
Abstract
Background: The COVID-19 pandemic led to wide adoption of telehealth in primary care. The impact of telehealth on subsequent follow-up visit volume is mixed. This study examines the association of newly expanded telehealth with short-interval follow-up visits during the COVID-19 pandemic in an academic primary care practice.
Methods: Scheduling data were used to compare rates of 0 to 60-day follow-up visits after telehealth and in-person visits before and after onset of the COVID-19 pandemic.
Results: Compared with in-person visits, telehealth visits were associated with significantly higher rates of total short-interval follow-ups and higher rates of first short-interval follow-ups occurring in 0 to 15 days.
Discussion: Higher rates of short-interval follow-up may be due to inefficiencies created by rapid expansion of telehealth including suboptimal scheduling algorithms, pandemic-related safety considerations, and discomfort with the visit modality. Short-interval follow-ups have potential negative impacts on practice access, patient-centered outcomes, and sustainability of telehealth in primary care.
Conclusion: Newly expanded telehealth visits conducted in the year after the onset of the COVID-19 pandemic resulted in higher rates and sooner first occurrence of short-interval follow-up visits. Future research should identify optimal scheduling processes for telehealth visits to minimize short-interval follow-ups.
- COVID-19
- Family Medicine
- Follow-Up Visits
- Pandemics
- Patient-Centered Care
- Primary Health Care
- Telemedicine
Background
The onset of the COVID-19 pandemic prompted rapid expansion of telehealth services to care for patients as safely as possible. This expansion was facilitated by policies easing delivery of telehealth.1 Telehealth use has declined from 32% of all outpatient visits immediately after the onset of the pandemic to 13 to 17% of current outpatient visits. Still, this represents 38 times greater use of telehealth compared with before the pandemic.2
Telehealth is likely to remain integral to primary care in the future. Many patients want to continue telehealth visits postpandemic.3⇓–5 Providers enjoy telehealth5 and are motivated to integrate it into future practice.6 Both patients and providers believe telehealth can address most medical concerns, improve access, and facilitate quality care.3,4,6 Furthermore, ongoing use of telehealth is supported by legislation in multiple states.7
In addition to patient, provider, and policy support, efficient use of telehealth is necessary for sustainable integration into primary care. Only one third of visits to primary care are estimated to be suitable to telehealth.8,9 Unsuitable visits conducted via telehealth may lead to short-interval follow-up visits, reducing access and adversely affecting practice efficiency. Data are mixed as to whether telehealth visits are more likely to lead to short-interval follow-up visits than in-person visits.10⇓–12
This study examines the association of newly expanded telehealth with short-interval follow-up visits during the COVID-19 pandemic in an academic primary care practice.
Methods
This study was conducted in a 4-clinic, academic family medicine department in the Southwest United States. Our department is not affiliated with a residency program. All patients are seen by physicians or advance practice providers. The clinics are distributed across a large metropolitan area but are all similar in composition of clinicians and offer the same primary care services. Before March 2020, local regulations afforded reimbursement parity for a limited number of telehealth services and our practice conducted relatively few telehealth visits. Irrespective of the pandemic, our institution was preparing for our state's plan to significantly expand telehealth service payment parity in 2021. Therefore, at the time of the COVID-19 public health emergency declaration and associated telehealth expansion waiver, our practice had the technology platform, scheduling, and billing workflows in place to quickly expand telephone and video synchronous telehealth services. In March 2020, we began widely offering telephone visits. Simultaneously, clinicians were provided online video and written training materials on synchronous video telehealth, and video cameras were distributed across the practice. Synchronous video visits were started in April 2020.
In our practice, telehealth visits were scheduled at the discretion of a provider or patient at the time of appointment request. After March 2020, all patients requesting appointments in our department were offered the option of a telehealth visit. Any patients reporting symptoms consistent with positive COVID-19 infection had their visit via telehealth. Patient self-scheduling was not possible before or during the study period.
Data from our electronic health record scheduling module were used to identify all telehealth and in-person visits conducted with a physician or advance practice provider from April 2019, 1 year before the onset of the pandemic, through March 2021, 1 year after the onset of the pandemic. Data from April 2019 through March 2020 were defined as the prepandemic period and data from April 2020 through March 2021 were defined as the pandemic period.
Routine follow-up is common in primary care, and many chronic conditions require a follow-up frequency of 3 months. To exclude visits associated with routine follow-up, a short-interval follow-up was defined as any visit, whether in-person or telehealth, for the same patient occurring within 60 days of an index visit, and an index visit was defined as a visit without another visit in our department in the preceding 90 days. It is possible to have multiple short-interval follow-up visits associated with a single index visit.
Short-interval follow-up visits were stratified into 3 subgroups, those occurring between 0 and 15 days, 16 and 30 days, and 31 and 60 days.
The rate of index visits leading to short-interval follow-up in the prepandemic period served as a baseline. The total short-interval follow-up rate and rate of first occurrence short-interval follow-up for pandemic period telehealth index visits were compared with baseline and to pandemic period in-person index visit short-interval follow-up rates.
Examined scheduling data did not include patient identifiers and institutional review board (IRB) review was deemed unnecessary by the Mayo Clinic IRB.
Description of Statistical Methods
Rate of short-interval follow-up was calculated for the first occurrence and categorized by time frame (0 to 15, 16 to 30, and 31 to 60 days). Comparisons between pandemic period and index visit type were made by use of Chi-Square (χ2) test for proportions. Cumulative incidence of first short-interval follow-up was calculated and compared between index visit type. R version 3.6.2 was used for statical analysis. P values < 0.05 were considered statistically significant.
Results
A total of 49,246 visits (including index and nonindex visits) were conducted during the prepandemic period, of which 48,763 (99%) were in person and 483 (1%) were telehealth. During the pandemic period, a total of 39,881 visits (including index and nonindex visits) were conducted and 27,362 (68.6%) were in person and 12,519 (31.4%) were telehealth. A similar distribution of age and sex was seen between prepandemic and pandemic periods (Table 1).
Patient Demographics in Prepandemic and Pandemic Period
During the prepandemic period a total of 30,715/49,246 (62.4%) visits were index visits, 30,446 of which were in person and 269 (0.9%) were telehealth (Table 2).
Index Visits and Short-Interval Follow-Up Rates by Visit Type in Prepandemic and Pandemic Period
During the pandemic period a total of 26,291/39,881 (65.9%) visits were index visits, of which 18,983 (72.2%) were in person and 7,308 (27.8%) were telehealth (Table 2).
Total Short-Interval Follow-Up Visits
Prepandemic Period
When the prepandemic index visit was in person (n = 30,446), 1 or more short-interval follow-up visits occurred in 6,661 (21.9%) of the index visits. A total of 14,071 short-interval follow-up visits occurred, of which 3,540 were between 0 and 15 days, 3,764 between 16 and 30 days, and 6,767 between 31 and 60 days.
When the prepandemic index visit was telehealth (n = 269), a total of 39 short-interval follow-up visits occurred, of which 12 were between 0 and 15 days, 12 between 16 and 30 days, and 15 between 31 and 60 days.
Pandemic Period
The rate of pandemic period in-person index visits resulting in short-interval follow-up was lower than baseline. When the pandemic index visit was in person (n = 18,983), 1 or more short-interval follow-up visits occurred in 3,191 (16.8%) of the index visits as compared with 21.9% of baseline prepandemic index visits. A total of 6,417 short-interval follow-up visits occurred, of which 1,455 were between 0 and 15 days, 1,745 between 16 and 30 days, and 3,217 between 31 and 60 days.
When the pandemic index visit was telehealth (n = 7308), 1 or more short-interval follow-up visits occurred in 1669 (22.8%) of the index visits. The rate of short-interval follow-up was similar for telephone and video index visits (Table 2). This rate was similar to the baseline prepandemic short-interval follow-up rate and significantly higher than the in-person index visit short-interval follow-up rate (Table 2). A total of 3767 short-interval follow-up visits occurred, of which 1148 were between 0 and 15 days, 1047 between 16 and 30 days, and 1572 between 31 and 60 days.
First Occurrence Short-Interval Follow-Up Visit
Prepandemic Period
In the in-person index visit group, 6661 index visits had short-interval follow-ups, of which 1559 (23.4%) were between 0 and 15 days, 1807 (27.13%) between 16 and 30 days, and 3295 (49.47%) between 31 and 60 days for the first occurrence.
Pandemic Period
Telehealth index visits were significantly more likely to result in earlier first occurrence short-interval follow-up than in-person index visits (Figure 1).
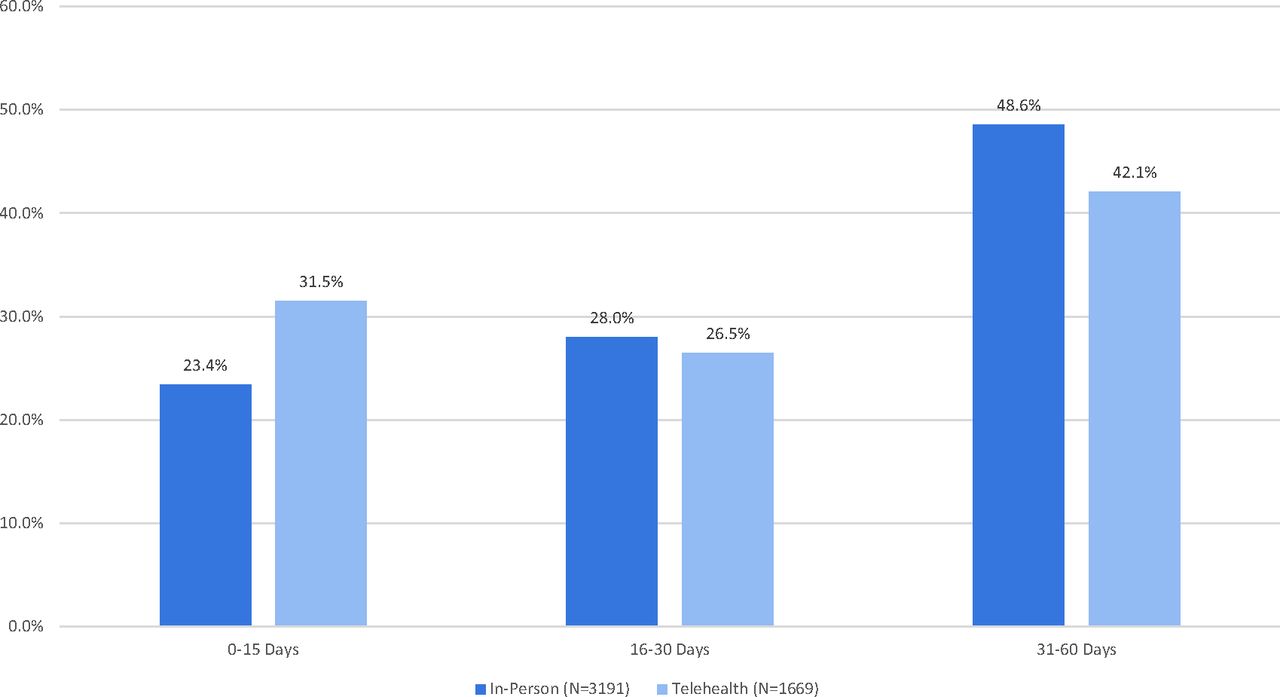
Timing of first occurrence short interval follow-up during the pandemic period (p value < 0.001).
In the in-person index visit group, 3191 index visits had short-interval follow-ups, of which 748 (23.44%) were between 0 and 15 days, 892 (27.95%) between 16 and 30 days, and 1551 (48.61%) between 31 and 60 days for the first occurrence.
In the telehealth index visit group, 1669 index visits had short-interval follow-up, of which 525 (31.46%) were between 0 and 15 days, 442 (26.48%) between 16 and 30 days, and 702 (42.06%) between 31 and 60 days for the first occurrence. No difference was found in timing of first occurrence short-interval follow-up between telephone and video index visits.
Discussion
Newly expanded telehealth visits were associated with significantly higher rates of total short-interval follow-up visits and sooner first occurrence of short-interval follow-up visits compared with in-person visits in the year after the onset of the COVID-19 pandemic. These findings are similar to prepandemic insurance claims data showing higher subsequent visit rates after video visits compared with in-person visits.11 However, a study of a large primary care practice with well-established telehealth services showed rates of short-interval follow-up between telehealth and in-person index visits were similar,13 suggesting telehealth can be implemented in a manner that does not increase downstream use in certain contexts.
Although the rate of telehealth-associated short-interval follow-up in the pandemic period was similar to the baseline prepandemic rate of short-interval follow-up, it was significantly higher than the rate of pandemic period in-person-associated short-interval follow-up. This suggests an important difference in rate of short-interval follow-up visits between in-person and telehealth index visits in the pandemic period. There are multiple potential reasons for this meaningful difference.
We found notably higher rates of short-interval follow-ups occurring within 2 weeks of a telehealth visit. This finding may be due, in part, to the sudden, rapid expansion of telehealth in our practice. We accelerated our implementation and provider training and did not have adequate time for patient education on telehealth. Therefore, providers and patients may have felt unprepared to navigate an encounter without the ability to fully gauge body language or perform a physical examination. This may have led both providers or patients to request an in-person follow-up visit in a few days to assure a thorough assessment had been completed and an accurate diagnosis reached. If initial unfamiliarity and discomfort with telehealth contributed to our findings, we expect rates of telehealth-associated short-interval follow-ups will decrease over time as patients and providers become accustomed to this visit modality.
Higher rates of telemedicine short-interval follow-ups may have been driven by the characteristics of our scheduling practices. Since the number of appointments on provider schedule template was fixed, increasing telehealth appointments decreased availability of in-person appointments. It is possible that the earliest available appointment was telehealth rather than in person. The patient or provider may have chosen the earliest available appointment regardless of perception of the appropriateness of visit type for the complaint, which may have increased the need for a short-interval follow-up.
Similarly, in the year following the onset of the pandemic, patients with COVID symptoms could only be seen via telehealth. While some evidence suggests patients initially seen for COVID symptoms do not require higher rates of follow-up if seen via telehealth,12 and many patients with acute illnesses will self-select out of telehealth when given the choice,14 prepandemic data of telehealth visits conducted for upper respiratory symptoms demonstrated significantly higher follow-up rates than in-person visits.10 As safety concerns related to the COVID-19 pandemic subside, identifying patients presenting with acute physical symptoms and directing them to in-person visits may reduce telehealth-associated short-interval follow-ups.
Some patients with nonacute reasons for visit may also be less suitable for telehealth. Patients who rate their health as poor are less likely to be satisfied with telehealth than those who rate their health as good.5 Refined telehealth scheduling algorithms should consider reason for visit and patient health status to improve patient and provider satisfaction with telehealth and potentially reduce rates of short-interval follow-ups. However, development of such algorithms in primary care is challenging. Most primary care visits address multiple issues,15 and many of these may not be shared with the scheduler when the appointment is made. In addition, as patient self-scheduling becomes more common in primary care, accurate and complete understanding of reason for visit may become even less predictable and appropriate assignment of visit type less reliable.
Our findings have significant implications for both primary care practices and patients. While some acute illnesses or disease exacerbations warrant close follow-up, unnecessary use of 2 visits because the initial visit type was inappropriate reduces overall clinic access. To accommodate the increased need for post-telehealth follow-up visits, especially those between 0 and 15 days, practices may have to reserve unusually high numbers of open appointment slots or risk further delaying appropriate evaluation, reducing patient satisfaction and potentially leading to unnecessary urgent care or emergency department visits. The negative impact on clinic access is particularly troublesome in primary care, where practices are often excessively busy and access is already limited.
Unnecessary short-interval follow-up may reduce patient satisfaction with their care and cause undue financial burden on patients who must pay for 2 visits when 1 visit of the optimal type could have sufficed. This would disproportionately affect self-pay patients and those with high deductible insurance plans and exacerbate waste in our health care system. If telehealth visits are perceived as contributors to low-value care due to need for higher rates of follow-up, insurance carriers and lawmakers may reduce reimbursement and legislative support for telehealth.
Future research is needed to identify strategies for optimization of telehealth scheduling processes to minimize need for short-interval follow-up, thereby improving practice efficiency, improving patient-centered outcomes including cost and patient satisfaction, and promoting sustainability of telehealth in primary care.
Limitations
Our study is limited by the observational design. While we used scheduling data to assess visit type, timing, and frequency of follow-up visits, we did not assess documented reasons for visit or patient factors, including diagnoses or heath status. These unmeasured factors may confound our results. We studied newly expanded telehealth visits in the year immediately after the onset of the pandemic. Our findings may not apply to long-established telehealth practices or those operating later in the postpandemic period. Our practice is an academic family medicine practice in the Southwest, and the results of our study may not translate to community practices or different geographic areas.
Conclusions
Newly expanded telehealth visits conducted in the year after the onset of the COVID-19 pandemic resulted in higher rates and sooner first occurrence of short-interval follow-up visits than in-person visits. High rates of short-interval follow-up visits can adversely affect primary care practices and patient-centered outcomes. Future research should identify optimal scheduling processes for telehealth visits to minimize short-interval follow-ups.
Notes
This article was externally peer reviewed.
To see this article online, please go to: http://jabfm.org/content/35/3/485.full.
Funding: No funding was received for this project.
Conflict of interest: All authors report no conflicting or competing interests.
- Received for publication December 17, 2021.
- Revision received February 11, 2022.
- Accepted for publication February 14, 2022.




{kind=link}