
Abstract
Background: During cancer treatments, patients often defer primary care and comorbidity management, which may not be optimal for overall health when patients transition into survivorship. We sought to quantify primary care utilization among cancer survivors who are ≥2 years post cancer treatments.
Methods: 951 cancer survivors were included in this national, prospective cohort study using the Regional Geographic and Racial Differences in Stroke (REGARDS) data.
Results: Nearly all (91.6%) cancer survivors had at least 1 annual PCP visit and most (54.6%) had a PCP as their dominant provider.
Conclusion: These findings underscore the urgent need for smooth handoffs from oncology back to primary care.
Introduction
During active cancer treatments, patients often exclusively see oncologists and other cancer care providers, deferring their primary care and comorbidity management.1 While this may be understandable during the acute cancer treatment phase, it may not be optimal for overall health when a patient transitions into survivorship. Among cancer patients who survive 5+ years from diagnosis, cardiovascular disease, rather than cancer, is the leading cause of death.2⇓⇓–5
Nearly 70% of cancer patients have least 1 co-occurring chronic medical condition.6 Prevalence of comorbidities in combination with direct cardio-toxic effects of certain cancer therapies7 may put cancer patients at increased risk for poor noncancer outcomes that could benefit from attention by a primary care provider (PCP). Prior reports show that cancer survivors who exclusively see oncologists are less likely to receive noncancer care (eg, cholesterol screening, influenza vaccinations, and bone densitometry) compared with survivors who were also cared for by PCPs.8
Previous studies have documented lack of care coordination between oncology and primary care at the conclusion of cancer treatments.1 PCPs and oncologists caring for cancer patients have reported that lack of coordination between the 2 specialties presented “substantial barriers” to effectively managing patients.9 However, the proportion of cancer survivors who return to primary care is not yet known. If the number of cancer survivors needing a handoff to primary care is large, it would suggest that systematic improvements in oncology-to-PCP handoffs are needed. We sought to describe primary care utilization among a population-based group of cancer survivors ≥2 years after the conclusion of cancer treatments.
Methods
Study Design, Population, and Data
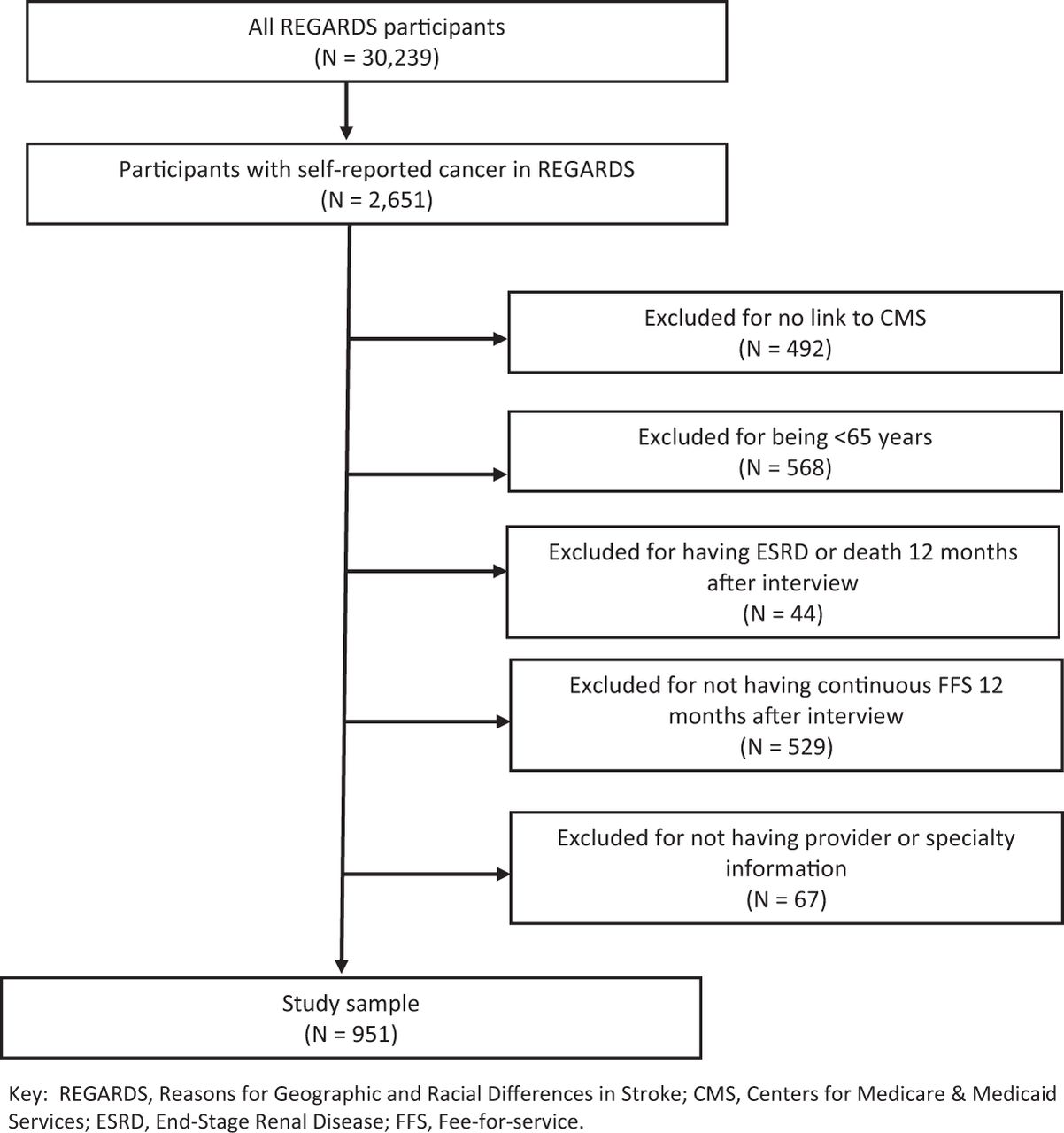
We conducted a national, prospective cohort study using the Regional Geographic and Racial Differences in Stroke (REGARDS)10 study data. Between 2003 to 2007, REGARDS recruited 30,239 individuals ≥45 years of age and observation is ongoing. Among adults who gave consent, REGARDS was linked to Medicare fee-for-service claims.11 For this study, we used baseline REGARDS data collected from 2005 to 2007 and Medicare claims for the first 12 months after the baseline survey. This study was approved by the Institutional Review Boards at the participating institutions. All participants provided written informed consent.
Cohort
There were 20,403 REGARDS participants linked to Medicare. Of those, we included adults who: 1) were ≥65 years old, 2) had continuous fee-for-service coverage for 365 days after their baseline survey, 3) did not have end-stage renal disease, and 4) had a self-reported history of cancer and had completed treatments ≥2 years ago.
Statistical Analyses
We examined ambulatory care visit patterns among cancer survivors in the 12 months after baseline REGARDS survey. We described median and interquartile ranges (IQR) of visits and providers. Then we described the specialty of the most frequently seen provider, which we call the “dominant provider.” We categorized the dominant provider as primary care versus not. We compared differences in socio-demographics, lifestyle, and comorbid conditions between those whose dominant provider was in primary care to those whose dominant provider was not.
Results
We included 951 cancer survivors who were ≥2 years since receiving cancer treatments (Figure 1). The mean age was 73.9 years, 42.9% were female, and 29.1% were Black (Table 1). Cancer survivors had a median of 9 visits (IQR 5,14) to a median of 4 providers (IQR 3,6) in the 12 months following their baseline survey. More than 90% (91.6%) had at least 1 visit with a PCP during this time. Nearly 88% of cancer survivors saw only a PCP, 3.8% saw both an oncologist and a PCP, 0.2% saw only an oncologist, and 8.2% saw neither an oncologist nor PCP. More than half (54.6%) of cancer survivors had a PCP as their dominant provider (Table 2). Two percent had an oncologist, 6.0% had a cardiologist, 1% had an endocrinologist, and 36.7% had other specialty providers as their dominant provider. We did not observe statistically significant differences in socio-demographics, lifestyle, and comorbid conditions between individuals with and without PCPs as their dominant provider.
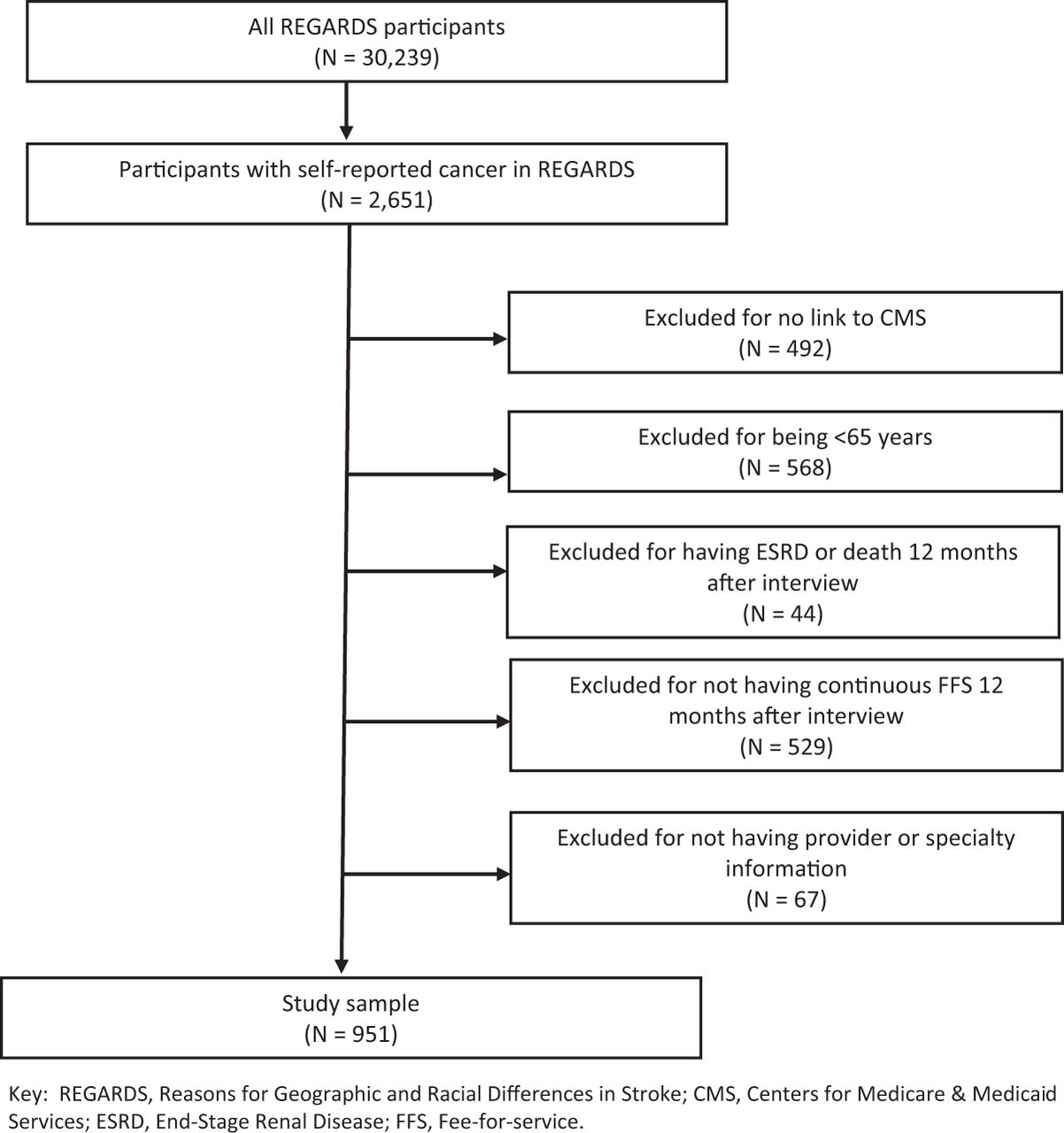
Exclusion cascade for sample derivation.
Cohort Characteristics Between Cancer Survivors With and Without a Primary Care Dominant Provider
Specialty Codes of the Dominant Providers
Discussion
To our knowledge, this is the first study to document that nearly all (91.6%) cancer survivors (that is, those who are ≥2 years since active cancer treatments) have at least 1 annual visit to a PCP. Moreover, most (54.6%) cancer survivors had a PCP as their dominant provider and 88% saw only a PCP. Our findings suggest that a large proportion of cancer survivors could benefit from a smooth handoff from oncology to primary care.
Several different strategies have been suggested as ways to improve handoffs between oncologists and PCPs.9 For example, survivorship care plans (SCP), have been proposed to improve communication between oncology and primary care at the end of active cancer treatments and increase cancer-specific knowledge among PCPs.12 A SCP would inform the PCP of specific cancer therapies that were received and how they may put cancer survivors at increased risk for noncancer outcomes including weight gain due to hormone therapy, elevated glucose due to steroids, and coronary artery disease due to chemotherapy regimens. However, these plans are inconsistently implemented, and many PCPs never receive the SCPs. Shared leadership (team-based care models that purposefully share responsibility and have mutual influence on patient care) has also been suggested as a solution to improve the transition from oncology to primary care by clearing defining provider roles and respon sibilities in the care of the patient.13 However, this approach has not been extensively implemented or tested. Given the suboptimal transitions from oncology to primary care, many cancer survivors are left unsure which provider should be responsible for their care following cancer treatments.12
Some limitations of this work include lack of data before the REGARDS baseline survey, lack of cancer-specific information (cancer type, tumor characteristics, cancer treatments received, and time since cancer diagnosis) as well as generalizability to cancer survivors at all time points in the cancer care continuum.
Our study indicates that nearly all cancer patients return to primary care after they complete cancer treatments. More research is needed on how best to achieve effective hand-offs and then how best to disseminate the most effective strategy. The potential benefits realized from efforts to improve transitions from oncology to primary care would not be restricted to a small subset of patients but may improve the quality of care for the majority of cancer survivors.
Acknowledgments
This manuscript was reviewed by the REGARDS Executive Committee prior to submission to ensure adherence to standards for describing the REGARDS study.
The authors thank the other investigators, the staff, and the participants of the REGARDS study for their valuable contributions. A full list of participating REGARDS investigators and institutions can be found at: https://www.uab.edu/soph/regardsstudy/.
Notes
This article was externally peer reviewed.
Funding: This analysis and the survey on healthcare experiences was supported by R01HL135199 from the National Heart Lung and Blood Institute, National Institutes of Health, Department of Health and Human Service. REGARDS is supported by cooperative agreement U01 NS041588 co-funded by the National Institute of Neurological Disorders and Stroke (NINDS) and the National Institute on Aging (NIA), National Institutes of Health, Department of Health and Human Service. This work was also supported by the National Cancer Institute at the National Institutes of Health (NCI) (K01 CA251645). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NHLBI, NINDS, NCI or NIA.
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/35/4/827.full.
- Received for publication January 6, 2022.
- Revision received March 14, 2022.
- Accepted for publication March 21, 2022.




{kind=link}