
Article Figures & Data
Figures
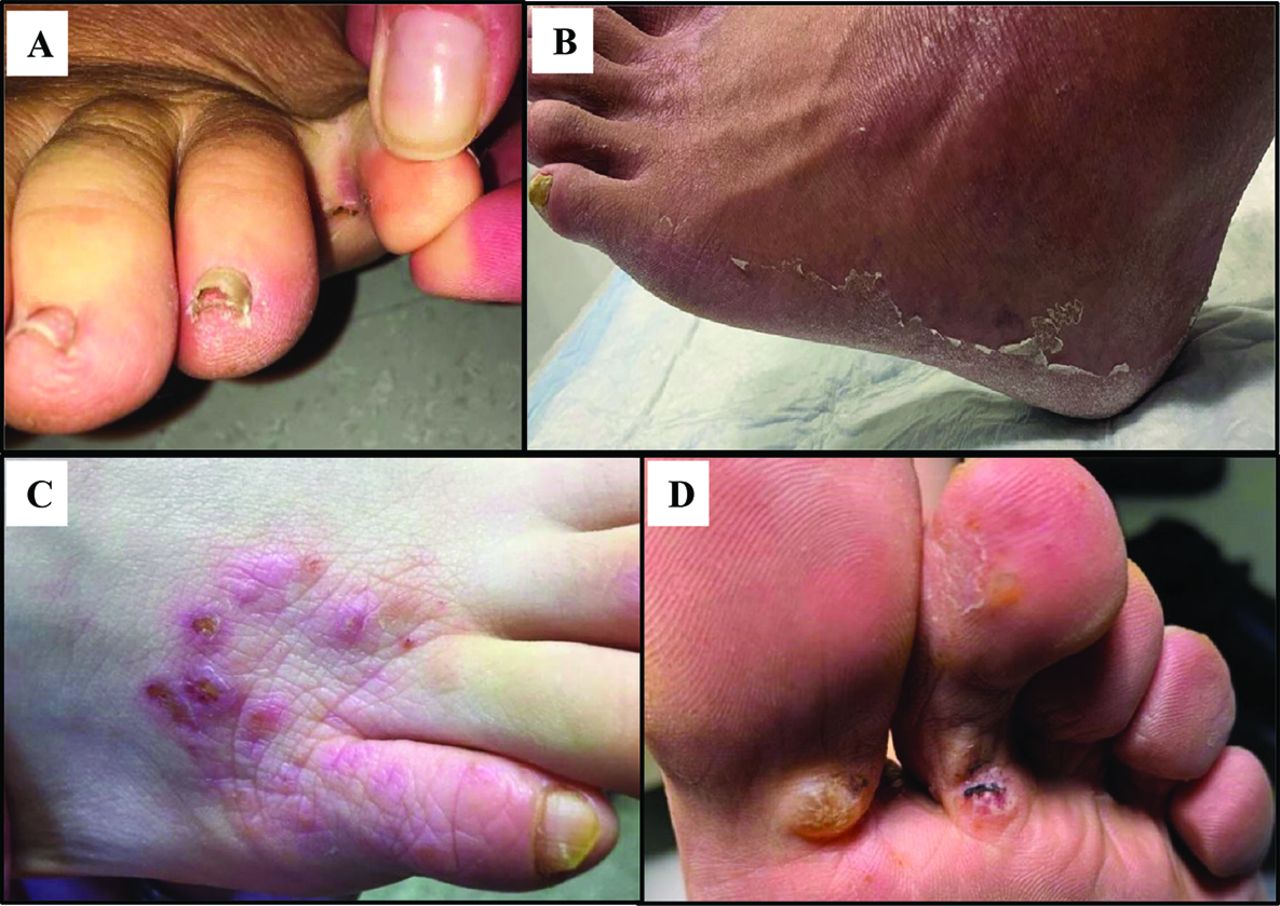
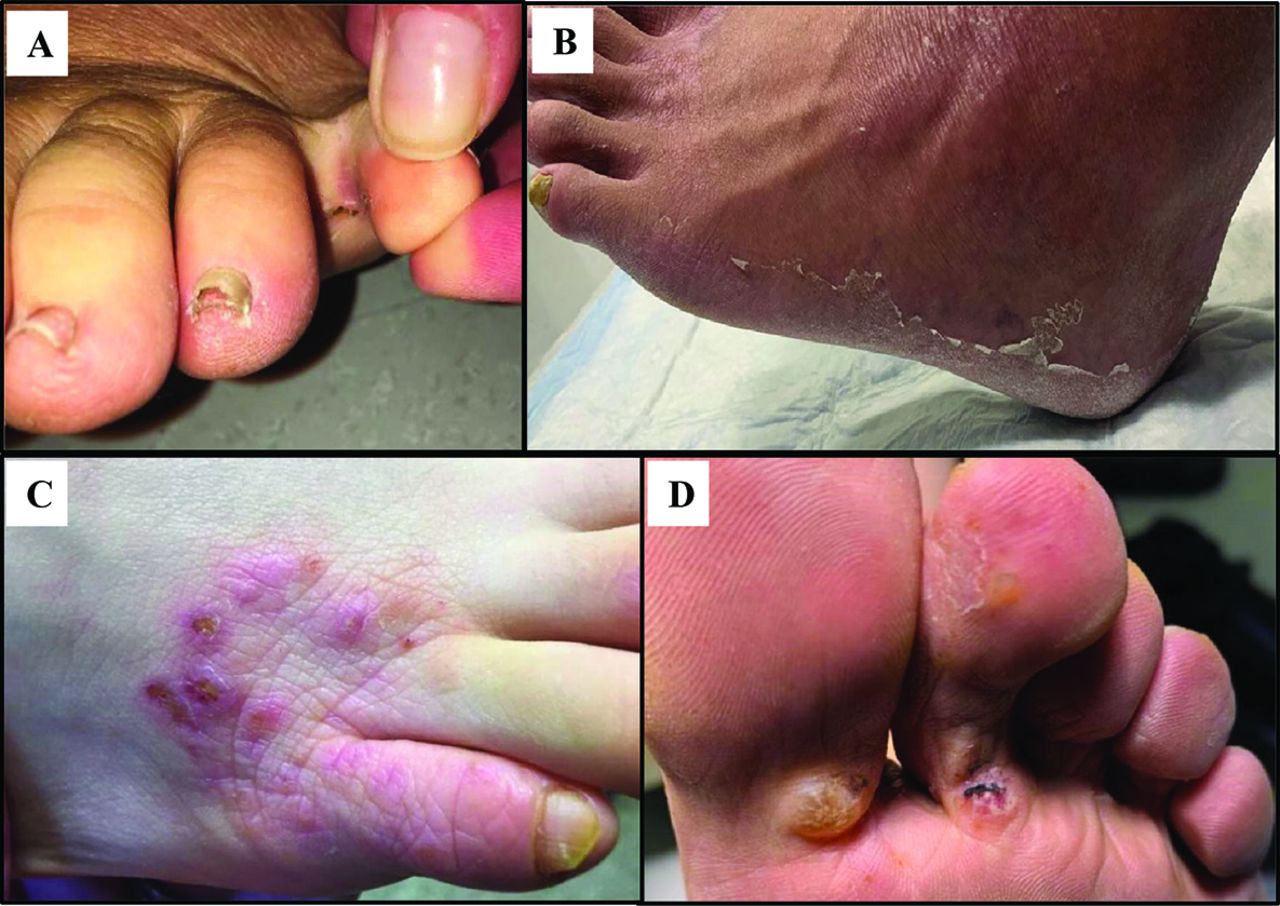
- Figure 1.
Tinea Pedis and Bullous Tinea. Tinea pedis often affects the webspace between toes 4 and 5 (A) and can present in a “moccasin distribution” characterized by superficial, desquamative scaling over the soles and lateral foot (B). Tinea incognito (C) is characterized by decreased itch and elimination of overlying scale that occurs after use of topical steroids, but tinea infection persists unless treated with proper antifungal therapy. Bullous tinea (D) characteristically develops as large superficial bullae over the in-step area.
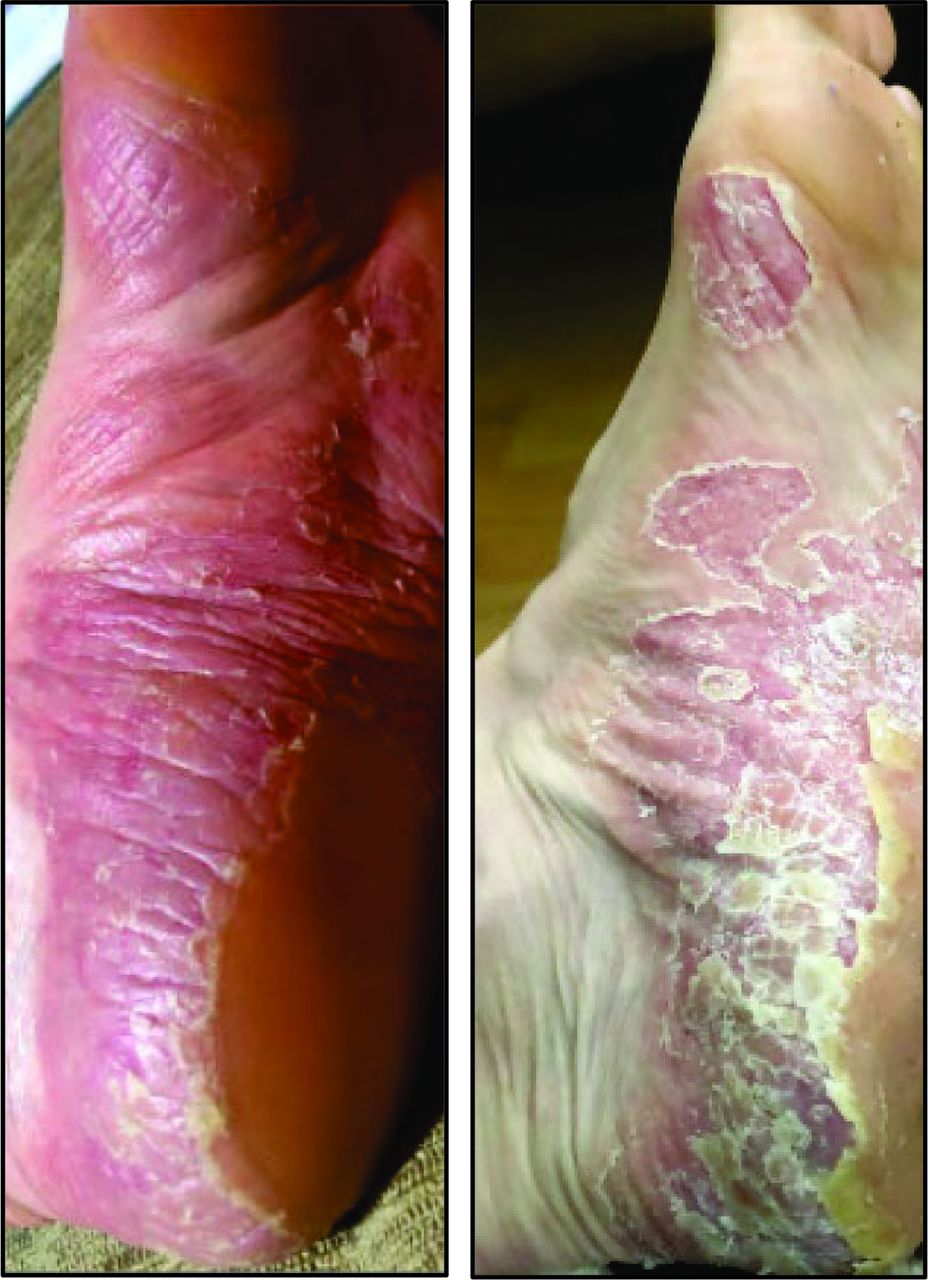
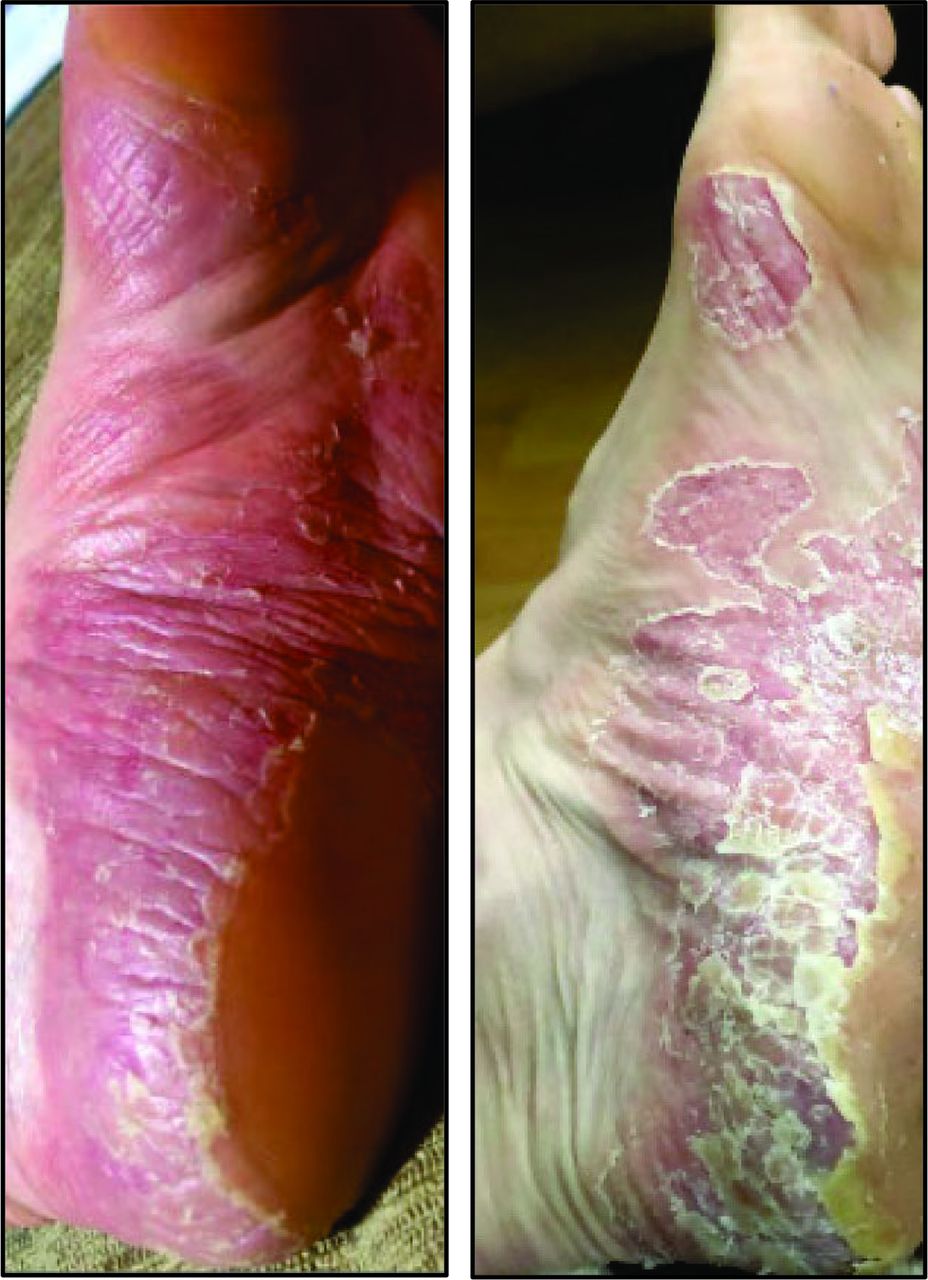
- Figure 2.
Psoriasis Vulgaris. Psoriasis vulgaris cases of the plantar feet often present with thick overlying scale and deep fissures. Psoriasis vulgaris may affect the plantar surfaces as well as other psoriasis-prone areas such as the umbilicus, gluteal cleft, scalp, and palms.
- Figure 3.
Allergic Contact Dermatitis. Allergic contact dermatitis (ACD) develops from immune sensitization, often after repeated exposure to the offending agent. Pictured here are hallmark manifestations of ACD, characterized as indurated pink plaques with eruption of vesicles and small bullae. The offending agent, in this case, was rubber components of this individual's shoes.
- Figure 4.
Dyshidrotic Dermatitis. Dyshidrotic dermatitis presents as crops of 1 to 2 mm deep vesicles primarily localized over the lateral and medial aspects of the soles and toes. After 2 to 3 weeks, the vesicles resolve with circular collarettes of scale and brown crust.
- Figure 5.
Juvenile Plantar Dermatosis. Juvenile plantar dermatoses present as desquamation arising at the base of the great toe with pink-red patches that have a glossy or “glazed” appearance. Hyperkeratosis and fissures will form over the weight-bearing regions. Web spaces are not classically involved.



Tables
Diagnosis Clinical Features Ancillary Tests Initial Therapy Tinea Pedis Onset: 31 to 60 years of age
Distribution: Asymmetrical, 4th–5th web space; in-step or “moccasin distribution”
Morphology: Fissuring, maceration, herpetiform vesicles, pustules, and bullae with pink base
Symptoms: Itch, pain, burning
Clinical clues: Concurrent onychomycosisKOH Preparation or fungal culture Topical:
First-line: Terbinafine 1% cream, butenafine 1% cream, naftifine 1% cream
Other: econazole 1% cream
Oral: terbinafine 250 mg dailyErythrasma Onset: Increased prevalence with age
Distribution: Often involves web spaces of 3rd–5th toes
Morphology: Well-marginated pink, brown patches
Symptoms: Asymptomatic or mild itchIllumination with Wood's lamp reveals coral-red fluorescence Topical:
Clindamycin solution, erythromycin gel, or benzoyl peroxide wash
Oral:Clindamycin, macrolides, or tetracyclinesPsoriasis (plaque vs. pustular) Plaque:
Onset: Late teens or 55 to 60 years of age
Distribution: Bilateral, symmetric, dorsal, or plantar feet.
Morphology: Well-demarcated pink scaly plaques
Symptoms: Asymptomatic or painful itch
Pustular:
Onset: 45 to 65 years of age
Distribution: widespread or limited to palms and soles
Morphology: Sterile pustules on an erythematous background, fissures
Symptoms: Pain, burning, itch
Other clues: Nail pitting or distal onycholysis;
Pink plaques on the scalp, umbilicus, gluteal cleft, elbows/kneesClinical diagnosis in most cases
Consider biopsy, though it may not be diagnosticTopical: Mid- to high-potency topical steroids, topical vitamin D analogs (eg, calcipotriene)
Systemic: Methotrexate, cyclosporine, acitretin, biologic agents
Other: PhototherapyContact Dermatitis
Allergic (ACD)
Irritant (ICD)Allergic Contact Dermatitis (ACD):
Onset: 8 to 28 days post-exposure
Distribution: Symmetrical or asymmetrical, geometric
Morphology:
Acute: oozing/weeping pink papules, vesicles, and plaques
Chronic: dry scaling and fissuring
Symptoms: Itch
Irritant Contact Dermatitis (ICD):
Onset: Minutes to hours
Distribution: geometric
Morphology:
Acute: red indurated plaques, vesicles, ulcers
Chronic: dry scaling and fissures
Symptoms: Pain and burningPatch testing (definitive diagnosis for ACD) Thorough removal of the irritant (for ICD)
Avoidance of allergens and irritants
Hypoallergenic fragrance-free soaps and emollients
Mid- to high-potency topical steroidsDyshidrotic Dermatitis Onset: Recurrent crops in summer and winter
Distribution: Symmetrical on the in-step and lateral toes
Morphology: 1-mm to 2–mm deep vesicles; “tapioca-like.” Resolution with halo-shaped desquamation and brown circular crusts
Symptoms: Severe itchClinical diagnosis Avoidance of harsh soaps and irritants
Liberal use of hypoallergenic emollients
Mid to high-potency topical steroidsJuvenile Plantar Dermatosis (JPD) Onset: Young, school-aged children
Distribution: Originating from the base of the big toe, sparing web spaces
Morphology: Redness, fissures, scaling, “glazed donut” appearance
Symptoms: ItchClinical diagnosis Avoid occlusive footwear and change socks frequently
Thick, bland emollients
Mid- to high-potency topical steroidsAbbreviations: ACD, Allergic contact dermatitis; CD, contact dermatitis; DD, dyshidrotic dermatitis; ICD, irritant contact dermatitis; JPD, juvenile plantar dermatosis; KOH, potassium hydroxide; PD, plantar dermatoses; PPP, palmoplantar psoriasis.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}