
Abstract
Background: To explore how the COVID-19 pandemic has affected exercise habits, we hypothesized that participants' physical activity would have increased by at least 30 min/wk after the onset of the pandemic.
Methods: We distributed an anonymous survey to ambulatory patients at the Family Medicine Clinic, University of Kansas Medical Center to analyze changes in exercise habits and weight.
Results: Of the 500 adult patients surveyed, 382 were included. Results were stratified by demographics, including employment status before and during COVID-19. The median change in weekly exercise duration was 0.0 minutes, but the mean change was –25.7 minutes; total exercise duration decreased after the pandemic's onset (paired Wilcox signed rank test P < .001). More individuals reported participation in virtual group classes (6.3% before the pandemic vs 13.1% during the pandemic; McNemar's P < .001). Individuals with home exercise equipment before the pandemic were more likely to acquire more than were those who had none before (Chi square test P < .005). Overall, there is a significant trend in the direction of weight gain (Wilcox signed rank test P < .001).
Conclusions: Most participants decreased physical activity during the unprecedented COVID-19 pandemic, expanding our understanding of how exercise habits change during stressful life events.
- Behavioral Sciences
- COVID-19
- Cross-Sectional Studies
- Disease
- Management
- Employment
- Family Medicine
- Health Behavior
- Lifestyle
- Pandemics
- Primary Health Care
- Retrospective Studies
- Surveys and Questionnaires
Introduction
The overall health benefits of physical activity are well documented. Regular physical activity can improve sleep, upregulate the immune system, and reduce all-cause mortality.2,11,21,26 Current guidelines recommend that adults weekly perform at least 150 minutes of moderate-intensity aerobic activity, or 75 minutes vigorous-intensity aerobic activity, or an equivalent combination of moderate and vigorous intensity aerobic activity.21 The guidelines also recommend muscle-strengthening activities that involve all muscle groups at least 2 days per week.21 Since the first guidelines were released in 2008, however, only 26% of men and 19% of women reported enough activity to meet the aerobic and muscle strengthening recommendations put forth by these guidelines.21
Although exercise has health benefits, there are many perceived barriers to increasing exercise time. One barrier commonly identified in adults across multiple studies is lack of time.4,8,17,20 A 2017 systematic review found that individuals who reported lack of time were less likely to participate in physical activity.8 Greater total work hours and overtime work hours were also both negatively correlated with participation in physical activity.8
Despite many adults using their waking time working, few studies have evaluated how work affects time spent exercising. Data indicate, however, that leisure-time physical activity levels were suboptimal among all major US worker groups.5 Moreover, workers who report feeling fatigued after work are less likely to engage in leisure time physical activity.3 In workers younger than 50 years old, this decrease could be as much as 50 min/wk among workers reporting that they were “very tired” after work.3 This is especially problematic because increased occupational physical activity has been found to be paradoxically harmful to health.15
In 2020, a novel coronavirus (COVID-19) outbreak traveled worldwide, resulting in over 540,000 fatalities in the US alone.7 This outbreak triggered unprecedented changes in all aspects of life. Lawmakers in most states imposed “Stay at Home” or “Safer at Home” orders to mitigate virus spread. These orders varied among states and often included actions such as closing indoor dining and gyms, restricting business hours, and mask mandates. Some states, such as Kansas (the study location), had extreme restrictions that led to the closure of all businesses and activities unless deemed “essential.”11 This led to a shift in working behavior, causing many US Americans to begin working from home.
We assessed how the unprecedented change in the US American workforce during the COVID-19 crisis affected leisure time physical activity. With almost all fifty states issuing a “Stay at Home” or “Shelter in Place” order as well as national social distancing practices, many workers found themselves spending a significant amount of time at home. All sporting events, and other various social events were canceled in the US during the spring of 2020 due to the COVID-19 outbreak. We evaluated the impact of the COVID-19 pandemic on (1) duration of exercise in min/wk, (2) setting of physical activity, (3) acquisition of home exercise equipment, and (4) weight change.
Methods
Participants
We surveyed English-speaking adults living in the US who attended a primary care appointment in the University of Kansas Medical Center Department of Family Medicine between September 2020 through November 2020. Exclusion criteria included persons who did not primarily reside in the US between February 1 and the time of the survey as well as incarcerated individuals.
Survey Implementation
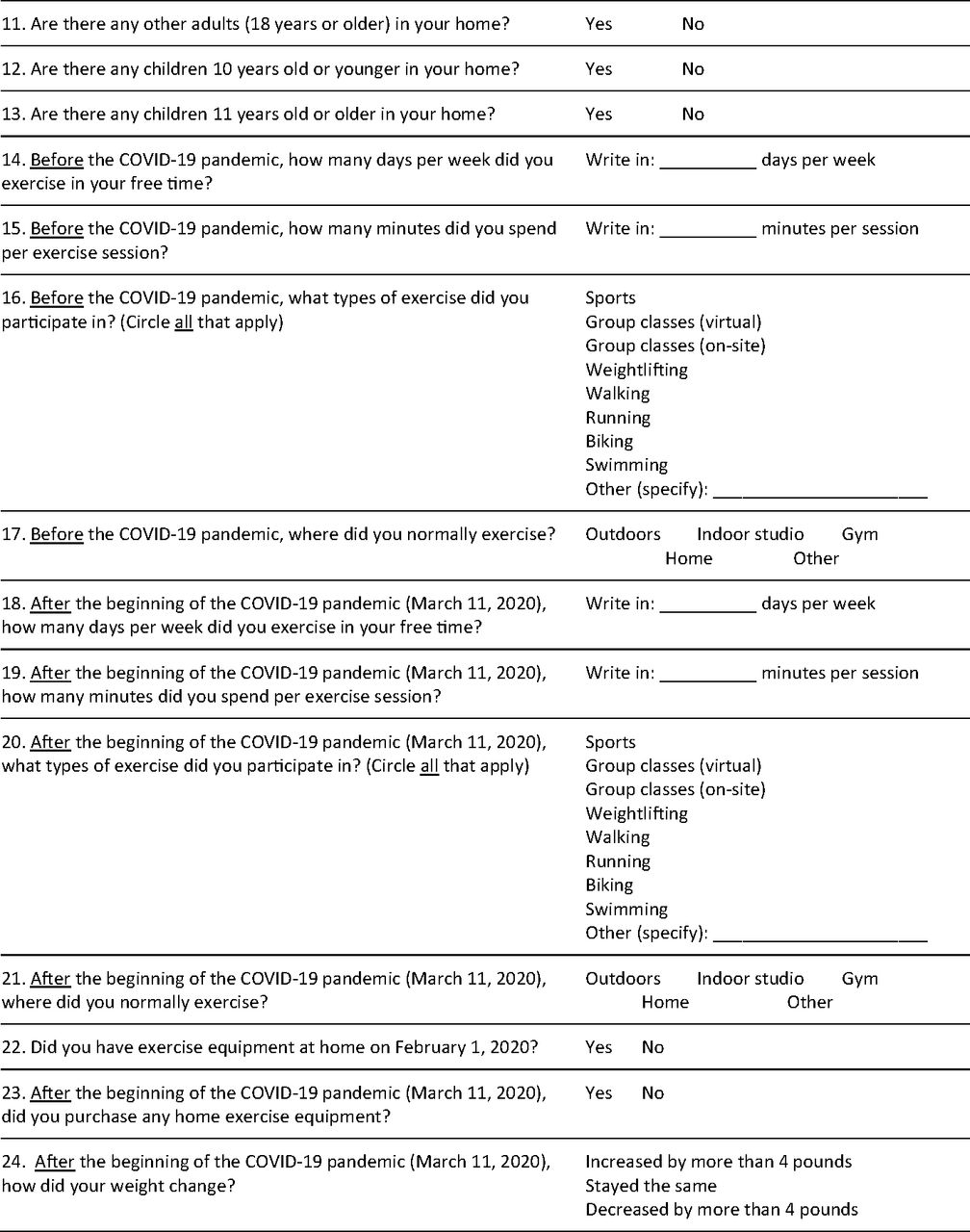
A 1-time, written, anonymous survey was distributed by front desk personnel to 500 patients (prespecified) attending ambulatory appointments and collected by a nurse when the patient was brought to an examination room. Surveys inquired about employment status, time spent exercising, type of exercise activities, location of exercise activities, and purchase of at home exercise equipment (exact formatting shown in the Appendix materials). Social and demographic information was collected, including race, gender, marital status, education attainment, and whether there were other adults or children in the home. 0.02w?>The evaluation of Leisure Time Physical Activity each week was modeled from the International Physical Activity Questionnaire12 to calculate exercise in time in min/wk and compare with goals set forth by current guidelines. Study data were collected and managed using REDCap electronic data capture tools hosted by the University of Kansas Medical Center.18,19 Written surveys were manually entered into the REDCap electronic data management system for further analysis.
Statistical Methods
Data were exported from REDCap and analyzed using R v. 3.6.1. Descriptive statistics were compiled using standard methods. Change in continuous and ordinal variables that were not normally distributed were analyzed with the Wilcoxon signed rank test (paired data) or Wilcoxon rank sum test (not paired). Proportions captured at a single point in time were compared using the Chi square test. Repeated proportions were analyzed with McNemar's test. We present unadjusted p-values throughout this article. Adjustment for multiple comparisons using the Benjamini-Hochberg procedure (which controls the false discovery rate) results in no change to the interpretation of any result. Using the more conservative Holm–Sidak procedure (which controls the familywise error rate), results only in the change in proportion of persons who exercised by running (see the Results section for details) to become nonsignificant.
Human Subjects Protection
This project was approved by the Institutional Review Board at the University of Kansas Medical Center.
Results
Characteristics of the sample are shown in Table 1. Of the 500 adult patient surveys collected, 382 were included after complete case analysis. Surveys that were improperly filled out were excluded in the final analysis. Respondents were widely distributed in age (median = 36 years; range = 18–74 years), sex, race, ethnicity, and educational attainment. Respondents were most commonly female (64.9%), White (65.7%), non-Hispanic (88%), college-educated (38%), single (41.6%) or married (40.8%), and residing without children (63.9%). Before the beginning of the pandemic, most participants were employed and worked away from home (56.8%); this proportion declined during the pandemic to 34.6%. Over the same period, the proportion of the population who was employed and working from home rose from 10.7% to 27%. Similarly, persons with a hybrid work setting (both at and away from home) rose from 9.4% to 13.1%.
Sample Demographics, Exercise Session Days/Wk, Session Duration, and Total Exercise Min/Wk
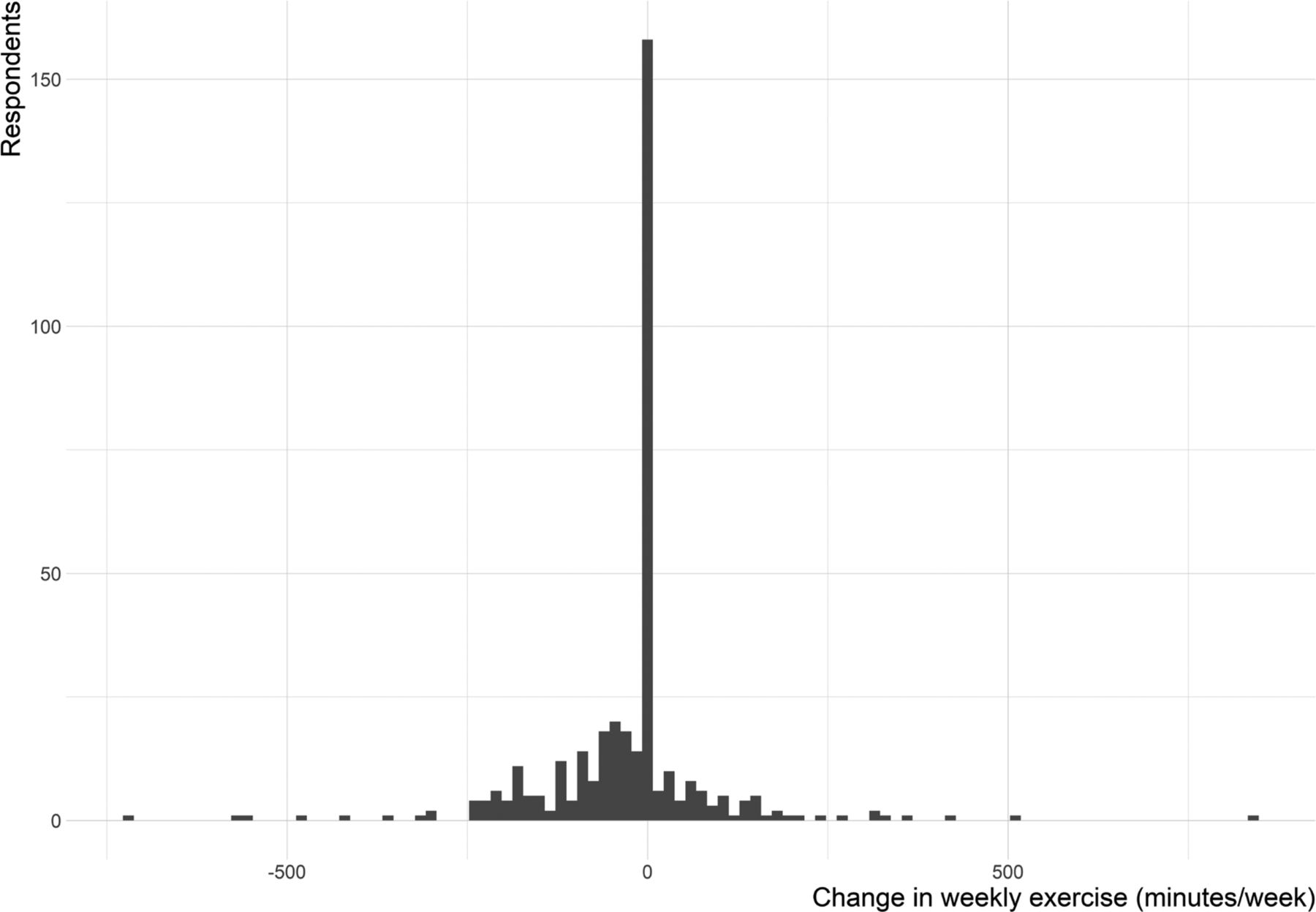
First, we evaluated the change in weekly total duration of exercise (Table 1). This distribution exhibited left skew (Appendix Figure 1): The median change in weekly exercise duration showed no change (0.0 min/wk), but the mean change was –25.7 min/wk. Across all participants, total duration of exercise was decreased after the onset of the pandemic (paired Wilcox signed rank test P < .001).
Next, we evaluated the proportion of individuals reporting exercising >150 min/wk, as recommended by the Physical Activity Guidelines for Americans. Before the pandemic, 157 of 382 (41.1%) persons met this guideline. During the pandemic, only 119 of 382 (31.1%) persons reported exercising >150 min/wk. Many individuals meeting the threshold before the pandemic fell short of meeting the threshold during the pandemic (63 of 157, 40.1%). Meanwhile, only 25 of the 225 (11.1%) of individuals not meeting the threshold started meeting the threshold during the pandemic. Significantly fewer individuals therefore met this guideline during the pandemic as compared with before the pandemic (McNemar's test P < .001).
We then evaluated the number and duration of weekly exercise sessions before and during the pandemic (Table 1 and Appendix Figure 2). The median interquartile range (IQR) exercise session duration before the pandemic was 36.2 minutes (20.0 to 60.0) as compared with 30.0 minutes (10.0 to 45.0) during the pandemic (paired Wilcox signed rank test P < .001). Likewise, the median (IQR) number of days exercised before the pandemic was 3 (2 to 4) days per week, while during the pandemic it was 2.5 (1 to 4) days per week (paired Wilcox signed rank test P < .001).
We next evaluated acquisition of home exercise equipment. Before the pandemic, 170 of 382 (44.5%) had home exercise equipment. Interestingly, only 90 of 382 (23.6%) purchased home exercise equipment, including 52 of the 170 (30.6%) of those who already had home equipment and only 38 of the 212 (17.9%) who lacked such equipment before the pandemic. Individuals who already had home exercise equipment before the pandemic were therefore more likely to acquire more equipment than those who had none to begin with (Chi square test P = .005).
Significant differences were found in the setting of exercise activity (Table 2). Individuals reported decreased participation in sports, on-site group classes, weightlifting, running and swimming (McNemar's P values shown in Table 2). In contrast, a greater proportion of individuals reported participation in virtual group classes (6.3% before the pandemic vs 13.1% during the pandemic; McNemar's P < .001).
Exercise Setting Before and During the Pandemic
We then evaluated changes in weight. The plurality (162 of 382, 42.4%) of respondents reported no change in their weight (Table 3). Among those with a weight change more than 4 lb, more individuals reported weight gain (148 of 382, 38.7%) than did weight loss (72 of 382, 18.8%). Overall, this represents a significant trend in the direction of weight gain (Wilcox signed rank test P < .001).
Self-Reported Change in Weight Stratified by Demographic Variables
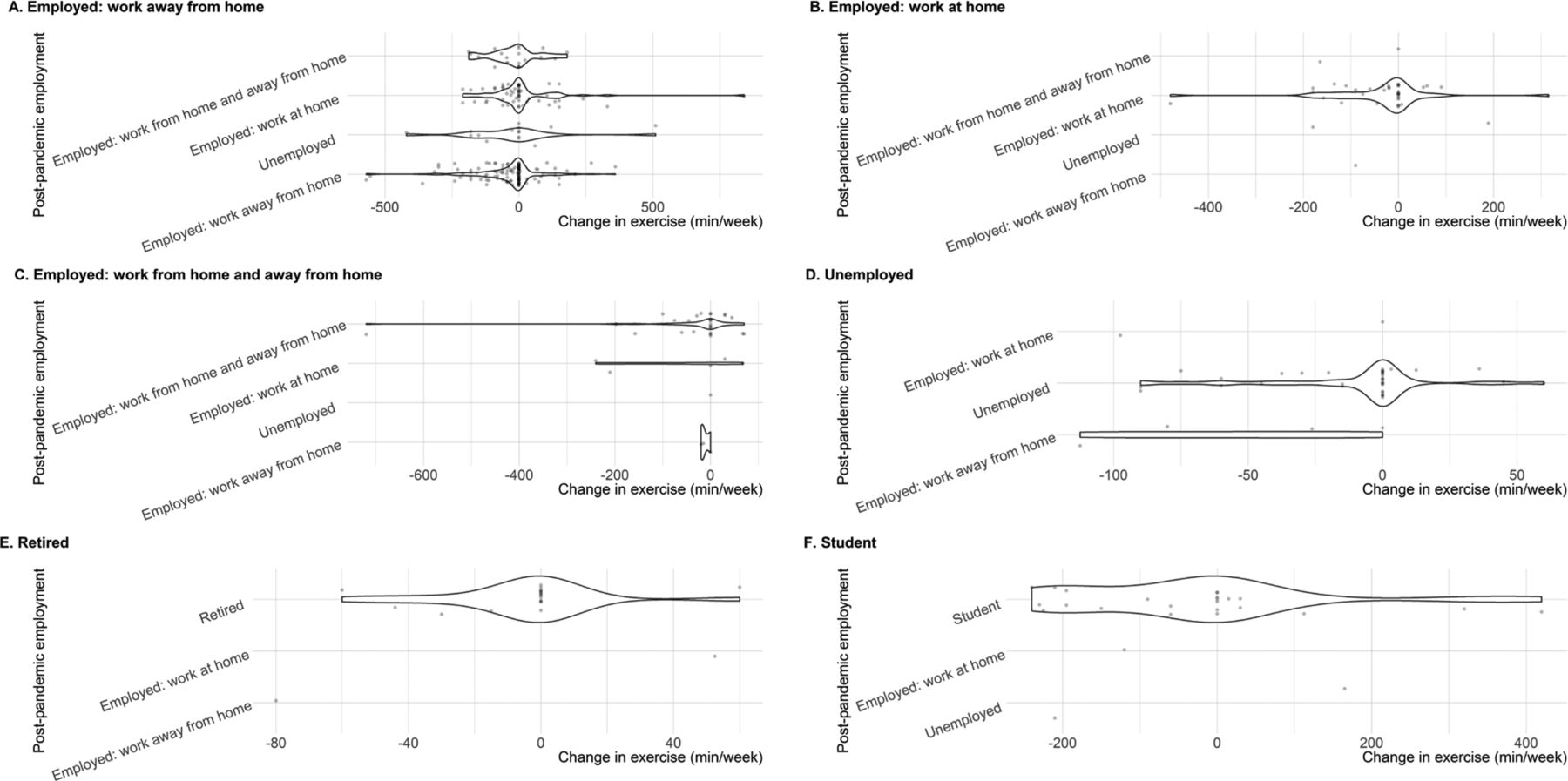
Finally, we evaluated whether change in employment setting was associated with change in either (1) total weekly exercise duration (Table 4) or (2) weight (Table 5). Among persons who worked away from home before the pandemic (n = 217), we failed to detect a difference in change in weekly exercise (Wilcoxon rank sum P = .141) or change in weight (Wilcoxon rank sum P = .974) among persons who continued to work away from home after the pandemic (n = 123) versus those who did not (n = 94, including work at home setting, hybrid work away and at home setting and unemployed persons). Similarly, we failed to detect an association between change in total weekly exercise duration (Wilcoxon rank sum P = .946) or weight (Wilcoxon rank sum P = .085) among persons who were employed before the pandemic (n = 294), stratified by whether they remained employed (n = 276) or became unemployed (n = 18).
Employment Status Before and During the Pandemic and Change in Total Weekly Exercise
Self-Reported Change in Weight Stratified by Before and During Pandemic Employment Status
Discussion
The aim of this study was to investigate the changes in exercise habits in the US workforce during the “Stay at Home” order of the COVID-19 outbreak in the US. This study did not find any significant change in total weekly exercise duration when stratified by change in employment status. However, across all participants, total duration of exercise was decreased after the onset of the pandemic. This finding is consistent with a similar study on the change of exercise habits during COVID-19 confinement.1 This large international study (n = 1047) found a negative impact on physical activity on all levels of intensity and a 33.5% decrease in overall weekly physical activity.1 This same international study also found that food consumption and meal patterns (the type of food, eating out of control, snacks between meals, number of main meals) were unhealthier during confinement.1 This could explain in part why 38.7% of our study participants reported weight gain during the pandemic. Our study is more applicable to the US population because the international study included only 31 participants who were included from continents other than Asia, Europe, and Africa.1
Importantly, our study found that before the onset of the pandemic, 41.1% of participants reported exercising more than 150 min/wk as recommended by the Physical Guidelines for Americans. After the onset of the pandemic this had a significant fall to 31.1% meeting this threshold. This fall in exercise participation occurred despite 23.6% of participants purchasing new home exercise equipment during the pandemic.
These findings are important in light of emerging evidence that physical activity should be promoted as a nonpharmacologic intervention to protect against 2019 novel coronavirus.10,16 A large study (n = 48,440) found that patients with COVID-19 who were consistently inactive were at increased risk of hospitalization, ICU admission, and death.22 Exercise-induced immunomodulation has been recognized for over 3 decades, with around 5000 peer reviewed original and review articles available in both MEDLINE and PubMed databases.16 Researchers suggest physical exercise can act as an immunomodulator by increasing pro- and anti-inflammatory cytokines such as IL-10 and IFN-β.10 Exercise also increases lymphocyte circulation and cell recruitment.10 This can lower incidence, symptom intensity, and mortality in viral infections.10 Suppression of IFN-α and IFN-β has been theorized as a possible pathology to COVID-19.10 These cytokines are especially important because they act as antivirals by influencing activities of macrophages and lymphocytes.10 There has been evidence that physical activity leads to decreased acute respiratory illness incidence, duration, and intensity of symptoms, as well as mortality.10 Heffmernan et al have suggested that exercise training could also improve immune response to COVID-19 by augmenting the ACE2-Ang1-7-Mas receptor axis to reduce pulmonary fibrosis.13 Carter et al proposed that regular physical activity, when particularly done outside, can alleviate risk factors for COVID-19 by increasing vitamin D exposure as well as decreasing adiposity.6
Another manner in which physical activity may benefit US Americans during the pandemic is through the relief of psychological stress. Studies have consistently found a relationship exists between physical inactivity and an increased risk for depression and anxiety disorders.9,14 This is specifically important in the setting of a global pandemic. Several studies and articles have been published regarding the psychological effects of the COVID-19 pandemic. A study of 1210 respondents from 194 cities in China found that 54% of respondents reported the psychological impact of the COVID 19 outbreak as moderate to severe.24 This same study also found that 29% of respondents reported moderate to severe anxiety symptoms.20 A meta-analysis of 6 studies suggests that exercise should be considered an evidence-based treatment for anxiety.23 Zhang et al found that physical activity directly alleviated general negative emotions during the COVID-19 pandemic in a cohort of 66 college students in China.25 From this study, it was found that about 108 minutes of light intensity, 80 minutes of moderate intensity, or 45 minutes of vigorous intensity exercise daily was a suitable amount of exercise to minimize negative emotions during the pandemic.25 This is why it is important for physicians to promote exercise in their patients as a preventative measure against COVID-19 induced psychological issues.
This study has limitations. Self-reported physical activity data may be over or underestimated by participants. There is also the possibility of recall bias because participants were asked to remember exercise habits from before February 2020, several months before the administration of the survey in the fall of 2020. An added bias may also be present by asking participants to evaluate their exercise habits before the pandemic and during the pandemic at the same point in time. There is possible selection bias of a healthy population by surveying patients willing to go to clinic during the COVID-19 pandemic when many delayed seeking routine medical care. Another limitation is that a nonvalidated form of the International Physical Activity Questionnaire form was used to evaluate exercise habits. A shorter version was used to maintain brevity in the survey and increase participation. Other limitations include that it was conducted at a single center and was limited to English-speaking participants. Our results are likely generalizable to patients seeing primary care at urban academic medical centers in the US; additional studies in community health centers and in rural locations are warranted.
Conclusion
In summary, the COVID-19 pandemic significantly altered exercise habits (decreasing total weekly duration of exercise, decreasing satisfaction of exercise guidelines, and changing the setting of exercise activity). These alterations occurred alongside a trend toward significant increases in weight. Although we observed large changes in employment setting—toward work-at-home and hybrid at-home/away settings—we did not find an association with postpandemic work setting and either exercise duration or weight. Our findings illuminate the exercise experience of individuals in the United States seeking primary care; this group is important because it is the group primary care physicians can intervene on to promote health outcomes. Further research to define pandemic-related changes in exercise habits of individuals in community and rural settings would be helpful. Further studies are also needed to assess strategies to maintain healthy habits during and post pandemic.
Acknowledgments
We thank the nursing and administrative staff at the University of Kansas Medical Center family medicine clinic for their assistance with distributing and collecting the survey.
Appendix.
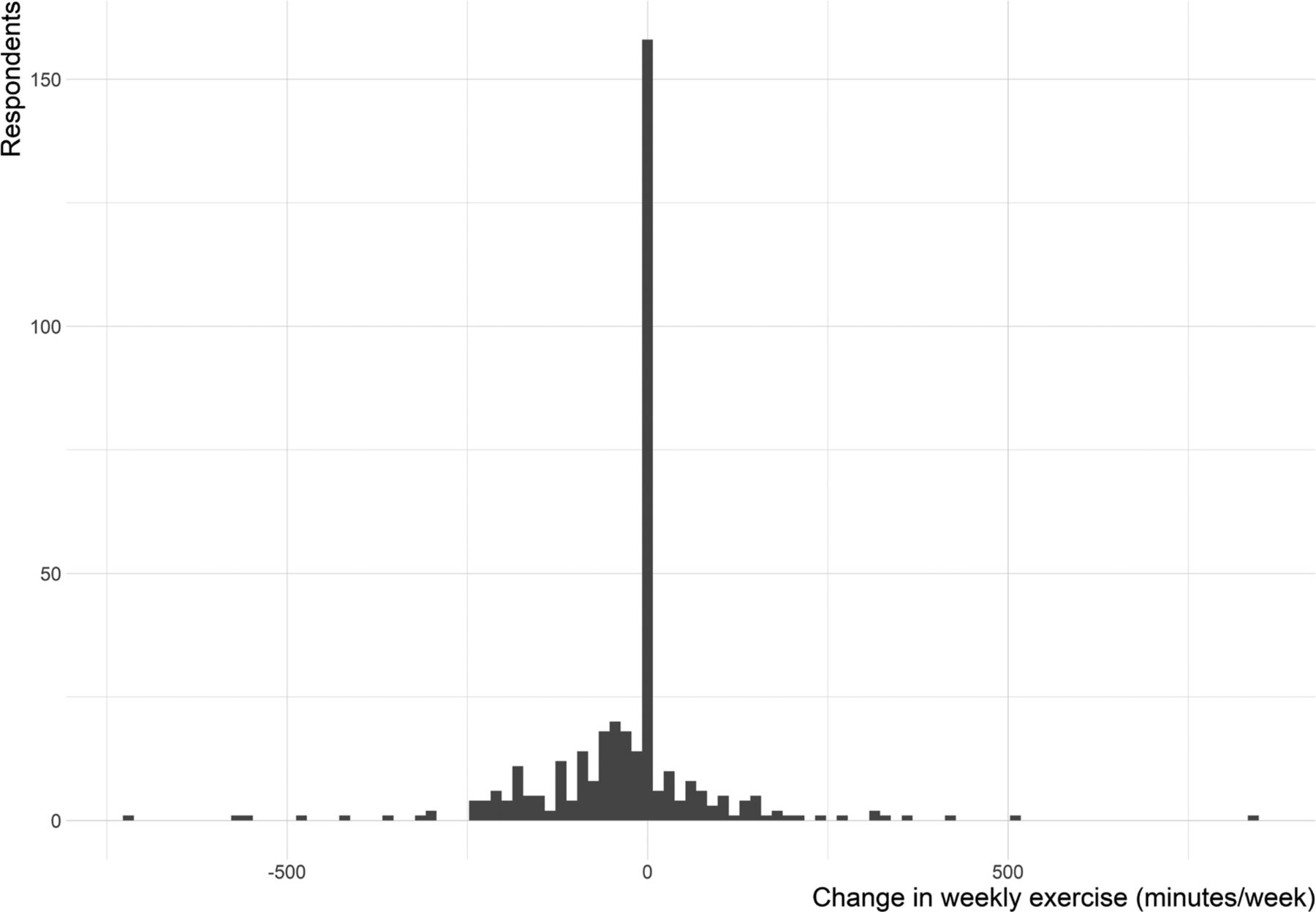
Distribution of Change in Total Minutes of Weekly Exercise Among Respondents.

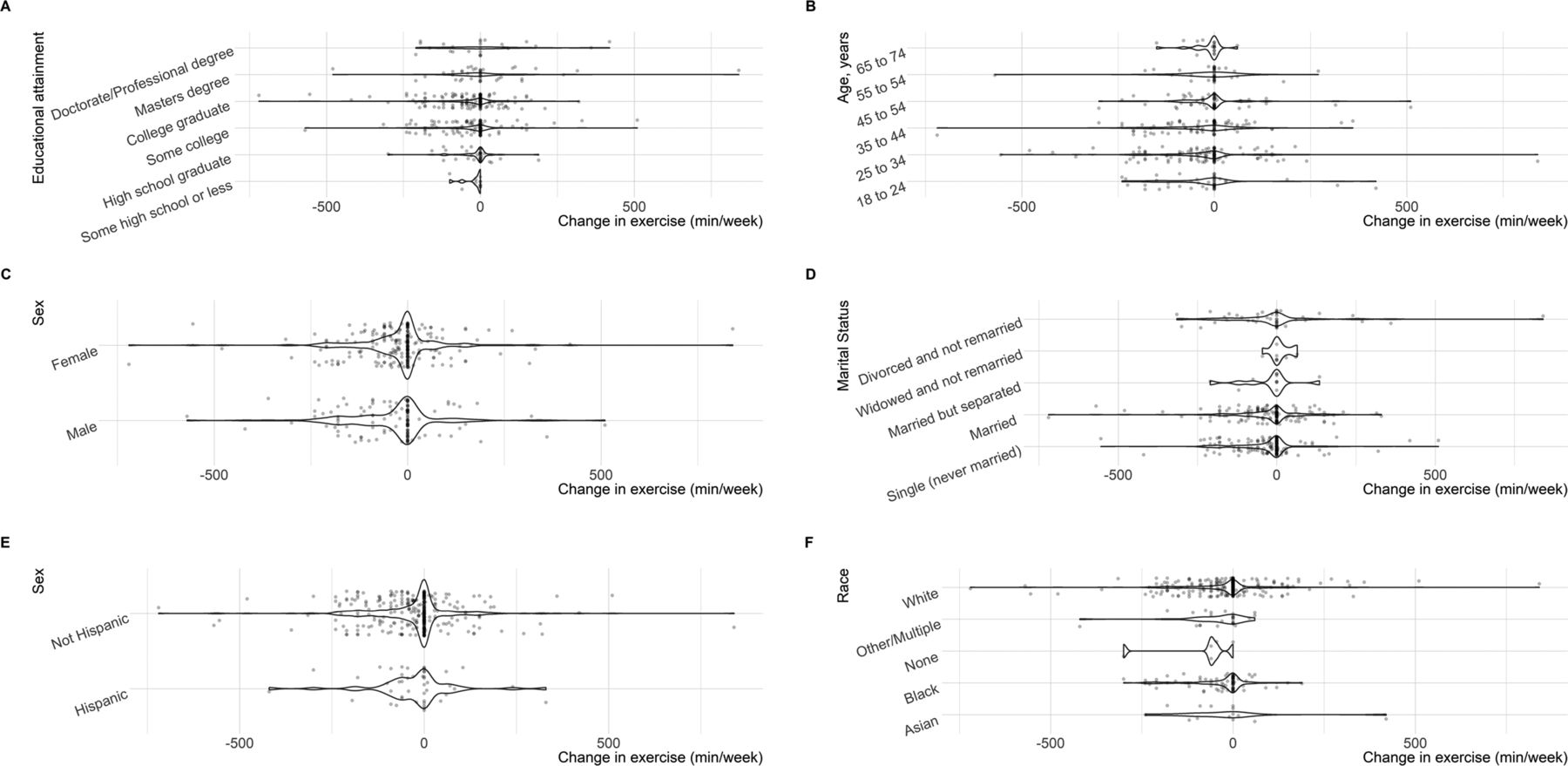
Distribution of Change in Total Weekly Exercise, Stratified by Demographic Variables.

Distribution of Change in Total Weekly Exercise, Stratified by Before the Pandemic Employment Status (Panels) and During the Pandemic Employment Status.


Research Survey About Exercise Habits Before and After the COVID-19 Pandemic.
Notes
This article was externally peer reviewed.
Funding: This work was supported in part by the University of Kansas Medical Center, who permitted the use of their REDCap electronic management data system for our data analysis.
Competing and conflicting interests: None declared.
To see this article online, please go to: http://jabfm.org/content/35/2/295.full.
- Received for publication July 21, 2021.
- Revision received October 7, 2021.
- Accepted for publication October 12, 2021.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}