
Abstract
Background: The COVID-19 pandemic has significantly impacted health care workers (HCW). Most research focused on the adverse mental health effects during the initial surge of cases; and yet little is known about approximately how workers are faring 1 year into the pandemic. The objective of this study is to examine stress, burnout, and risk perception in an academic medical system, 1 year after the start of the pandemic.
Methods: HCW across care specialties participated in online surveys in Spring 2020 and Spring 2021. The surveys included questions related to workplace stress and risk perception related to COVID-19. Correlates of stress and burnout were explored using multivariable linear regression models. Professional Quality of Life Scale (PROQOL) questions were added to the second survey.
Results: While HCW reported significantly fewer concerns about the risk of COVID-19 transmission to themselves and their families during the 2021 survey (compared with 2020), the percentage of workers who reported feeling excess stress at work or considered resigning stayed the same. One year into the pandemic, 57% of study participants met criteria for moderate or high levels of traumatic stress and 75% met criteria for moderate or high levels of burnout. As compared with participants who cared for no COVID-19 deaths, participants who cared for COVID-19 patients who died had significantly higher traumatic stress (1 to 10: Coef. = 2.7, P = .007; >10: Coef. = 6.7, P < .001) and burnout scores (1 to 10: Coef. = 2.7, P = .004; >10: Coef. = 2.6, P = .036).
Conclusion: While Although perceptions of risk declined over the course of the year, levels of stress still remained high despite high vaccination rates. Those who witnessed more COVID-19 deaths were more likely to report increased burnout and post-traumatic stress. As our nation continues to grapple with the COVID-19 pandemic and new variants emerge it is imperative to focus on recovery strategies for high burnout groups to ensure the wellbeing of our health care workforce.
- Caregivers
- COVID-19
- Critical Care
- Emergency Medicine
- Health Personnel
- Linear Models
- Mental Health
- Nurses
- Pandemics
- Perception
- Quality of Life
- Workplace
Introduction
The COVID-19 pandemic has had varying psychological effects on frontline workers. Early COVID-19 studies from China reported that the majority of health care workers (HCW) experienced increased stress, and many exhibited signs of depression due to the demands of the crisis.1 In the first months of the pandemic, the major factors leading to stress included exposure and risk of disease contraction, fear of potential transmission to loved ones, lack of information, limited resources, increased work hours, and loss of work-life balance.2 At the same time, many HCW reported being driven by altruism and purpose, which may be protective against negative mental health effects.3
Studies examining the mental wellbeing of HCW in previous epidemics, including SARS, MERS, and Ebola, similarly found elevated levels of stress due to social isolation, risk of contracting disease, and fear of loved ones becoming ill.4,5 Studies of respiratory epidemics specifically, including SARS, MERS, and numerous strains of influenza, revealed widespread anxiety, PTSD, and depression among HCW who were highly exposed to infected patients, and postepidemic psychiatric morbidity remained prominent in a subset of HCW.5,6
HCW during the COVID-19 crisis reported their frustrations with lack of treatment options, an inadequate global response, and excess mortality.7 However, many HCW join the field for the purpose of aiding in a crisis, and this altruism has been found during previous epidemics as well.8 Despite their fears and frustrations, Ebola crisis workers working 2-month deployments conveyed high levels of professional satisfaction as they experienced the gruesome realities of the disease.9 However, longer-term studies are less optimistic and suggest that this resilience wanes; 10% of HCWs experienced PTSD and many more showed clinical depression 3 years after the SARS pandemic.10,11
Few could have predicted the longevity or magnitude of the COVID-19 pandemic 1 year later.12 Many of the initial stressors, including lack of personal protective equipment (PPE), access to testing, and hospital overcrowding, have improved.12–14 With a better understanding of disease characteristics and widespread vaccination efforts, the risks of exposure and transmission have declined in many parts of the world.12–16 Although case numbers are decreasing in the United States, many frontline providers continue to witness daily suffering and death as a result of COVID-19.12–14 Recently, the Kaiser Family Foundation reported that 30% of US HCW show signs of burnout 1 year into the pandemic, suggesting that the stamina across the field may be waning.17
The longitudinal and cumulative effects of stress from the COVID-19 pandemic on HCWs remains unknown. The objective of this study was to examine HCW stress, burnout, and professional quality of life in an academic medical system, 1 year after the start of the pandemic. Our hypothesis was that both perceptions of risk and stress would decrease over the course of the year. We also hypothesized that HCWs who cared for more COVID-19 deaths would have higher levels of burnout and stress, but that the vaccine could have a protective factor.
Methods
Study Participants and Setting
This survey was conducted at The George Washington University (GWU) Hospital, a 431 bed academic medical center in urban Washington D.C. GWU Hospital's COVID-19 demographics largely paralleled those of the city; GWU Hospital treated over more than 3000 COVID-positive patients from March 2020 to April 2021. Approximately 1800 of those patients were admitted and 300 of those patients died. Our institution never experienced a surge beyond our cap with COVID-19 patients. By contrast, there were about approximately 6300 confirmed covid cases and over more than 300 lives lost in the city by Spring 2020 and about approximately 50,000 total cases and over more than 1100 lives lost by Spring 2021.18 As a quaternary care center, COVID-19 patients are also accepted as direct transfers from regional facilities for a higher level of care including extracorporeal membrane oxygenation (ECMO) evaluation and ventilator support specialization. COVID-positive patients were cohorted on isolated wards, occupying 1 medical floor and 1 to 2 15-bed intensive care units (ICU). Although there were exceptions, advanced practice providers (APP) mainly staffed the COVID ICU due to their greater familiarity with critical care, while whereas residents staffed the COVID-19 medical floor, with attending physicians supervising the respective teams.
Participants across care specialties were invited to participate in the study, including: attending physicians, residents, nurse practitioners (NP), physician assistants (PA), nurses, patient care technicians, respiratory therapists (RT), case managers, rehabilitation therapists, and other supportive personnel (eg, environmental services, food services, laboratory, pharmacy).
The first wave of the survey was fielded between March 27, 2020, and May 31, 2020, and the second wave was fielded between March 7, 2021, and April 14, 2021. There were 791 surveys completed during the first round of surveys and 359 surveys completed during the second round.
Survey Tool
The survey tool was disseminated electronically and through physical flyers with a scannable QR code. Multiple reminders were sent electronically to individuals at the institution. Participants completed the survey using an online REDCap (Vanderbilt University; Nashville, TN) data collection form. The informed consent was presented at the beginning of the survey and was required before proceeding with the survey questions. Survey responses were stored directly into REDCap, a secure, web-based application designed to support data capture for research studies.
Measures
In the Spring of 2020, HCWs were surveyed about about their perceived risk of contracting COVID-19 and workplace stress (Appendix Table 1).19 The survey was repeated with HCW at the same institution in 2021 for further analysis. Survey questions were adapted from 2 previous studies that assessed perceived risk and stress related to SARS among hospital employees in Taiwan and China.10,11 Additional survey questions were added to the survey instrument including a question about about the perception of being a hero, based on the media's frequent portrayal of HCW as heroes during the first months of the pandemic, and willingness to continue working if COVID-19 was to continue for another year.20 Participants were not required to complete the entirety of the survey. The questions were assessed on a 5-point Likert scale (strongly disagree; disagree; neutral; agree; strongly agree). In this study, we operationalize these measures as binary variables and compare agree and strongly agree to neutral, disagree, and strongly disagree to remain consistent with the previous study.19
Demographic and Professional Characteristics of Study Participants
The Professional Quality of Life Scale (PROQOL) Version 5 was also added to the survey tool. The PROQOL is a widely utilized, validated measurement tool for assessing HCW burnout and stress. It has been used in over more than 200 peer-reviewed studies of trauma across various specialties, including health care professionals, social service, clergy, firefighters, disaster responders, and many more.21 The PROQOL tool consists of 3 subscales, measuring compassion satisfaction, burnout, and secondary traumatic stress. Compassion satisfaction refers to the feelings of accomplishment that arise from caring for patients. Burnout is defined as a chronic state of exhaustion caused by excessive emotional, mental, and/or physical stress. Secondary traumatic stress refers to the phenomenon in which a caregiver develops characteristics of PTSD in response to another individual's person's trauma.21 Each of these subscales consists of 10 questions measured by 5-point Likert scales scored from 1 to 5 (never to very often). Possible points on each scale range from 10 to 50. The subscales are typically interpreted as categorical variables (low: 11 to 22, moderate: 23 to 41, and high: 42 to 50). The wording of the questions was slightly modified to assess the professional quality of life as it relates to caring for patients during the COVID-19 pandemic. As the majority of participants in the study had moderate scores on all 3 scales, these scores were also examined as continuous variables.
To understand the correlates of stress and burnout during the COVID-19 pandemic, we surveyed HCW on the following demographic and professional characteristics. Our 2 main variables of interest were COVID-19 care intensity, defined as the number of COVID-19 patients that the HCW cared for that died (no deaths, 1 to 10 deaths, more than 10 deaths), and COVID-19 vaccination. Other characteristics included in the survey were age (<30, 30 to 39, 40 to 59, 60+), sex, race/ethnicity (White, Black, Hispanic, Asian, other), and specialty (emergency medicine, critical care, surgery/anesthesia, medicine, other), and any time spent in quarantine for COVID-19 (either because of infection or exposure). We examined different positions based on the amount of time spent at the bedside: attending physician, resident/fellow, advanced practice provider (APP) including NPs and PAs, nurse/nursing assistant/respiratory therapist (RT) (categories merged due to the low number of responses from nursing assistants and RT and similar amount direct patient care), rehabilitation therapist (category separated out due to high response rate), and other.
Data Analysis
Demographic and professional characteristics of the study participants were compared across the 2 survey rounds using Chi square tests (2020 vs 2021). Risk perception and stress measures fielded during both rounds of the survey were also compared using c2 tests (2020 vs 2021). Burnout, secondary traumatic stress, and compassion satisfaction categories (low, moderate, high) were compared across COVID-19 care intensity using c2 tests (only 2021). Multivariable linear regression models were used to model the association between COVID-19 care intensity and continuous measures of burnout, secondary traumatic stress, and compassion satisfaction (measures had a fairly normal distribution) while controlling for demographic and professional characteristics of participants (only 2021). P-values less than 0.05 were considered significant. All data analyses were conducted in STATA 15.1.
Results
Demographics
About 67% of study participants were under 40 years of age, 72% were female, and about approximately 65% were white (Table 1). Compared with the 2020 survey, 2021 study participants were younger, there was a greater percentage of males, and there was less racial/ethnic diversity. A greater percentage of study participants were attending physicians and APPs. The intensity of COVID-19 care was added to the 2021 survey to assess how many deaths HCW witnessed due to COVID-19. The care intensity response options were as follows: no deaths, between 1 to 10 deaths, and greater than 10 deaths. The 2021 survey found that nearly 25% of all surveyed HCW witnessed more than 10 deaths due to COVID-19. COVID-19 care intensity was greatest among fellows/residents and APPs, providers who work in emergency medicine and critical care, and workers who received the COVID-19 vaccine (Appendix Table 2). A total of 93% of participants in the 2021 survey had received the COVID-19 vaccine.
Risk Perception and Work Stress by COVID-19 Care Intensity
Longitudinal Comparisons of Risk Perception and Work Stress
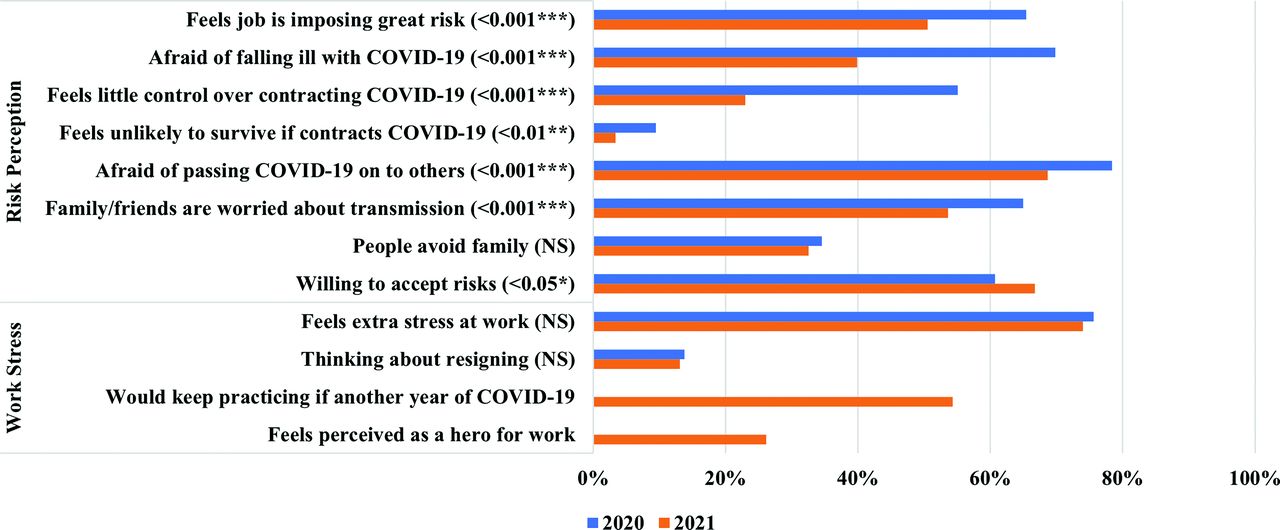
For almost all survey questions related to the perception of COVID-19 risk to self or family, the rate of HCW perceiving risk was much lower during the 2021 survey (Figure 1). HCW were less likely to feel afraid of falling ill with or spreading COVID-19, feel that their job was putting them at risk, feel little control over contracting COVID-19, and feel as though they would die if contracted COVID-19. Although study participants were less likely to report that their friends and family are concerned about about catching COVID-19 from them, they were as likely to report that community members avoid their family. A slightly greater percentage of study participants reported willingness to accept the risks of caring for patients with COVID-19, but there was no statistical difference in the percentage of study participants who reported feeling extra stress at work or considering resigning across the 2 survey rounds. Only 26% of HCW felt like heroes in 2021 and only 54% reported that they would keep practicing if COVID-19 was to go on at a similar pace for another year.
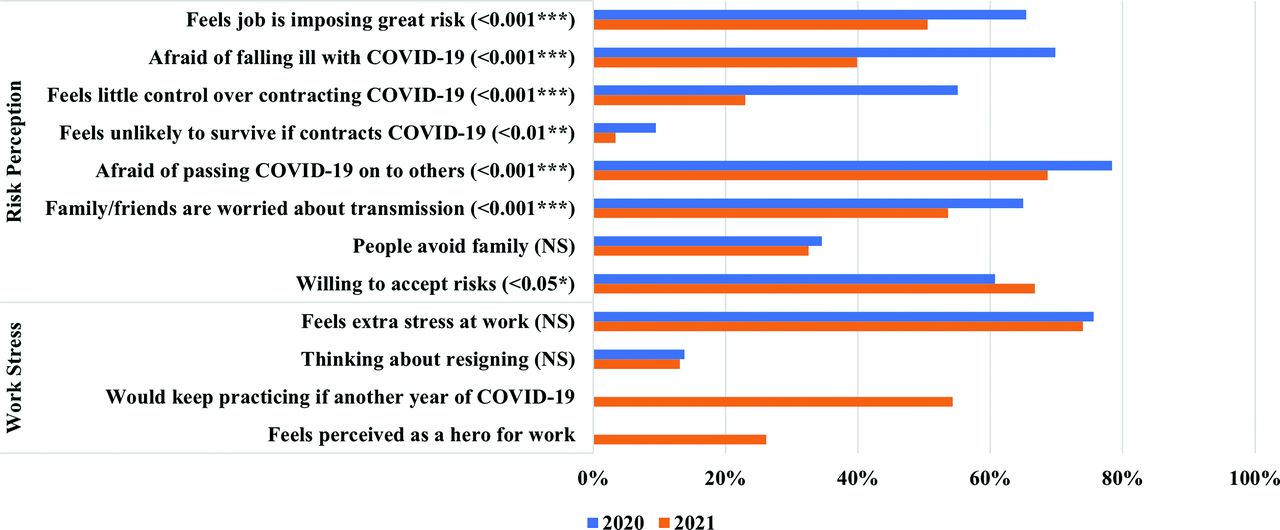
Comparison of risk perception and work-related stress: Spring 2020 versus Spring 2021 (n = 1150).
Risk Perception and Work Stress by COVID-19 Care Intensity
HCW experiencing more than 10 deaths were significantly more likely to feel that their job is putting them at risk (Table 2). At the same time, workers experiencing more than 10 deaths were more likely to view themselves as heroes. There were no differences in perception of risk and work stress across the over measures by COVID-19 care intensity.
Professional Quality of Life 2021
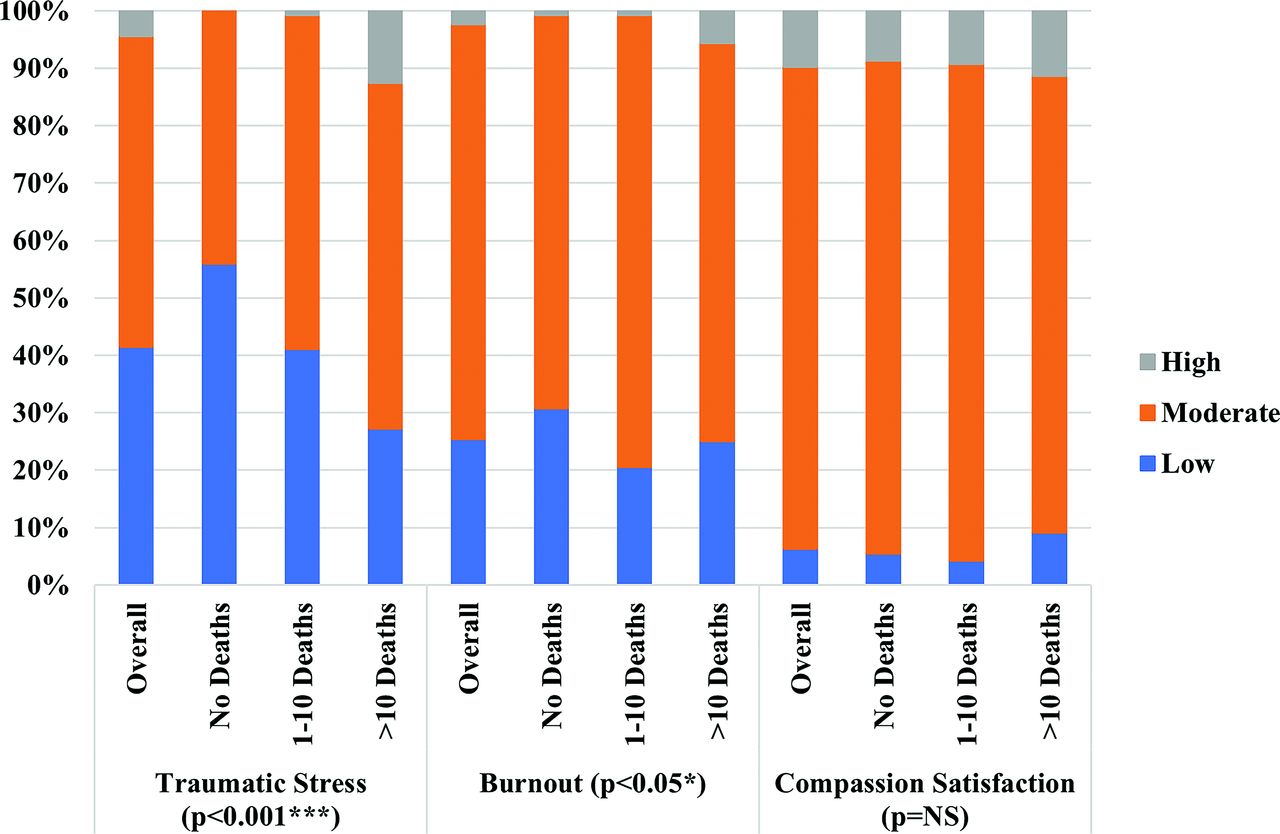
One year into the COVID-19 pandemic, 57% of study participants met criteria for moderate or high levels of traumatic stress overall, and 75% met criteria for moderate or high levels of burnout (Figure 2). The vast majority met the criteria for moderate or high levels of compassion satisfaction (94%). The rate of participants experiencing moderate to high levels of traumatic stress increased as the COVID-19 care intensity increased. Participants who cared for more than 10 COVID-19 deaths were more likely to experience high levels of burnout. The distribution of compassion satisfaction was similar across the 3 COVID-19 care intensity groups.

Traumatic stress, burnout, and compassion satisfaction by COVID-19 case intensity (n = 356).
In the linear regression model (Table 3), traumatic stress was associated with COVID-19 care intensity. As compared with participants who cared for no COVID-19 deaths, participants who cared for 1 to 10 deaths scored 2.7 (P = .007) points higher on the traumatic stress subscale and participants who cared for 10 or more deaths scored 6.7 (P < .001) points higher. As compared with attending physicians, APPs (5.0 points, P = .002), nursing/respiratory therapists (4.3 points, P = .002), and rehab therapists (4.2 points, P = .044) all had significantly greater traumatic stress scores. In addition, participants who were in quarantine for COVID-19 and received the COVID-19 vaccine had higher traumatic stress scores.
Multivariable Linear Regression Exploring the Association between COVID-19 Care Intensity and Traumatic Stress, Burnout, and Compassion Satisfaction (n = 352)
Similar results were observed in assessing burnout. Providers who cared for COVID-19 deaths had significantly higher burnout scores, (1 to 10 deaths: 2.7 points, P = .004; >10 deaths: 2.6 points, P = .036), however, there was no significant difference between the 1 to 10 and >10 death groups. APPs (4.2 points, P = .005) and rehab therapists (4.8 points, P = .013) had significantly higher burnout scores than attending physicians. For both traumatic stress and burnout, there was no statistically significant difference across ages, sex, race/ethnicity, or specialty. There was no difference between attending physicians and trainees (residents or fellows).
There were largely no significant correlates of compassion satisfaction in our model. Asian participants did have significantly higher compassion satisfaction scores than white participants (3.0 points, P = .020), while whereas participants that identified as “other” had lower compassion satisfaction scores (-3.0 points, P = .017).
Discussion
In the first months of the pandemic, our institution performed an initial study on the perception of risk and stress in the hospital environment. The study found that HCW had an increased level of stress compared with baseline due to the fear of contracting the virus or transmitting the virus to friends or family. Nurses, who provide more direct patient care than clinicians, were 4 times more likely to resign due to COVID-19. However, our initial study also revealed there was a significant level of altruism and willingness to care for patients with COVID-19 from many members of the health care team.19
Since that time, there has been a considerable amount of progress made in understanding and combating the virus, including use of Remdesivir and Dexamethasone, and widespread vaccine efforts.15,16 In our current study, we found the extra workplace stress experienced by HCW has not changed significantly 1 year into the pandemic despite widespread vaccination among HCW at our institution. About Approximately half of respondents felt they could not continue practicing at this level if COVID-19 were to continue for another year. This finding demonstrates the persistent challenges HCW face amid the pandemic and highlights the ongoing need for developing effective interventions to manage stress, avoid burnout, and increase well-being in the workplace.
COVID-19 care intensity was a highly significant predictor of traumatic stress and burnout, especially for those who witnessed more than 10 patient deaths. Previous studies have shown that HCW grief is associated with burnout and distress, which were exacerbated by the pandemic.22 The accumulation of unprocessed grief, combined with high levels of traumatic stress, often leads to burnout and leaves the providers with an increased risk of developing mental health issues.23 Furthermore, persistent grief, stress, and trauma from the workspace are detrimental to HCW and can lead to early resignation which further stresses our health care system.
Although HCW overall experienced high levels of extra stress at work, the degree varied based on the number of COVID-19 deaths observed and their specific role. In our institution, APPs experienced 4 more points and nurses experienced 3 more points on the traumatic stress scale relative to attending physicians. Previous studies have similarly demonstrated greater increases in severe mental health symptoms among nurses during disease outbreaks.24 Fellows and residents, on the other hand, scored similarly to attending physicians. This pattern may be explained by the fact that COVID-ICU services, where COVID-19 patients with a greater burden of illness were admitted and cared for, were staffed almost entirely by APPs with attending supervision. In such a case, proximity to patients with severe COVID-19 and providing for their intensive care needs, rather than the provider's specific role, may be more predictive of burnout. This may be an important strategic consideration when preparing for future pandemic responses within hospitals.
HCW in rehabilitation positions also experienced a significant amount of traumatic stress and burnout.25 A very recent study of over more than 20,000 HCW found that nearly half of all participants experienced burnout, with the highest rates occurring among speech therapists, occupational therapists, and social workers. During the pandemic, rehabilitation workers faced new challenges of caring for patients with extremely high oxygen requirements, COVID-19 delirium, and isolation from family. They were also often required to work with COVID-19 patients on their own in an effort to minimize the number of staff members in COVID-19 patient rooms.25
The majority of vaccinated HCW were more likely to report higher levels of caregiver stress and burnout; this group also witnessed more patient deaths, possibly making them more likely to accept early vaccination. Thus, we could not conclude if the vaccine was protective due to the high rate of vaccinated staff at our facility and the positive relationship between COVID-19 care intensity and vaccination.
Recommendations/Policy Implications
The prevalence of mental illness and burnout among HCW has been a focus of public health officials, policy makers, administrators, and researchers and now brought to the forefront during the pandemic This heightened awareness presents a unique opportunity for health care systems to reevaluate how it can help medical professionals manage and cope with stress. Interventions focused on addressing the growing issues of increased stress, burnout, feeling unvalued, and processing trauma, among many others, have gained significant traction. By way of example, a group in the United Kingdom explained their approach for providing stress management techniques for HCW through a digital package platform with modules focused on social stigma, peer and family support, self-care strategies related to sleep and rest, and healthy lifestyle behaviors.26
Aside from medical institutions, government entities at the local, state, and federal levels can also play a salient role in improving the mental health of frontline HCW. Local governments could partner with health care institutions to recognize and appreciate HCW, as feeling valued may lead to lower burnout.26 Furthermore, state and federal entities may improve the mental health of frontline personnel by lessening their financial burden, a significant stressor for many HCW. A bill establishing a COVID-19 frontline HCW loan forgiveness program may become a reality in the state of New York.27 Although some preliminary steps have been taken, Other innovative programs and strategies are needed to support the essential health care professional.
Limitations
This study was limited by the number of respondents as well as the demographics of respondents. Due to the anonymous nature of the survey and high staffing turnover, a denominator for participation could not be determined. Furthermore, participants were not required to complete the survey in its entirety, and could have their responses recorded more than once; only completed responses were analyzed thus the n for each table varies. The primary survey performed at the inception of the pandemic had a higher response rate with a different demographic distribution when compared with this study performed 1 year into the pandemic. In the 2020 survey, there was no free text field for HCWs to describe their profession or specialty if noted as “other.” In the 2021 survey, a free text field was included to specify categorization of position and specialty and free text responses were able to be categorized; as a result, there were much lower percentages of workers classified as “other” in the 2021 survey. This is most likely due to the novel nature of the virus and willingness to participate in COVID-19 research. In addition, the study was performed at a single academic institution thus results may not be generalizable. Lastly, as with all anonymous survey studies, there may be sample bias, and answers can be biased and lack objectivity.
Conclusion
In this follow-up survey study, we evaluated the perceptions of risk of viral transmission as well as overall stress among HCW caring for COVID-19 patients in an inpatient setting. Our primary hypothesis that perceptions of both risk and stress would decrease over the course of the year held true, but levels of stress still remained high despite high vaccination rates. We also found that those who witnessed more COVID-19 deaths were more likely to report feeling burnt out and stressed. With an optimistic view that our nation recovers from the COVID-19 pandemic, it is imperative to focus on recovery strategies for high burnout groups to ensure the wellbeing of our health care workforce.
Appendix
Survey Questions*
Care Intensity Analysis
Notes
This article was externally peer reviewed.
Funding: The authors received no financial support for the research, authorship, and/or publication.
Conflict of interest: To the best of our knowledge, the named authors have no conflict of interest, financial or otherwise.
To see this article online, please go to: http://jabfm.org/content/35/2/284.full.
- Received for publication July 2, 2021.
- Revision received November 10, 2021.
- Accepted for publication November 11, 2021.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 'You just dont feel like your work goes recognised: healthcare worker experiences of tension related to public discourse around the COVID-19 pandemic
- Development, implementation and usefulness of an intervention to support psychological resilience during the COVID-19 pandemic: a study from a Swedish hospital based on interviews, documents and a survey
- This Issue's Emphasis: Inequity and COVID-19, Intertwined