
Abstract
Plantar dermatoses (PD) are common, occurring either spontaneously on healthy skin or developing secondarily from previously established foot disease. PD share similar symptoms and morphology, making them challenging to differentiate. A few of the most frequently encountered PD include tinea pedis, psoriasis, contact dermatitis, dyshidrotic dermatitis (or recurrent vesicular palmoplantar dermatitis), and juvenile plantar dermatosis. This review offers practical advice for diagnosing and treating the most common PD in the primary care office.
Introduction
Inflammatory skin conditions frequently affect the plantar feet (ie, plantar dermatoses [PD]), often first presenting in primary care clinics. While most PDs are a mild nuisance, severe forms cause substantial morbidity with reduced mobility, physical discomfort, and employment limitations, leading to a demonstrable reduction in quality-of-life measures.1⇓⇓–4 PD pose diagnostic and treatment challenges as eruptions may share similar clinical features yet require distinct treatments (Table 1). As they are likely the principal point of contact for affected patients, primary care providers play a pivotal role in the diagnosis and management of PD. In this review, we discuss diagnostic symptoms, therapeutics, and indications for referral for the most common PD.
Common Plantar Dermatoses
Tinea Pedis
Clinical Features
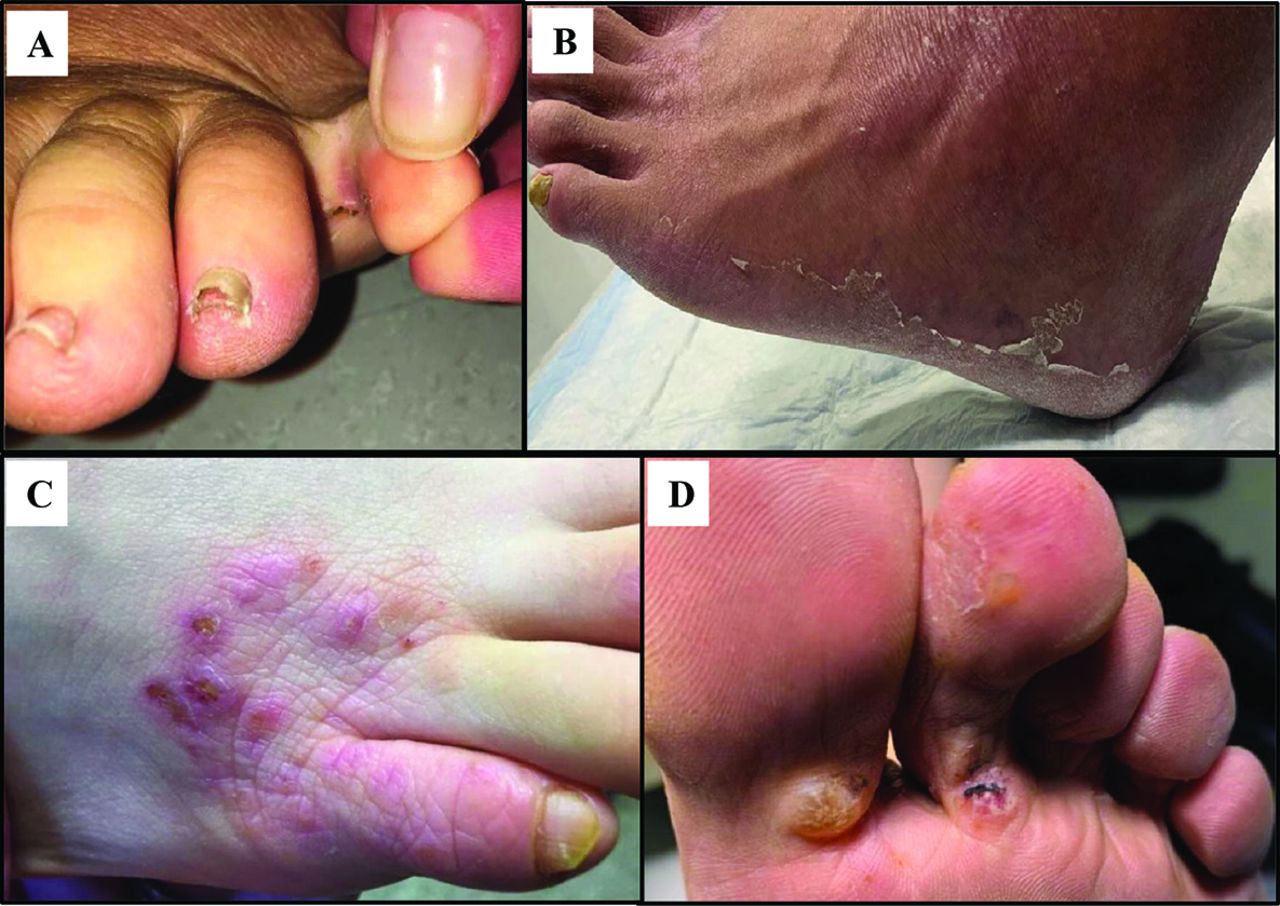
Tinea pedis (Figure 1), or “athlete's foot,” is the most common plantar dermatosis affecting nearly 3% of adults.5 Tinea pedis is most prevalent in males aged 31 to 60 years and is acquired through direct contact with dermatophytes that are often transferred in sites, such as bathrooms, gyms, and swimming pool areas, and flourish in the warm damp environments created by occlusive footwear.6
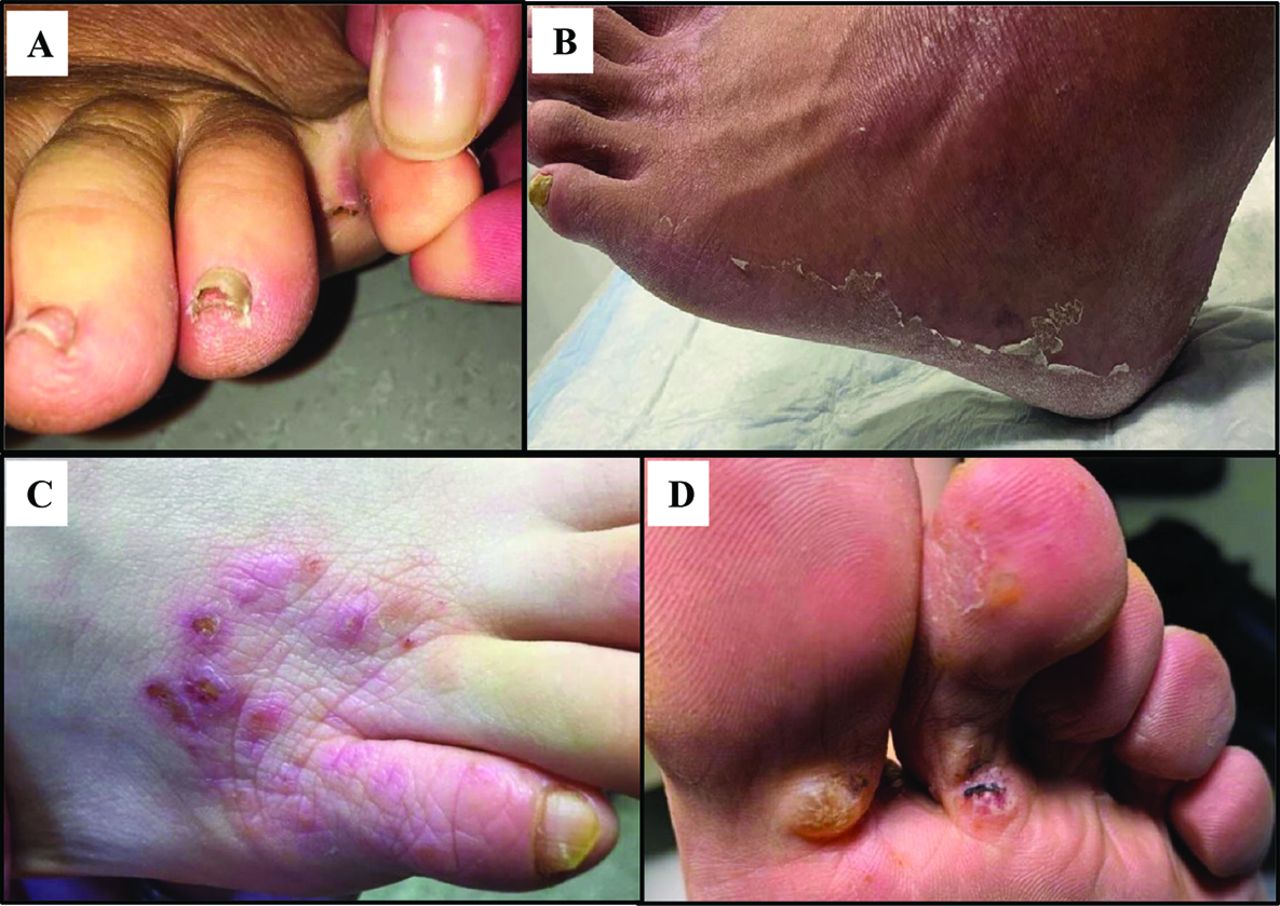
Tinea Pedis and Bullous Tinea. Tinea pedis often affects the webspace between toes 4 and 5 (A) and can present in a “moccasin distribution” characterized by superficial, desquamative scaling over the soles and lateral foot (B). Tinea incognito (C) is characterized by decreased itch and elimination of overlying scale that occurs after use of topical steroids, but tinea infection persists unless treated with proper antifungal therapy. Bullous tinea (D) characteristically develops as large superficial bullae over the in-step area.
Itching and burning are typical symptoms. Skin maceration, peeling, and white scale is often asymmetrical in distribution. The interdigital subtype is most common, favoring web spaces of the fourth and fifth toes. Conversely, a “moccasin distribution” presents with superficial, desquamative scaling (or fine and powdery) diffusely over the soles and lateral feet. The leading edge of the eruption may be slightly raised and annular or arcuate. With bullous tinea, tense vesicles, bullae, and/or pustules favor the instep. Sometimes, bullous tinea may seem purpuric, mimicking vasculitis.5 Onychomycosis often co-occurs with tinea and may be a diagnostic clue.
Erythrasma (corynebacterial infection) is a clinical mimic of tinea with maceration in the web spaces, but illumination with a Wood's lamp (365 nm) reveals the characteristic coral-red fluorescence of Corynebacteria.
Testing
Skin scraping with potassium hydroxide (KOH) provides a definitive diagnosis. If unavailable, a fungal culture should be collected by scraping the leading edge of the scale into a sterile container. Pathogenic species include Trichophyton and Epidermophyton. Feet often harbor soil contaminants, so the growth of molds does not indicate infection.
Therapy
Topical terbinafine 1% cream (or other allylamine antifungals including butenafine and naftifine) are effective first-line fungicidal agents.7 Topical azoles like econazole may be considered. In severe cases or with concurrent onychomycosis, oral terbinafine is preferred.
Additional Considerations
Tinea is exceptionally common and mimics many of the other PD. It should always be excluded as a cause of foot rash before initiating therapy.
Dermatitis may improve with topical antifungals due to their moisturizing and anti-inflammatory properties. Tinea pedis is often challenging to control and may recur after cessation of therapy; however, dermatitis should be considered in recurrent rashes, particularly those with a negative KOH scraping and/or fungal culture.
Initial improvement with the use of a topical steroid does not exclude tinea. Topical steroids may decrease itch and eliminate overlying scale, producing “tinea incognita.”
Psoriasis
Clinical Features
Plaque and pustular psoriasis may preferentially target the feet.4,8,9 Many patients experience itch and severe pain from fissuring. Psoriasis has a bimodal age distribution, presenting in the late teens or between ages 55 to 60 years.10 Psoriasis should not be overlooked as a cause of PD in children.
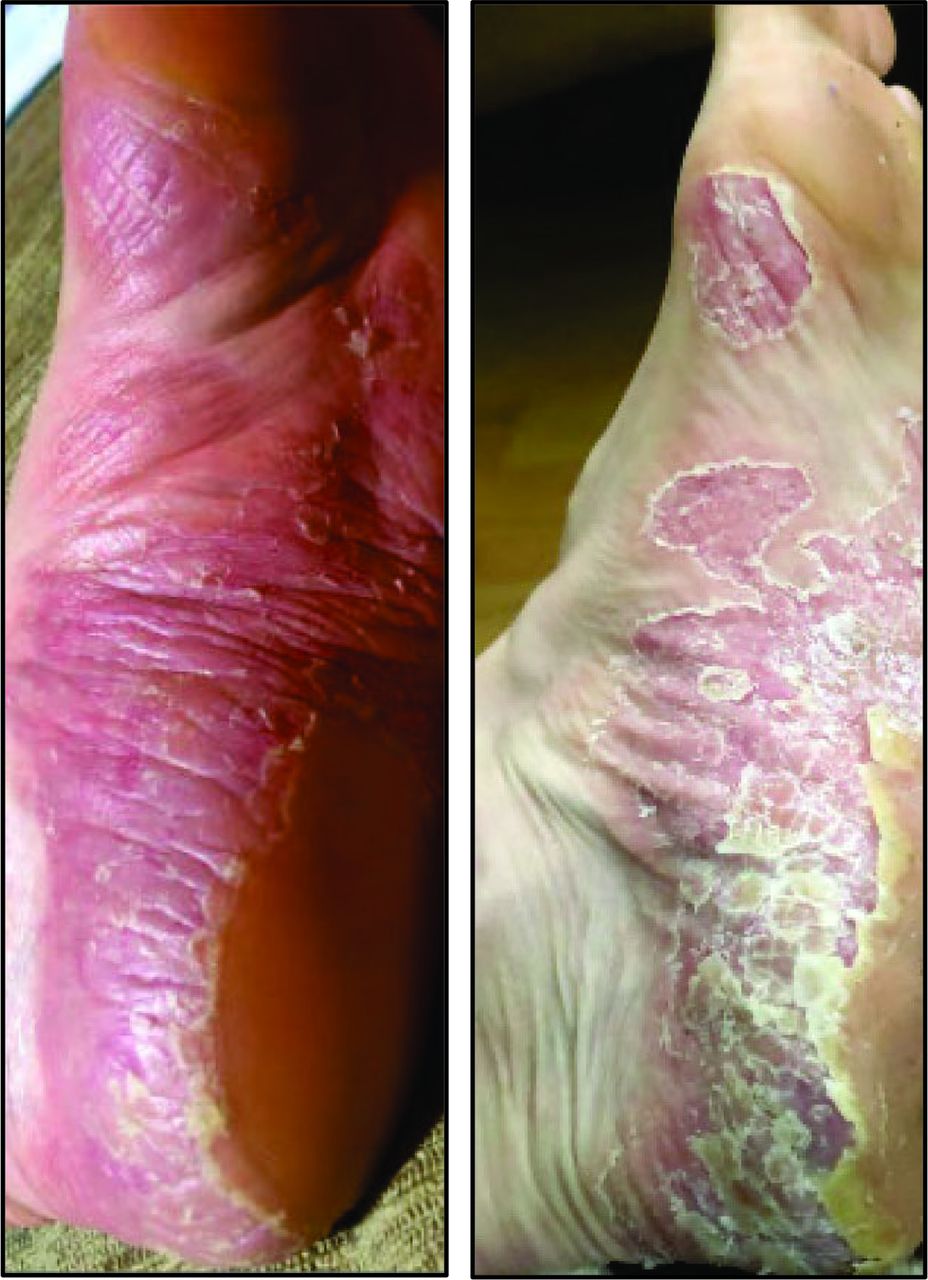
Palmoplantar psoriasis (PPP) classically presents as bilateral, symmetrical red-pink plaques with sharp borders. As shown in Figure 2, plaques extend up the lateral or medial aspects of the feet and may involve the dorsal foot or toes. The overlying scale can be thick with deep fissures.8
Palmoplantar pustular psoriasis is a rare variant in which sterile pustules form over the palms and soles.4
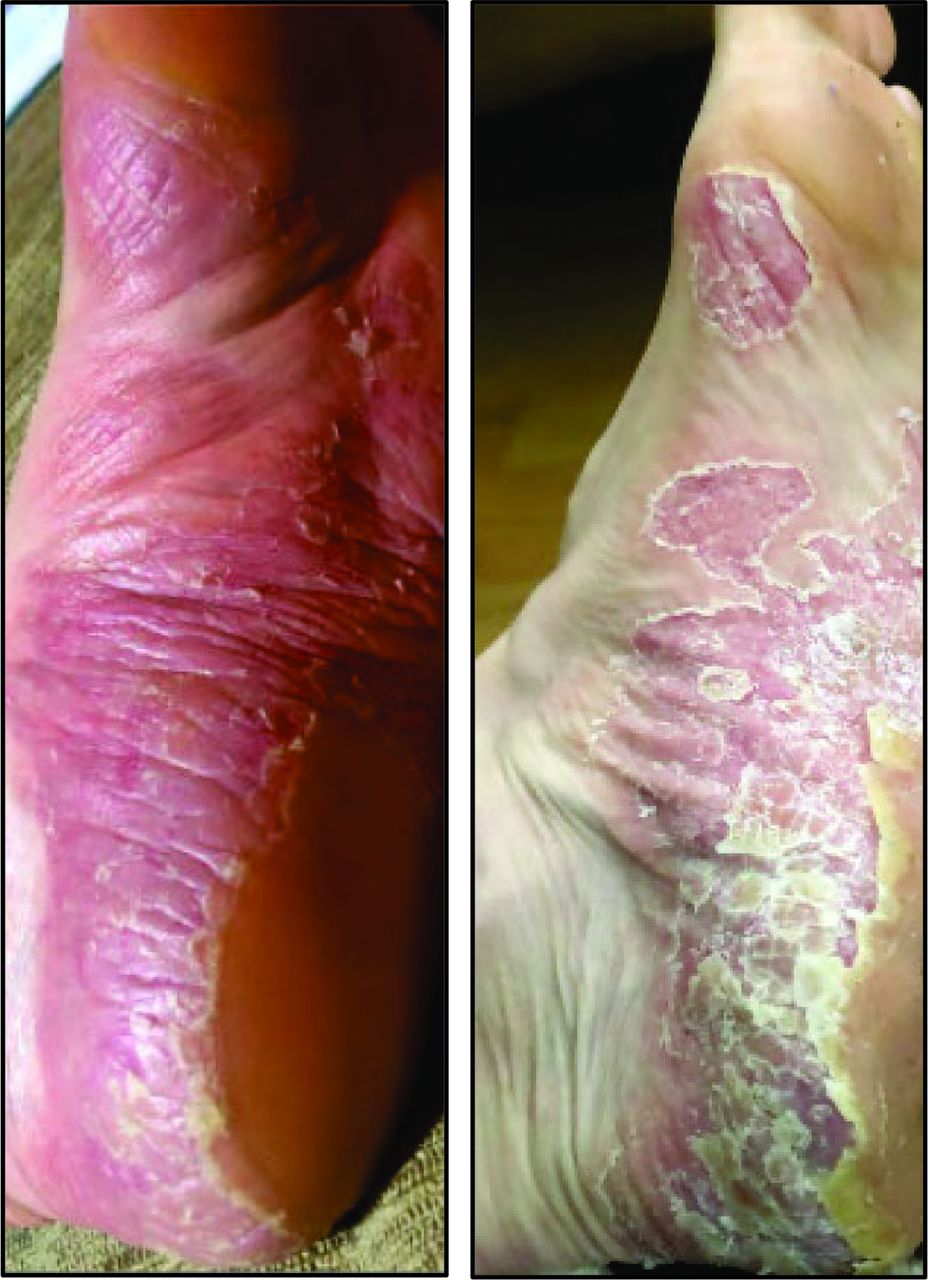
Psoriasis Vulgaris. Psoriasis vulgaris cases of the plantar feet often present with thick overlying scale and deep fissures. Psoriasis vulgaris may affect the plantar surfaces as well as other psoriasis-prone areas such as the umbilicus, gluteal cleft, scalp, and palms.
Features favoring PPP over dermatitis or tinea include the presence of scaling plaques in other psoriasis-prone areas (eg, umbilicus, gluteal cleft, scalp, palms) and psoriatic nail changes (eg, pitting, distal onycholysis).11 Itch is more typical of dermatitis and tinea than of psoriasis, but this is not universal. Oozing of the skin with serous drainage and/or secondary infection would suggest dermatitis over psoriasis.9
Patients often self-treat with over-the-counter agents before presenting to the clinic. If adequate topical antifungal agents have been tried and failed, tinea is an unlikely diagnosis.
Testing
Tinea must first be excluded. Skin biopsies have limited use as PPP and dermatitis exhibit histologic similarities that can be challenging to distinguish.12 Initial treatment options for plantar dermatitis and psoriasis are similar; therefore, additional testing may be reserved for patients unresponsive to topical corticosteroids.
Therapy
High-potent to ultrapotent topical steroids (eg, augmented betamethasone (often the most cost-effective), clobetasol, or halobetasol) are the first-line treatment for PPP, as thicker acral sites are often unresponsive to lower-potency formulations.12⇓–14 Topical vitamin D analogs (eg, calcipotriene) and topical retinoids (eg, tretinoin, tazarotene) are useful adjuncts.15 The application of medications on damp skin (“soak and smear”) or under occlusion with damp socks or plastic wrap can greatly enhance penetration.
Consider dermatology referral in cases refractory to topical therapies. Second-line treatments include phototherapy and systemic retinoids. In recalcitrant cases or in those with concurrent psoriatic arthritis, systemic immunomodulators (eg, methotrexate, cyclosporine) and injectable biologic agents are utilized.4,14⇓–16
Contact Dermatitis
Clinical Features
Contact dermatitis arises from skin irritation or allergy.17 Allergic contact dermatitis (ACD) and irritant contact dermatitis (ICD) are estimated to affect 4% of the United States population.18 ICD is more prevalent, accounting for 80% of all occupational-related CD compared with 20% for ACD.19 Aging populations and atopic individuals are at risk of ICD (and ACD with atopy) due to skin barrier dysfunction.19
Direct chemical irritation induces ICD. ACD results from immune sensitization following allergen-skin contact, reproducible with subsequent skin exposure. ACD develops 8 to 28 days after initial exposure, which complicates the identification of the allergen.20 Repetitive exposure may trigger immune sensitization at any time.21⇓–23 Common foot allergens include shoe materials (eg, rubber accelerators, dyes, adhesives, metals of buckles/decoration).16 Over-the-counter topical medications (eg, antibiotics, antifungals, steroids) all may provoke ACD.17
Well-demarcated, geometric lesions are present in acute ACD and ICD. In acute ICD, skin redness and edema localizes to the exposed area within minutes to hours. Necrotic ulcers may form in severe ICD, but not ACD.19 ICD management includes removal of the irritant and standard wound care (eg, gentle cleansing, application of bland emollient ointment, covering to prevent infection).
Acute ACD presents with delayed onset of indurated pink plaques over areas of contact (Figure 3). In severe cases, vesiculation and bullae are present. Itch is the primary symptom of ACD, whereas burning and pain are more likely with ICD.19

Allergic Contact Dermatitis. Allergic contact dermatitis (ACD) develops from immune sensitization, often after repeated exposure to the offending agent. Pictured here are hallmark manifestations of ACD, characterized as indurated pink plaques with eruption of vesicles and small bullae. The offending agent, in this case, was rubber components of this individual's shoes.
Chronic forms of ACD and ICD are difficult to differentiate, both presenting with itching pink plaques, xerosis, and fissuring. A detailed exposure history may help to discern these entities.19
Testing
In chronic, recurrent, or recalcitrant cases, dermatology referral for patch testing is encouraged.23,24 Patch testing identifies cutaneous delayed hypersensitivity reactions.
Treatment
Exposures as infrequent as monthly can perpetuate ACD; therefore, assessing all potential allergens is critical. Skin eruptions may align with shoe components (eg, straps from sandals, hardware, glued seams). Yellow crusting and oozing indicate a secondary bacterial infection which should be treated with topical or oral antibiotics in conjunction with mid- to high-potent topical steroids to minimize inflammation.
Patients with sweat-induced ICD are encouraged to wear moisture-wicking socks and avoid occlusive shoes.19 Consistent use of hypoallergenic emollients aid in skin barrier enhancement.
Dyshidrotic Dermatitis
Clinical Features
Dyshidrotic dermatitis (DD) may develop as early as preschool and is commonly provoked by cold, dry weather.25 Crops of 1 to 2 mm “tapioca-like” deep vesicles erupt on the lateral and medial aspects of the soles and toes (Figure 4). Vesicles resolve over 2 to 3 weeks with circular collarettes of scale and brown crust. Frequently, the palms and lateral aspect of fingers are also involved. Despite severe itch, the base of the lesions is not erythematous.25⇓–27

Dyshidrotic Dermatitis. Dyshidrotic dermatitis presents as crops of 1 to 2 mm deep vesicles primarily localized over the lateral and medial aspects of the soles and toes. After 2 to 3 weeks, the vesicles resolve with circular collarettes of scale and brown crust.
Bullous tinea, a clinical mimic, is also seen on the in-step area, but these vesicles tend to be larger and more superficial than DD.
Juvenile Plantar Dermatosis (JPD)
Clinical Features
JPD impacts school-aged children (males>females), spontaneously resolving during early teen years. Flares occur in both summer and winter, precipitated by sweating due to hot, humid weather or occlusive boots. 28⇓–30
Initially, desquamation occurs at the base of the great toe (Figure 5), revealing pink-red patches with a glossy or “glazed” appearance that expand posteriorly along the forefoot. 28,29 Hyperkeratosis and fissures form over weight-bearing regions, allowing bacteria to infiltrate. Over time, the epidermal ridges flatten, resulting in anhidrosis.31,32 Classically, web spaces are not involved.28⇓–30 JPD is often misdiagnosed as a dermatophyte infection, which is uncommon in children.

Juvenile Plantar Dermatosis. Juvenile plantar dermatoses present as desquamation arising at the base of the great toe with pink-red patches that have a glossy or “glazed” appearance. Hyperkeratosis and fissures will form over the weight-bearing regions. Web spaces are not classically involved.
Treatment
Patients should avoid occlusive shoes and change out sweaty socks. Petrolatum-based emollients applied under socks can greatly improve symptoms. Topical steroids can alleviate inflammation and pain.28
Concluding Recommendations
PD can be effectively diagnosed and treated in the primary care clinic in most cases. Diagnostic exclusion of tinea is the most important first step in making a treatment plan because topical anti-inflammatory agents may potentiate fungal infection. Referral to dermatology should be considered when skin biopsy, patch testing, or systemic treatments are required.
Acknowledgments
Erin Warshaw, MD, MS (Minneapolis, MN), graciously provided clinical images of allergic contact dermatitis.
Notes
This article was externally peer reviewed.
Funding: No governmental or non-governmental funding was obtained or used for this study.
Conflict of interests: None.
To see this article online, please go to: http://jabfm.org/content/35/2/435.full.
- Received for publication August 3, 2020.
- Revision received August 30, 2021.
- Accepted for publication September 28, 2021.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}