
Article Figures & Data
Figures
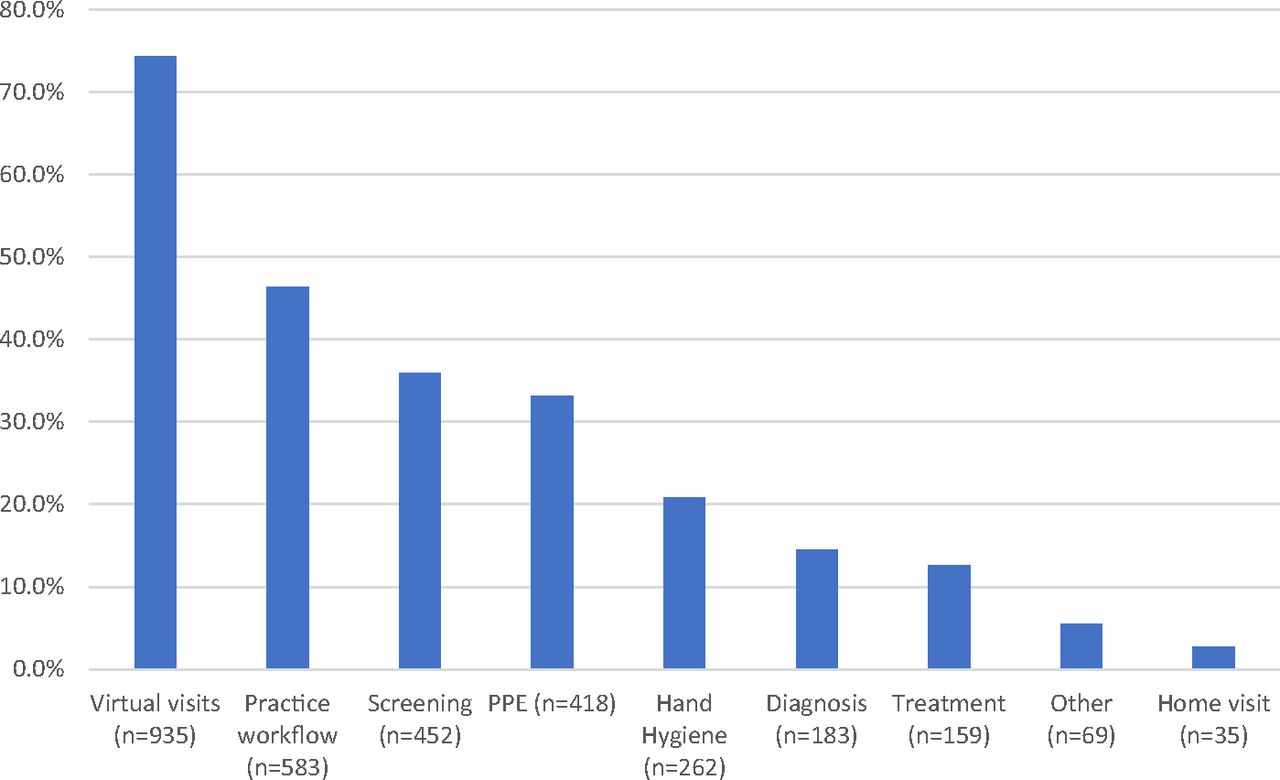
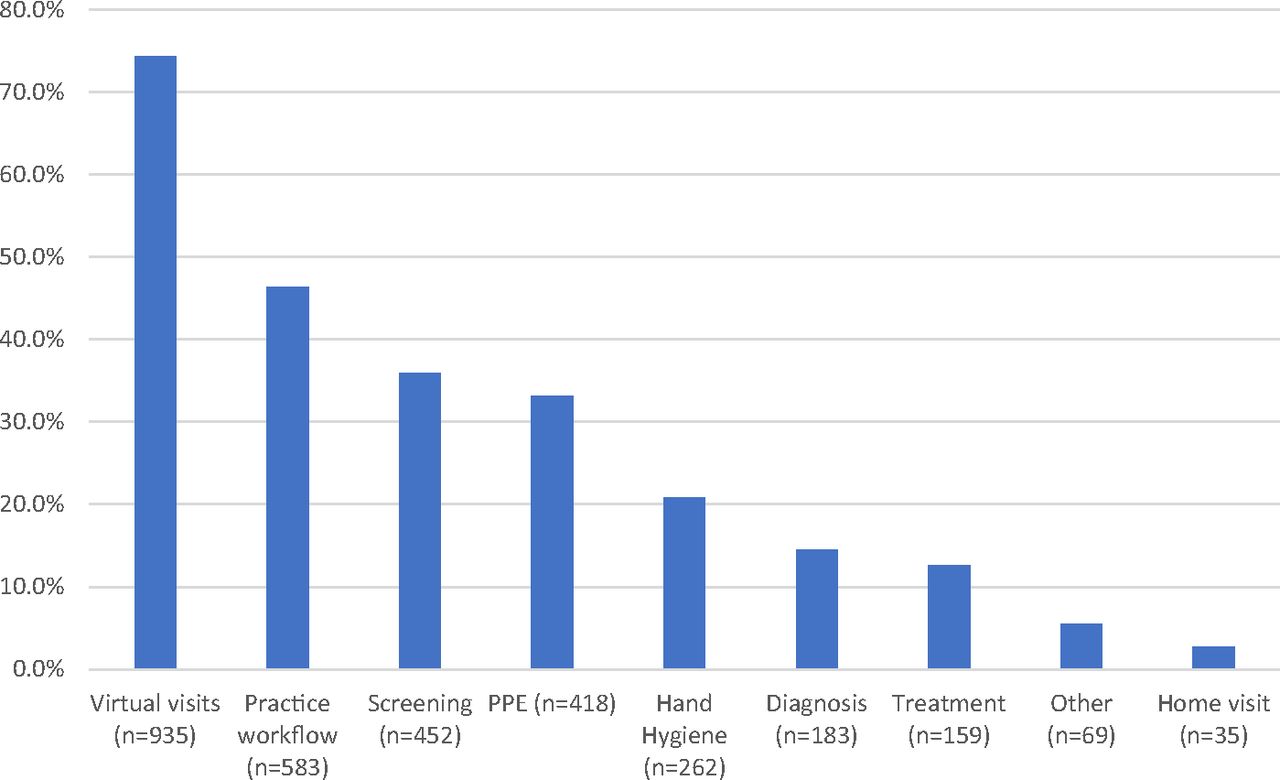
- Figure 1.
COVID-19 Performance Improvement Topic Areas From Diplomates Submitting COVID-PI Activities, April 1–June 30, 2020 (n = 1259). Abbreviation: PPE, personal protective equipment.
Tables
- Table 1.
Characteristics of Diplomates Submitting COVID-PI Activities, April 1–June 30, 2020 (n = 1259)
Submitting diplomates All ABFM diplomates Characteristics (n, %) (n, %) Gender Male 515, 40.91% 54102, 53.58% Female 744, 59.09% 46868, 46.42% Time since initial certification <5 years 177, 14.06% 18022, 17.85% 5 to 10 years 313, 24.86% 19387, 19.20% 11 to 20 years 332, 26.37% 27042, 26.78% >20 years 419, 33.28% 36519, 36.17% Not currently certified* 18, 1.43% 0, 0.00% Practice characteristics Solo 34, 2.70% 2735, 2.71% 2 to 5 providers 135, 10.72% 8477, 8.40% 6 to 20 providers 105, 8.34% 8111, 8.03% >20 providers 85, 6.75% 6459, 6.40% No data available† 900, 71.49% 75188, 74.47% Faculty (medical school and/or residency) No 294, 23.35% 21242, 21.04% Core/salaried faculty 34, 2.70% 2930, 2.90% Volunteer/clinical faculty 83, 6.59% 6110, 6.05% No data available† 848, 67.36% 70688, 70.01% Primary practice site Hospital-/health system-owned medical practice (not managed care or HMO) 145, 11.52% 8925, 8.84% Independently owned medical practice 105, 8.34% 7685, 7.61% Managed care/HMO practice 20, 1.59% 1602, 1.59% Academic health center/faculty practice 20, 1.59% 2006, 1.99% Federally qualified health center 13, 1.03% 1641, 1.63% Rural health clinic (federally qualified) 3, 0.24% 564, 0.56% Indian Health Service 3, 0.24% 157, 0.16% Government clinic, nonfederal (eg, state, county, city, maternal/child health, public health center) 7, 0.56% 415, 0.41% Military, Veterans Administration, Department of Defense 19, 1.51% 1079, 1.07% Workplace clinic 3, 0.24% 470, 0.47% Other 21, 1.67% 1240, 1.23% No data available† 900, 71.49% 75186, 74.46% Specialty mix Family medicine only 175, 13.90% 12035, 11.92% Primary care specialty mix (family medicine, internal medicine, and/or pediatrics) 80, 6.35% 6516, 6.45% Multiple specialties (not only primary care) 73, 5.80% 5345, 5.29% No data available† 931, 73.95% 77074, 76.33% Site ownership No official ownership stake (100% employed) 356, 28.28% 26950, 26.69% Sole owner 37, 2.94% 3110, 3.08% Partial owner or shareholder 56, 4.45% 5747, 5.69% Self-employed as a contractor (including locums) 16, 1.27% 1347, 1.33% Other 8, 0.64% 558, 0.55% No data available† 786, 62.43% 63258, 62.65% - Table 2.
COVID-19 Performance Improvement Lessons Learned by diplomates Submitting COVID-PI Activities, April 1–June 30, 2020
Theme Definition Illustrative remarks Safety (n = 363) Safety or protection of patients and/or staff, including PPE and measures that helped to control spread of COVID-19 and reduce risk, and/or appreciation that these measures are necessary “In terms of minimizing risk of COVID-19 infections in our patients, I have no doubt that the move to phone visits was absolutely necessary.”
“…the viral clinic allowed us to quickly screen patients who were symptomatic before they spent significant time in the waiting room, nearby others who did not have symptoms.”
“All of these above interventions helped greatly conserve our PPE and make it safer for both our staff and patients. … Our triage nurses were able to keep most patients at home to decrease PPE use and unnecessary visits. Our virtual visits helped decrease exposure of our chronic disease patients to acute illnesses and decrease spread.”Process of care/workflow (n = 312) Processes and workflow must evolve/adapt to meet changing context and patient needs; time related issues around patient care, practice changes, and so forth “We are steadily increasing our telemed visits although not to goal yet. I understand there continues to be changes but we will try to evolve as the changes come.”“We learned that the ability to deliver MRI results by phone is a practice we likely can continue post-COVID pandemic because it is an effective way to communicate and determine next steps/ follow up to save the patient time and free our staff/ schedules.” Positive view of virtualization (n = 225)* General comments highlighting that virtual visits were helpful or benefitted patient careIndication of intent or commitment to continue virtual visits after the pandemic “[We} Learned that telehealth can be utilized for quality care.”
“We learned that the virtual visits are an invaluable underestimated tool in primary care. Something that we plan to implement in the future as part of our regular care.”Access to care (n = 203) Changes in patient access to care (increased access due to virtual option, or decreased access due to challenges with virtual or clinic closures/reduced hours) “Virtual visits provided excellent patient access in the setting of a pandemic.”
“As a result of the measures taken to begin telemedicine in our practice, our clinic was able to provide over 50% of our medical care virtually. We learned that we can rapidly adapt to a pandemic situation to ensure safety of staff and clients and to ensure continuity and access of care to our patient population.”
“One of the problems with virtual visits is that the other population that we serve do not have computers and are not able to do virtual visits due to lack of computer knowledge.”Patient satisfaction (n = 193) Patients are happy with the quality of virtual care or appreciated access to care during the pandemic “Telehealth has and continues to have some bumps put patients like it and it provides a great way to reach patients when access is challenged. Patients really like it.”
“I was concerned at first that quality of care would be compromised with virtual visits, but I came to learn that it was not and in many instances was enhanced. Patients were appreciative of having a way to stay connected to their physician that did not put them at risk of exposure to COVID-19.”
“This has been a very positive activity. The patients who participated in the virtual visits had the time allotted to address their questions, review and update the medical history, and make sure that we discussed their medical conditions as well as all the medications we had listed in their chart. The patient was followed up by my office nurse with a 3-question phone satisfaction survey. The results were that they all (100%) felt that the telehealth experience was excellent. They would all (100%) have another telehealth visit in the future, and they all (100%) would recommend a telehealth visit to other patients.”Team (n = 113) Importance of the healthcare team working together to accomplish goals; comments on the educational needs or shifting/evolving of team roles in response to the pandemic “I learned that many visits can be done virtually and that teamwork was more important than ever to quickly adapt to a changing healthcare world.”
“Patients and staff felt safe and comfortable in managing patients and we were able to provide continuing care for our patients. This does require ongoing education for the staff and patients, as we assure patients the distance and masks are for their and our protection.”Patient/physician communication (n = 87) Comments about the quality and/or frequency of communication with patients “Possible decrease transmission but decreased quality of interaction.”
“I learned that patients are much more comfortable at home and were more talkative, less nervous than in the office. It was also insightful seeing their home environment.”Quality of care (n = 85) Potentially improved, maintained, or decreased quality of care “By implementing the above changes and using Telehealth more effectively we found no significant difference in quality of care or patient satisfaction compared to face to face visits.”
“I do feel there is some risk involved in doing alternate type visits since we cannot get vitals/do any physical exam.”Technology (n = 79) Patients struggle with or lack of access to technology; issues implementing or integrating new technological platforms in practice “At the beginning of the pandemic, CMS only was approving telehealth visits via audio-video, but many of our geriatric and disabled population do not have access or know how to use this technology. Or they need help to use it, and in getting help, may end up divulging sensitive personal information in order to be able to get quality health care. This is not right and must change. We are looking at how to restructure/better structure a home health/visit program for this population.”
“I also learned the necessity of a good telemedicine platform that is user-friendly so that some of these visits could be completed virtually.”Patient visit volume (n = 58) Changes (or stability) in patient volume due to QI intervention “We learned that virtual visits enabled us to conduct not just a portion but close to our usual office volume of visits, in the setting of a global pandemic.” Coding/reimbursement/ regulatory issues (n = 37) Challenges with billing or reimbursement. Challenges with or learning new ways of coding “Overhead increased and revenue plummeted, and we have yet to see insurance reimbursement on the telemedicine.”
“Our providers learned many lessons and developed new skills, including… coding telehealth visits with the use of appropriate E and M codes.”Stress–burnout (n = 12) Toll on physicians, staff, practices of dealing with changes/pressures brought by COVID-19 “We have asked staff to participate in stress control as well as many of us have suffered from profound fatigue with the constant amount that we feel we have to read to keep up to date and able to care for our friends and families.” ↵* Of these reflections, 93 (41.3%) indicated an intent to continue offering some virtual visits after the pandemic.
Abbreviations: PPE, personal protective equipment; QI, quality improvement.




{kind=link}