
Abstract
Family physicians who are self-identified members of Black, Hispanic, and American Indian/Alaska Native racial groups are more likely to practice in disadvantaged areas but also tend to have narrower scopes of practice when compared with White family physicians, despite holding the same certification. Considering the established benefits of comprehensive primary care, these results suggest the need for policies incentivizing and supporting broader scopes of practice in disadvantaged areas
Insufficient access to needed services from trusted sources of care has been associated with persistent health outcome inequities in Black, Hispanic, and American Indian/Alaska Native racial/ethnic groups. Family physicians (FPs) are the most broadly and evenly distributed of all medical specialties, and the specialty trained to provide the widest scope of health care services.1 Evidence suggests that FPs' broader scope of practice is associated with stronger health systems, higher health care quality, higher certification examination scores, fewer hospitalizations, decreased total costs, and lower rates of physician burnout.2⇓–4 Although prior research found that FPs from Black, Hispanic, and American Indian/Alaska Native racial groups are more likely to practice in disadvantaged areas compared with their White peers,5 little is known about variation in their scope of practice, which may have implications for access and disparities.
We used the data collected from 6768 FPs completing the 2018 American Board of Family Medicine Continuing Certification Examination application questionnaire to examine variation in scope of health care services provided by FPs. Data were stratified by race/ethnicity and geographic social inequality as a proxy for lack of services in an area. Respondents self-reported their race as either White, Black, Asian, American Indian or Alaska Native, Native Hawaiian or Other Pacific Islander, or Other, and their ethnicity as Non-Hispanic or Hispanic/Latino. Self-reported scope of practice was measured on the “SP4PC,” which is calculated based on the Rasch model and ranges from 0 to 30, with larger value indicating broader scope of practice.6 Geographic social inequality was assigned according to Zip Code Tabulation Areas Social Deprivation Index (SDI),7 which is normally distributed with a score from 0 to 100, where higher numbers suggest higher deprivation.8 The American Academy of Family Physicians Intuitional Review Board approved this study.
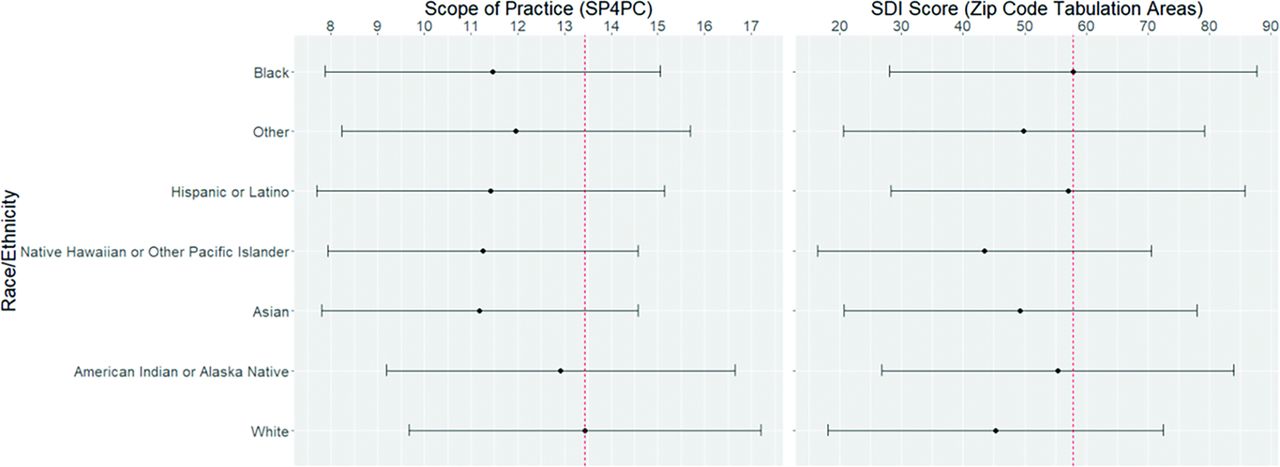
As Figure 1 reveals, Black FPs (n = 457; 6.8%) and Hispanic or Latino (n = 519; 7.7%) tended to serve in more disadvantaged areas (right panel of Figure 1, SDI = 57.9; t = 9.497, P < .001); SDI = 57.1; t = 8.393, P < .001, respectively) but had approximately 2 points (t = -11.42, P < .001; t = -9.951, P < .001, respectively) lower scope of practice (SP4PC reflected in the left panel, Figure 1) than their White counterparts. White FPs (n = 4745; 70.1%) reported the widest scope of practice but tended to practice in the least disadvantaged areas (SDI = 45.3; F = 20.58, P < .001). Asian (n = 1037; 15.3%) and Native Hawaiian or Other Pacific Islander (n = 44; 0.7%) had the narrowest self-reported scope of practice (SP4PC = 11.2; t = -18.70, P < .001; SP4PC = 11.3; t = -3.946, P < .001) and tended to serve in less disadvantaged counties than Hispanic/Latino or Black FPs. American Indian or Alaska Native (n = 62; 0.9%) also served in counties with moderate disadvantage (SDI = 55.4; t = 2.225, P = .026) but reported similar scope of practice as White physicians (SP4PC = 12.9; t = -0.408, P = .683).

SP4PC (left panel) and Social Deprivation Index (SDI) score (right panel) for family physicians of each race/ethnicity (vertical axis), from 2018 American Board of Family Medicine continuing certification candidates. Within each panel, dot and half bar length denote mean and standard deviation, respectively. The red dotted line in each panel serves as reference, representing the largest racial/ethnic group mean of SP4PC and SDI, respectively. Detailed information about SDI can be retrieved from Robert Graham Center website.10
Our results confirm the tendency of FPs from Black, Hispanic, and American Indian/Alaska Native racial groups to practice in counties with greater SDI, a proxy for poorer access, but also to report narrower scope of practice than White FPs. The benefits of comprehensive primary care and those associated with patient-physician racial concordance are well established,9 as are the challenges in accessing needed health care services in areas with high SDI.8 Our findings suggest that removing barriers to practicing broad-scope family medicine and incentivizing all FPs who work in disadvantaged counties may improve access to care and help reduce health care inequities.
Notes
This article was externally peer reviewed.
Funding/support: None.
To see this article online, please go to: http://jabfm.org/content/35/3/454.full.
Funding: The authors received no funding to conduct this research.
Conflict of interest: TW, AE, and AB are employees of the American Board of Family Medicine. AA is a member of the Board of Directors of the American Board of Family Medicine.
See Related Commentary on Page 597.
- Received for publication September 1, 2021.
- Revision received November 1, 2021.
- Accepted for publication November 3, 2021.




{kind=link}