facilitators and barriers across multiple levels show a complex picture of difficulties and opportunities faced while implementing evidence-based interventions in primary care. In general, the most commonly reported facilitators and barriers fell under: (1) clinic's implementation readiness and climate, and network and communication between the clinic team members (CFIR domain: clinic's internal setting); (2) project engagement, execution, and evaluation (CFIR domain: implementation process); (3) knowledge and beliefs about the intervention of individuals involved (CFIR domain: characteristics of individuals); and (4) patients' need and resources (CFIR domain: outer setting). Furthermore, while the majority of reported implementation facilitators and barriers are generic to improvement work in primary care, some were more specific to CRCS intervention implementation. The CRCS intervention specific facilitators included: providers', leaders', and organizations' motivation and commitment to improve CRCS rate; creation of awareness about CRCS to patients and family; and review of data to improve CRCS efforts. Some of the CRCS intervention specific barriers included: conflicting opinions of clinical staff on approaches to improving CRCS; FIT kit mail-out approach being too impersonal/inferior to face-to-face encounters; unavailability of FIT kits; and impact on colonoscopy access for higher number of positive FIT results (as a result of increased FIT participation). These findings suggest that planners of intervention programs could benefit from considering implementation factors important both in general for primary care and specific to the particular intervention.
However, it is important to acknowledge that these observed findings are also dependent on what was measured and reported in the studies. The studies that used implementation science frameworks captured the implementation factors more comprehensively than those that did not use a framework. They captured both general and CRCS intervention specific factors across different aspects of implementation. While no other systematic review has been conducted on facilitators and barriers to CRCS intervention uptake, our findings are consistent with the literature on intervention implementation in primary care. Multi-level factors such as organizational leadership and managerial engagement, individual and organizational capacity and practices (tools, staffing, time, health professionals' motivation, skills, and knowledge), monitoring and evaluation, and multidisciplinary team communication influence implementation in primary care.32,33
Key Gaps and Policy/Practice Implications
We were surprised at how relatively few articles were studying the implementation factors of widely recommended interventions to improve CRCS in OECD countries. The studies had limited methodological rigor and lacked clarity on implementation details. The description of length/duration of implementation, adoption and adaptation of strategies, measurement constructs, implications or utility of identified barriers and facilitators was inadequate. Similarly, the relationship between the researcher and participants, which impacts response bias, was not mentioned in any of the qualitative studies. We suggest that future research be undertaken using implementation science frameworks to enhance clarity and transparency of reporting the implementation and methodology rigor.11,13,19,34⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓–45
Behavioral interventions or strategies for health services are rarely “one-size-fits-all” due to the tremendous diversity of populations and real-world settings.41,46⇓–48 Assessment of barriers and facilitators is an essential step to help understand the implementation context. We recommend future studies to develop customized strategies through intervention mapping based on the barriers and facilitators identified49 and evaluate these strategies. Overall, commitment to both implementing patient-centered CRCS improvement interventions in primary care settings and conducting implementation research to generate knowledge of real-world applicability are critical to improve CRCS participation.
Strengths and Limitations of the Review
We used a systematic approach, rigorous, yet feasible methods in a resource constrained health services research environment. Efforts were made to maintain consistency across reviewers (eg, training, regular meetings). However, we were unable to include 2 independent reviewers fully in each step. We mapped the reported findings with CFIR constructs to provide a comprehensive, systematic picture of facilitators and barriers to guide the identification of strategies that could be tailored, implemented and tested in the future. However, the barriers and facilitators reported here are the experiences of diverse primary care contexts. We did not analyze the barriers and facilitators by the types of participants, settings, and specific intervention due to the data limitations. The implementation challenges regarding organizational structure, implementation climate and readiness, and implementation process may differ across them. In addition, this analysis relied on peer-reviewed published articles and is subject to publication bias.
Conclusions
The summary of synthesized findings improves our understanding of facilitators of and barriers to the implementation of interventions to increase CRCS uptake/FIT participation in primary care practice. The understanding can help researchers, decision makers, primary care practitioners, and program developers in the careful design of interventions and development of strategies to optimize implementation. Future studies assessing CRCS intervention implementation factors would benefit from the use of implementation science frameworks to further understand the context of implementation and enhance understanding of how to implement these programs more effectively.
Notes
This article was externally peer reviewed.
Conflict of interest: The authors have no conflict of interest.
Funding: This research was funded by Alberta Health through the Alberta Cancer Prevention Legacy Fund (ACPLF). Provision of funding by Alberta Health does not signify that this project represents the policies or views of Alberta Health. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
To see this article online, please go to: http://jabfm.org/content/35/4/840.full.
- Received for publication October 4, 2021.
- Revision received December 6, 2021.
- Revision received December 20, 2021.
- Accepted for publication December 21, 2021.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Social Determinants of Health Influencing Colorectal Cancer Screening Behaviors Among Community Residents in China: A Scoping Review Protocol
- Evaluating the implementation of a multicomponent intervention to improve faecal immunochemical test-based (FIT) colorectal cancer screening in primary care
- Barriers and facilitators of implementing a multicomponent intervention to improve faecal immunochemical test (FIT) colorectal cancer screening in primary care clinics, Alberta
- Primary care provider interventions for addressing cancer screening participation with marginalised patients: a scoping review protocol
- Family Medicine Researchers Explore the Social Determinants of Health, COVID-19 Issues, and Cancer Survivor Care