
Article Figures & Data
Figures
- Figure 1.
PRISMA flow diagram of the search process.












































Tables
Author, Year Country Patients Studied Mean or median age % Male Definition of Bad Outcome Mortality Rate, % Yu, 202032 China Adults with COVID-19 from 27 hospitals in Jiangsu Province with a CT scan 48 (median) 53.0 Composite of ICU admission, acute respiratory failure occurrence, or shock during hospitalization 15.0 Wang, 202033 China Adults with COVID-19 who were discharged from 2 hospitals (Wuhan and Hubei Province) 51 (median) 53.3 Death 17.8 Chen, 202034 China Adults with COVID-19 classified as moderately, severely or critically ill in 1 hospital in Wuhan 68 (median) 62.4 Death 41.2 Zhou, 202035 China Adults with COVID-19 who had been discharged or died in 2 Wuhan hospitals 56 (median) 62.3 Death 28.0 Liu, 202036 China Adults with COVID-19 pneumonia in 3 tertiary hospitals in Wuhan 38 (median) 50 Clinical deterioration 14.1 Liang, 202019 China Adults with COVID-19 from 575 hospitals in 31 regions of China 48.9 (mean) 57.3 Composite of admission to ICU, invasive ventilation, death 3.2 Xie, 202037 China Adults with COVID-19 who had been discharged from or died in 2 hospitals in Wuhan 62 (median) 53.8 Death 50.5 Yan, 202038 China Adults with COVID-19 in 1 hospital in Wuhan 58.83 (mean) 58.7 Death 46.4 Cao, 202039 China Adults with COVID-19 in 1 hospital in Shanghai 50.1 (mean) 51 Admission to ICU NR Hu, 202040 China Adults with COVID-19 in 1 hospital in Wuhan 61 (median) 51.4 Death or progression 10.8 Luo, 202041 China Adults with COVID-19 with a clinical outcome in 1 hospital in Wuhan 57 (median) 50.3 Death 28.2 Petrilli, 202042 United States Adults with laboratory confirmed critical COVID-19 in 1 hospital in New York City 54 (median) 49.5 Composite of ICU, mechanical ventilation, discharge to hospice or death. 24.3 Wu, 202043 China Adults with COVID-19 pneumonia in 1 hospital in Wuhan 51 (median) 63.7 ARDS 21.9 Li, 202044 China Adults with laboratory confirmed severe COVID-19 infection 57 (median) 58 Death 14.7 Jang, 202045 Korea Adults with COVID-19 hospitalized at a tertiary hospital in Daegu, Korea 56.9 (mean) 43.6 Compositive of ARDS, ICU care, or death 7.3 Xu, 202046 China Adults with laboratory-confirmed COVID-19 admitted to 16 tertiary hospitals from 8 provinces in China 46.1 (mean) 54 Composite of death, ICU, or requiring mechanical ventilation. 4.7 Zhou, 202047 China Adults with laboratory-confirmed COVID-19 collected from 47 locations in Sichaun 43 (median) 56.6 Vasopressors or respiratory failure + 3 of: respiratory rate >30, PaO2/FIO2 ≤250 mm Hg, infiltrates, confusion, BUN ≥20 mg/dL, leukopenia, hypothermia, thrombocytopenia, or hypotension. NR Hou, 202048 China Adults with laboratory-confirmed COVID-19 hospitalized at Beijing hospitals 50.9 (median) 43.6 Progression defined as having a clinically advanced type of COVID-19, ICU admission, or death during hospitalization 5.0 Zhang, 202049 China Adults with laboratory-confirmed COVID-19 in 1 hospital in Wuhan, China 38.0 (median) 41.4 Disease deterioration including the transfer to ICU and death 13.5 Liu, 202050 China Adults with laboratory-confirmed COVID-19 in 1 hospital in Wuhan, China 65.5 (median) 35.0 Severe disease defined as having shortness of breath, RR ≥30 bpm, O2 sat ≤93%, PaO2/FIO2 ≤ 300 mm Hg, and progression on imaging NR Zhu, 202051 China Adults with confirmed COVID-19 at 1 hospital in Zhejiang, China 50.9 (mean) 35.4 Severe disease defined as shortness of breath, RR ≥30 bpm, O2 sat ≤93%, PaO2/FIO2 ≤300 mm Hg, or lesion progression NR Hu, 202052 China Adults with laboratory-confirmed critical COVID-19 in 1 hospital in Wuhan, China 60.8 (mean) 50.9 Death 18.0 COVID-19, coronavirus 2019; CT, computed tomography; RR, respiratory rate; O2 sat, oxygen saturation; BUN, blood urea nitrogen; ICU, intensive care unit; ARDS, acute respiratory distress syndrome.
- Table 2.
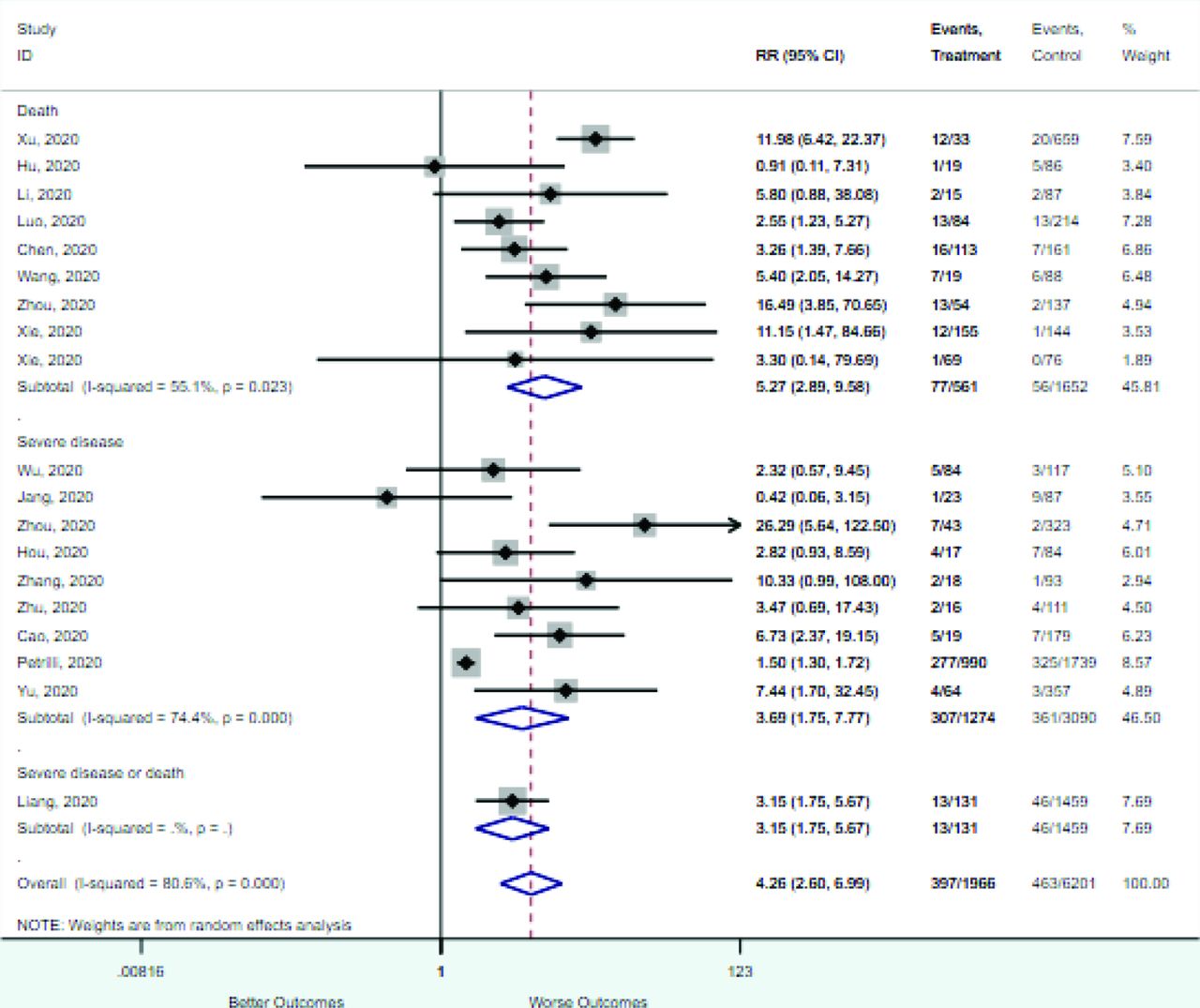
Association between Categorical Variables and Mortality or Severe Disease in Patients with COVID-19
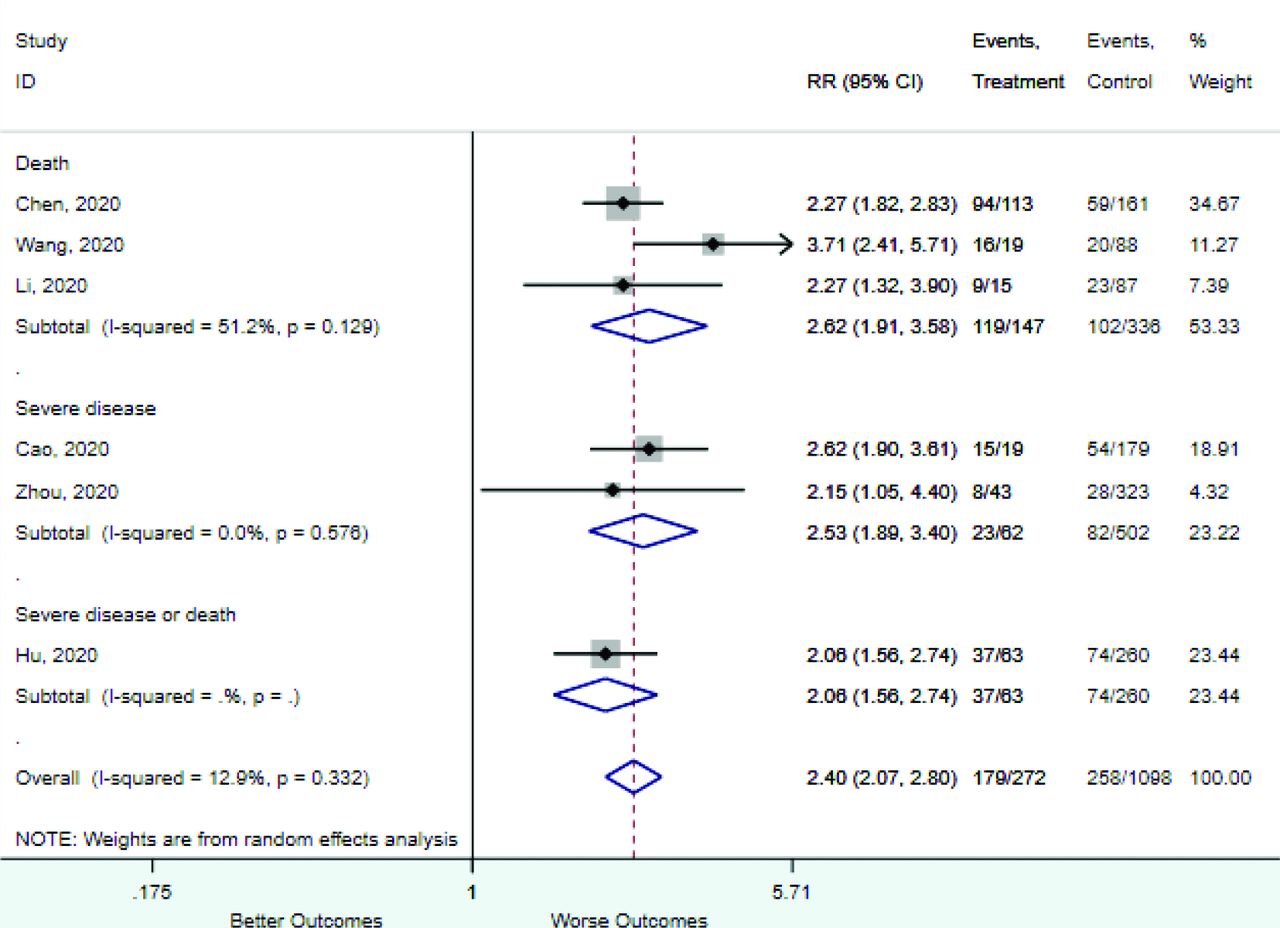
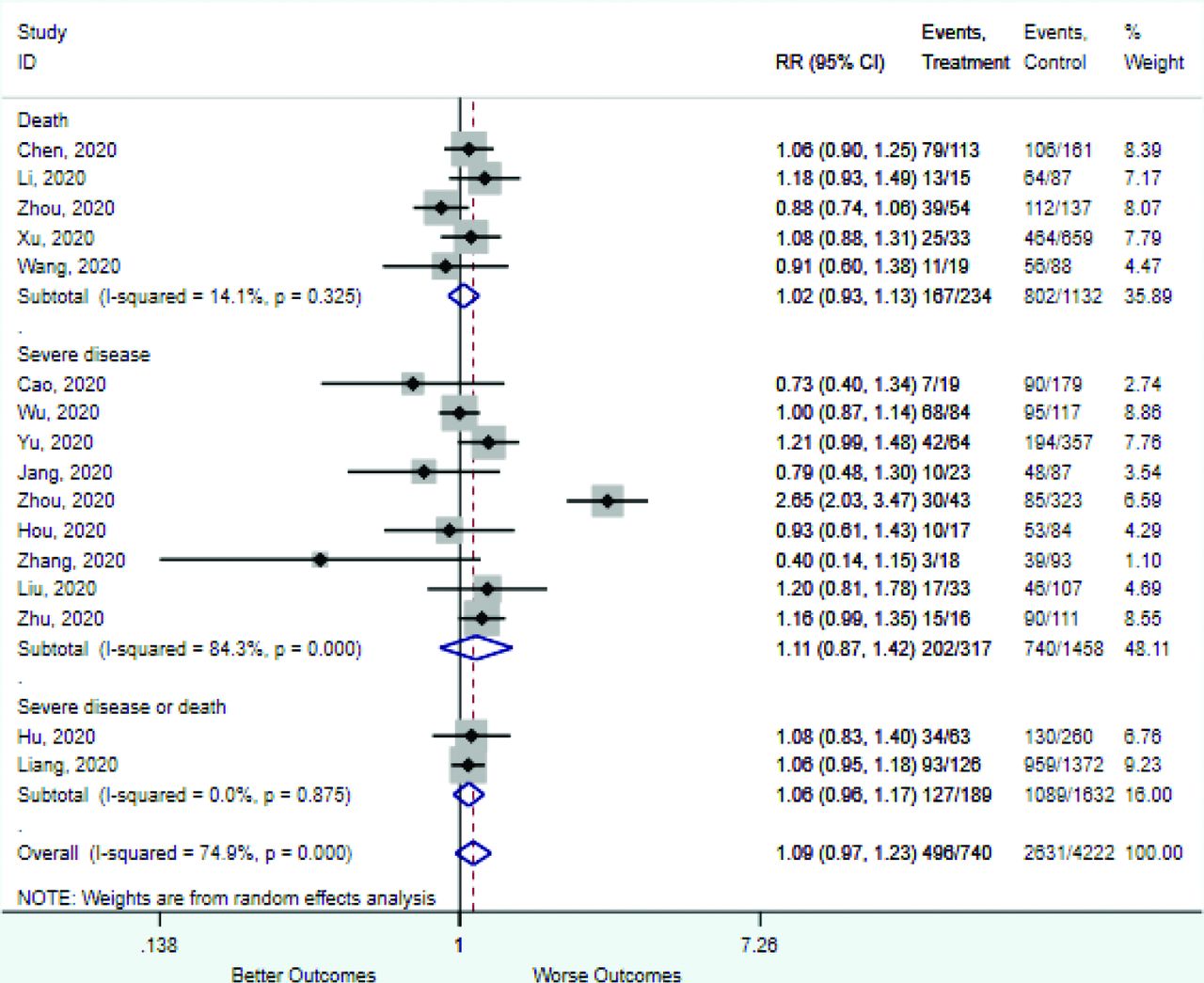
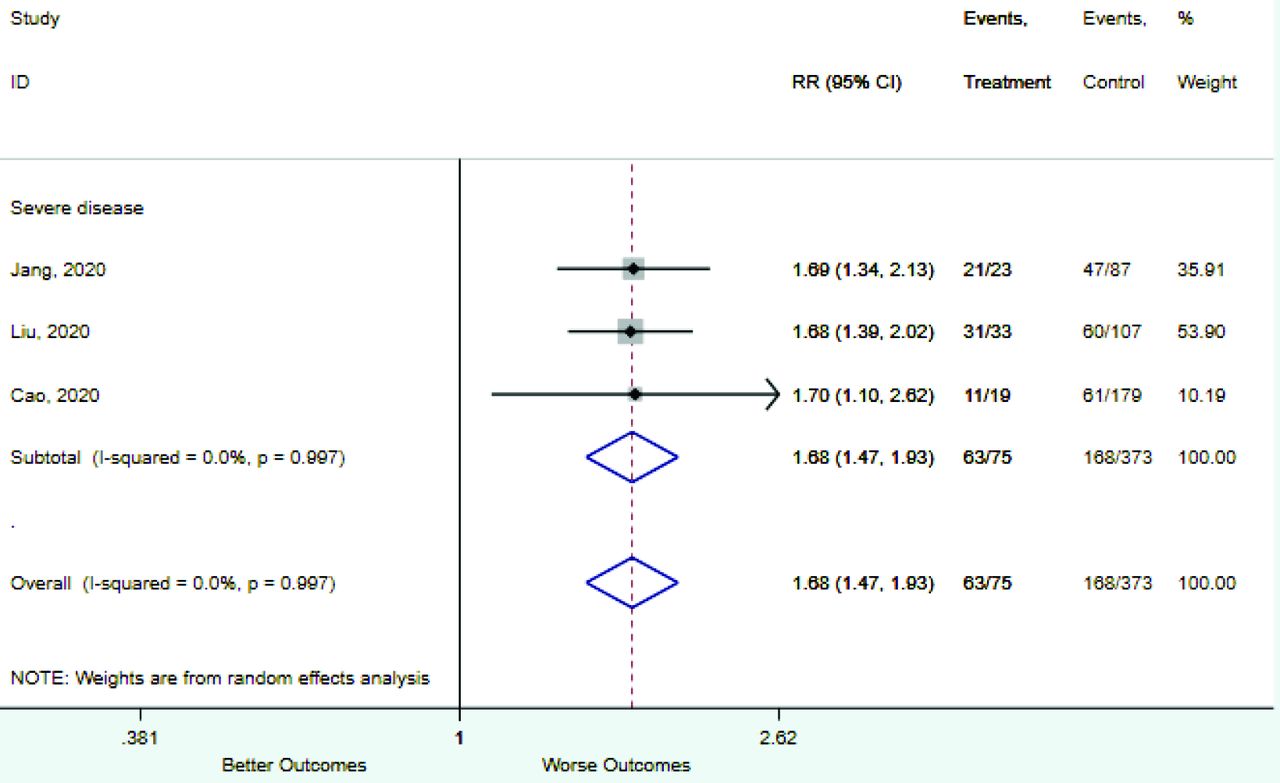
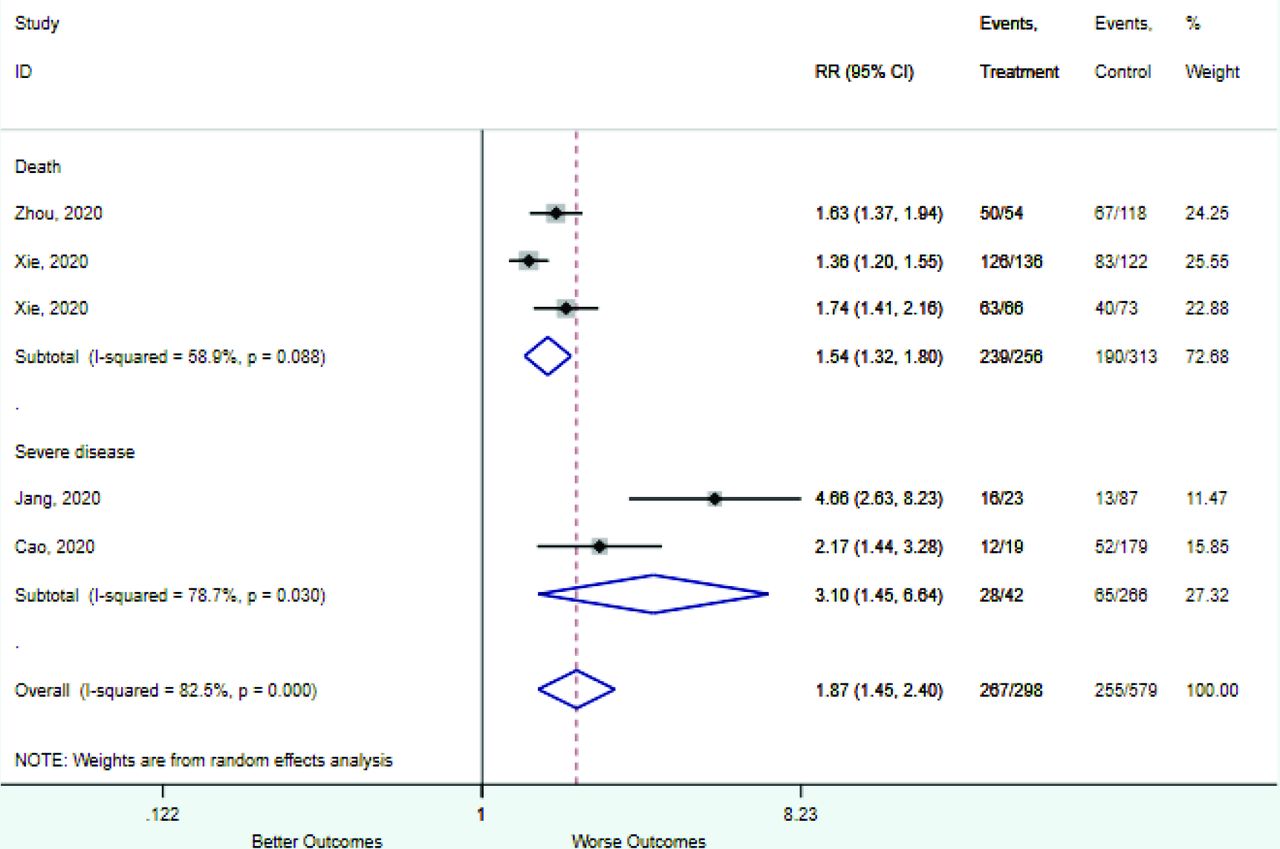
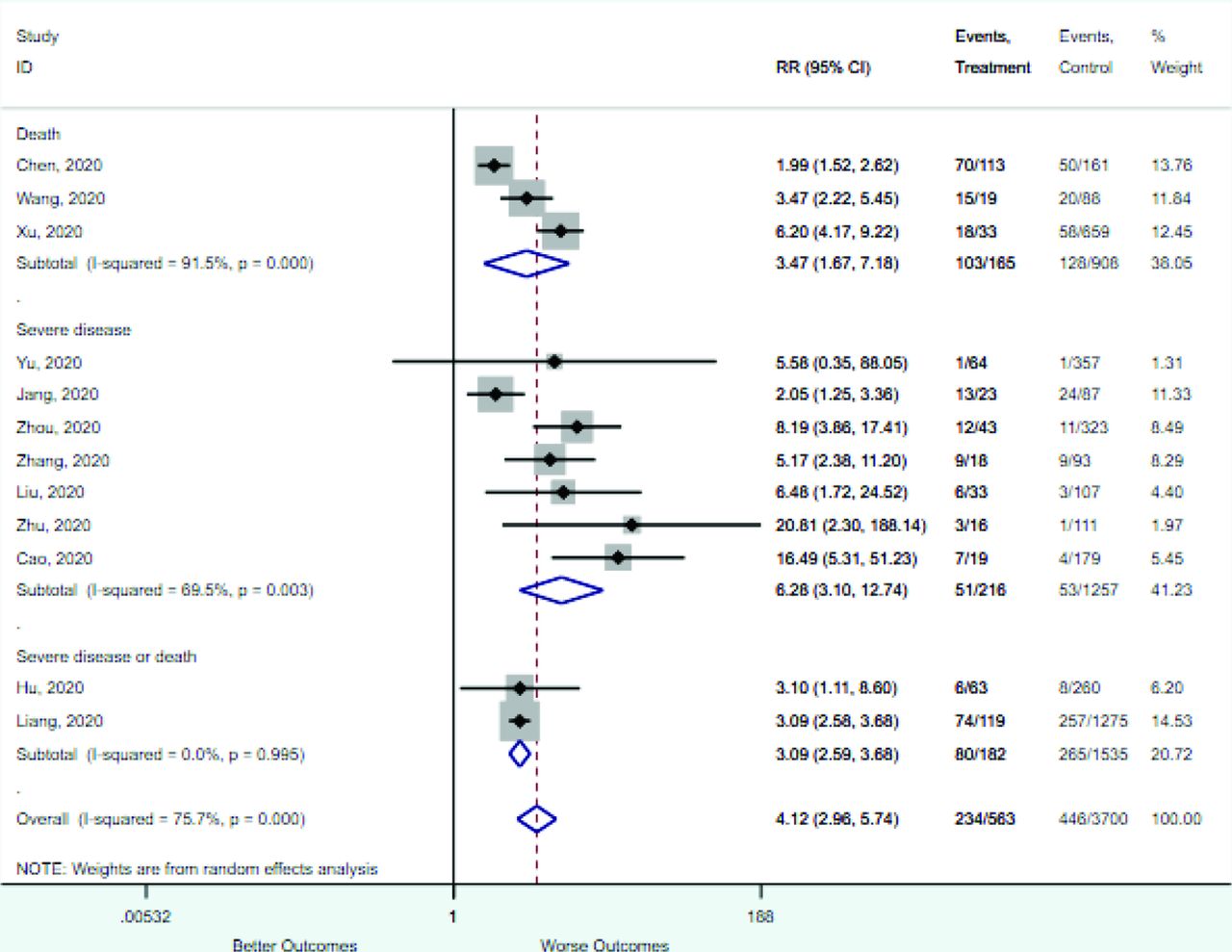
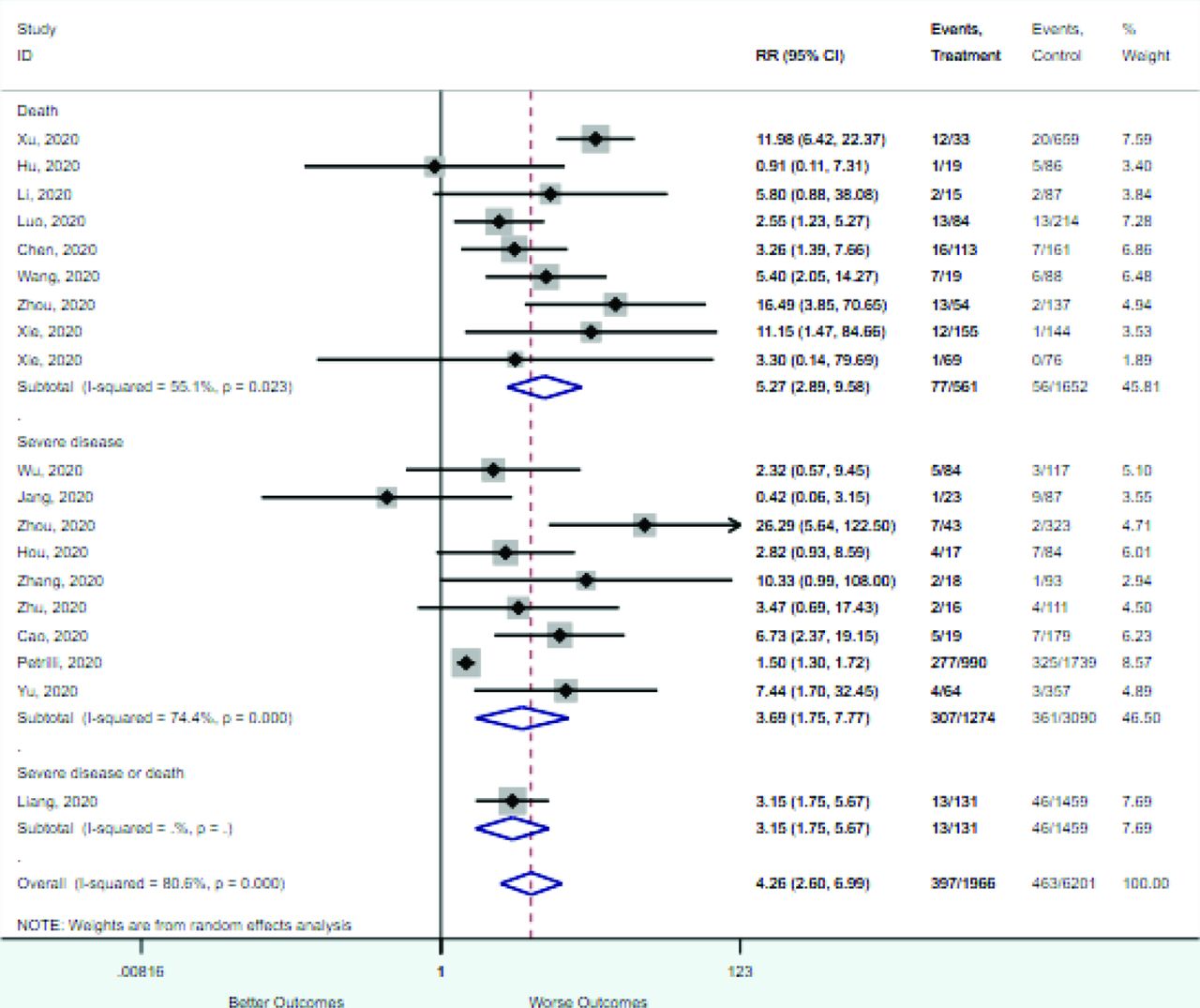
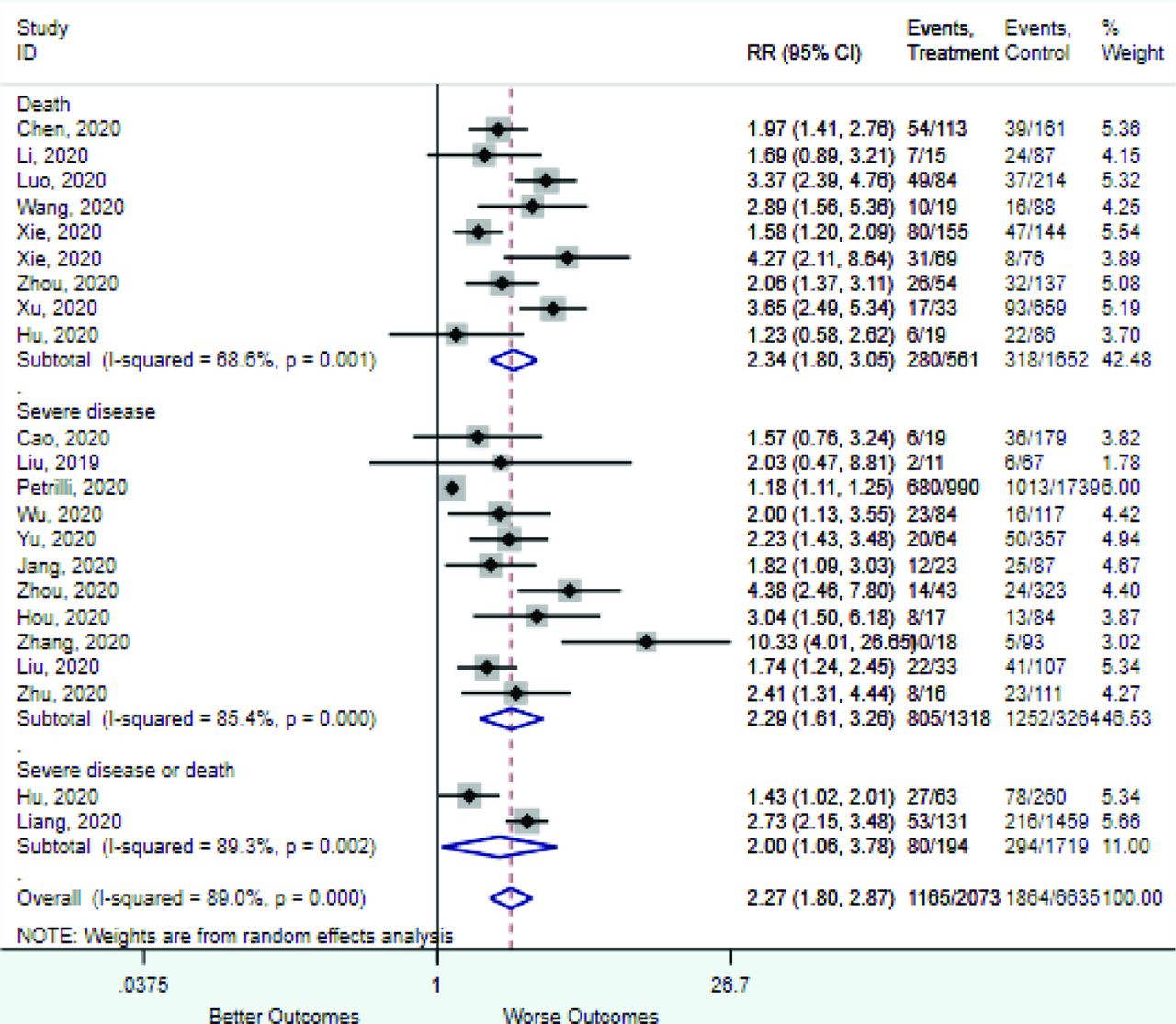
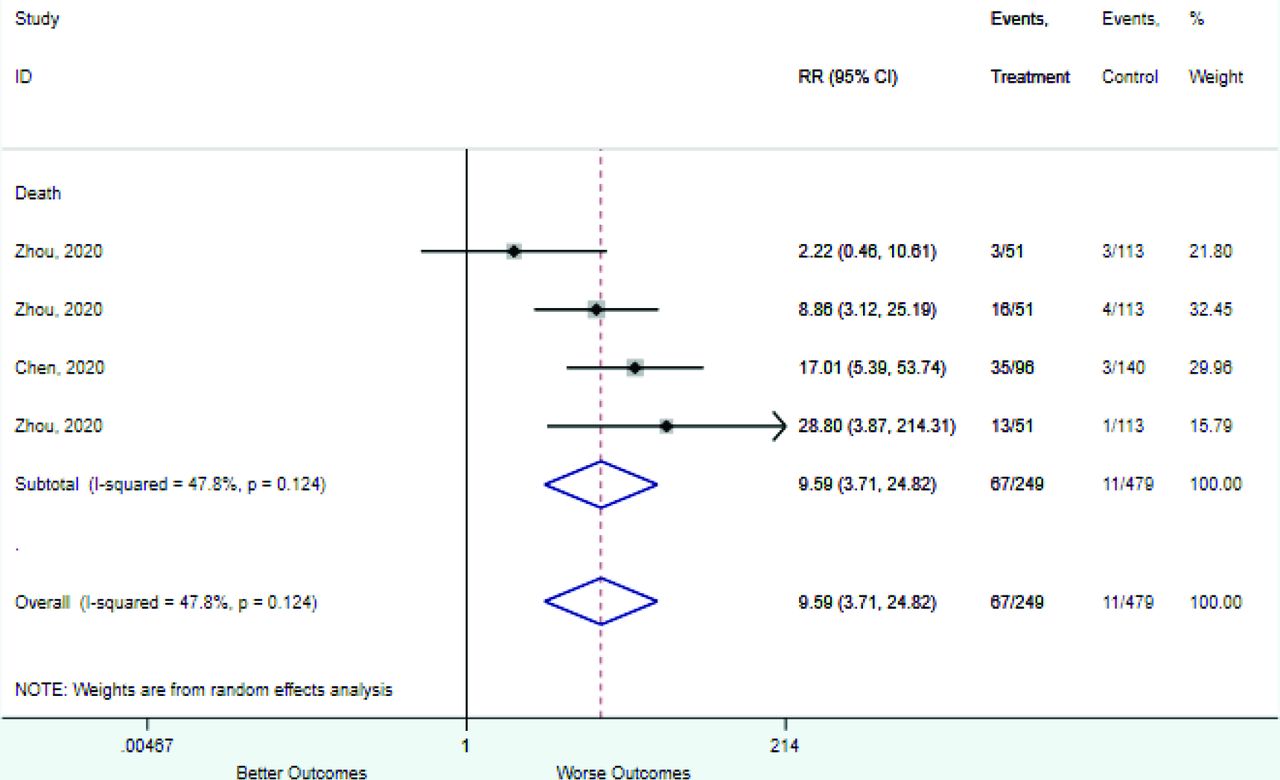
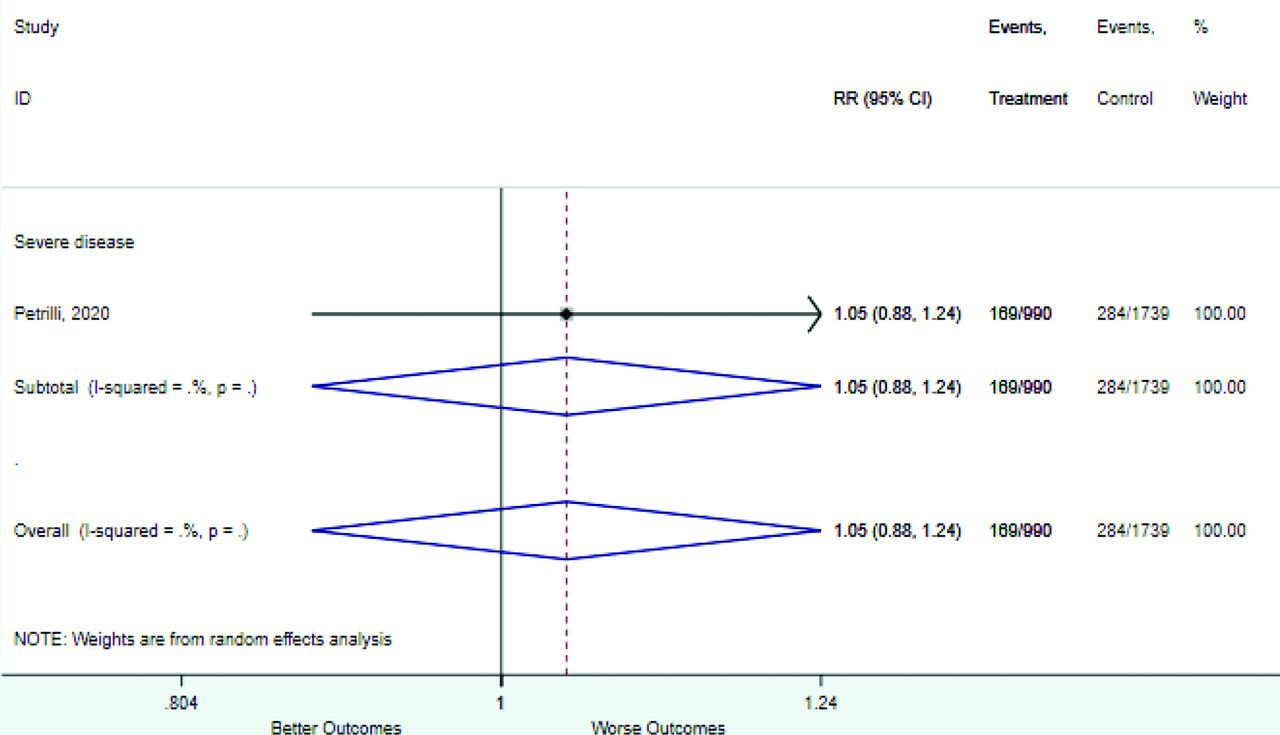
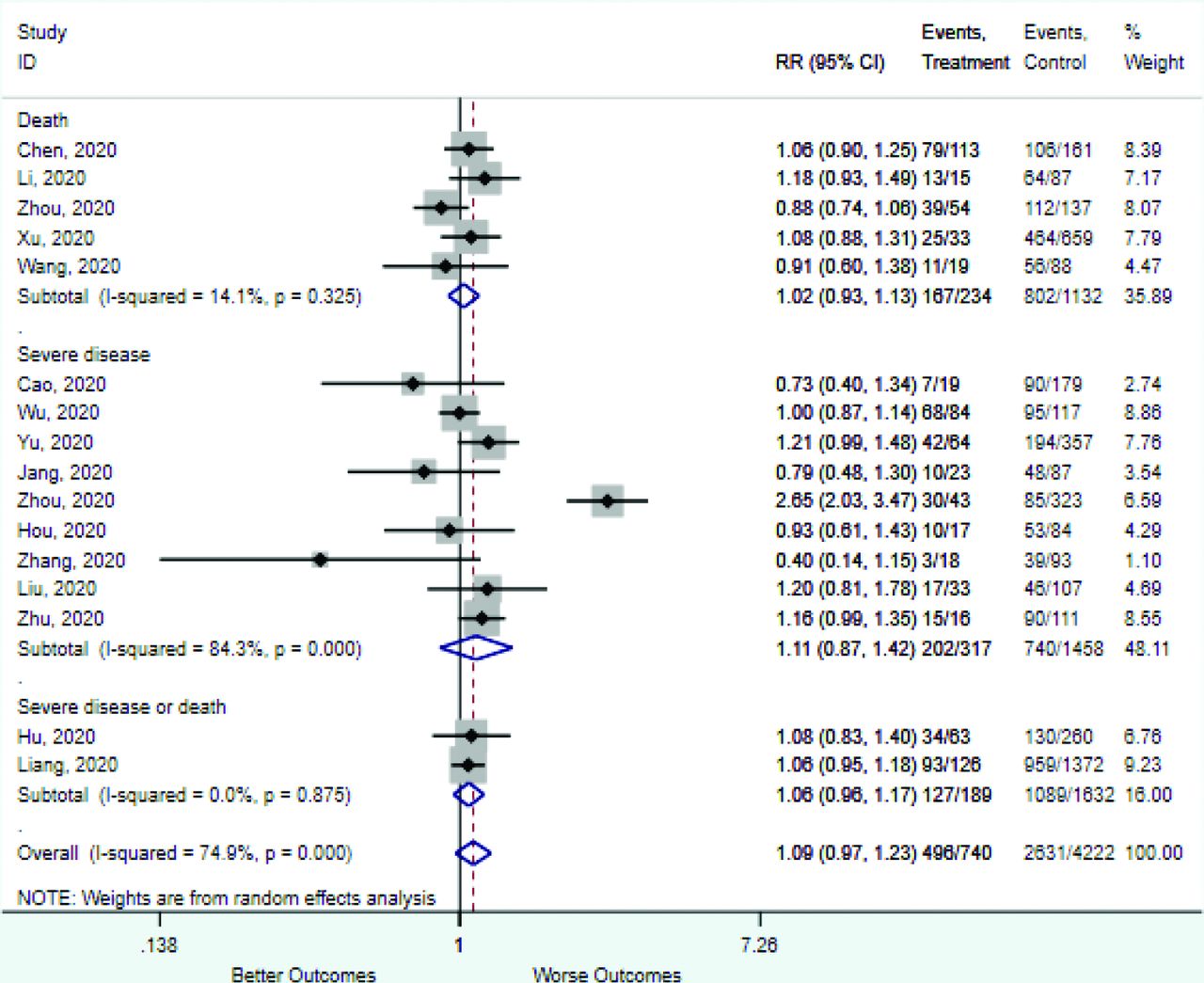
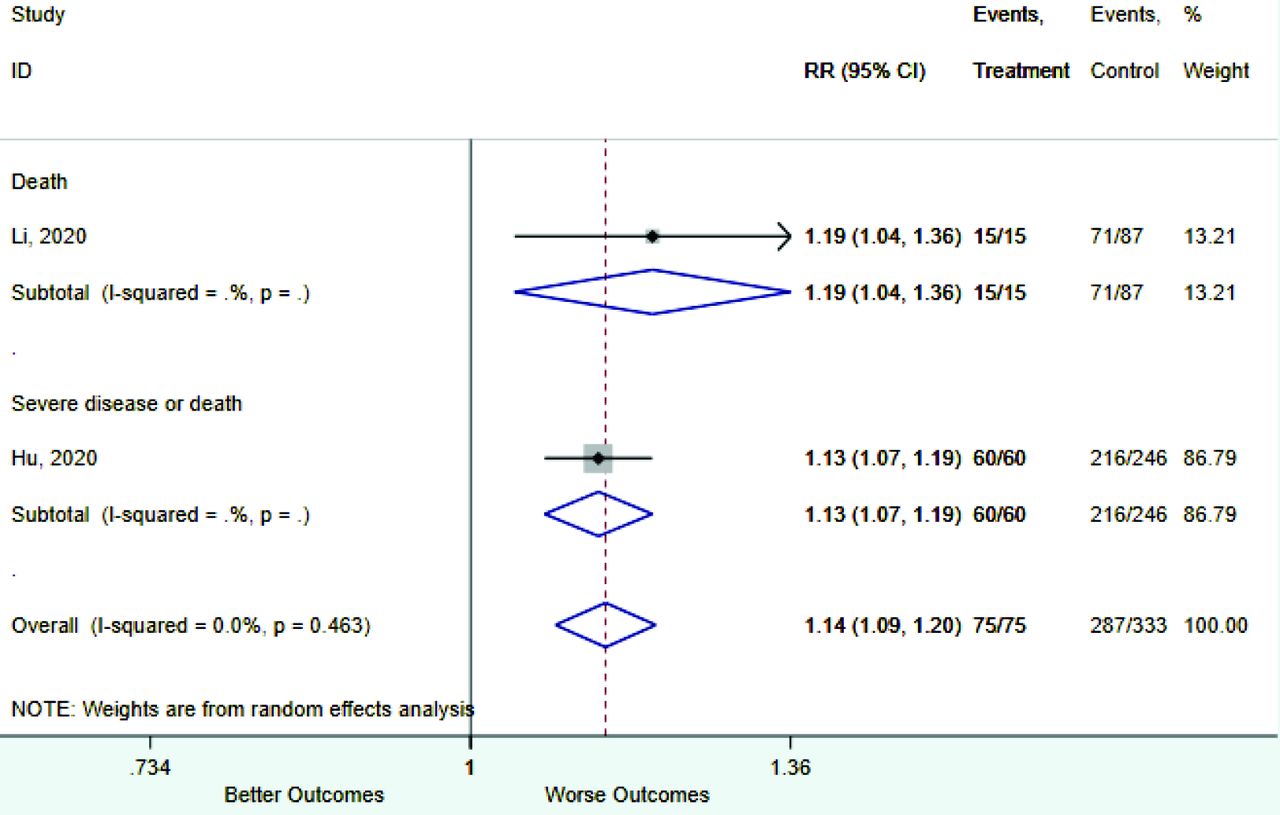
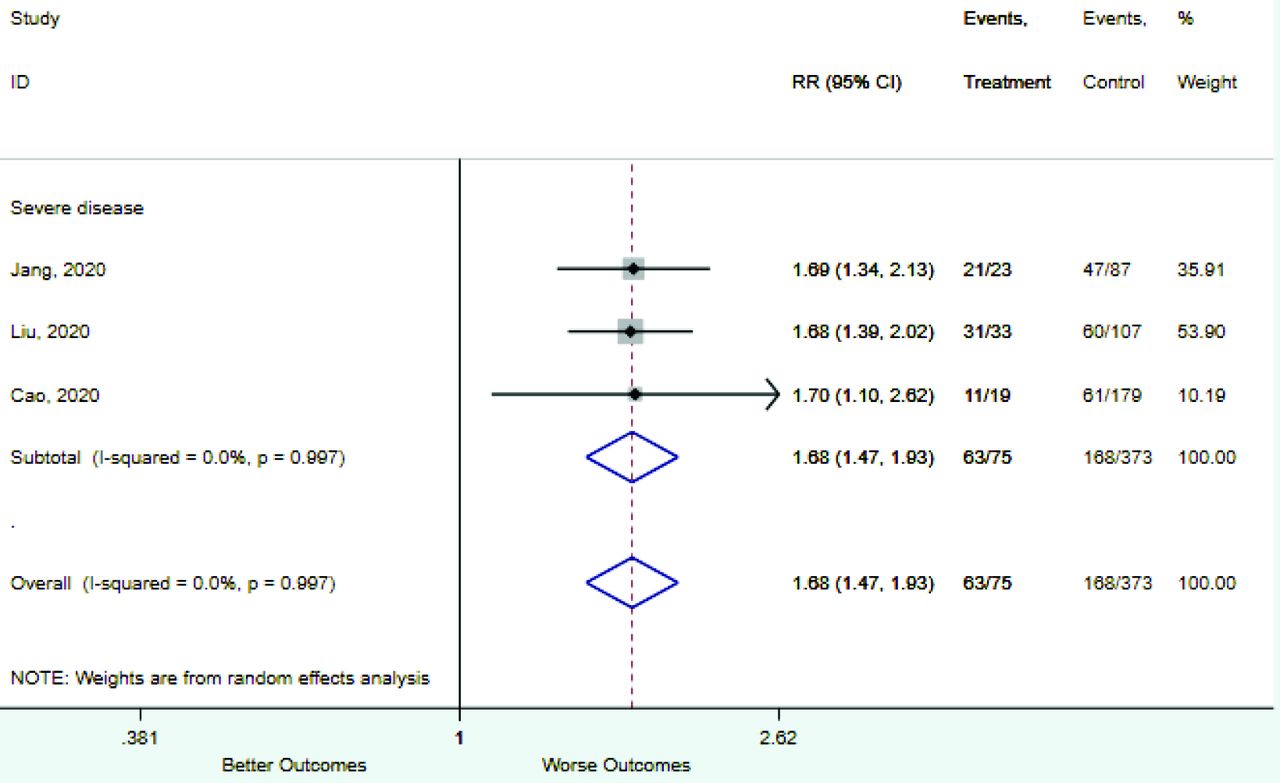
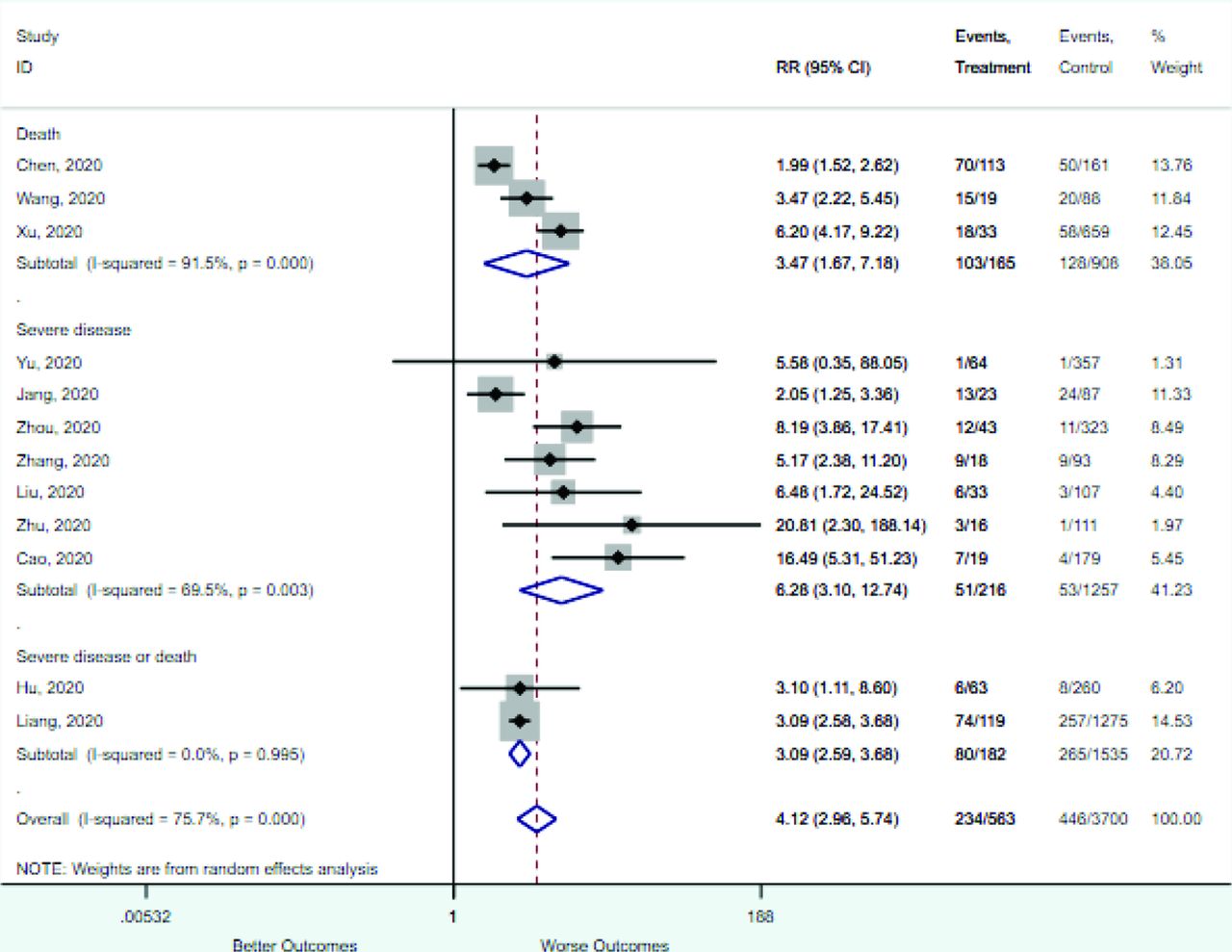
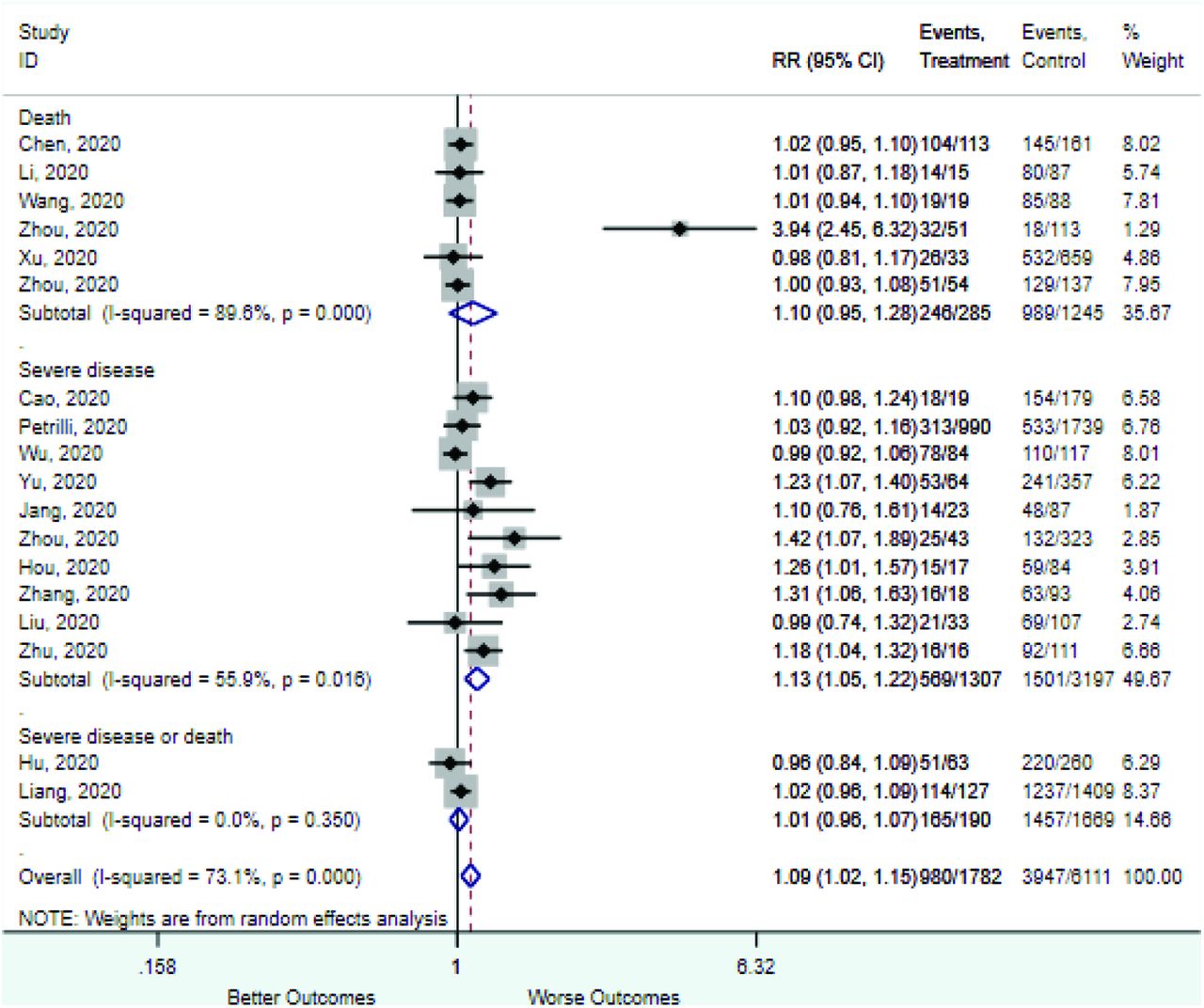
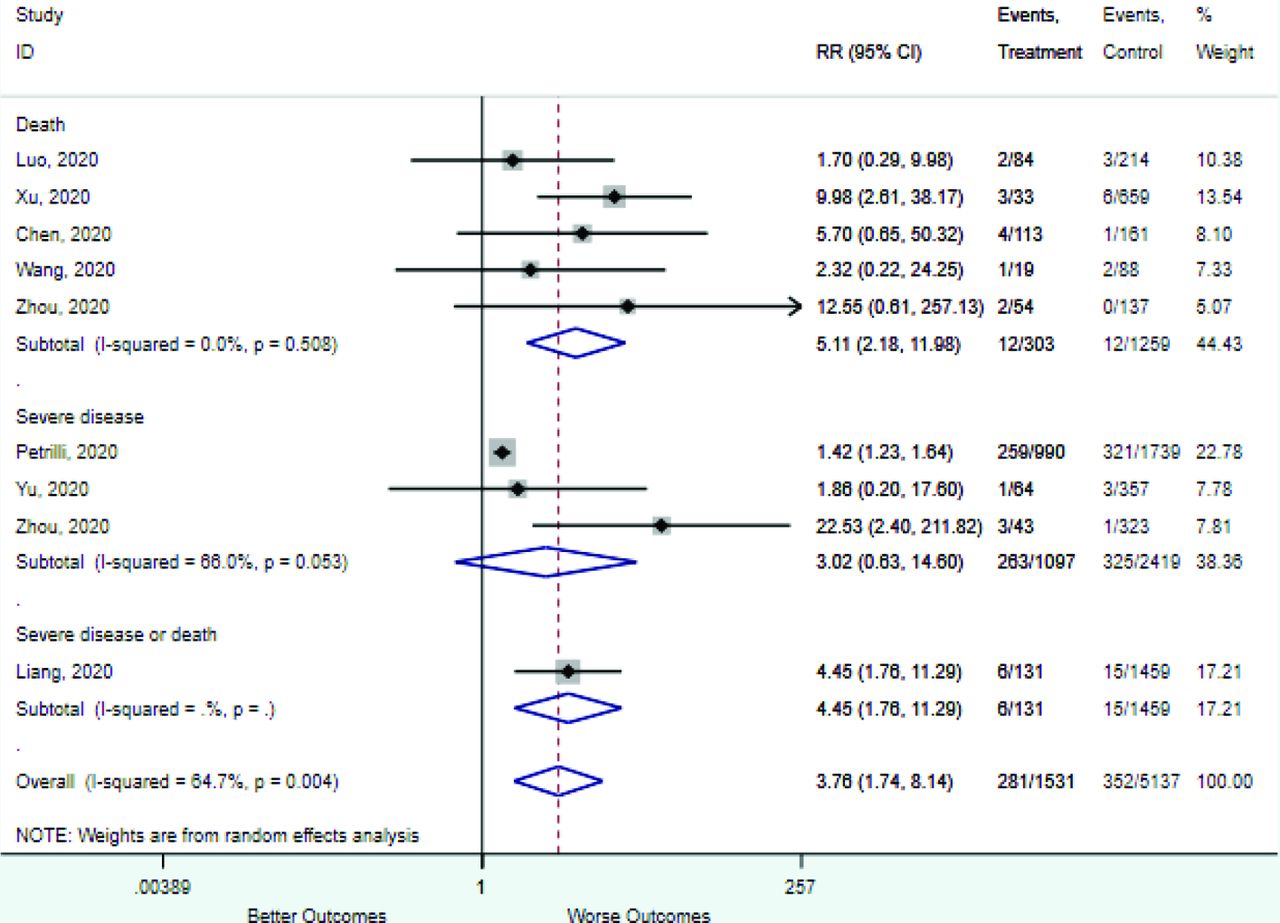
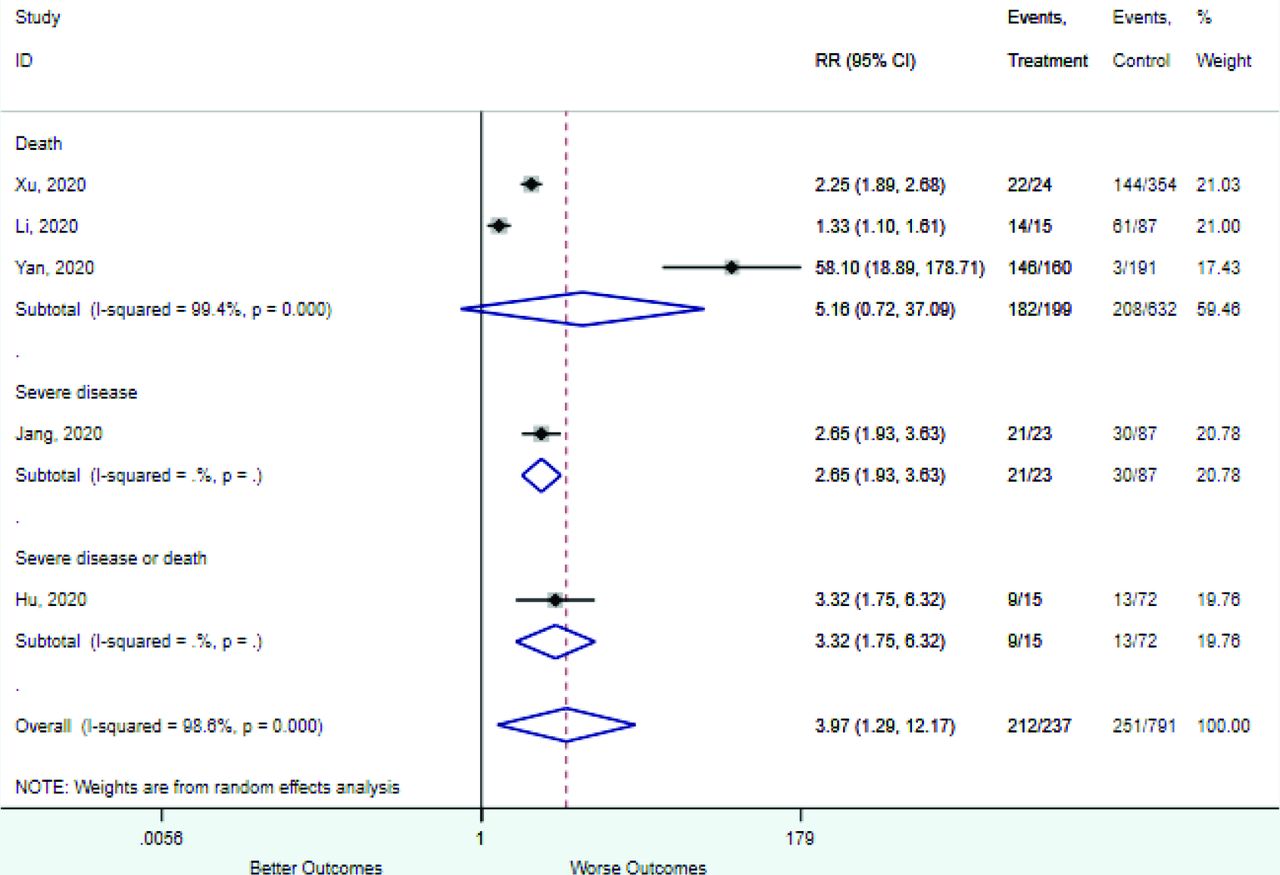
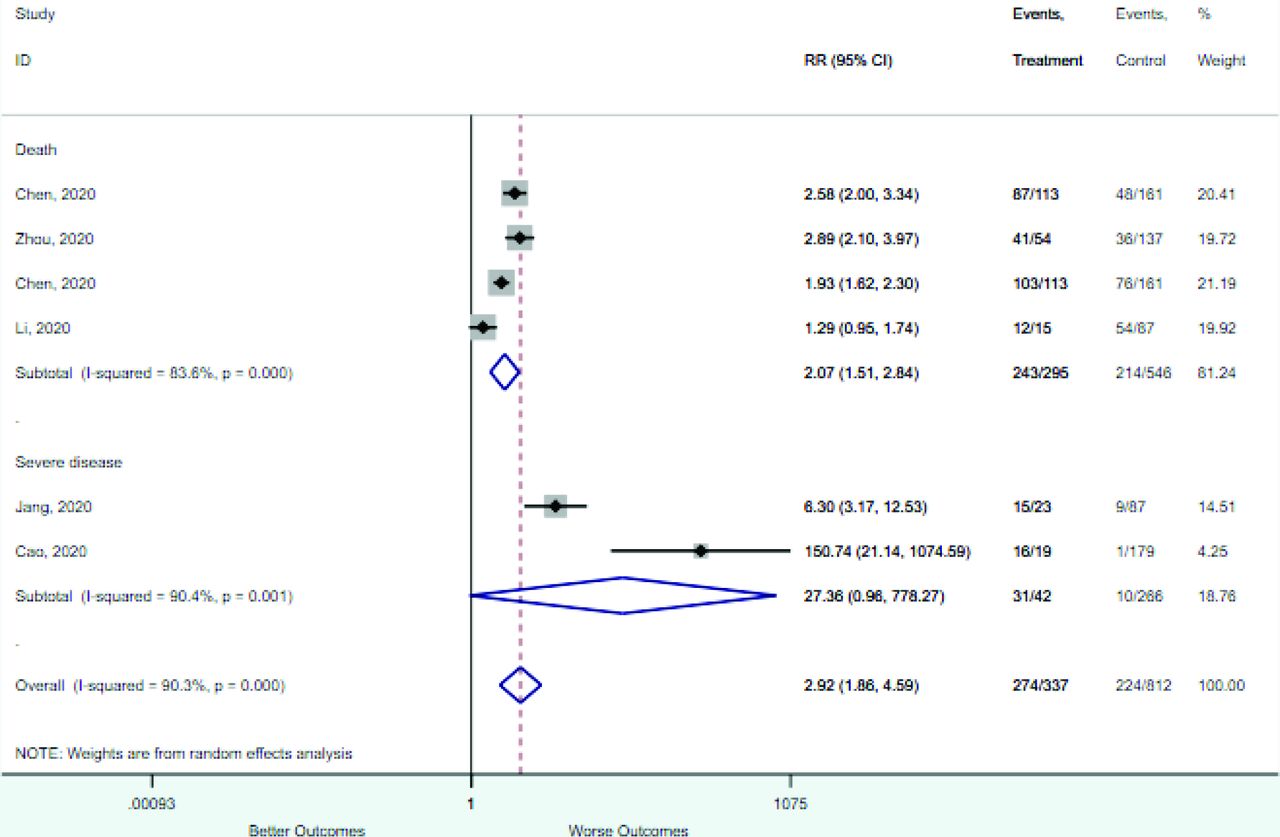
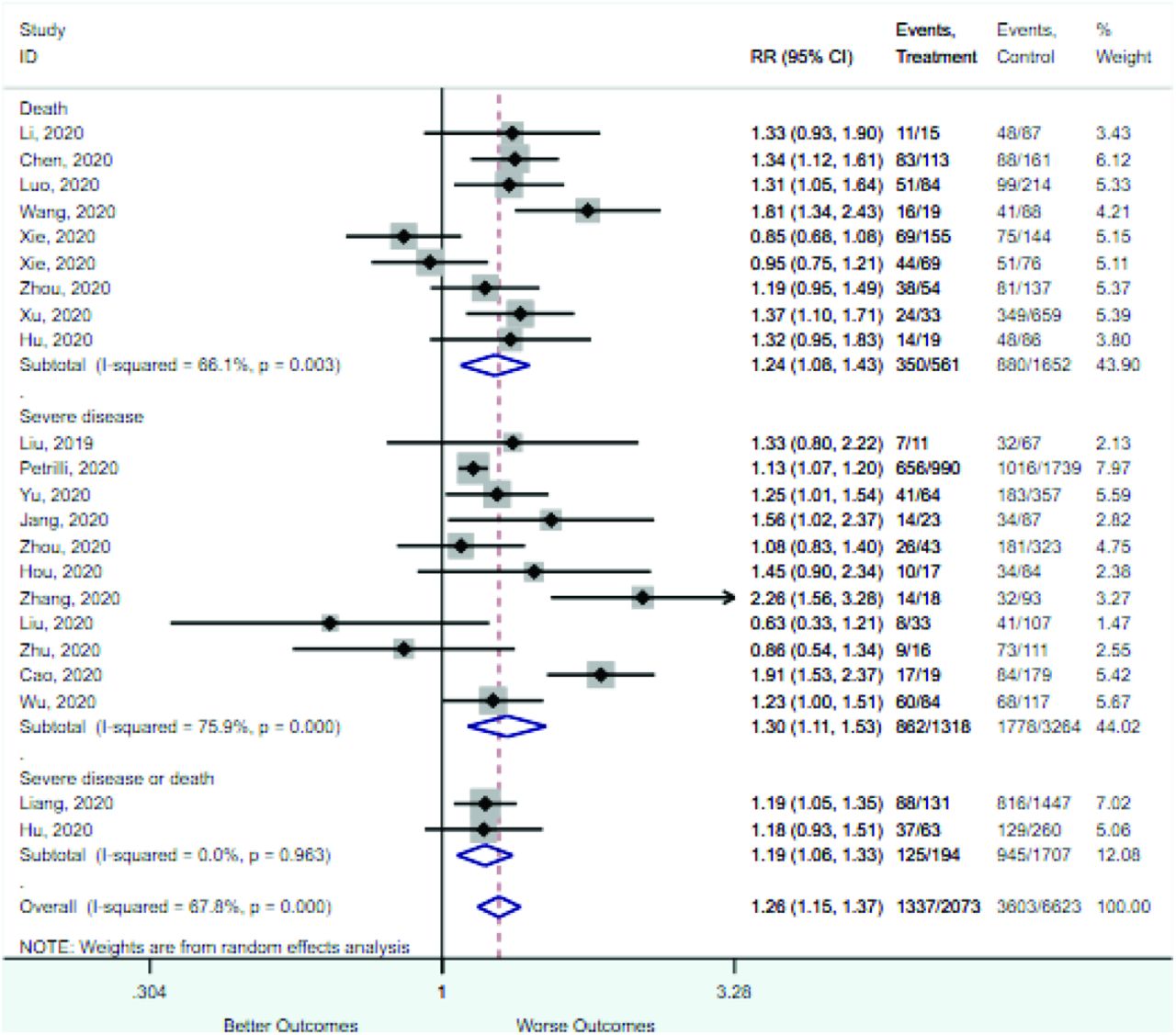
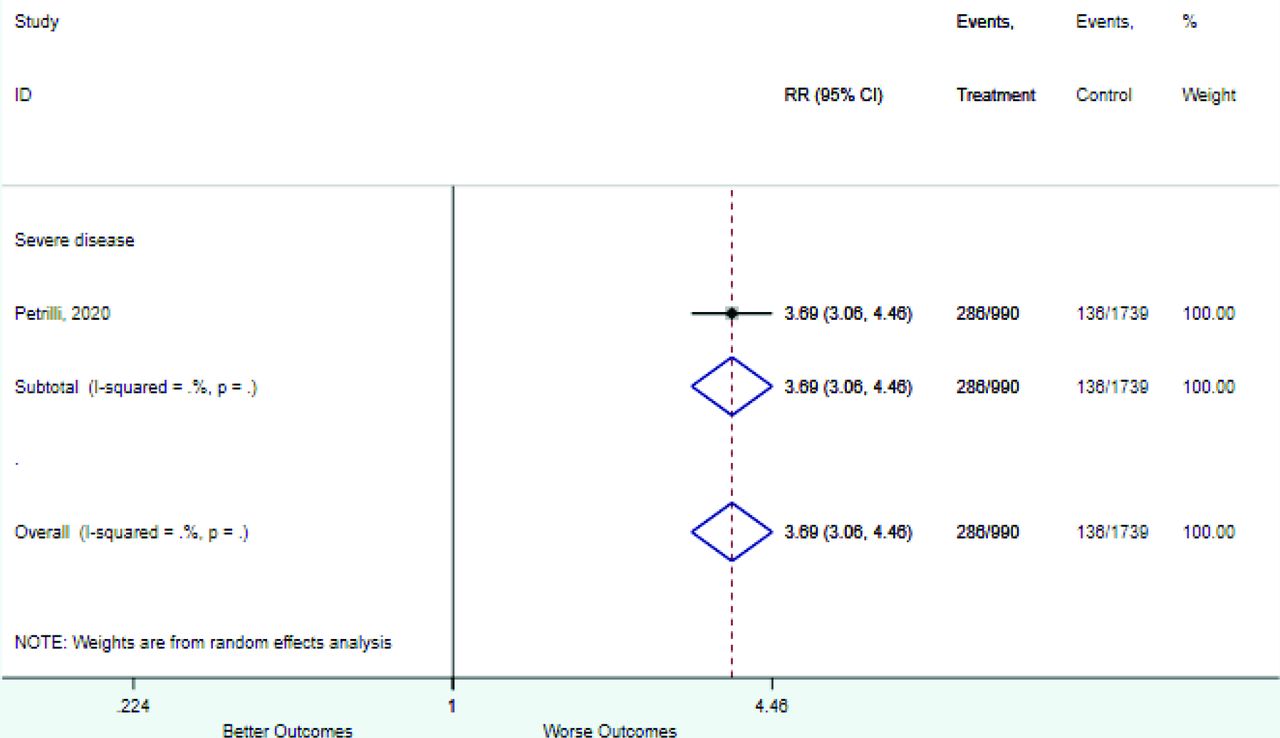
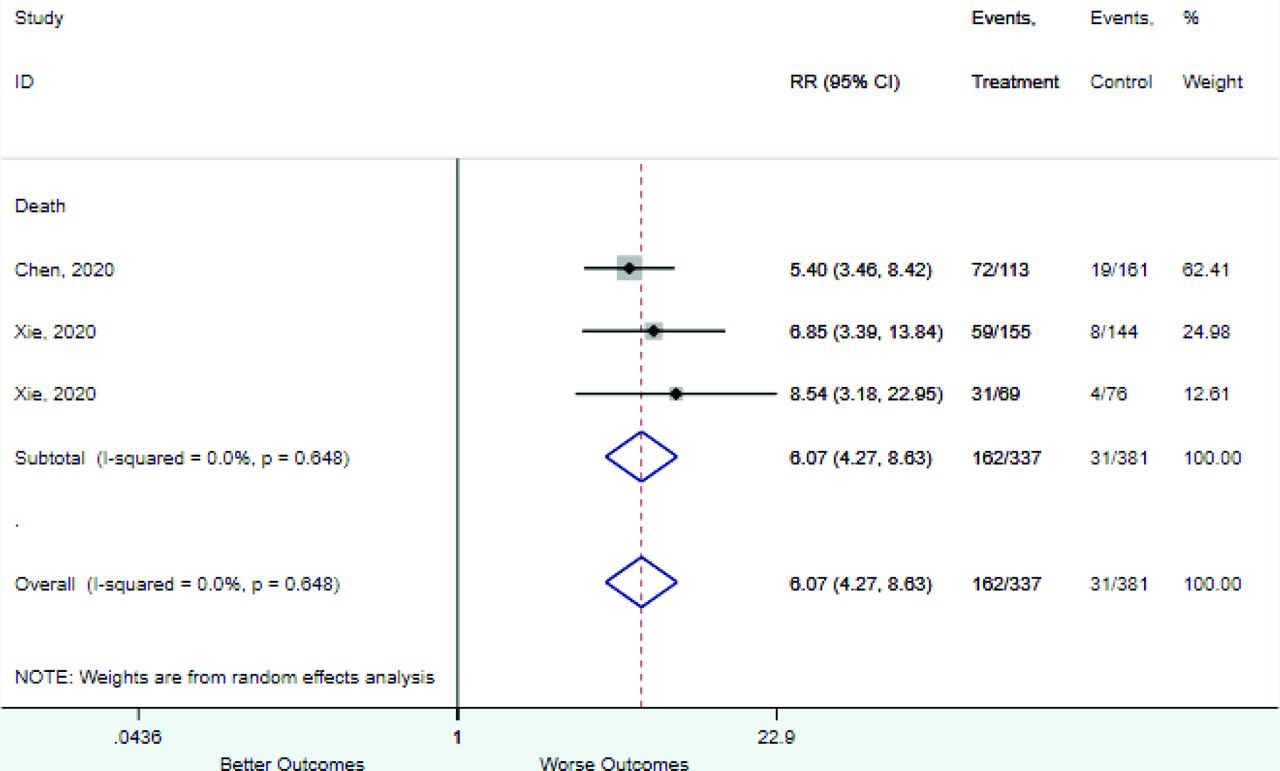
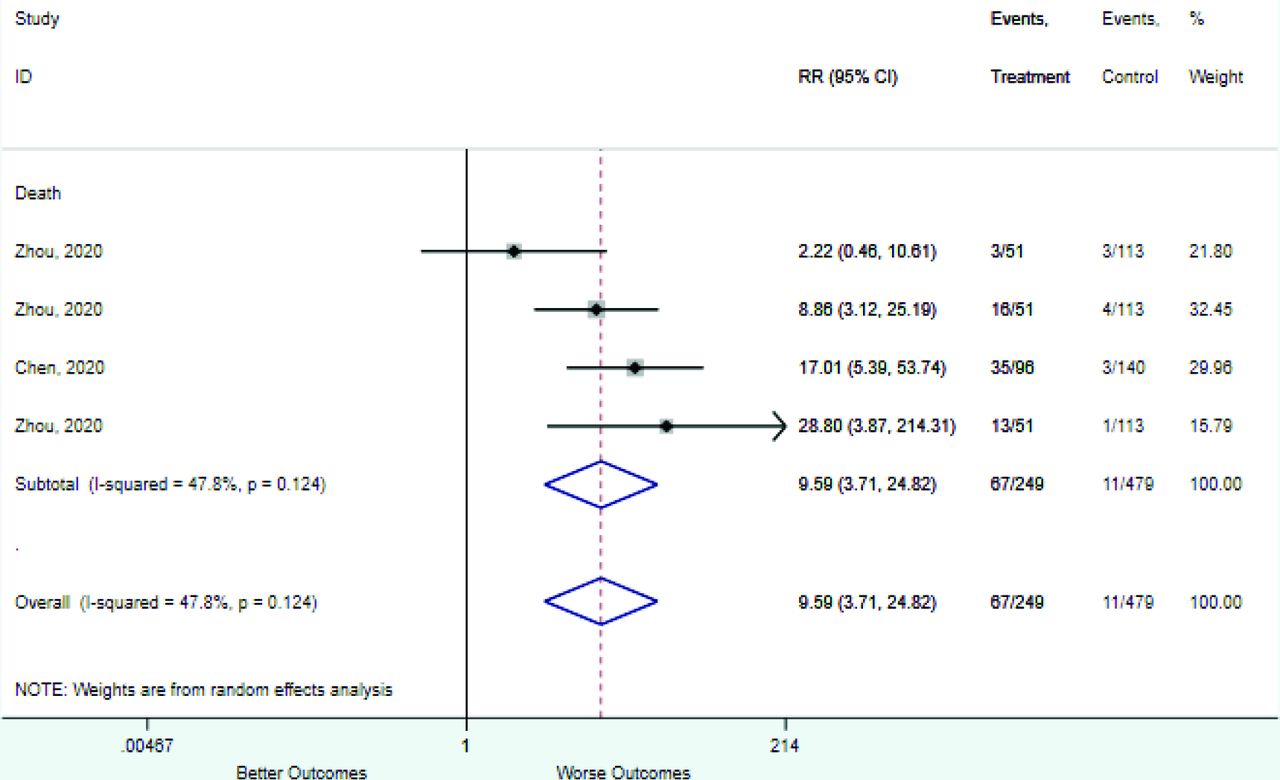
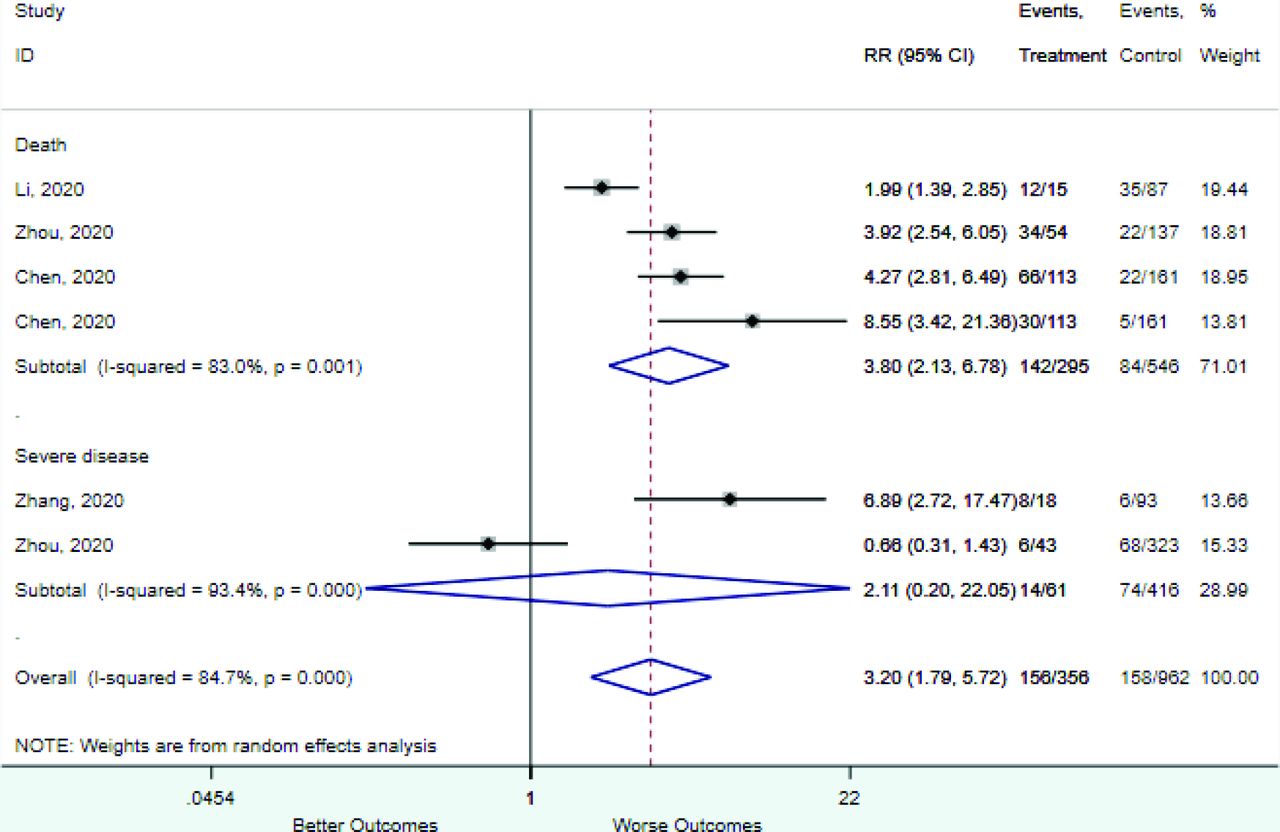
Variables Studies Total Patients RR (95% CI) Outcome = death Demographics and vital signs Oxygen saturation < 90% to 93% 3 718 6.07 (4.27–8.63) Respiratory rate >20 to 30 breaths/min 4 841 3.80 (2.13–6.78) Age ≥60 to 65 years 3 483 2.62 (1.91–3.58) Male sex 9 2213 1.24 (1.08–1.43) Comorbidities Coronary heart disease 9 2213 5.27 (2.89–9.58) Chronic kidney disease 5 1562 5.11 (2.18–12.0) Chronic obstructive pulmonary disease 9 2213 3.79 (2.51–5.72) Hypertension 9 2213 2.34 (1.80–3.05) Diabetes mellitus 9 2213 2.15 (1.46–3.15) Symptoms Dyspnea 3 1073 3.47 (1.67–7.18) Fever 6 1530 1.10 (0.95–1.28) Cough 5 1366 1.02 (0.93–1.13) Laboratory tests Procalcitonin ≥0.25 to 0.5 ng/mL 4 728 9.59 (3.71–24.8) Increased LDH 3 831 5.16 (0.72–37.09) D-dimer ≥1.0 mg/L 4 718 2.56 (2.10–3.13) D-dimer ≥0.5 mg/L 3 569 1.54 (1.32–1.80) D-dimer 0.5-1.0 mg/L 4 718 0.45 (0.31–0.64) D-dimer ≤0.5 mg/L 4 718 0.19 (0.12–0.30) Lymphocyte count < 0.8 to 1.1 × 109/mL 4 841 2.07 (1.51–2.84) WBC ≥4 × 109/mL 3 567 1.07 (0.81–1.41) WBC < 3.5 - 4 × 109/mL 3 567 0.34 (0.20–0.56) WBC 4 to 10 × 109/mL 3 567 0.65 (0.54–0.78) Outcome = severe disease Male sex 11 4582 1.30 (1.11–1.53) Comorbidities Coronary heart disease 9 4364 3.69 (1.75–7.77) Chronic kidney disease 3 3516 3.02 (0.63–14.6) Diabetes mellitus 11 4582 2.57 (1.59–4.17) Chronic obstructive pulmonary disease 7 1033 2.47 (1.34–4.52) Hypertension 11 4582 2.29 (1.61–3.26) Symptoms Dyspnea 7 1473 6.28 (3.10–12.7) Fever 10 4504 1.13 (1.05–1.22) Cough 9 1775 1.11 (0.87–1.42) Laboratory tests Procalcitonin >0.05 ng/mL 3 448 4.06 (0.65–25.3) C-reactive protein >5 to 0 mg/L 3 448 1.68 (1.47–1.93) Variables reported by fewer than 3 studies are not included but can be found online.
RR, risk ratio; CI, confidence interval.
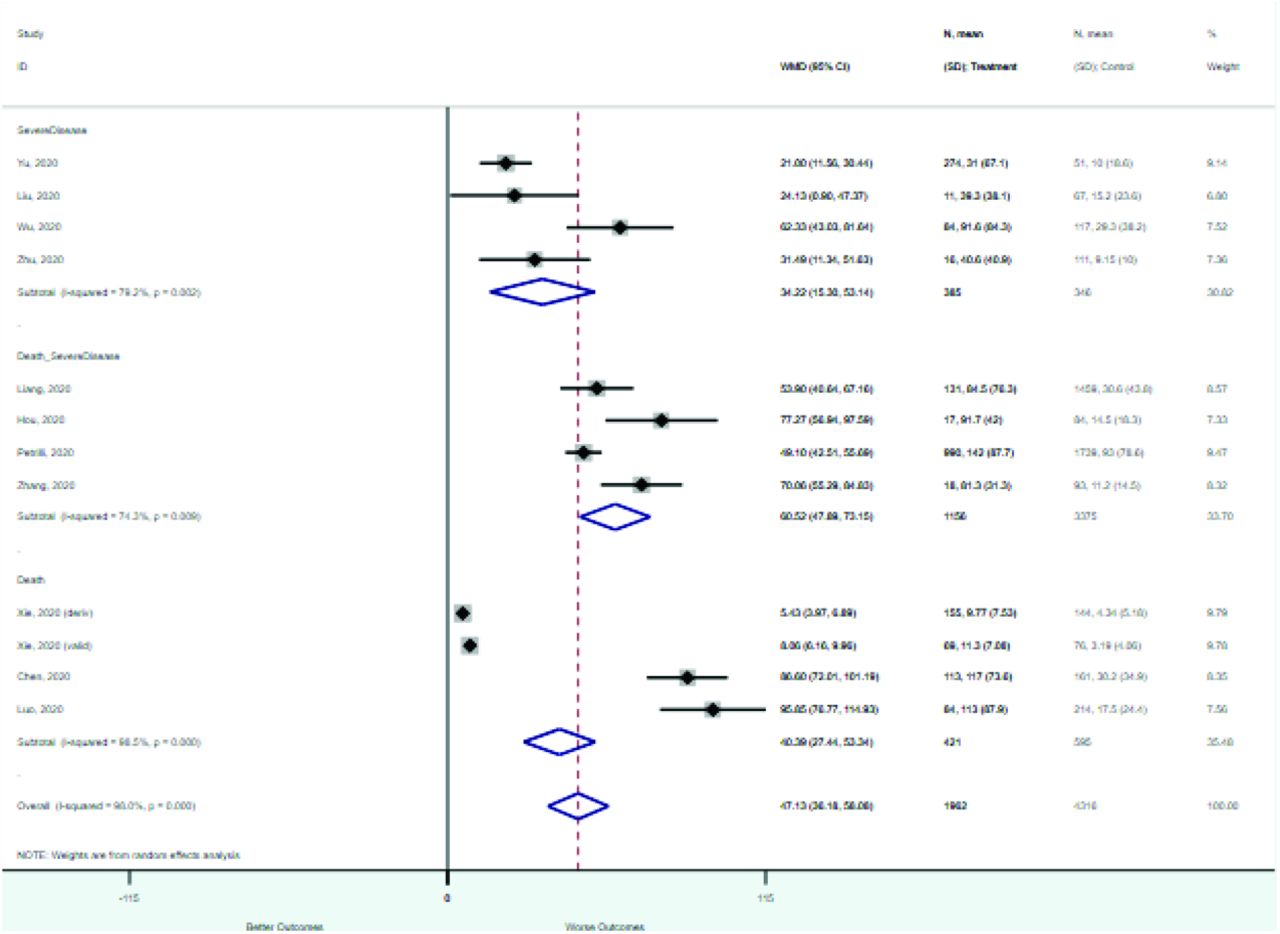
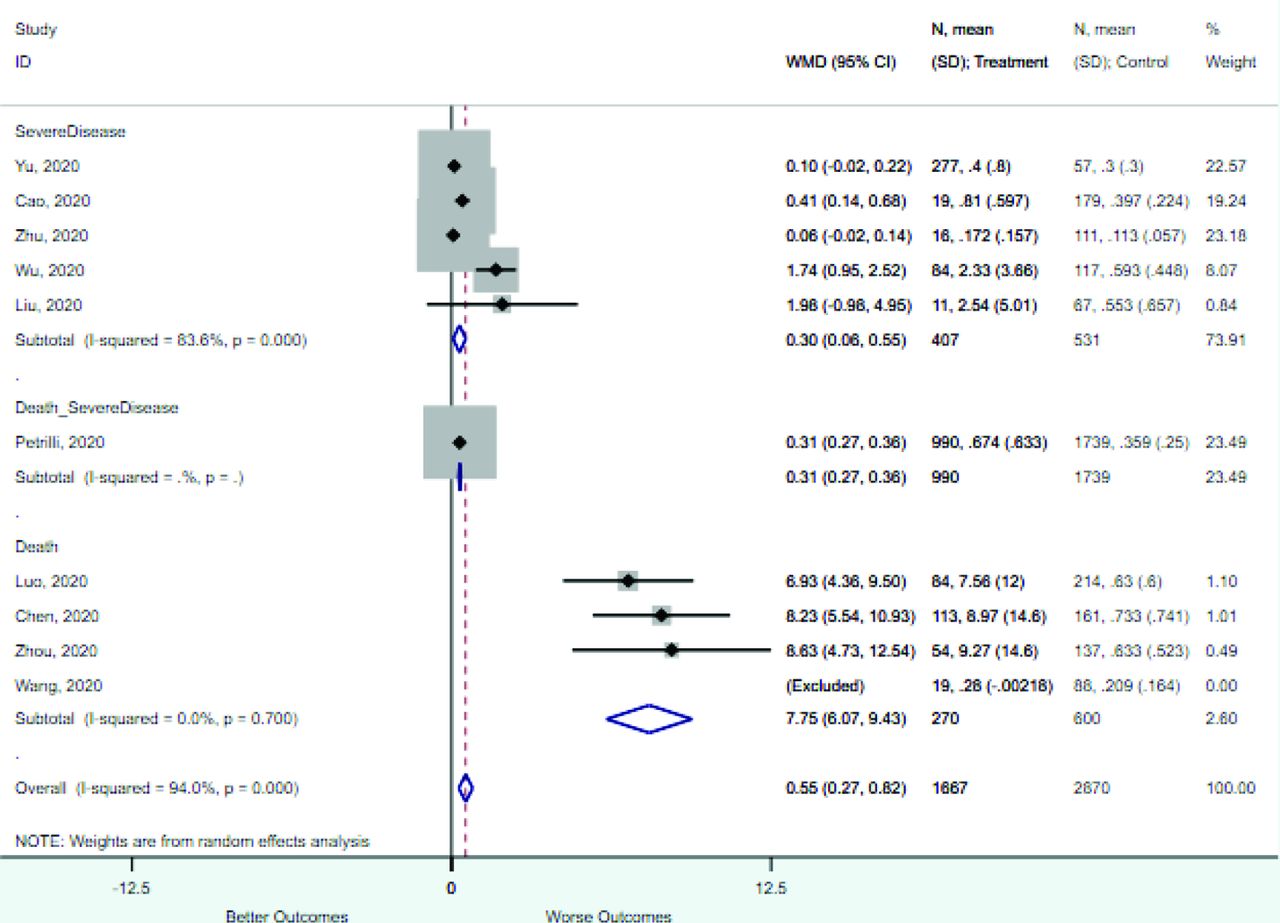
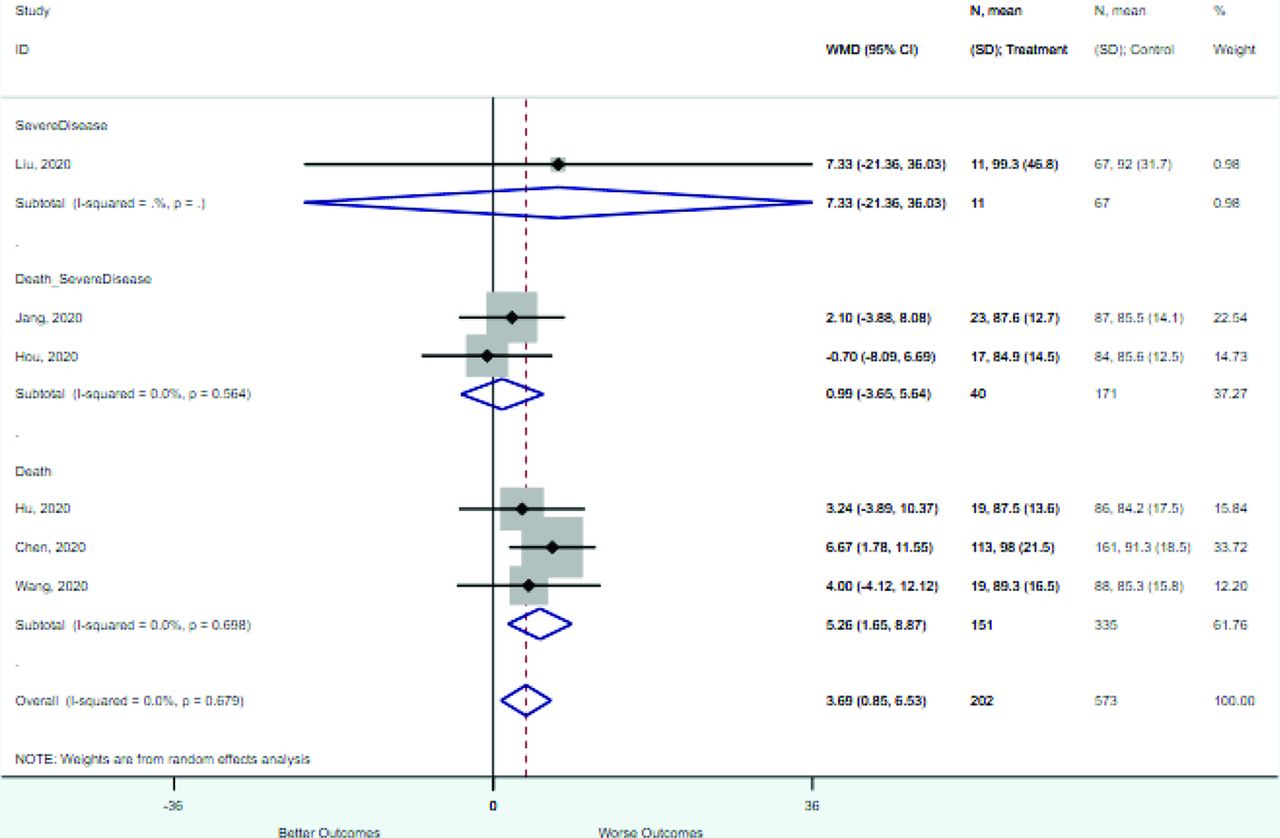
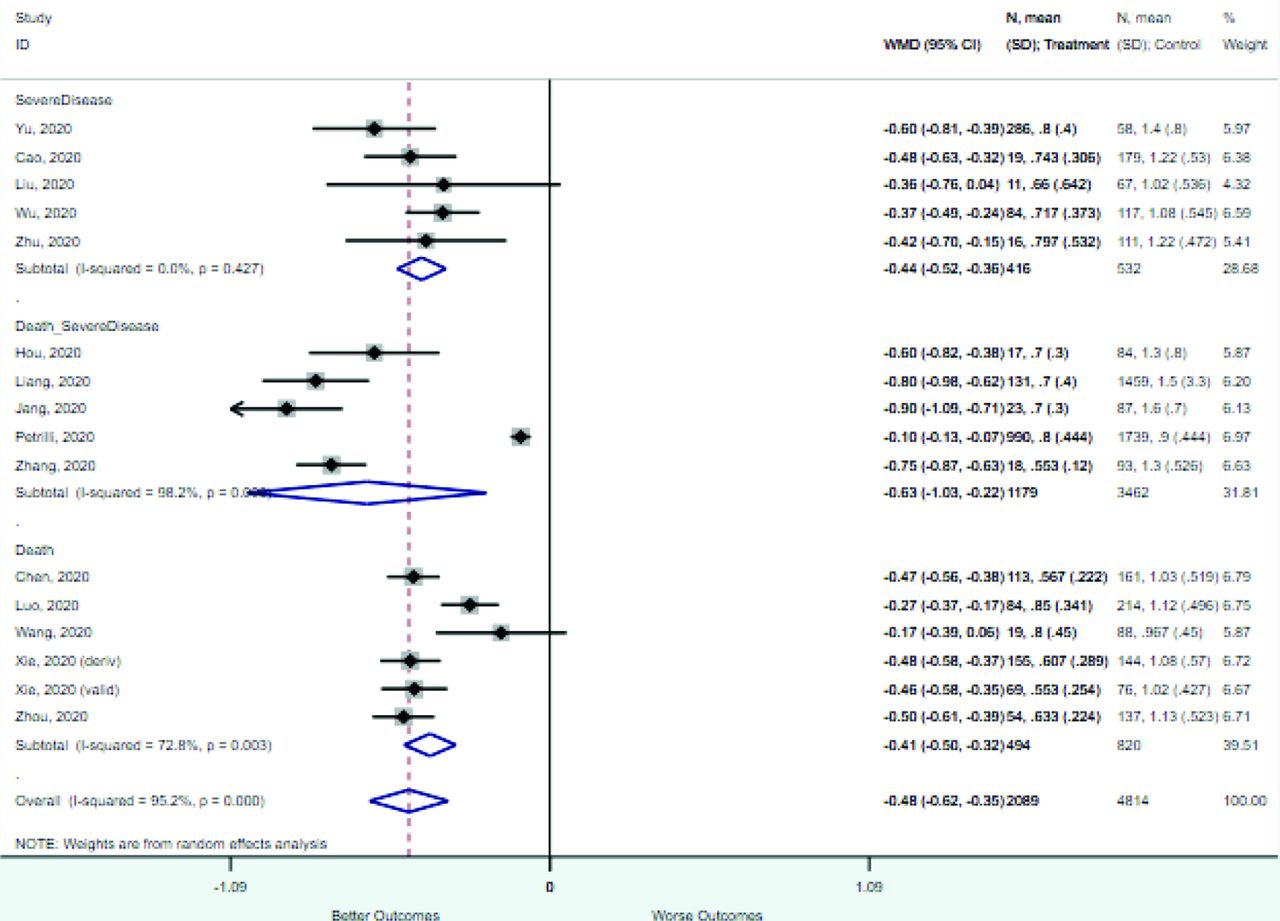
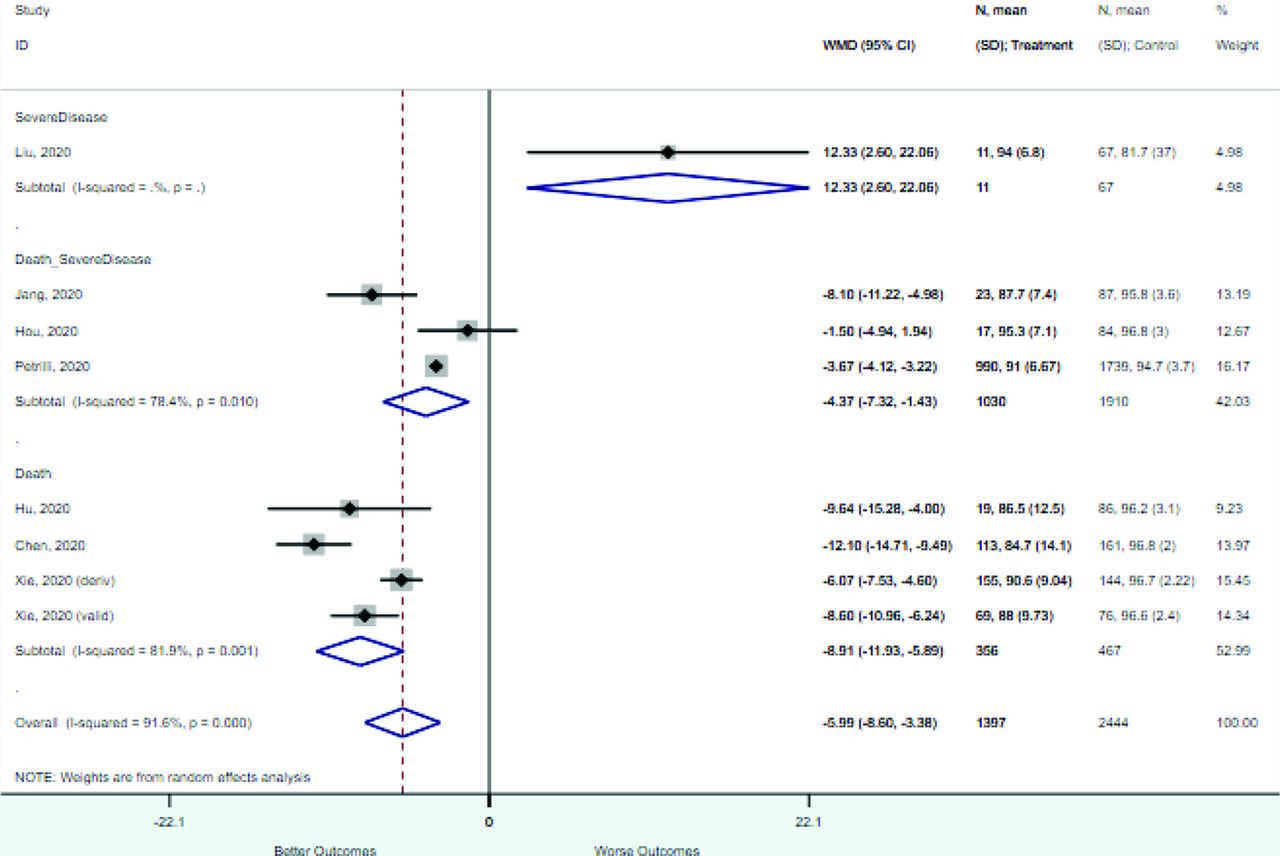
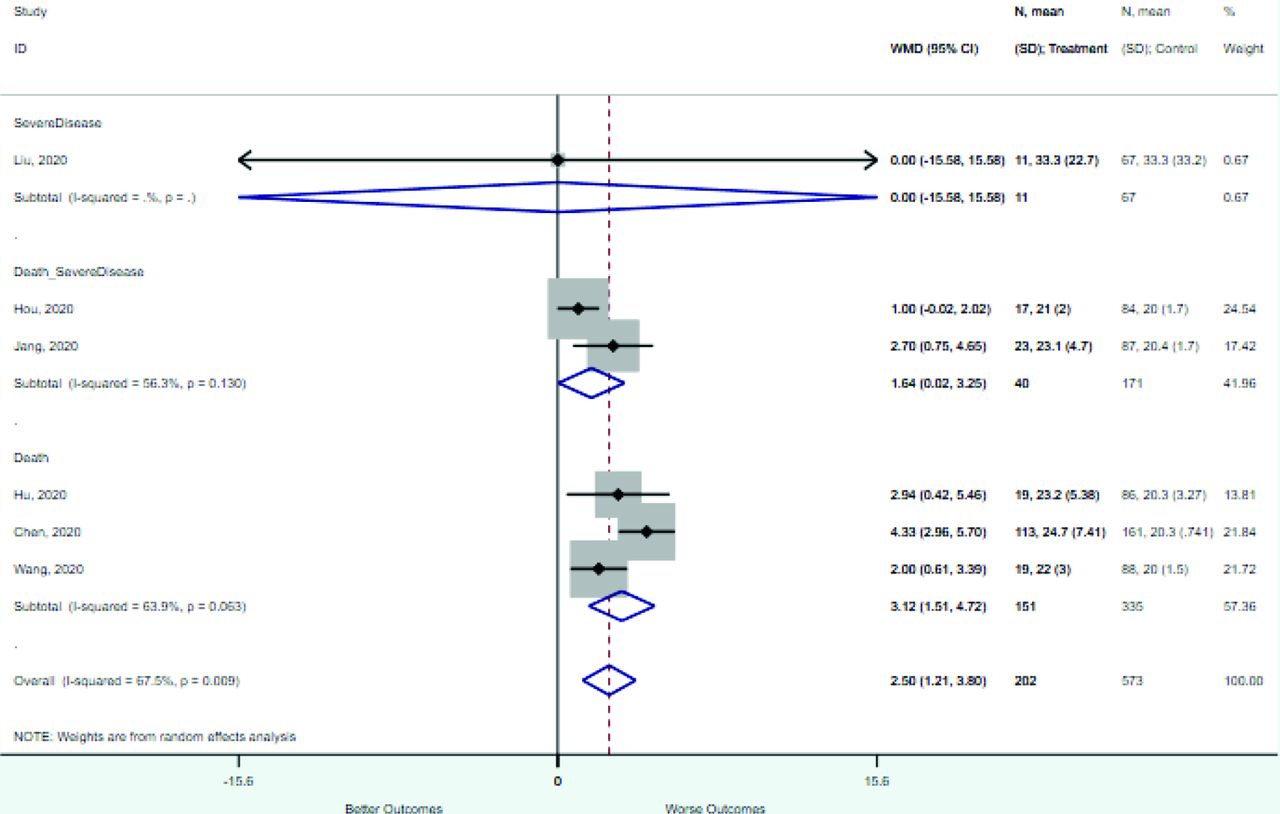
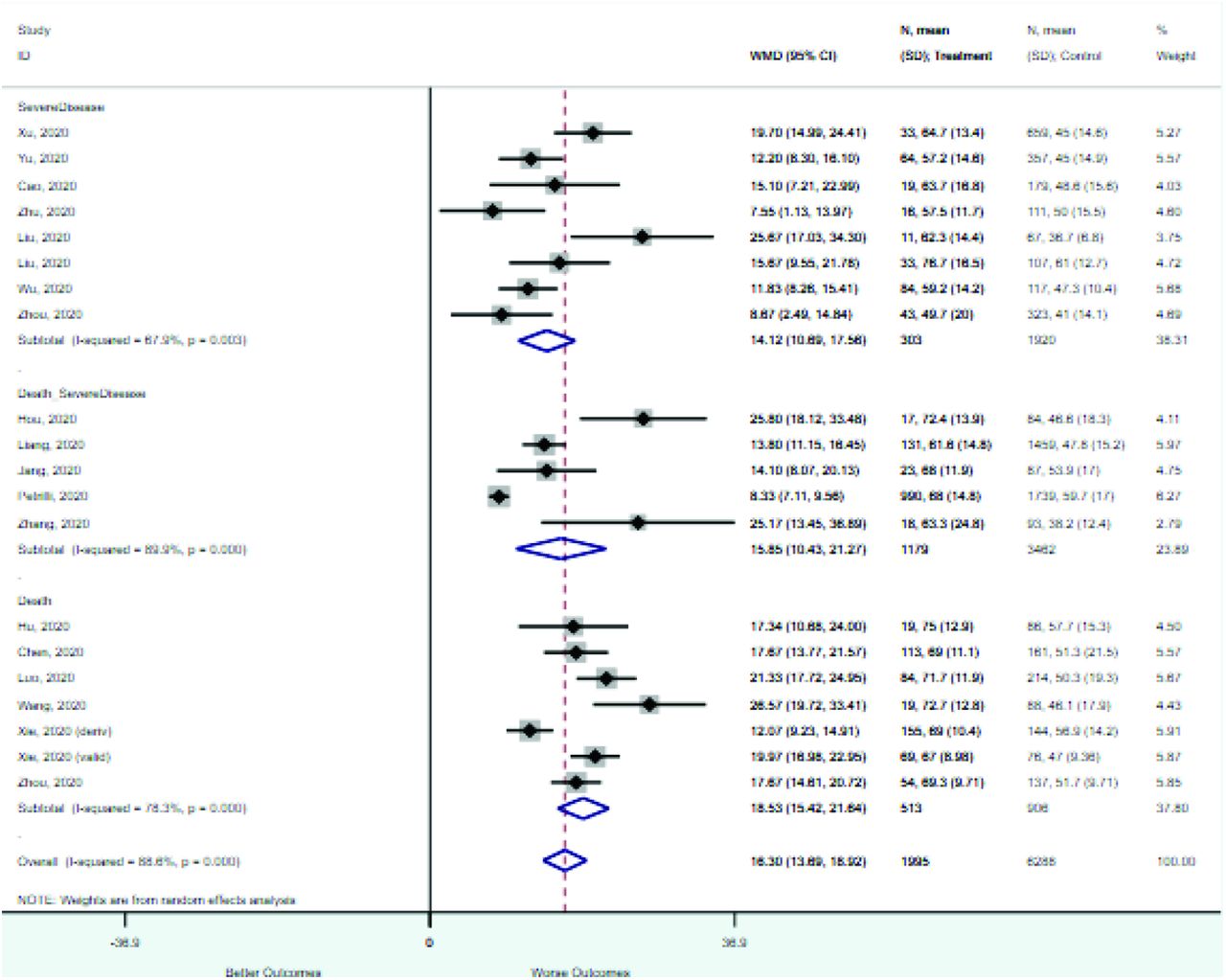
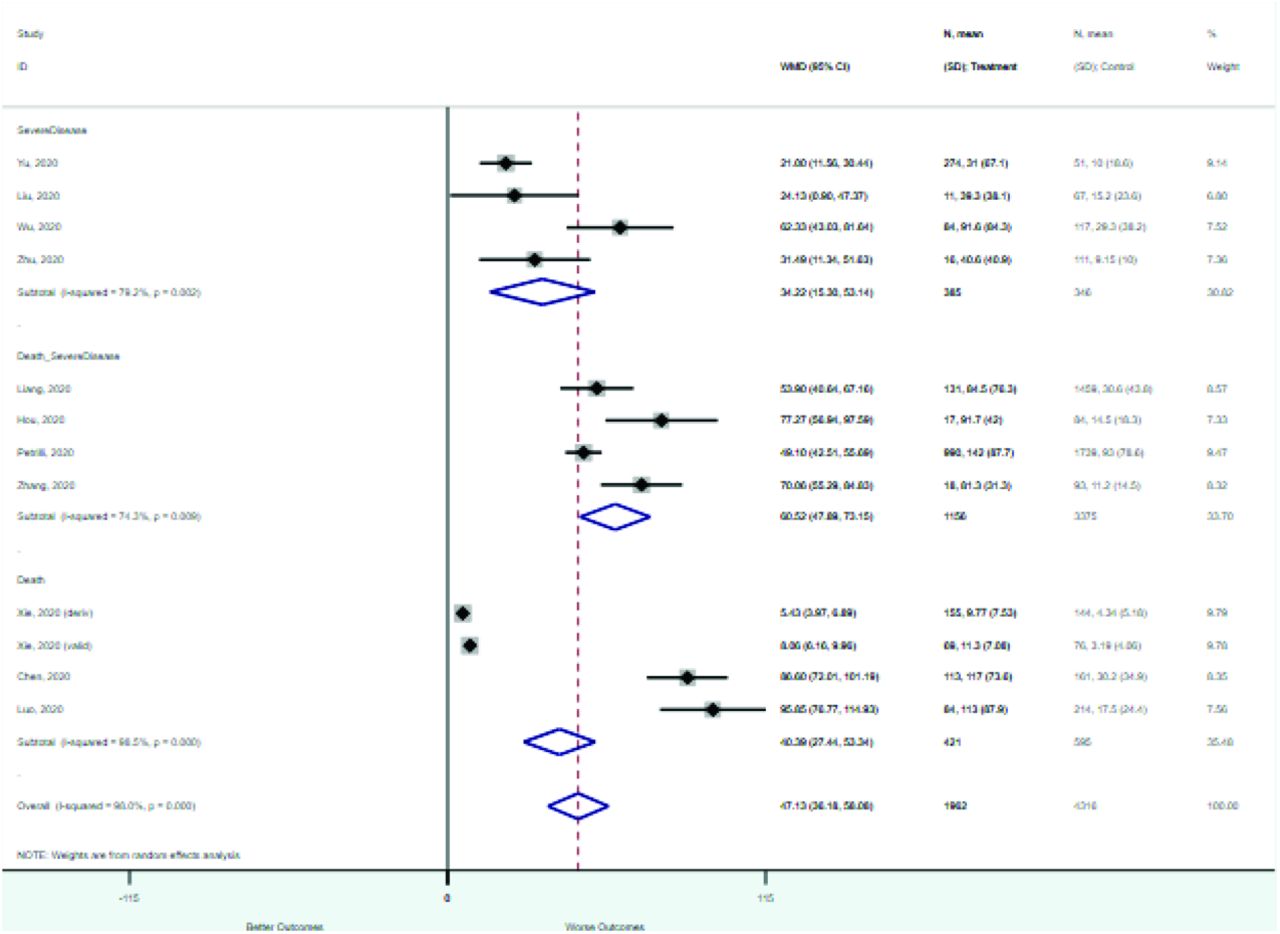
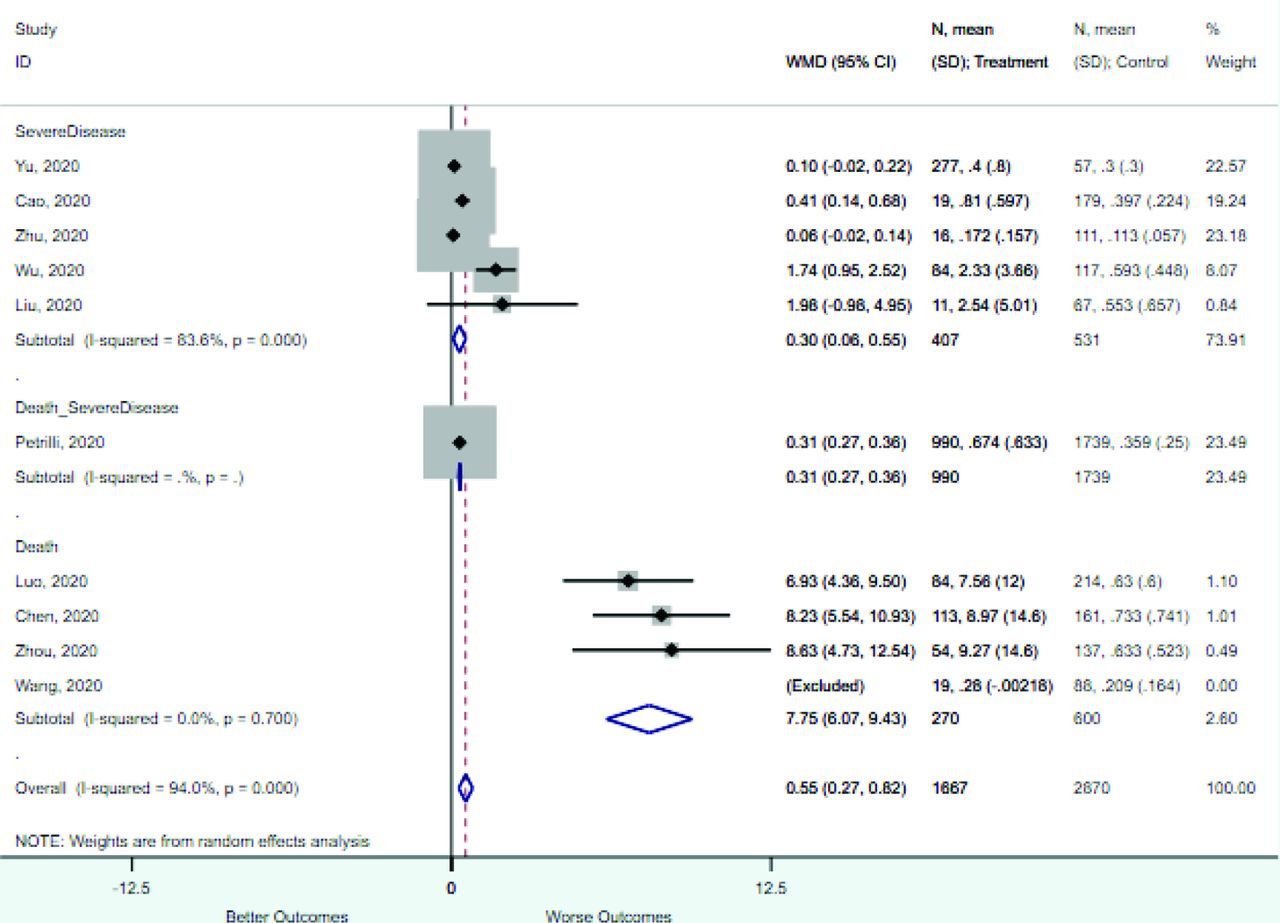
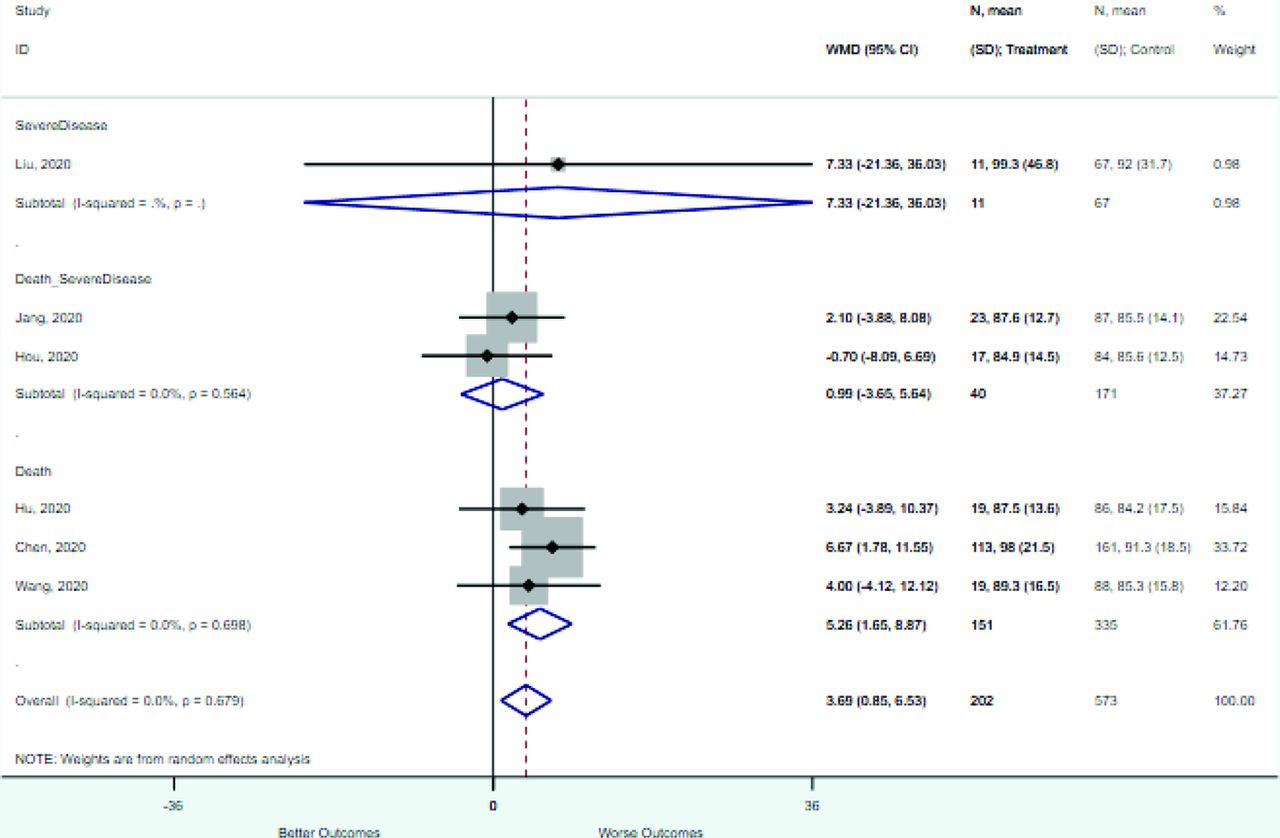
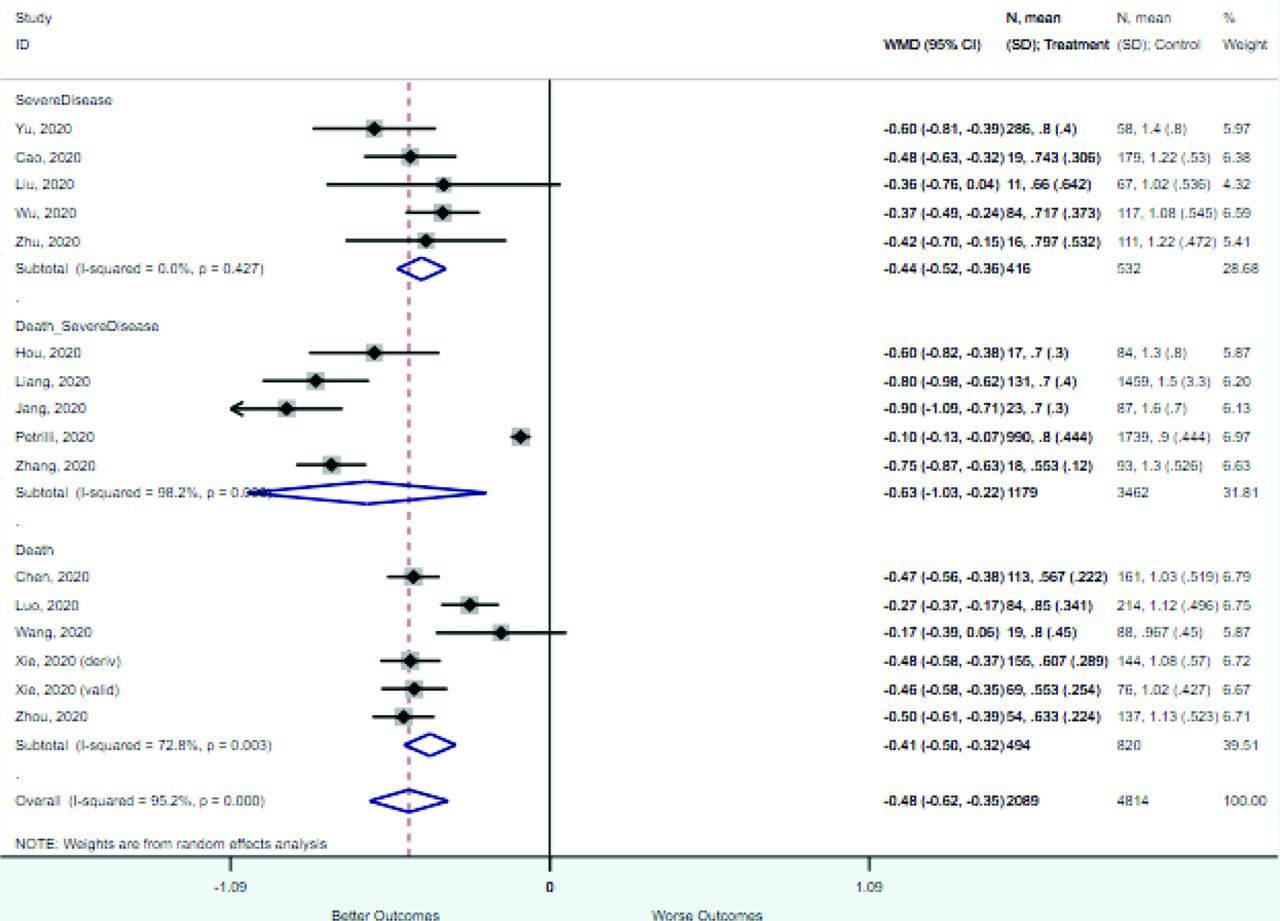
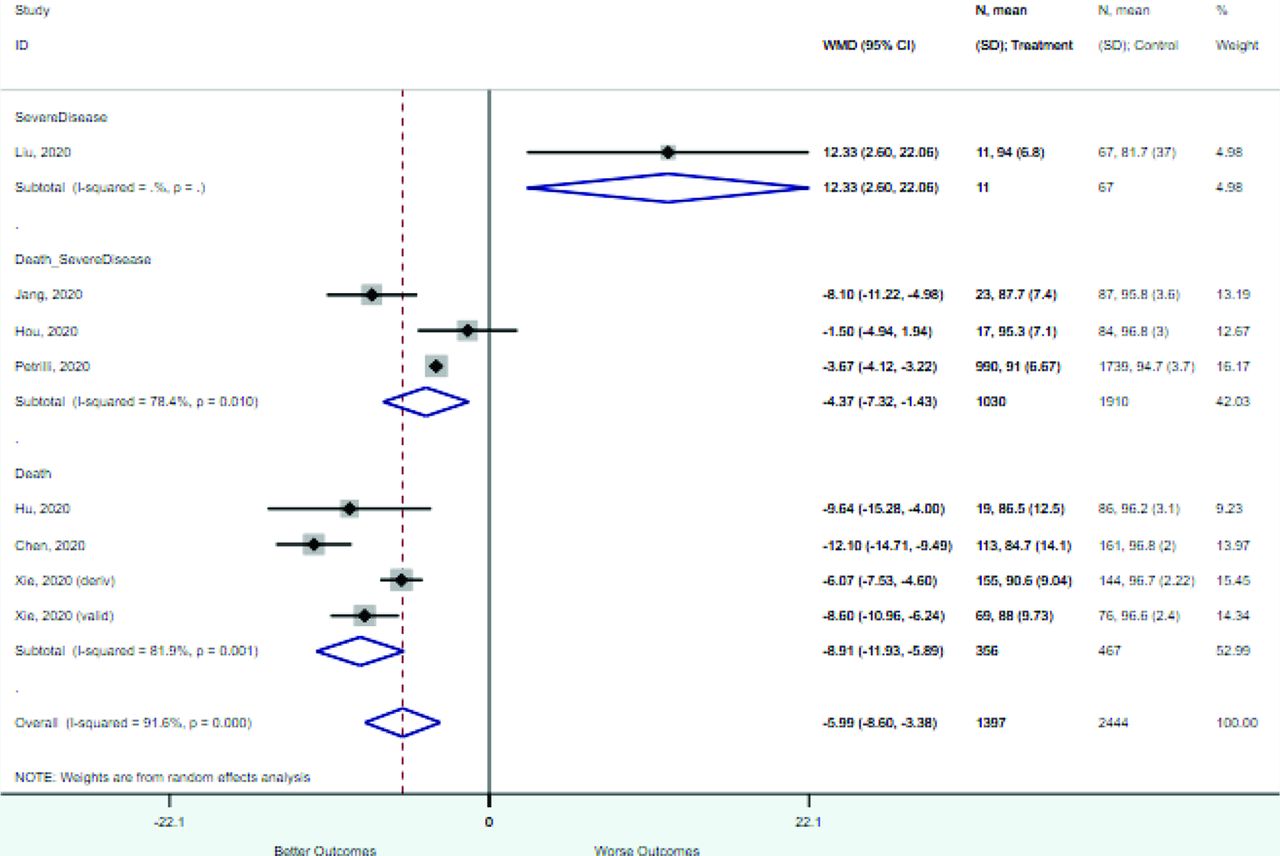
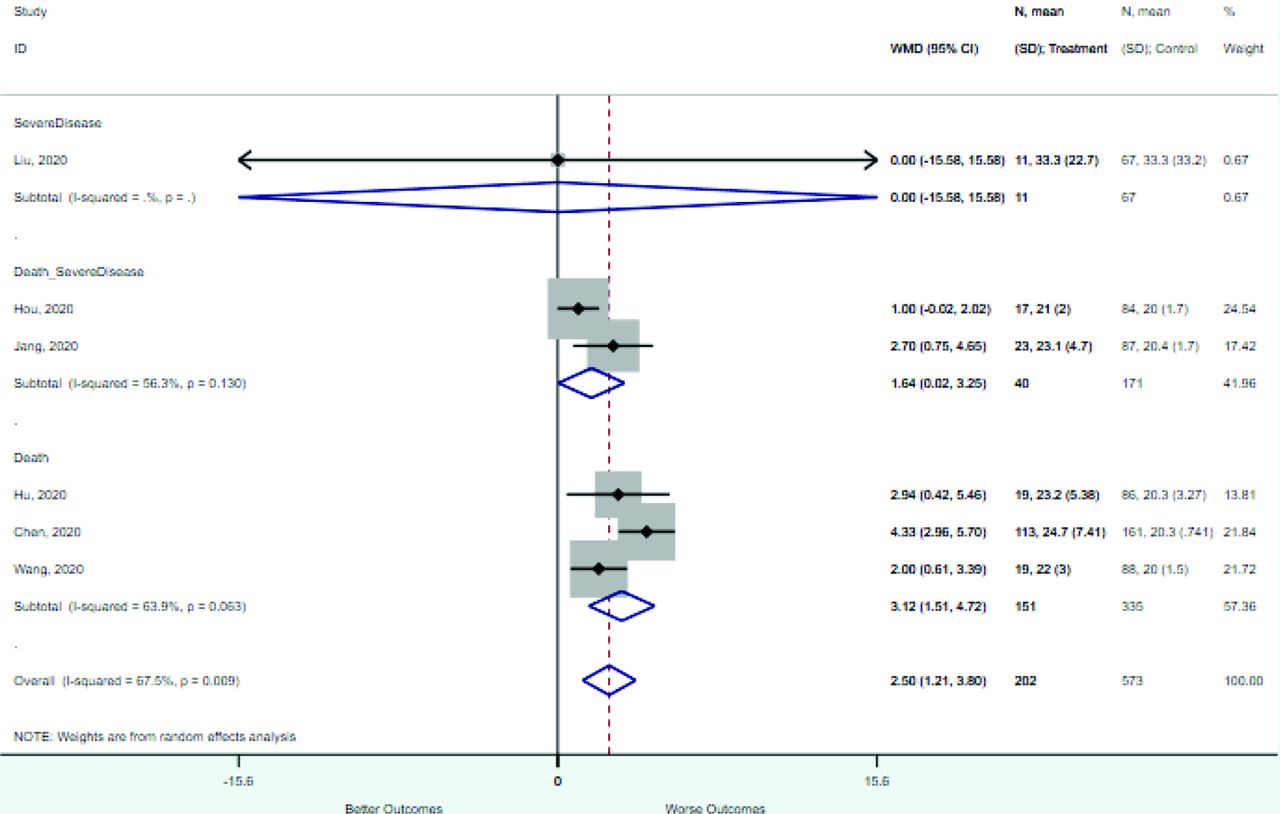
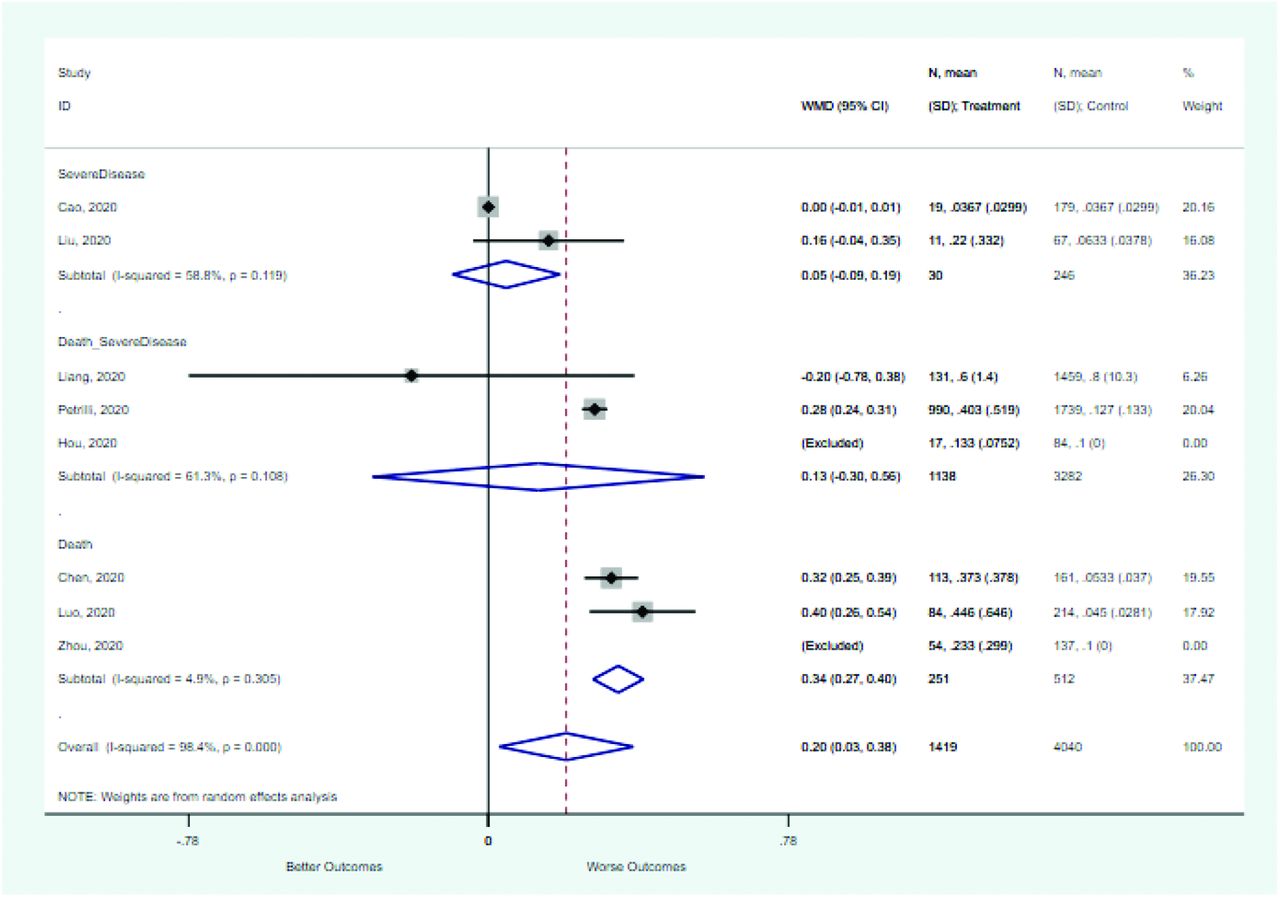
Risk Factor Studies Patients WMD (95% CI) Outcome = death CRP (mg/L) 4 1016 40.4 (27.4–53.3) Age (years) 7 1418 18.5 (15.4–21.6) D-dimer (mg/L) 4 870 7.8 (6.1–9.4) Heart rate (beats/minute) 3 486 5.3 (1.7–8.9) Neutrophil count (×109/mL) 3 679 4.3 (2.7–5.8) WBC count (×109/mL) 6 1314 4.0 (3.4–4.6) Respiratory rate 3 486 3.1 (1.5–4.7) Procalcitonin (ng/mL) 3 763 0.34 (0.27–0.40) Oxygen saturation (%) 4 823 −8.9 (−11.9 to −5.9) Lymphocyte count (×109/mL) 6 1314 −0.41 (−0.50 to −0.32) Outcome = severe disease CRP (mg/L) 4 731 34.2 (15.4–53.1) Age (years) 8 2223 14.1 (10.9–17.6) Neutrophil count (×109/mL) 5 752 0.94 (−0.42 to –2.3) WBC count (× 109/mL) 5 954 0.73 (−0.63 to 2.1) D-dimer (mg/L) 5 604 0.30 (0.06–0.55) Lymphocyte count (×109/mL) 5 948 −0.44 (−0.52 to −0.36) Outcome = severe disease or death CRP (mg/L) 4 4531 60.5 (47.9–73.2) Age (years) 5 4641 15.9 (10.4–21.3) Neutrophil count (×109/mL) 4 1912 2.6 (2.1–3.2) WBC count (×109/mL) 3 322 2.0 (0.98–3.0) Procalcitonin (ng/mL) 3 4420 0.13 (−0.30 to 0.56) Oxygen saturation (%) 3 2940 −4.4 (−7.3 to −1.4) Lymphocyte count 5 4641 −0.63 (−1.0 to −0.22) Variables reported by fewer than 3 studies are not included but can be found in the online Appendix B.
WMD, weighted mean differences; WBC, white blood count; CRP, c-reactive protein.
- Table 4.
Summary of Variables Included in Multivariate Models to Predict an Adverse Prognosis for COVID-19
Variable Zhang, 2020 (J Clin Virol) Zhou, 2020 (PLOS One) Xu, 2020 (Theranostics) Liu, 2020 (J Clin Virol) Jang, 2020 (JKMS) Hou, 2020 (Infect Dis) Yu et al, 2020 (Theranostics) Wang, 2020 (Crit Care) Zhou, 2020 (Lancet) Liu, 2020 (Chin Med J) Liang, 2020 (JAMA Intern Med) Xie, 2020 (medRxIV) Yan, 2020 (medRxiv) Hu, 2020 Luo, 2020 (Clin Infect Dis) Petrilli, 2020 (BMJ) Li, 2020 Number of Models Including This Variable Demographics Age (increasing) x x x x x x x x x x x 11 Male sex x x 2 Vital signs Temperature (elevated) x x x 3 Oxygen saturation (decreased) x x 2 Comorbidities Presence of comorbidities x x x 3 Diabetes mellitus x x 2 Tobacco use x x 2 History of cancer x x 2 Hypertension x 1 Cardiovascular disease x 1 Heart failure x 1 Chronic liver disease x 1 Chronic kidney disease x 1 Use of hypnotic x 1 Symptoms Dyspnea x x 2 Cough x 1 Hemoptysis x 1 Loss of consciousness x 1 Laboratory results C-reactive protein (elevated) x x x x x x x 7 Lymphocyte count (decreased) x x x x x x 6 Lactate dehydrogenase (increased) x x x x 4 WBC count (increased) x x 2 Neutrophil count (increased) x x 2 Troponin (increased) x x 2 Procalcitonin (increased) x x 2 D-dimer (increased) x x 2 Interleukin-6 >32.1 pg/mL x 1 CK-MB (elevated) x 1 Albumin (decreased) x 1 Neutrophil/lymphocyte ratio x 1 Direct bilirubin (increased) x 1 Serum creatinine (increased) x 1 WBC, white blood count; CK-MB, creatine kinase-MB.
Study Predictor Variables Outcome Predicted Validation (Country) Type of CPR With Outcome Lu, 2020* Age, CRP Death Internal validation (China) Classification tree: Low: 0% mortality Mod: 6% mortality High: 33% mortality Xie, 2020 Age, LDH, lymphocytes, SpO2 Death External validation in 1 hospital (China) Probability assessment using full logistic model as nomogram Yan, 2020 LDH, CRP, lymphocytes Death Internal validation (China) Classification tree Yu, 2020 Age, sex, diabetes mellitus, lymphocytes, procalcitonin Death Internal validation (China) Risk score High risk (>3 points): 22.8% Low risk (≤3 points): 5.4%) Shi, 2020 Age, sex, hypertension Death or severe disease Internal validation (China) 0 factors: 0% 1 factor: 6% 2 factors: 19% 3 factors: 40% Galloway, 2020 Age, sex, race, oxygen saturation, chest radiograph, neutrophils, CRP, albumin, creatinine, diabetes mellitus, hypertension, chronic lung disease Death or critical care Internal validation (UK) Risk score High risk (≥4 points): 40.7% Low risk (<4 points): 12.4% Petrilli, 2020 Age, SpO2, procalcitonin, troponin, CRP, hypertension Severe disease Internal validation (US) Classification tree Liang, 2020 Age, neutrophil/lymphocyte ratio, LDH, direct bilirubin, chest radiograph, hemoptysis, dyspnea, unconsciousness, comorbidities, cancer Severe disease External validation in 3 hospitals (China) Logistic regression model requiring online calculator Zhou, 2020 Temperature, cough, dyspnea, hypertension, chronic liver disease, chronic kidney disease, cardiovascular disease Severe disease Internal validation (China) Nomogram Kaeuffer, 202020 Age, BMI, sex, dyspnea, neutrophil count, lymphocyte count, CRP Severe disease External validation Risk score: Low risk (≤6): 13% Moderate risk (6–14): NR High risk (>14): 66% Knight, 202021 Age, sex, number of comorbidities, respiratory rate, SpO2, level of consciousness, urea level, CRP Mortality External validation Risk score from 0 to 21 points Low risk (0–3): 1.2% Intermediate risk (4–8): 9.9% High risk (9–14): 31.4% Very high risk (≥15): 61.5% ↵* Study included some patients with suspected but not confirmed COVID-19. Preprint at MedRxIV: Lu J, et al. ACP risk grade: a simple mortality index for patients with confirmed or suspected severe acute respiratory syndrome coronavirus 2 disease (COVID-19) during the early stage of outbreak in Wuhan (https://doi.org/10.1101/2020.02.20.20025510).
CPR, clinical prediction rule; CRP, c-reactive protein; LDH, lactate dehydrogenase; BMI, body mass index.
Authors Study Participation Study Attrition Prognostic Factor Measurement Outcome Measurement Study Confounding Statistical Analysis and Reporting Yu et al, 2020 M L L L L L Wang, 2020 M L L L L L Chen, 2020 M H L L H L Zhou, 2020 M L L L L L Liu, 2020 M L L L L L Liang, 2020 M L L L L L Xie, 2020 M L L L L L Yan, 2020 M H L L L L Cao, 2020 M L L L H L Hu, 2020 M H L L L L Luo, 2020 M L L L L L Petrilli, 2020 M H L L L L Wu, 2020 M H L L H L Li, 2020 M H L L L L Jang, 2020 M L L L L L Xu, 2020 M H L L L L Zhou, 2020 M L L L L L Hou, 2020 M L L L L L Zhang, 2020 M H L L L L Liu, 2020 M L L L L L Zhu, 2020 M L L L L L Hu, 2020 M L L L L L L, low risk of bias; M, moderate risk of bias; H, high risk of bias.
Variables Study Participation Study Attrition Prognostic Factor Measurement Outcome Measurement Study Confounding Statistical Analysis and Reporting High risk of bias Specialized population (ie, pregnant, elderly) or subset of very ill patients only Incomplete outcome ascertainment (some patients still hospitalized) Unclear definition for prognostic factors Outcome not defined No multivariate analysis performed Selective reporting of results, no clear analytic strategy Moderate risk of bias Only inpatients Complete ascertainment but >10% loss to follow-up Post hoc selection of cut points Unclear definition Low risk of bias Inpatient and outpatient Complete ascertainment and <10% loss to follow-up Typical cutoffs used, clearly defined Clear and reproducible definition Multivariate analysis reported Full reporting, analytic strategy clearly described Association between categorical variables and mortality, severe disease, or both in patients with COVID-19
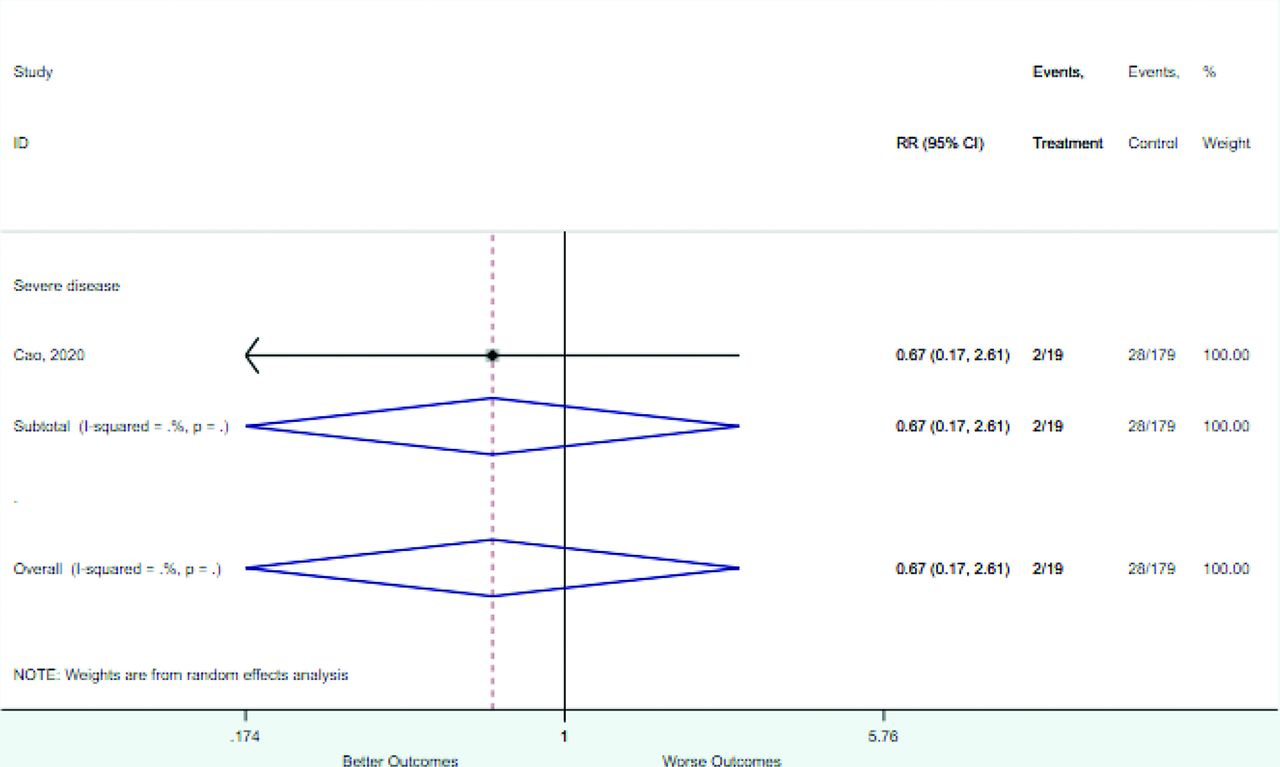
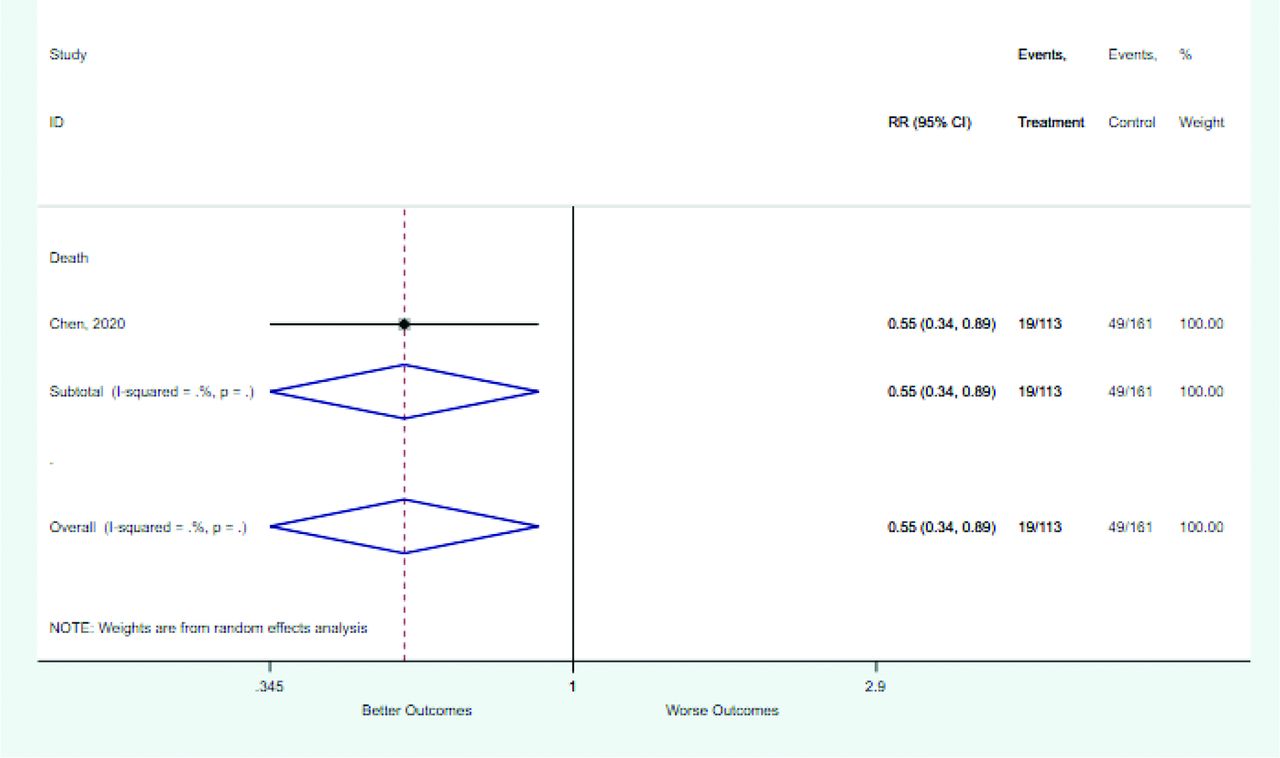
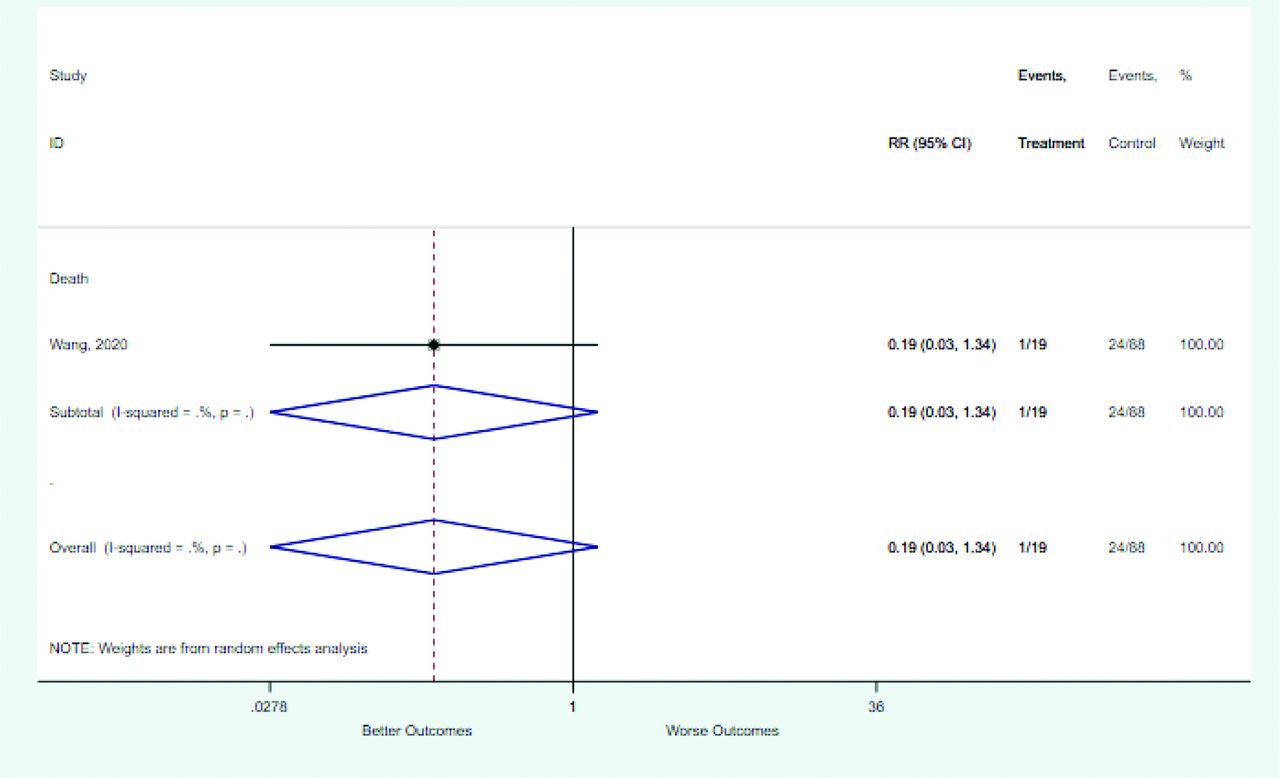
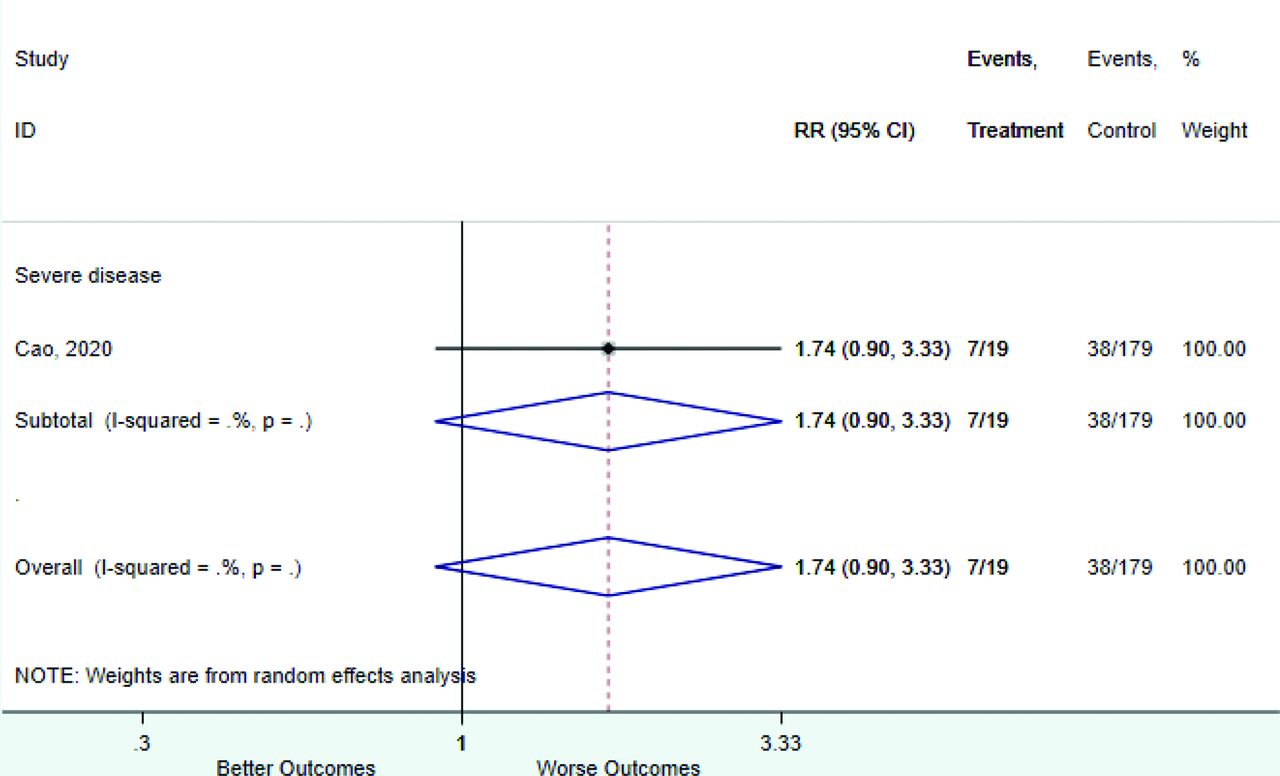
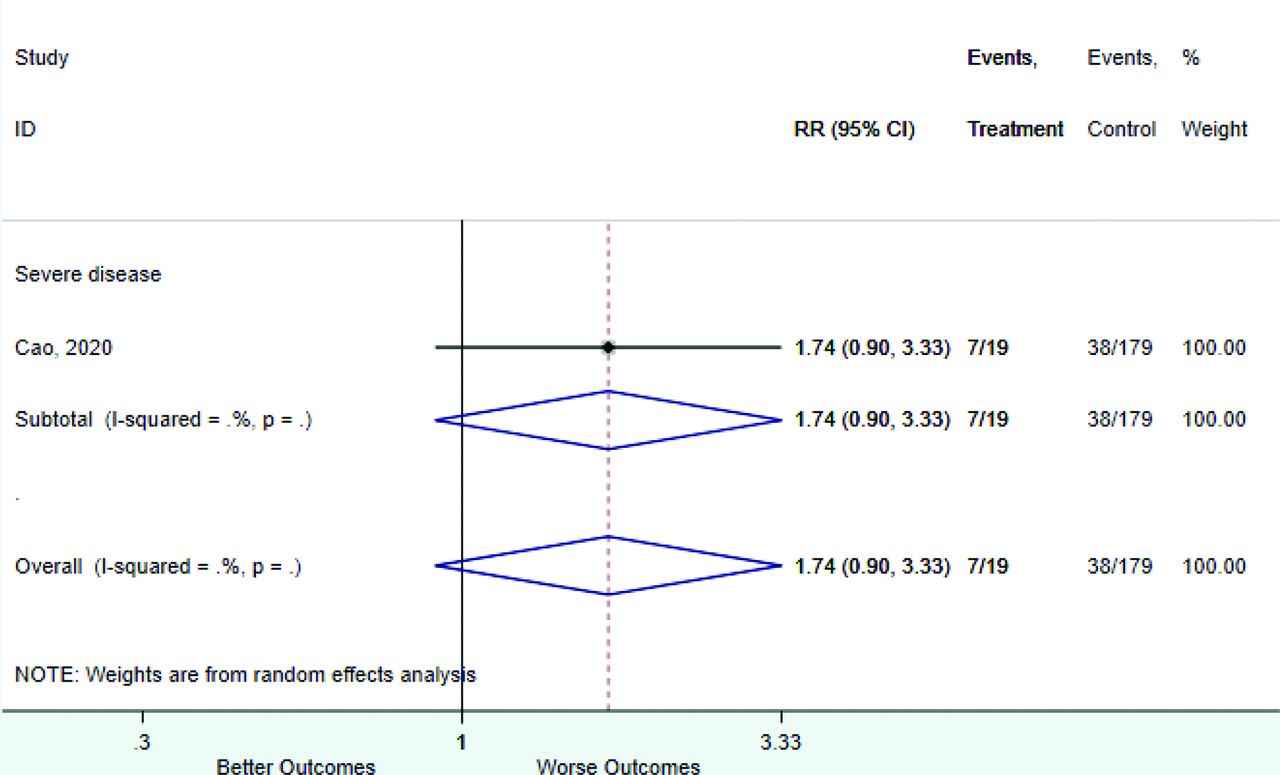
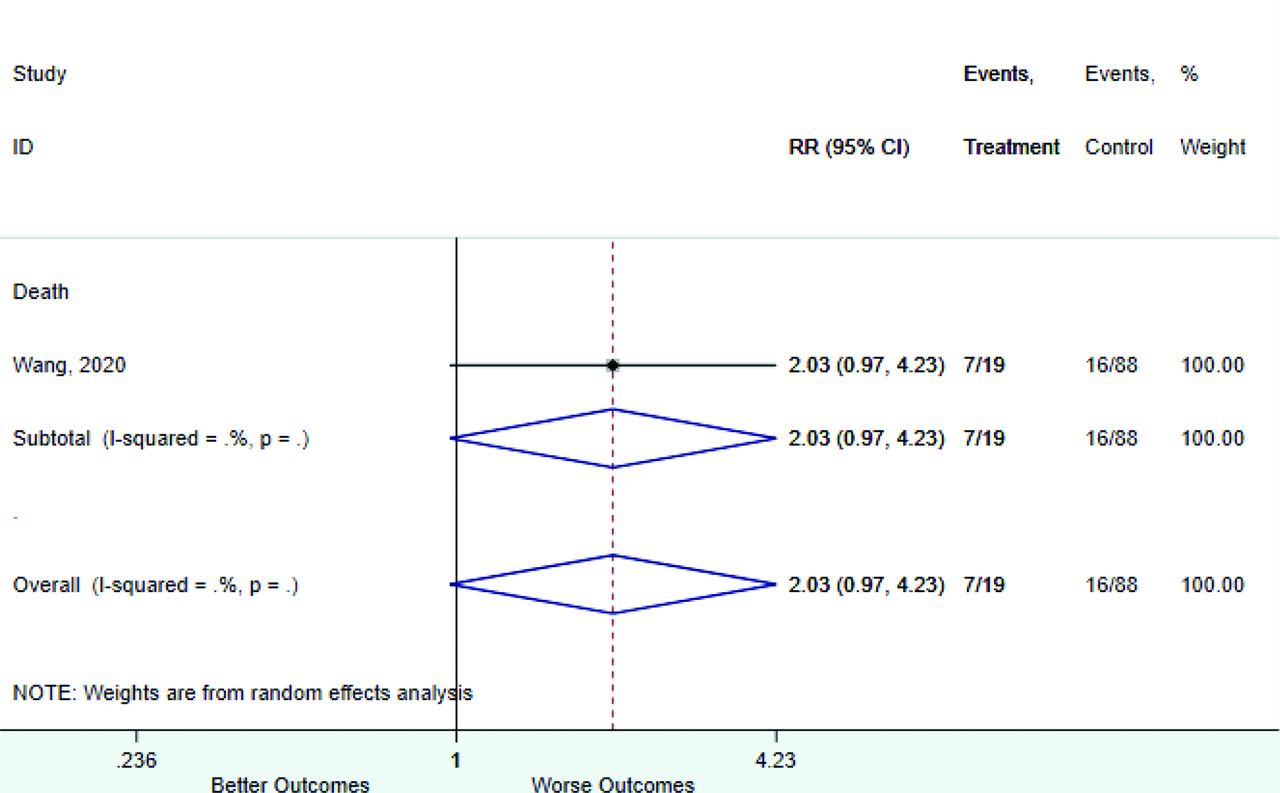
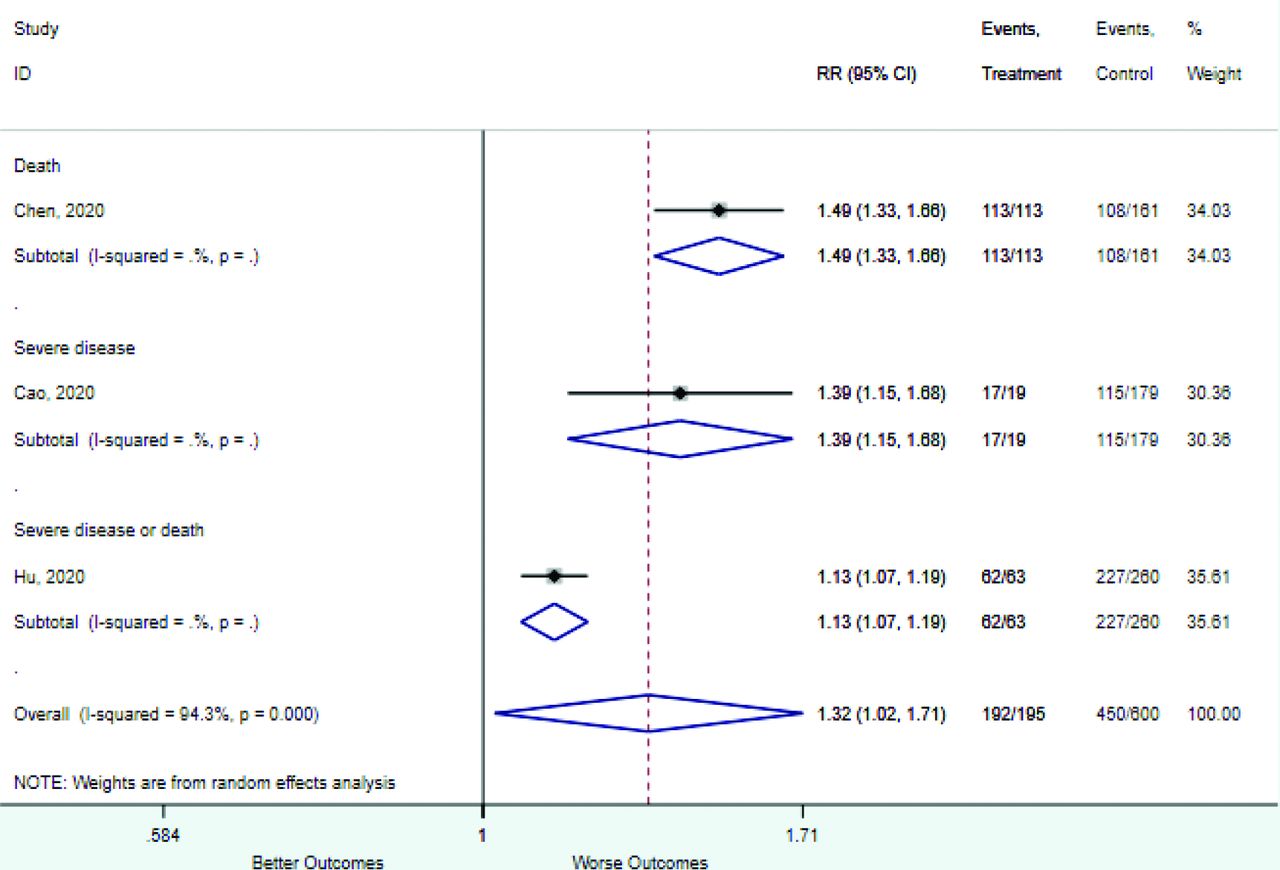
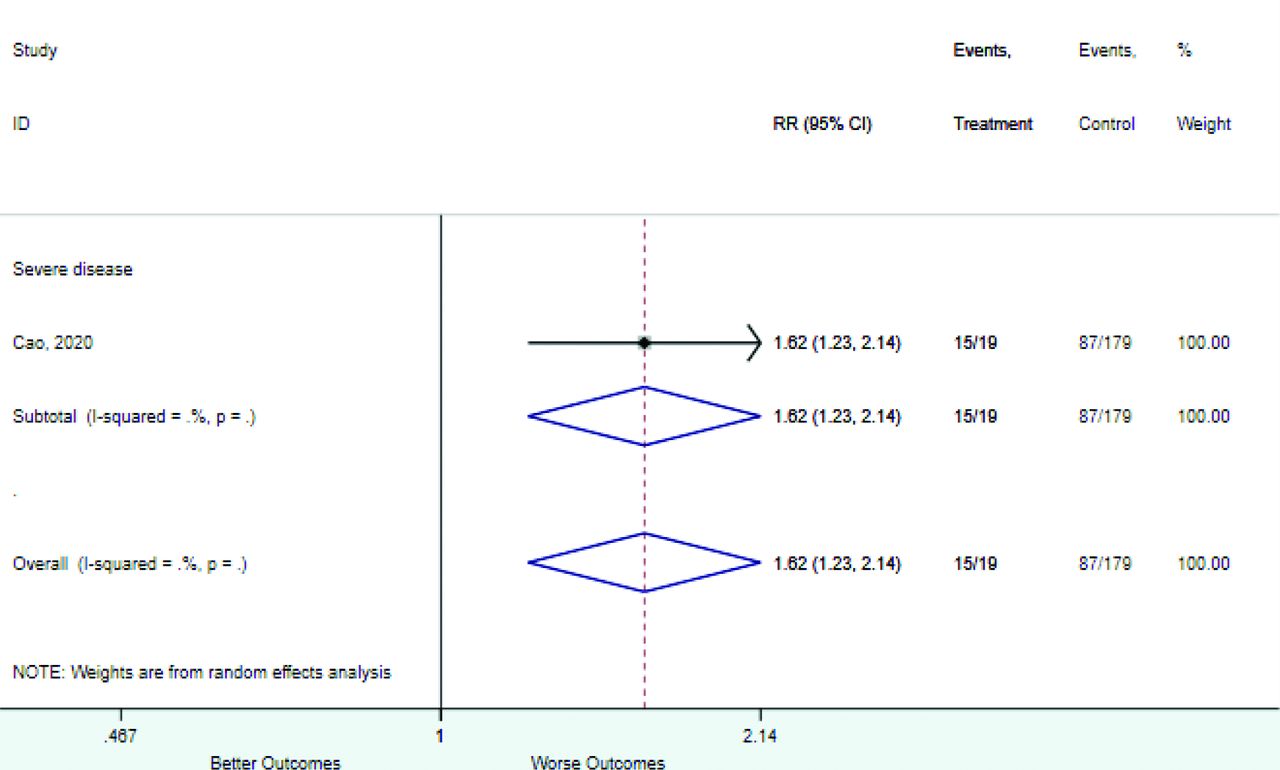
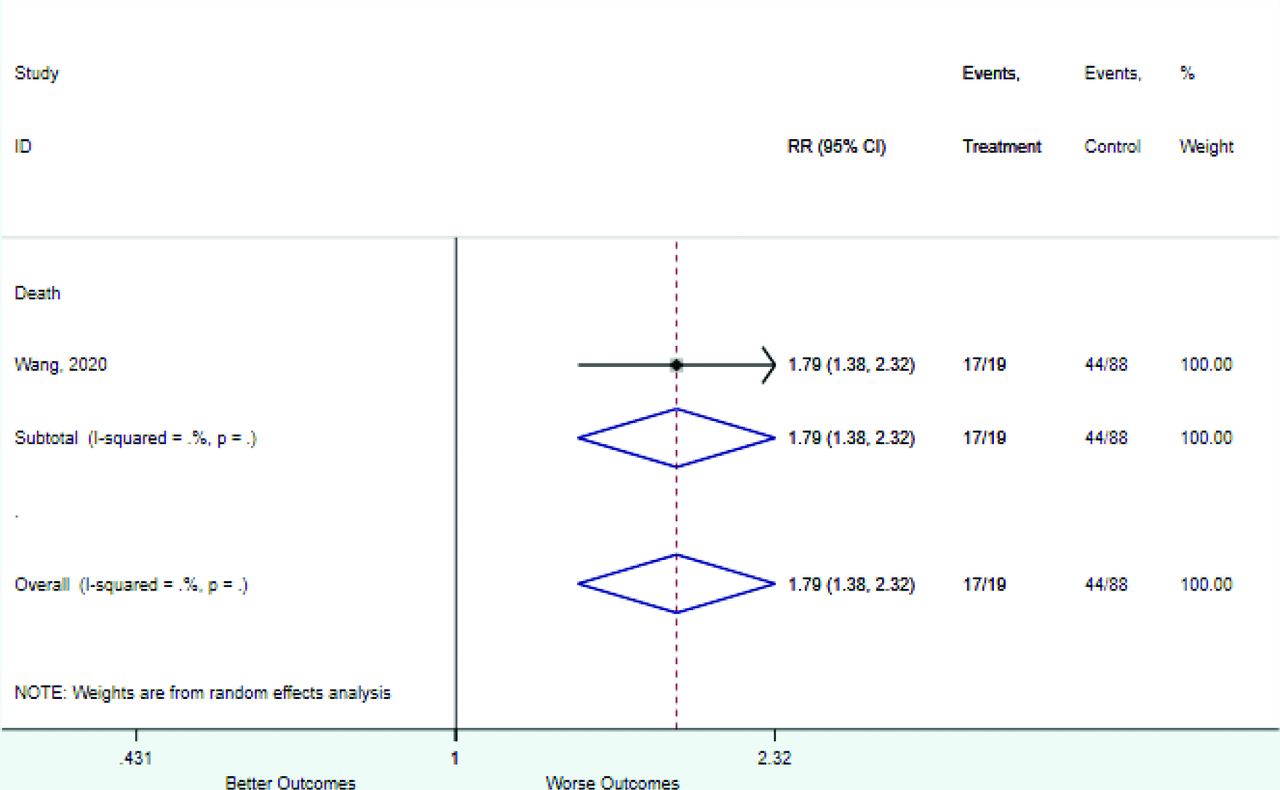
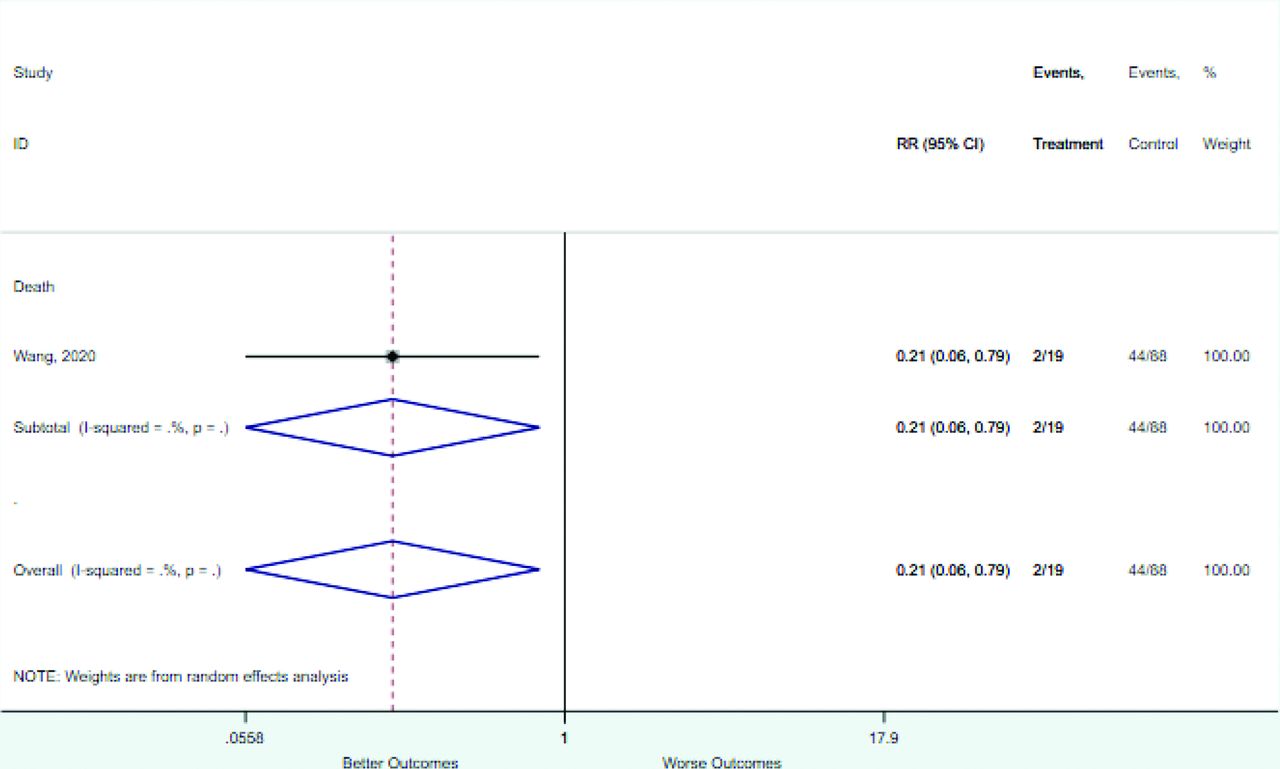
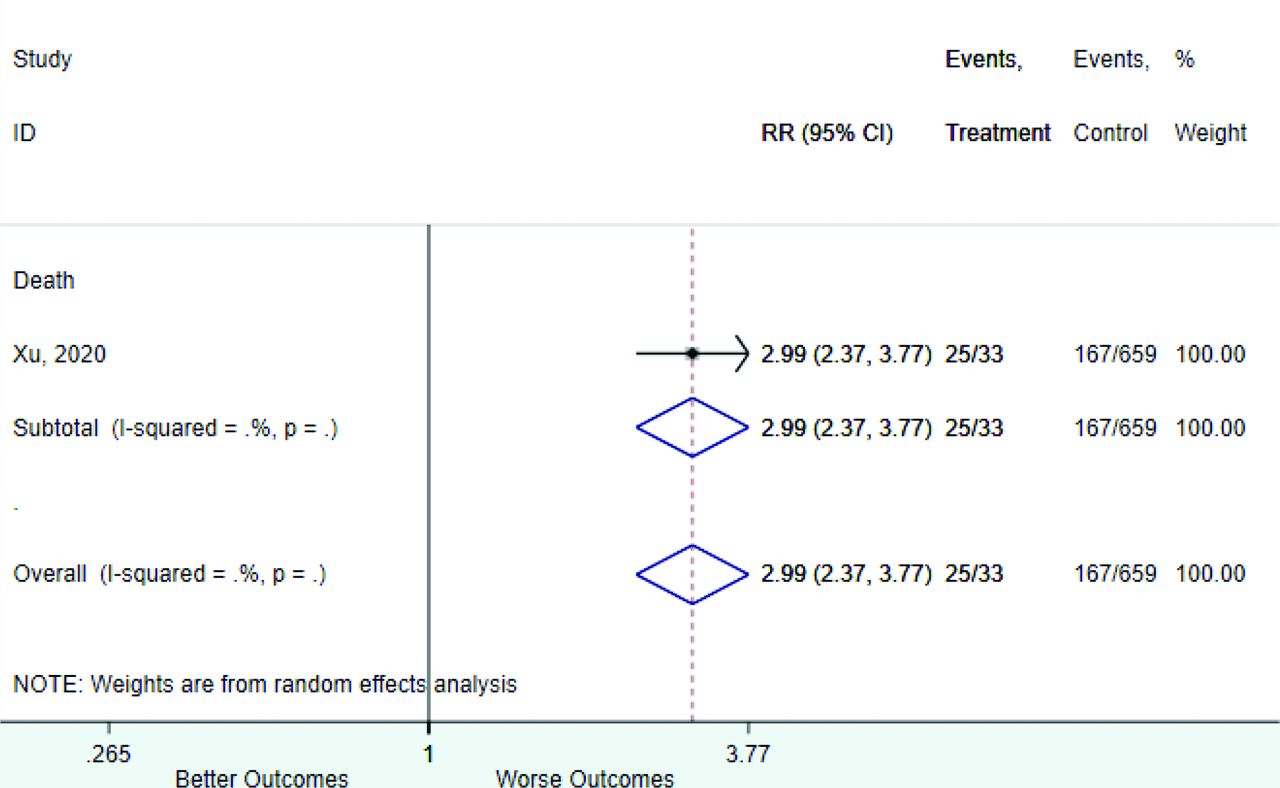
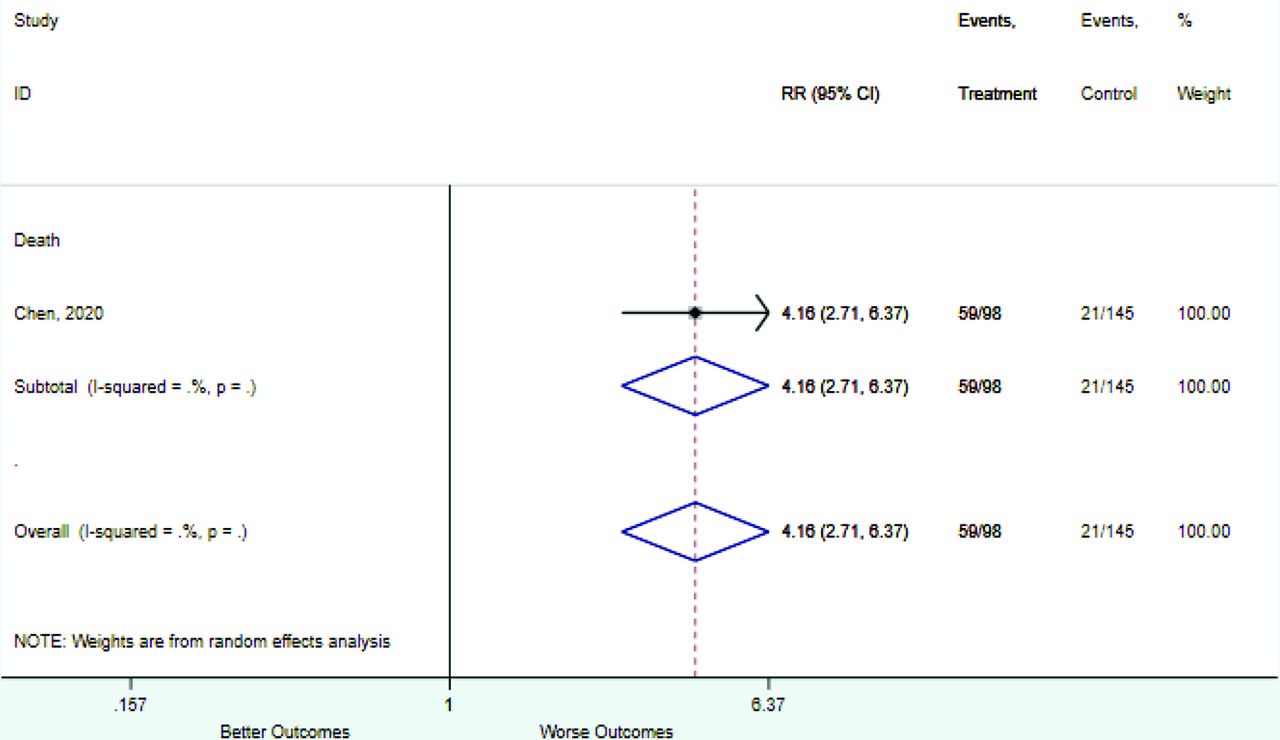
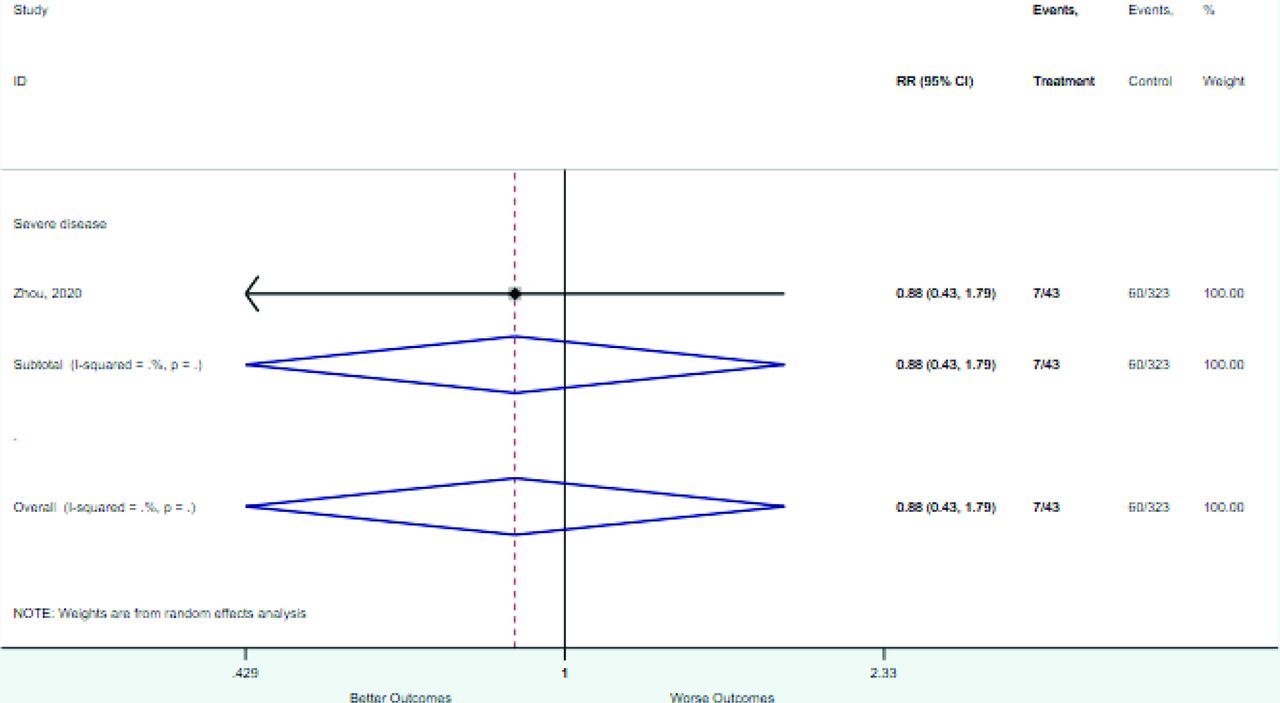
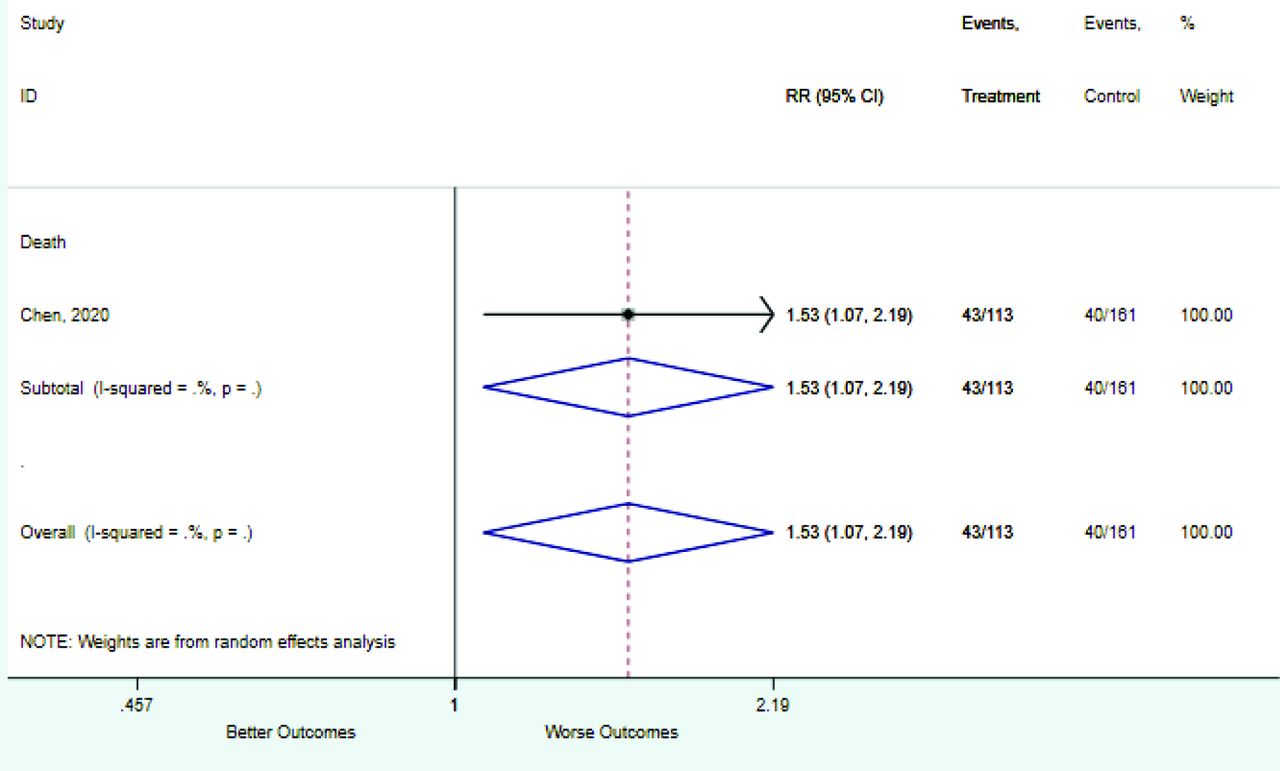
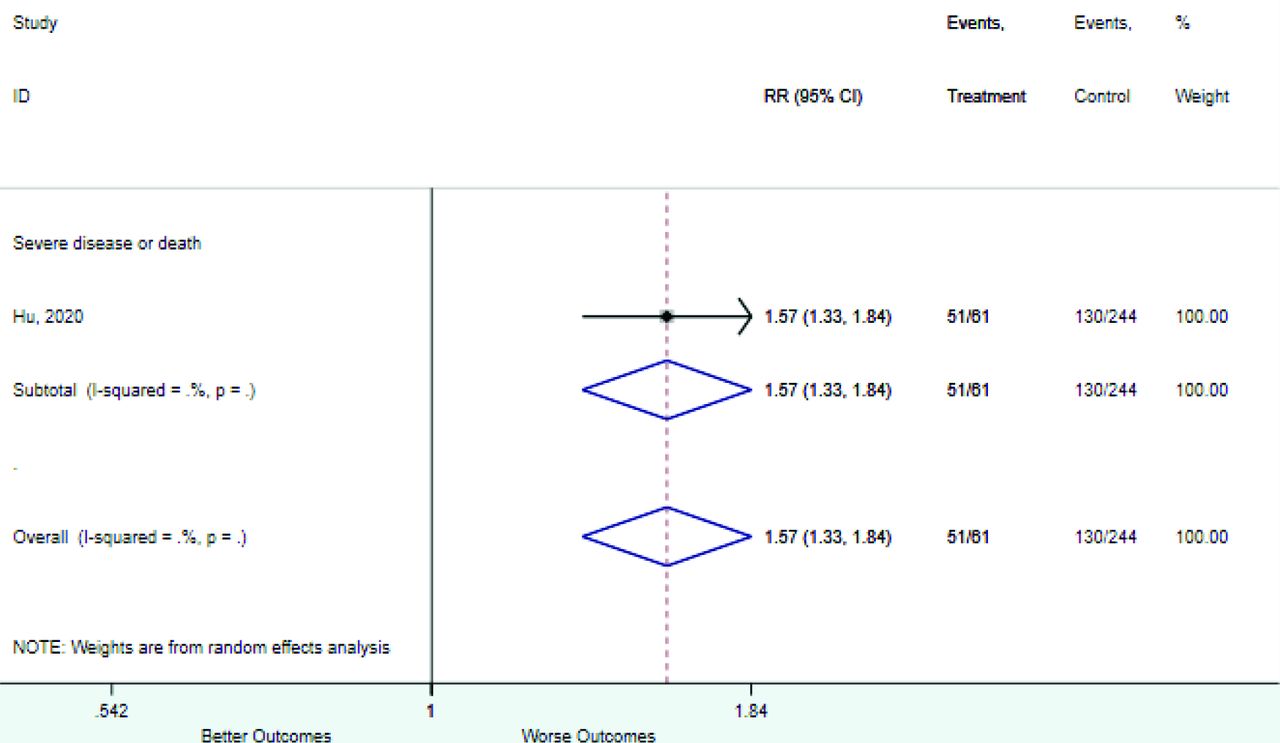
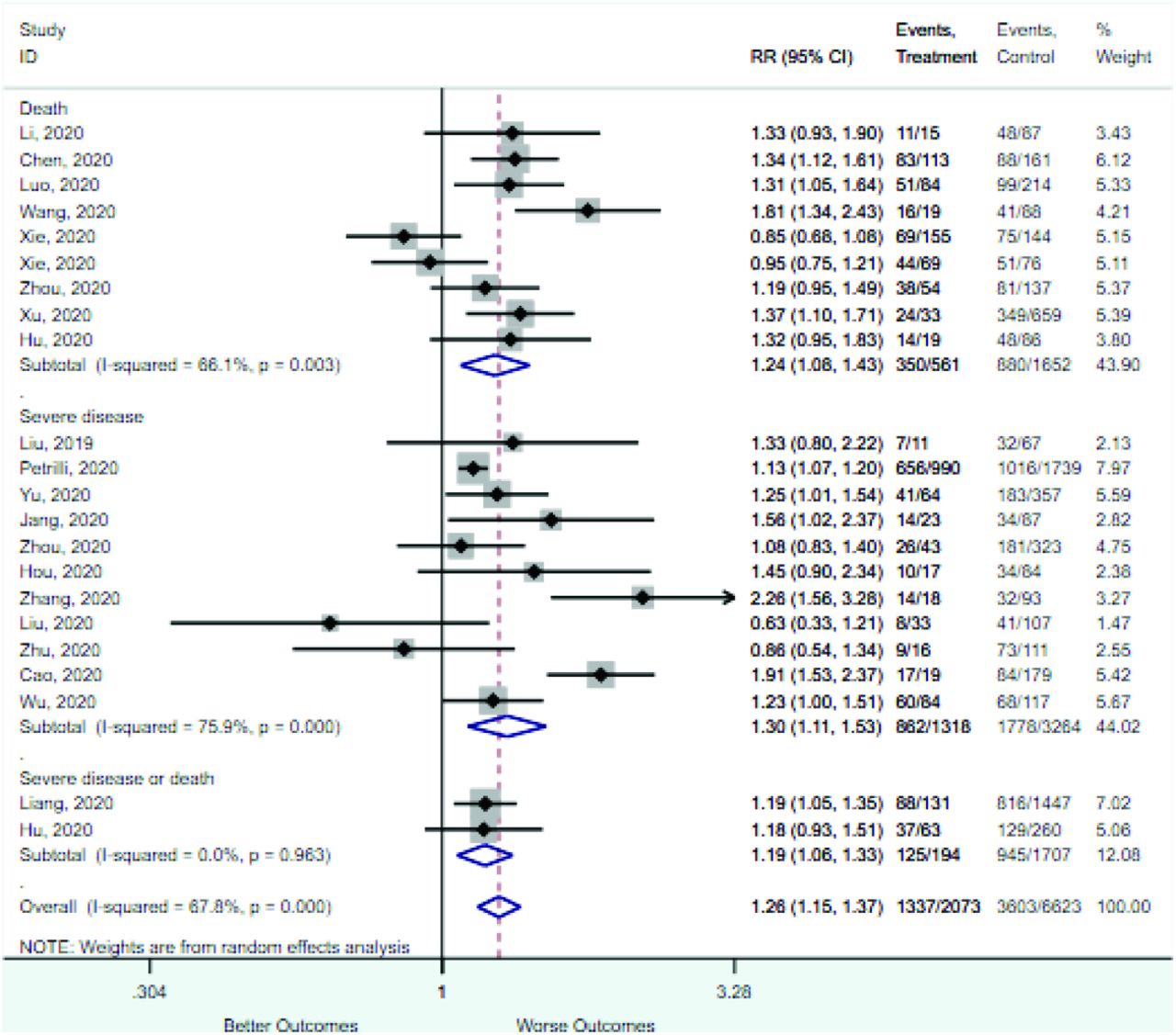
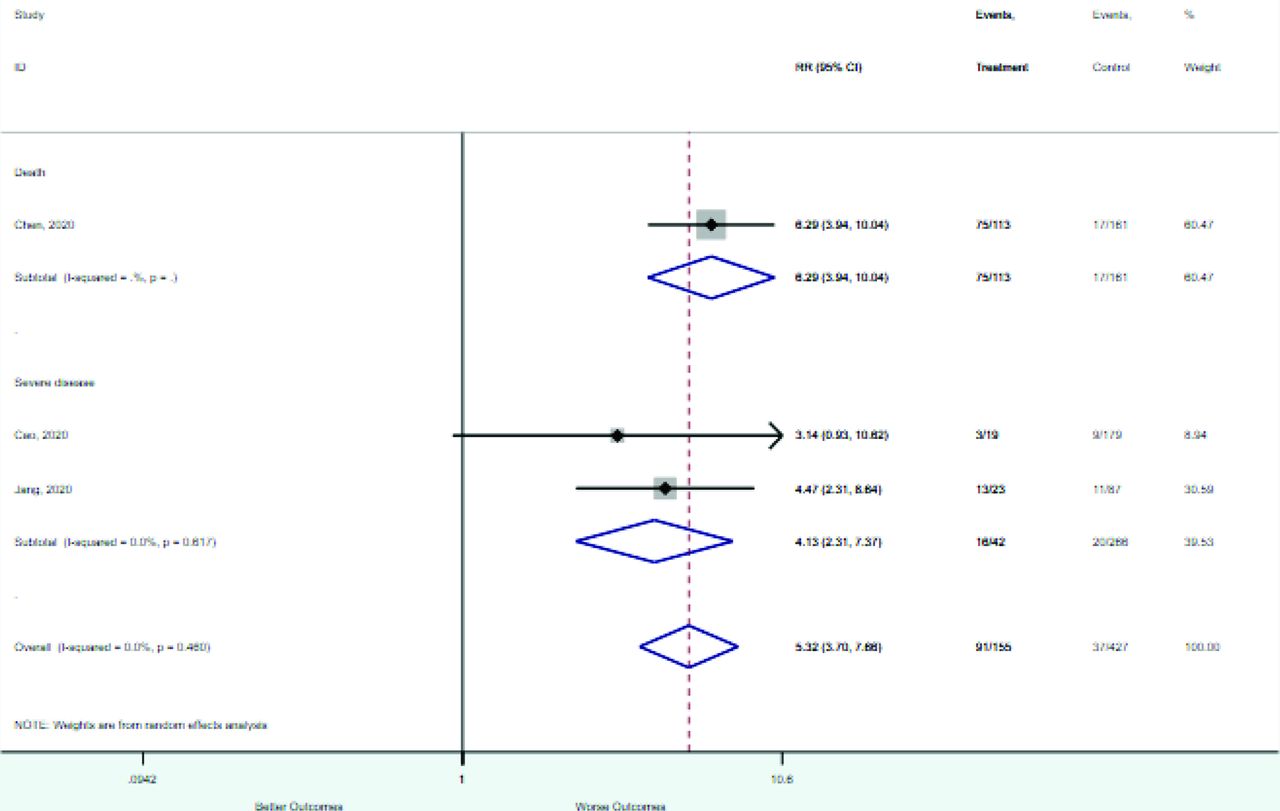
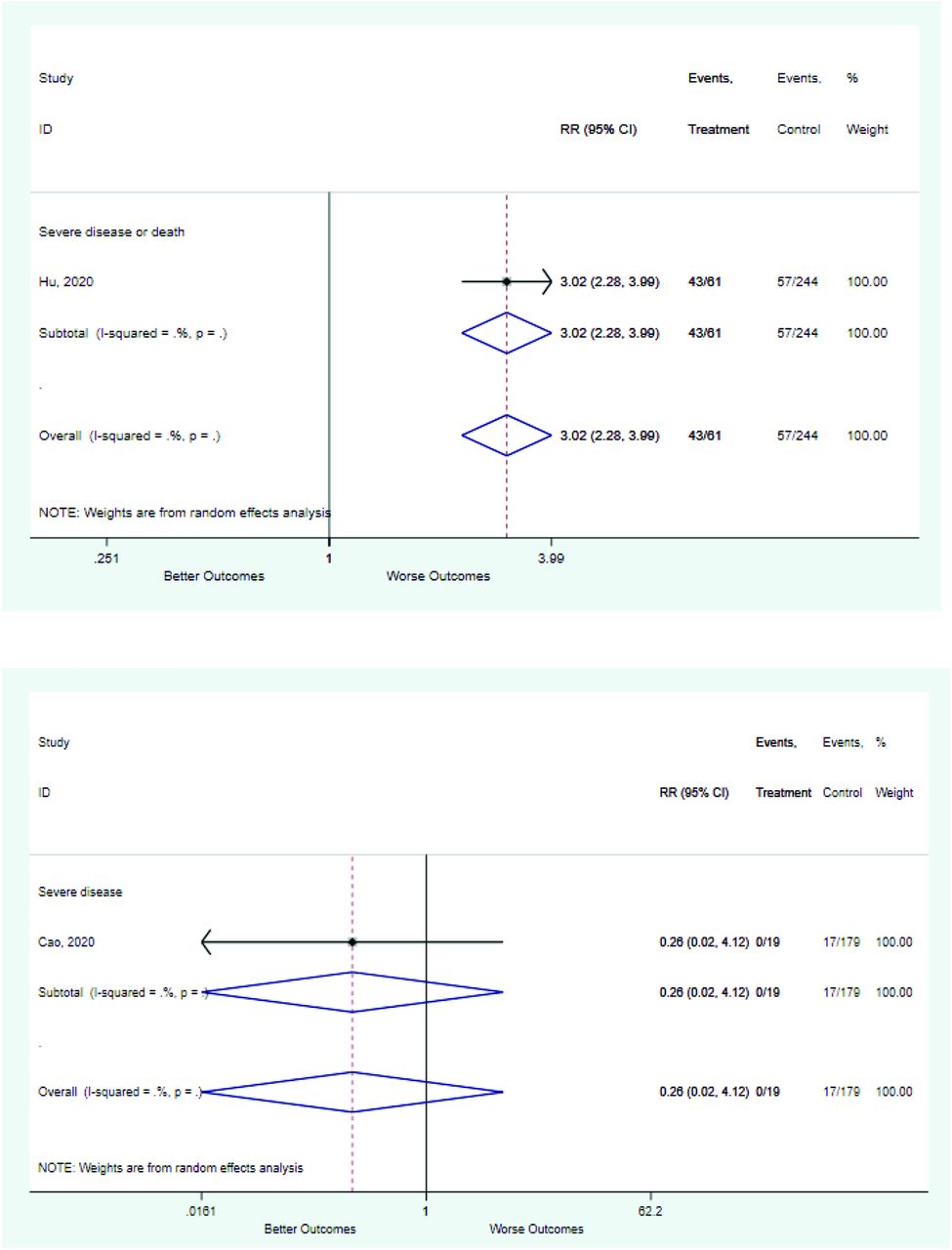
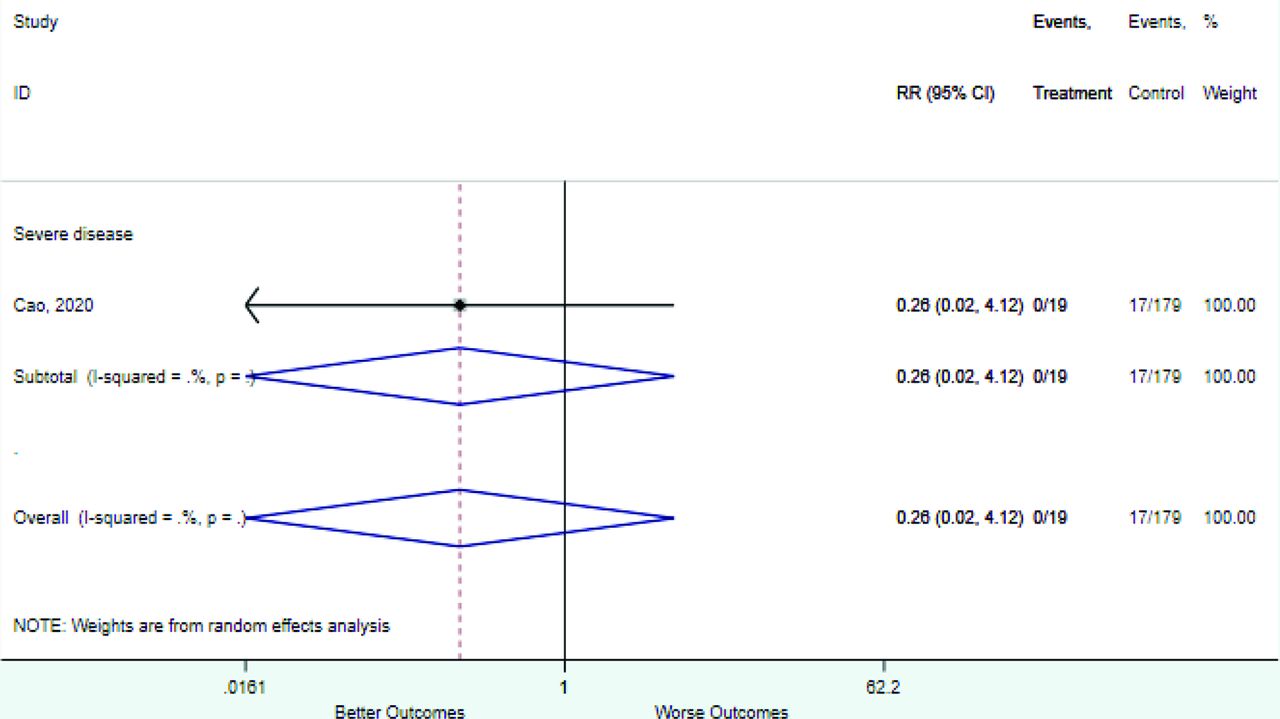
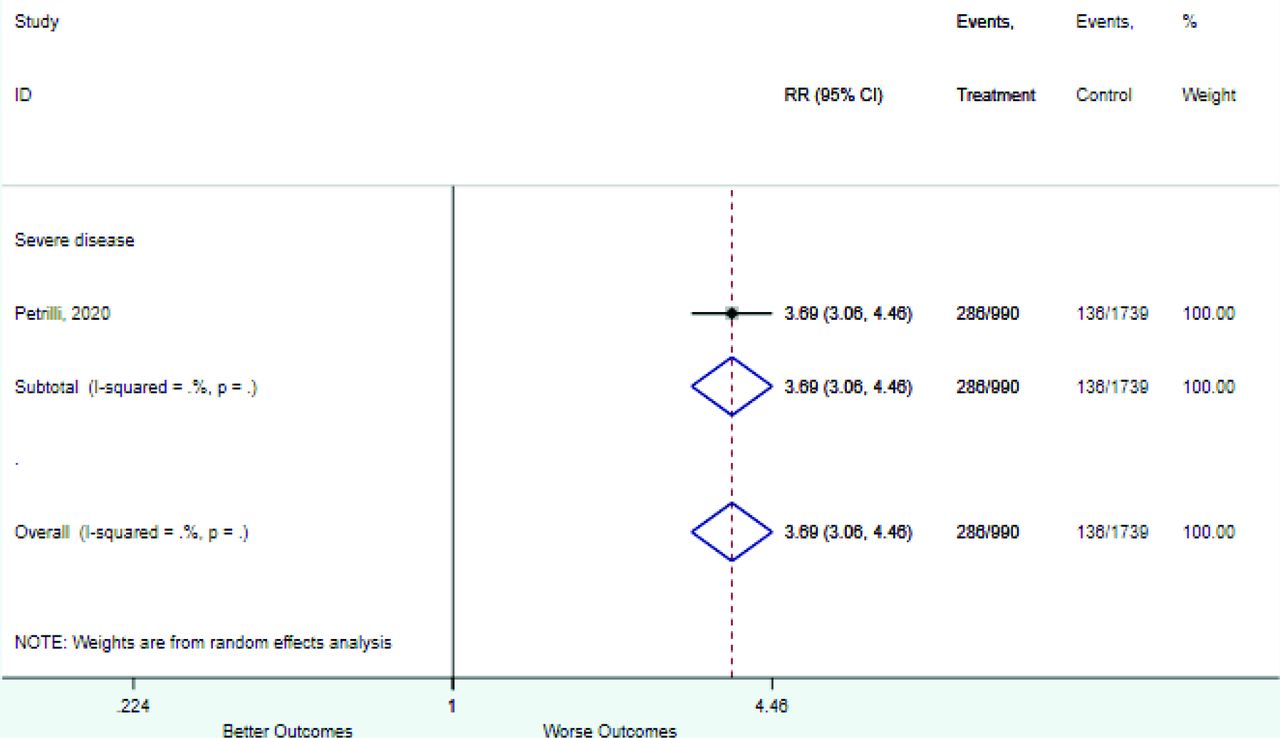
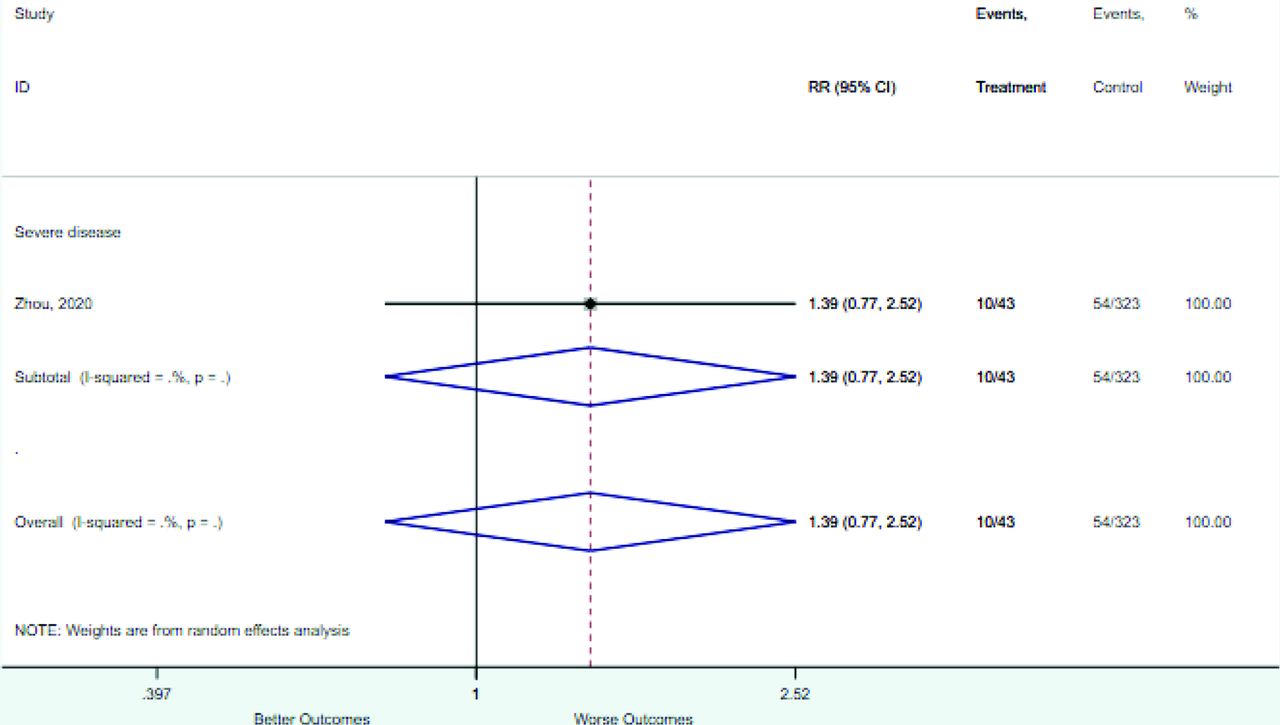
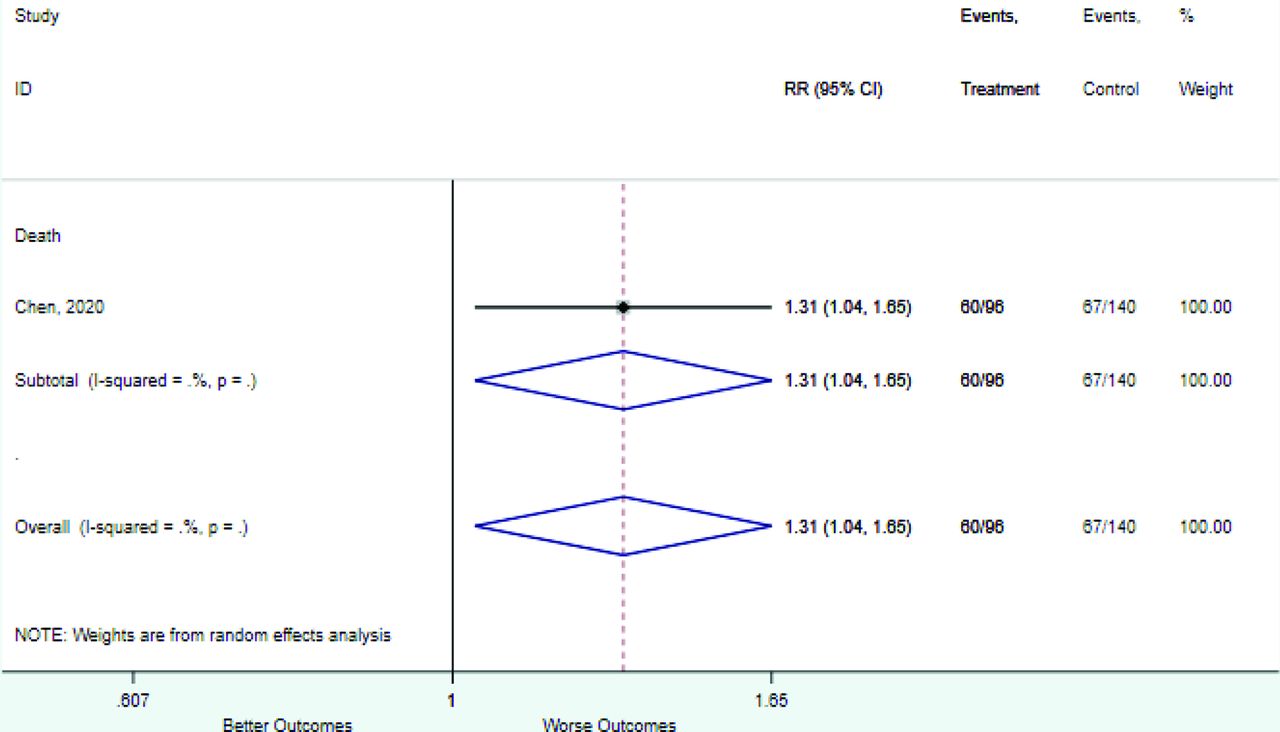
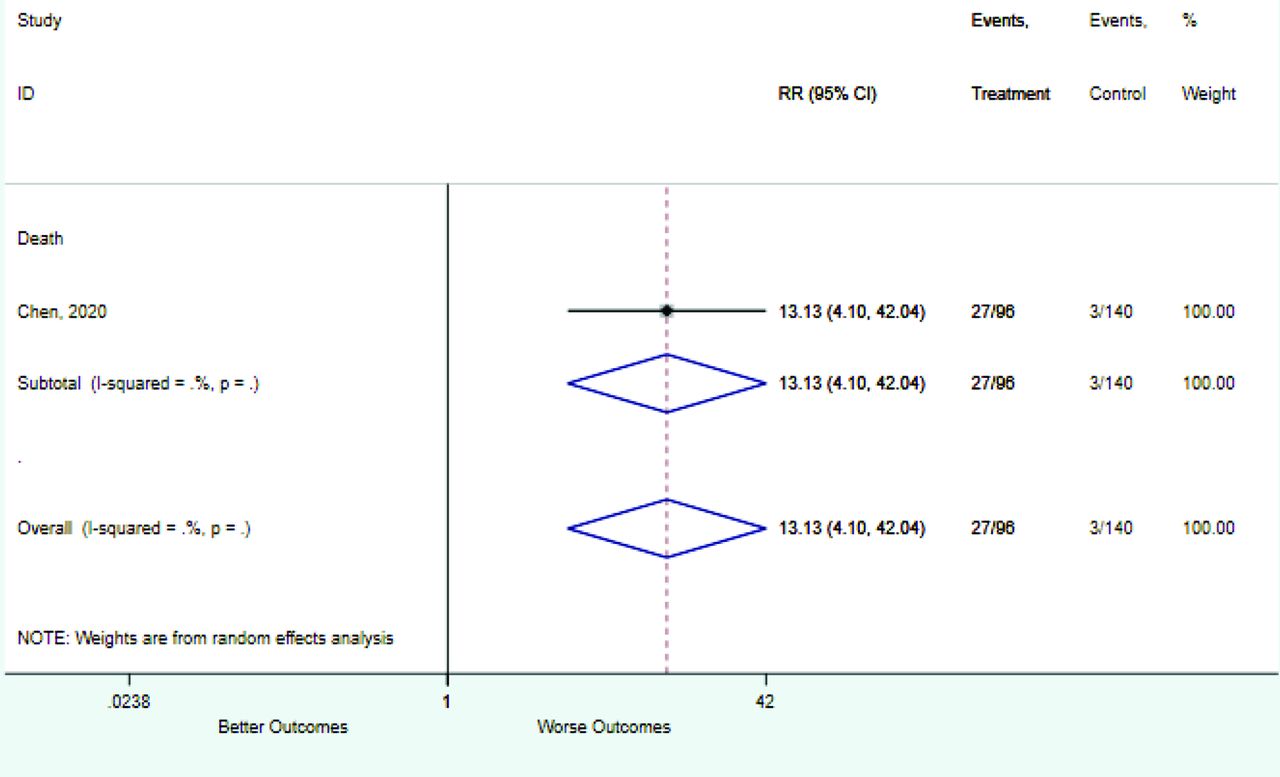
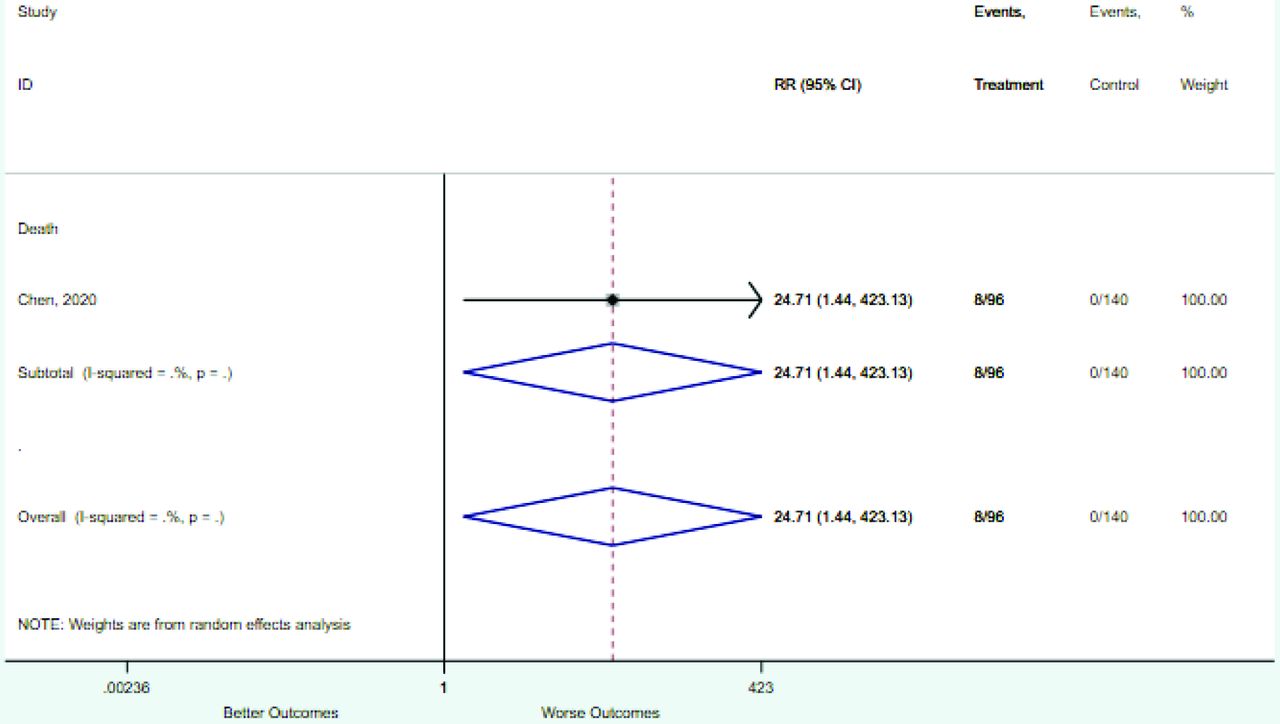
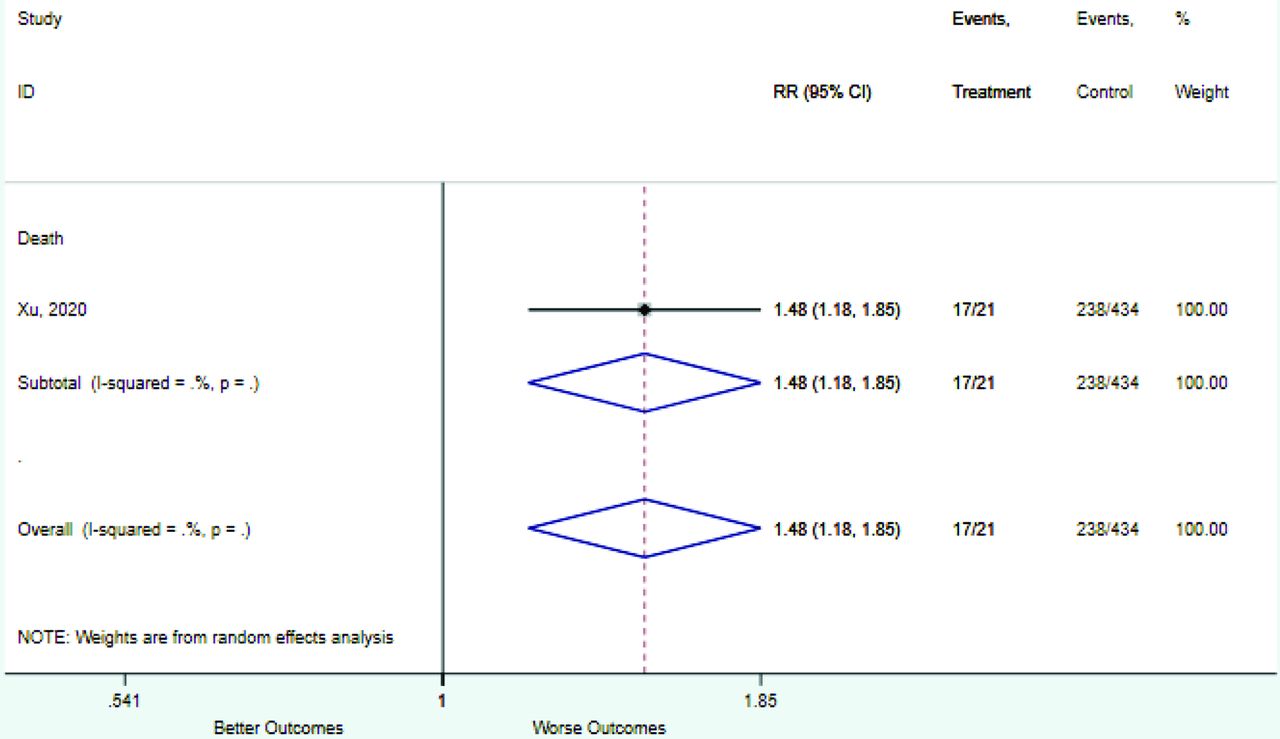
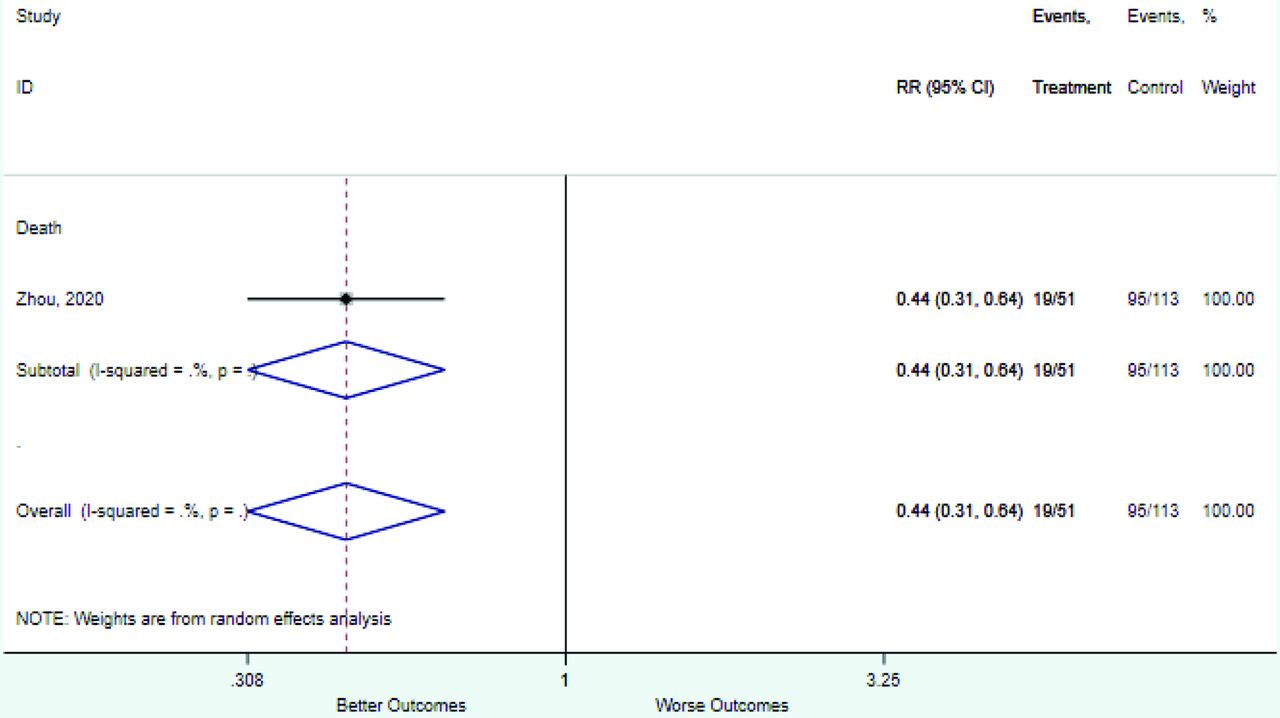
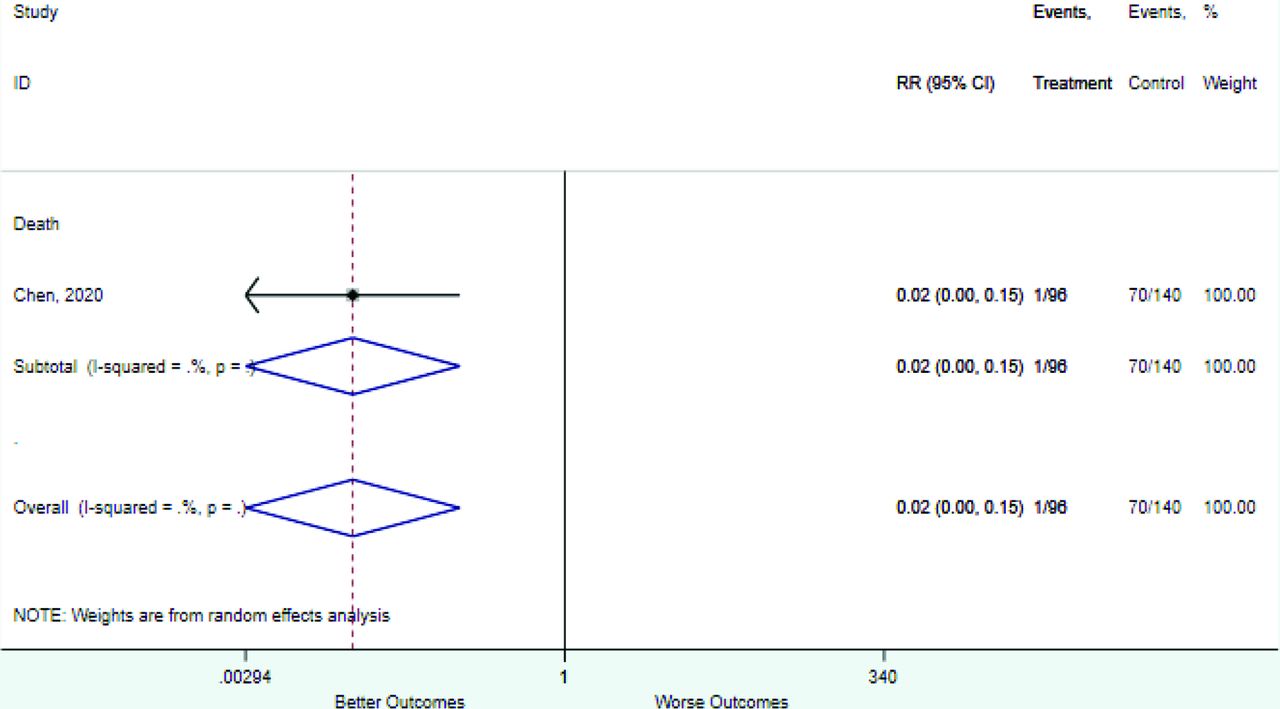
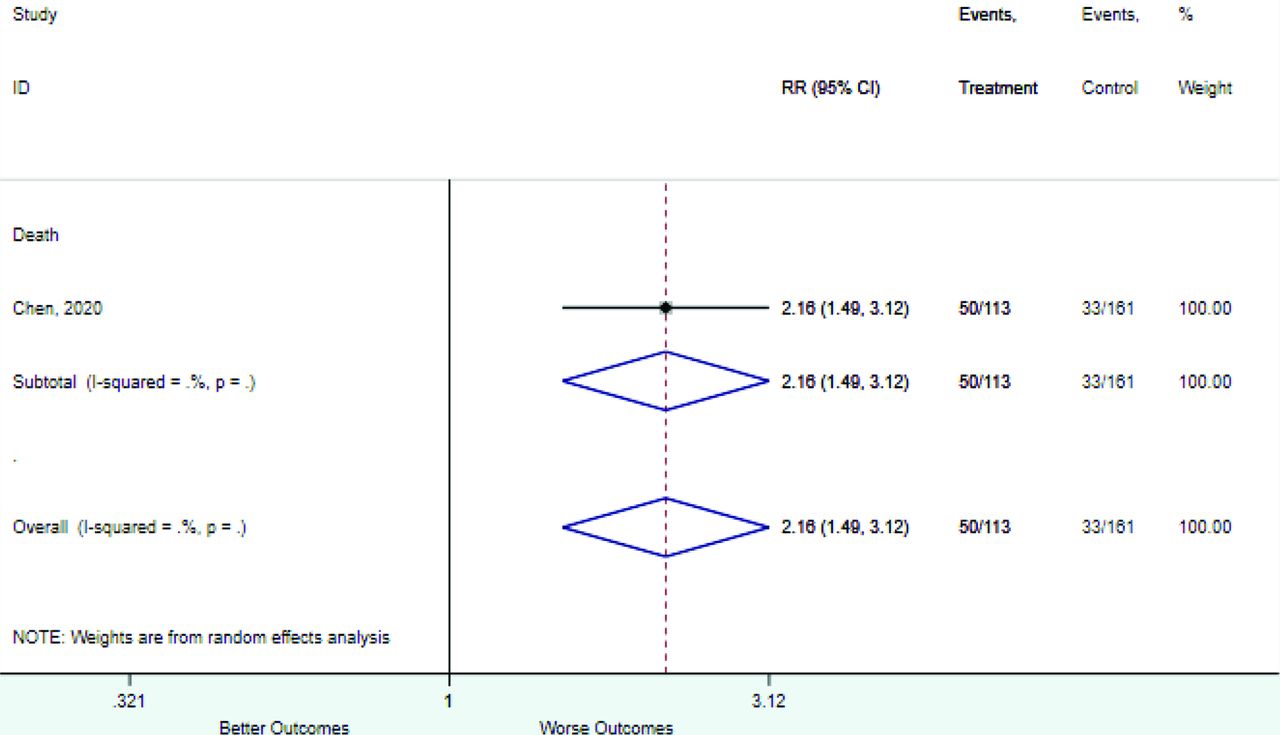
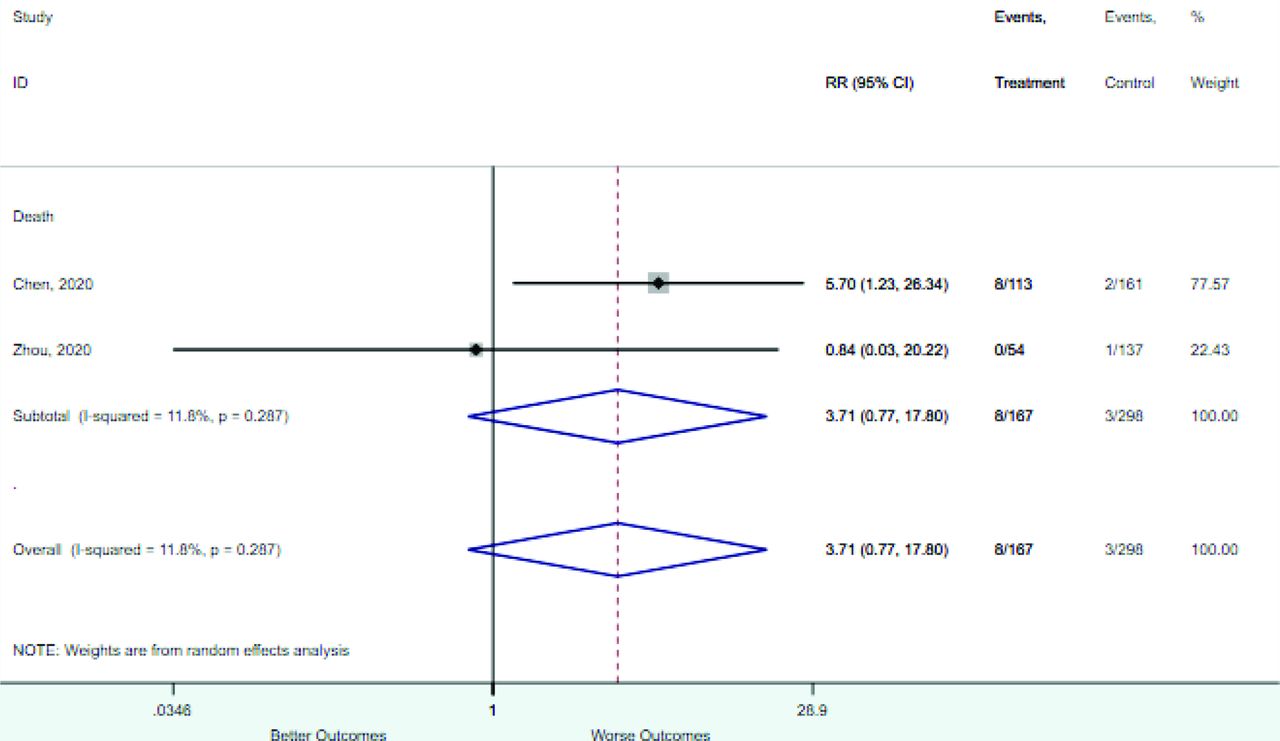
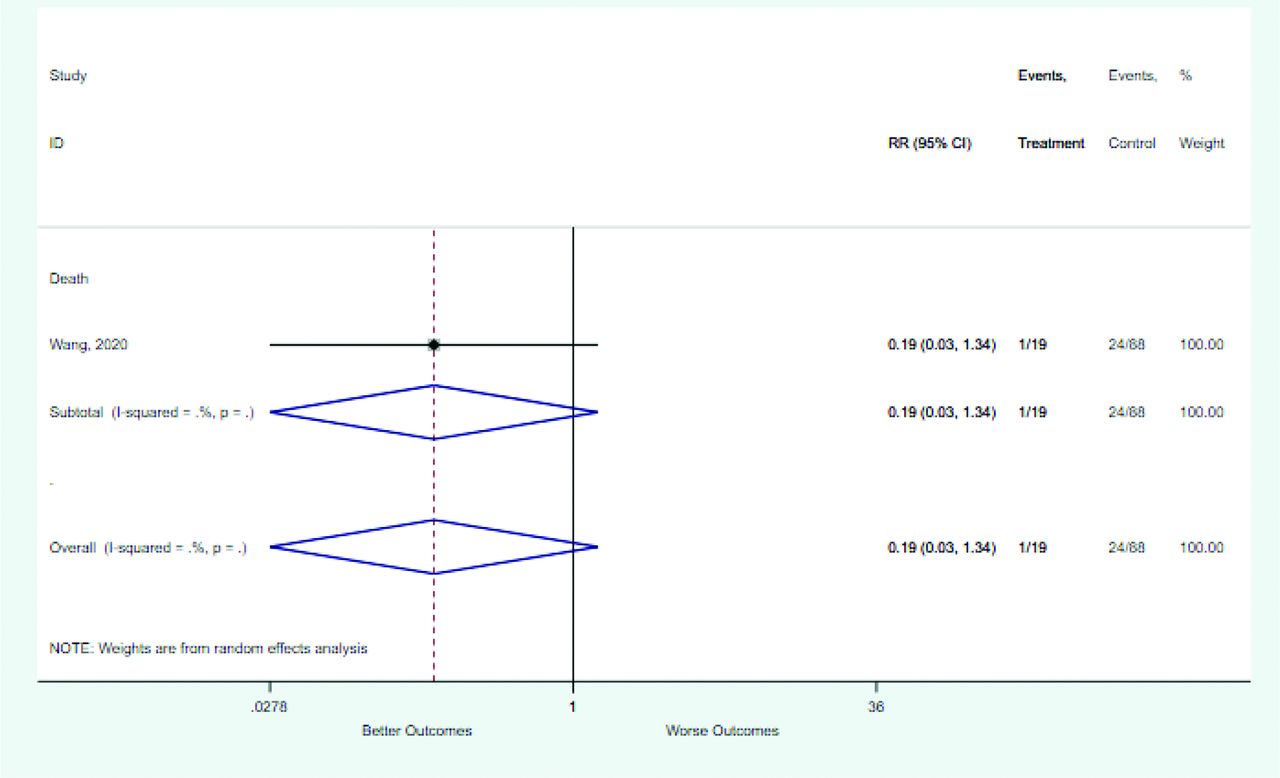
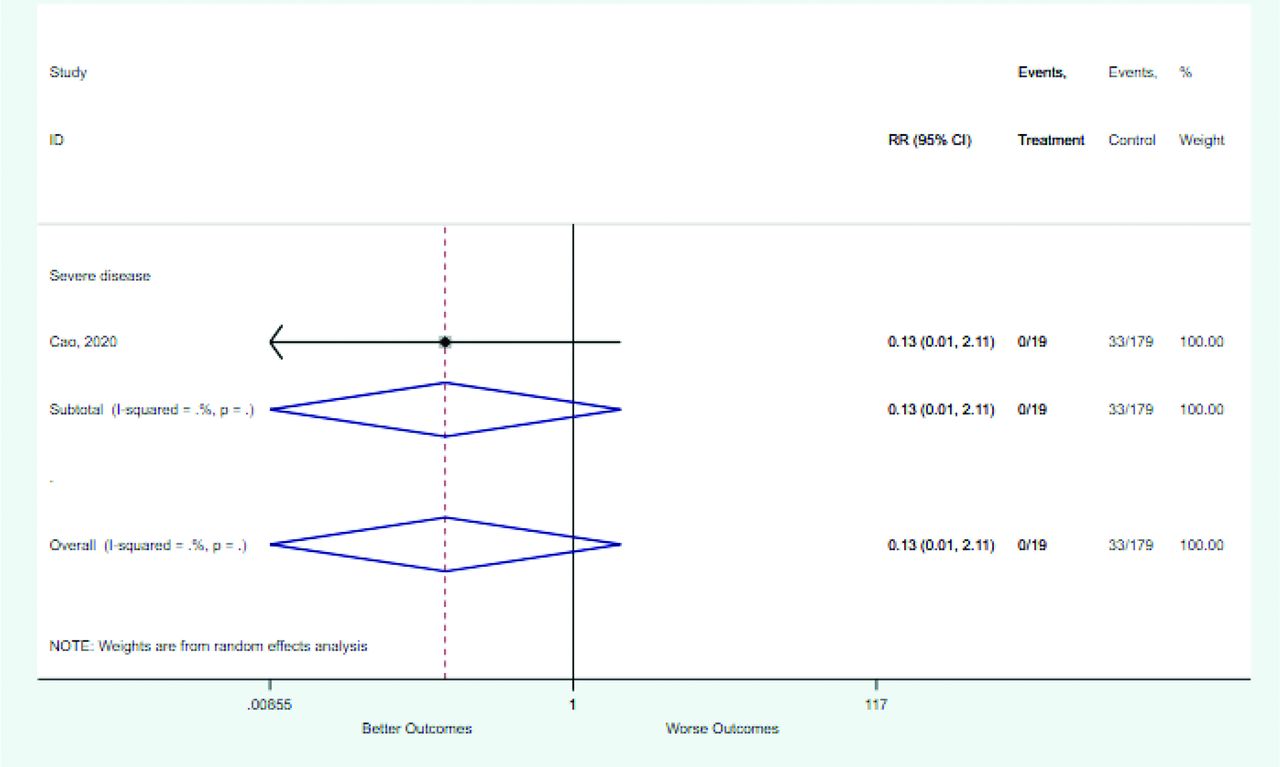
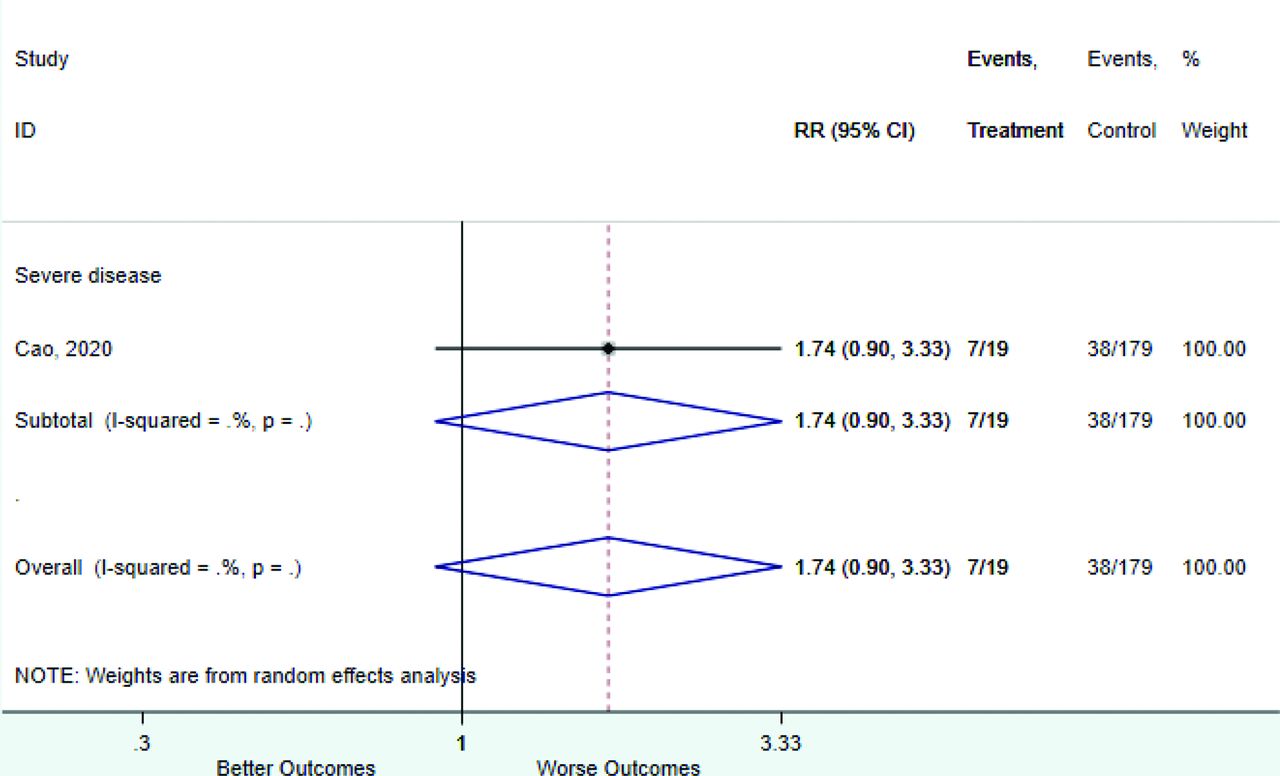
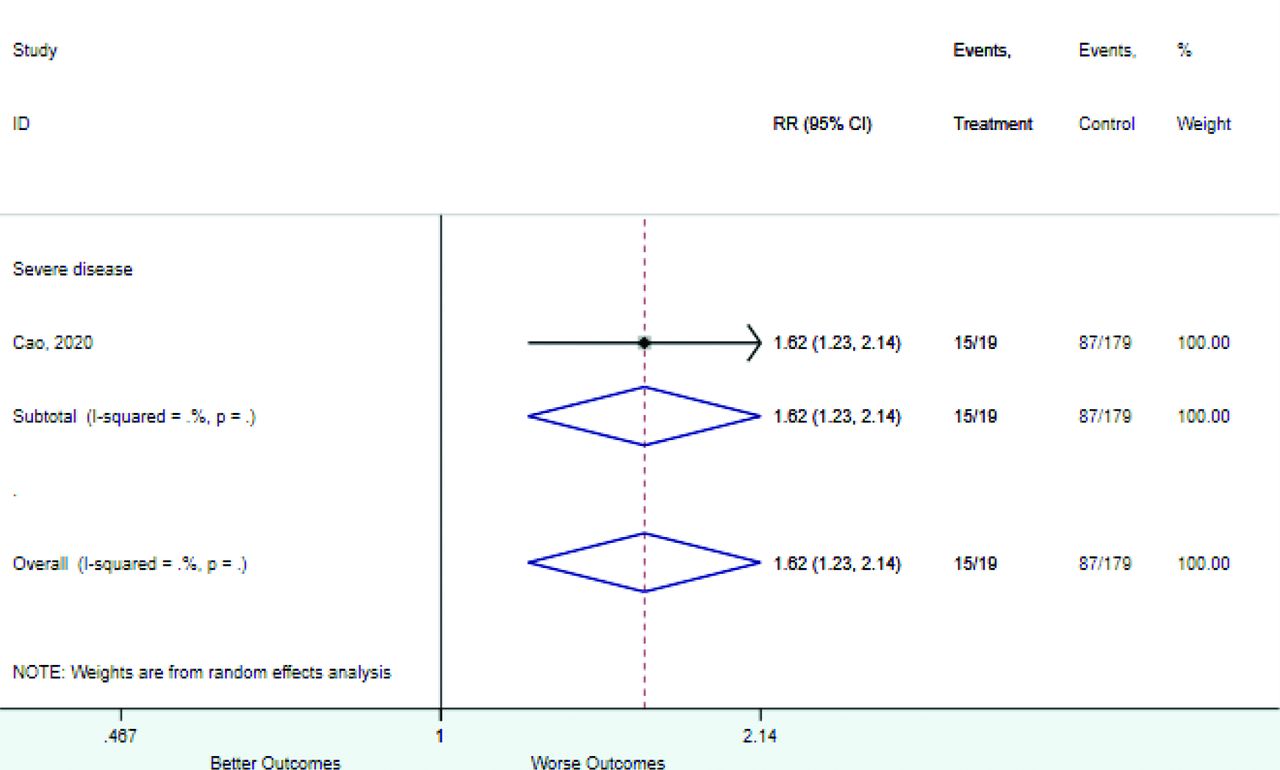
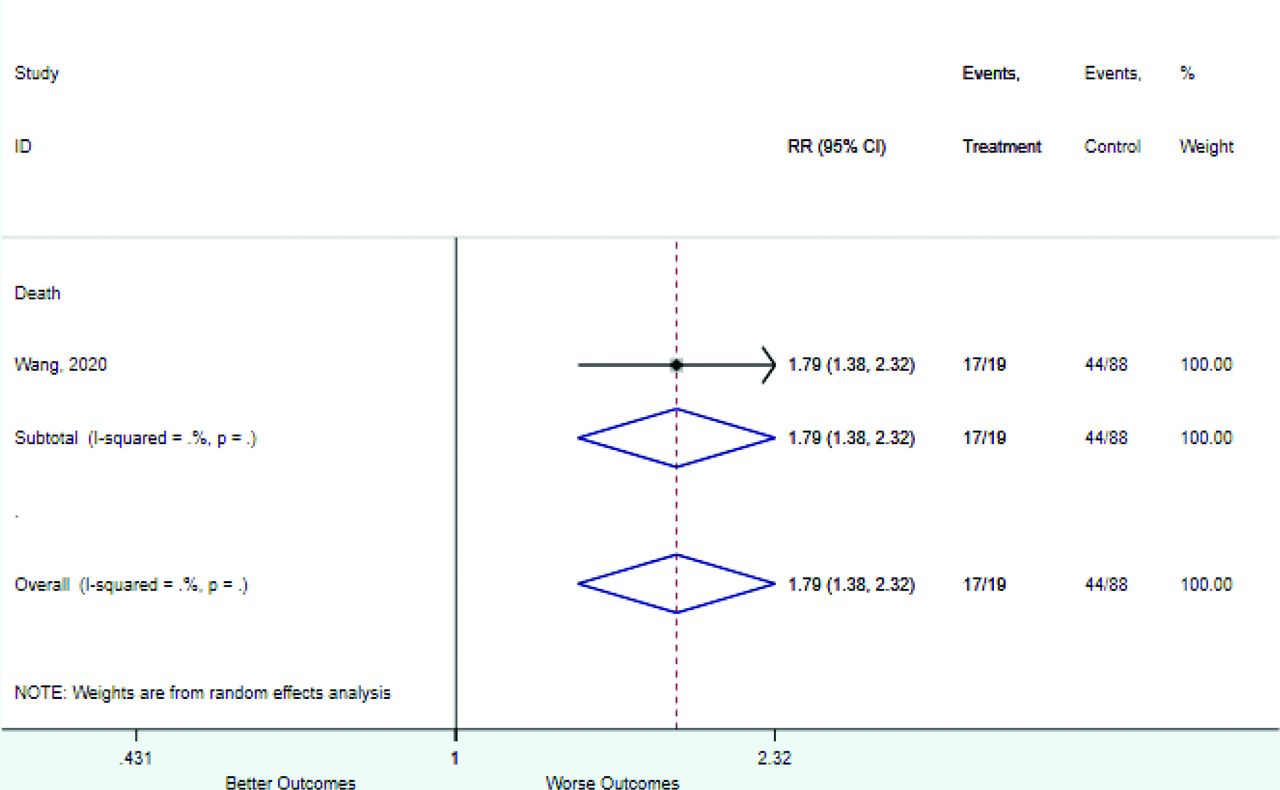
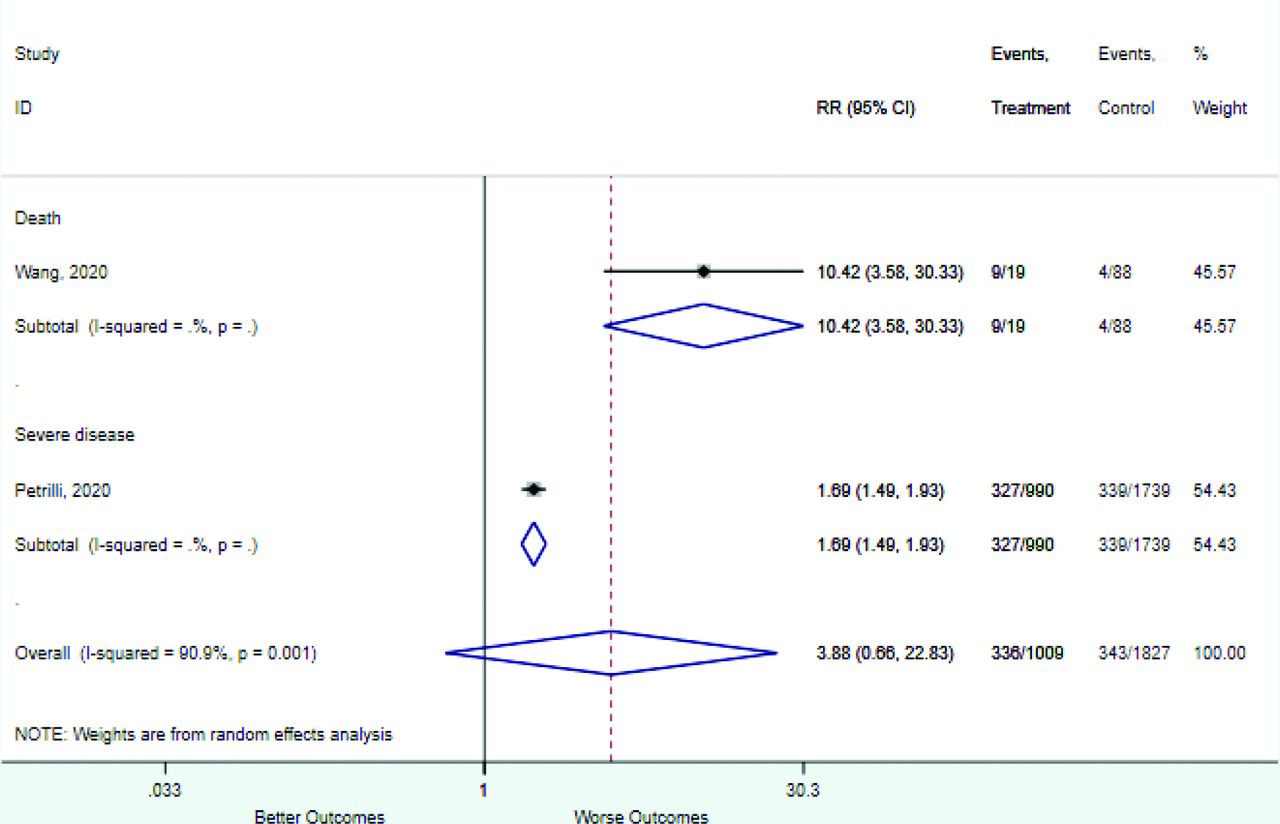
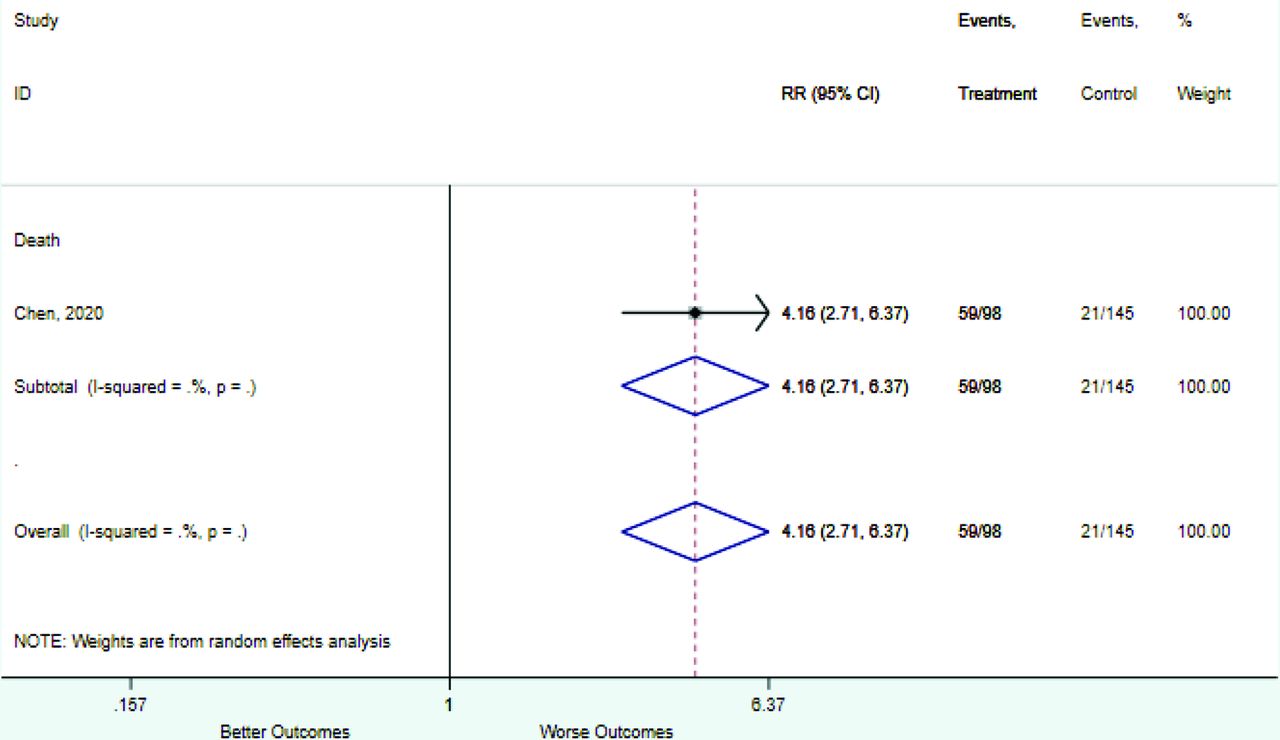
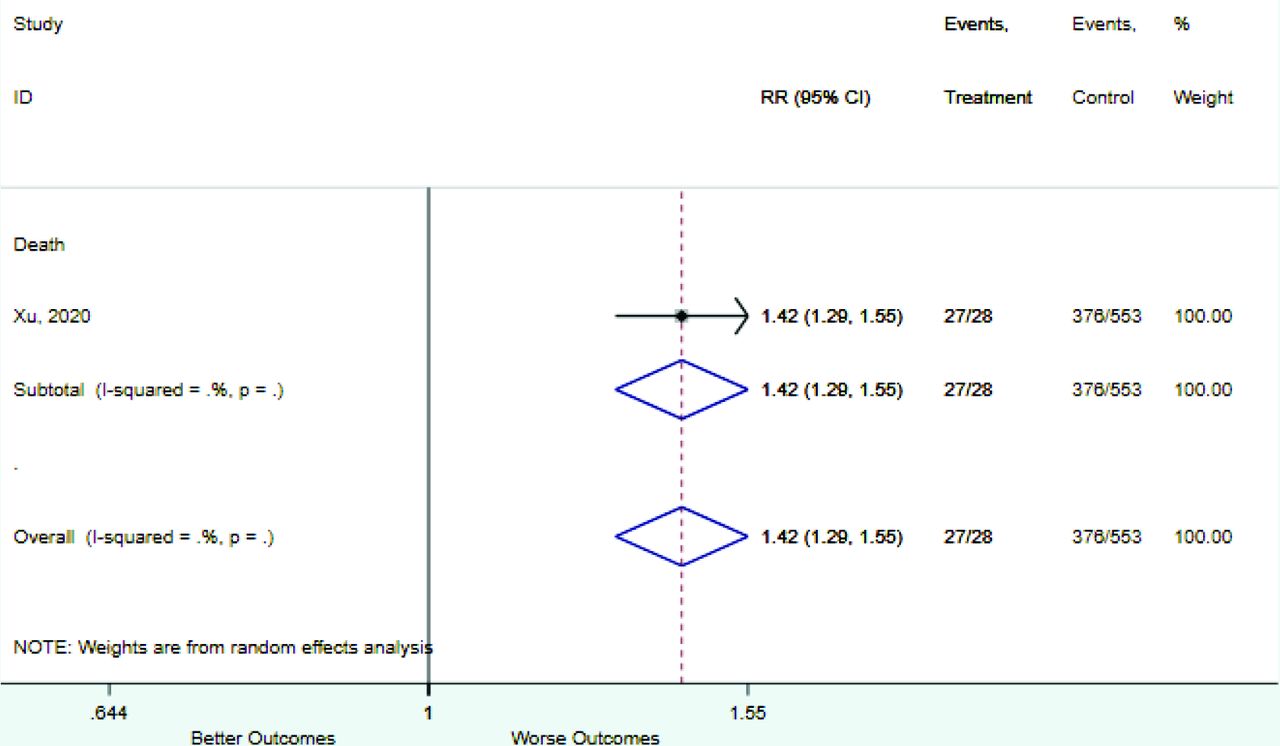
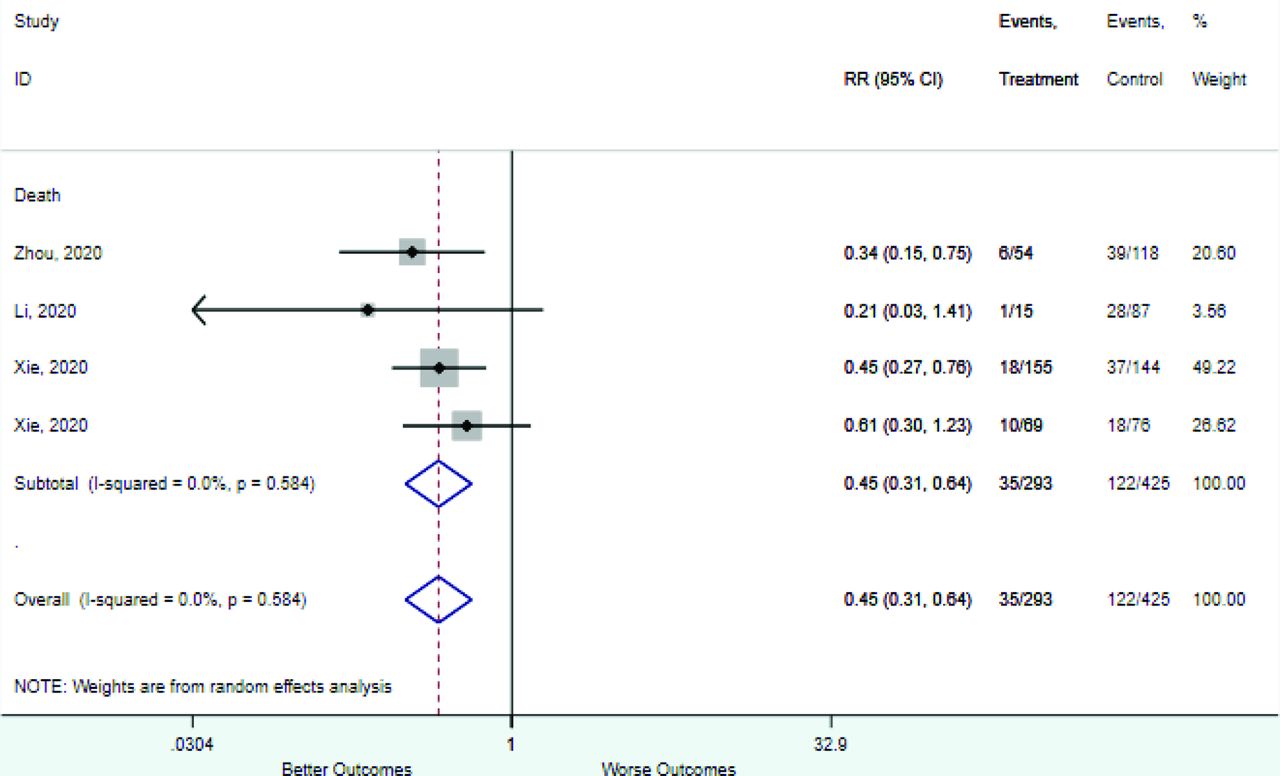
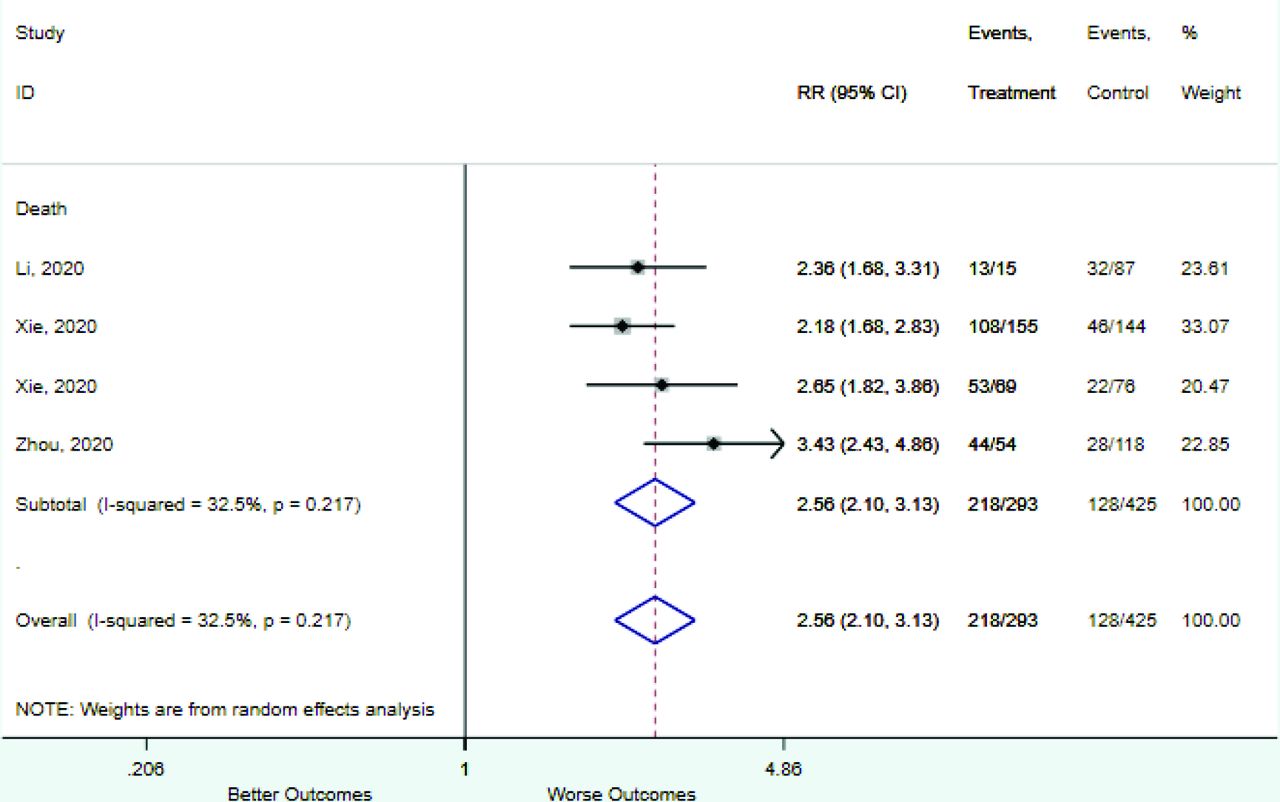
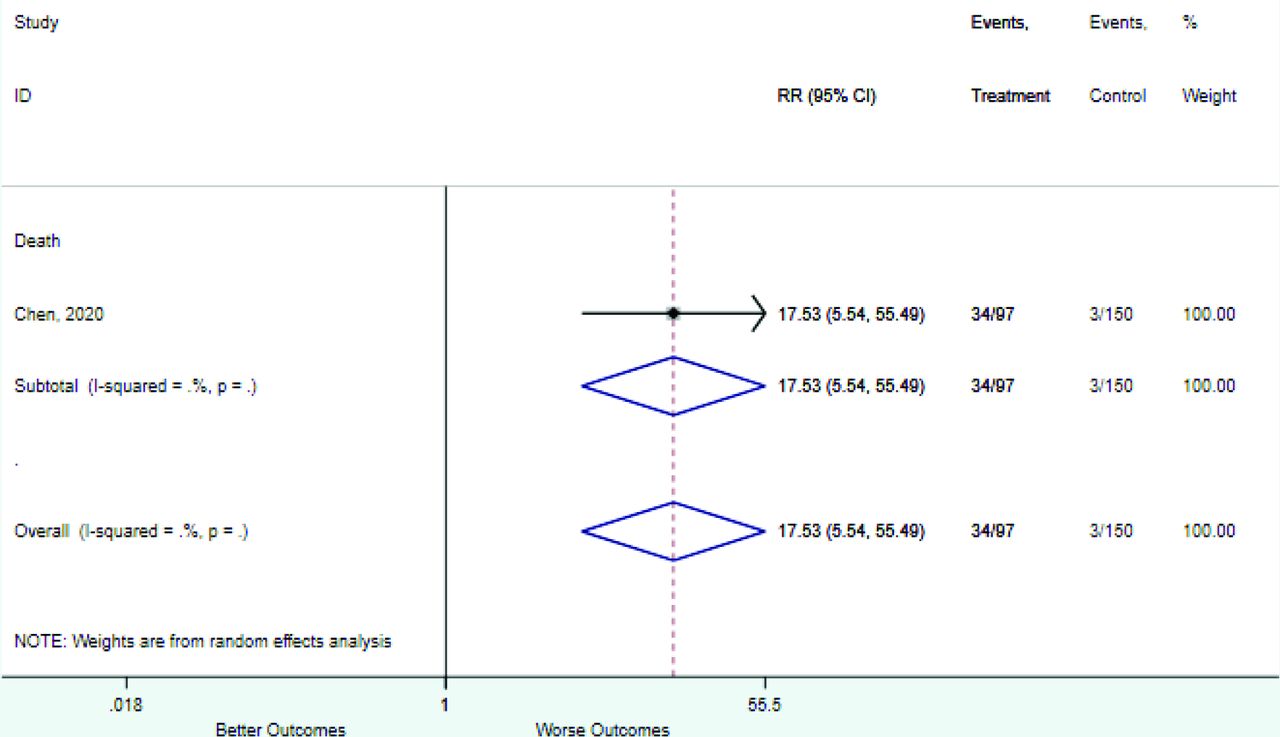
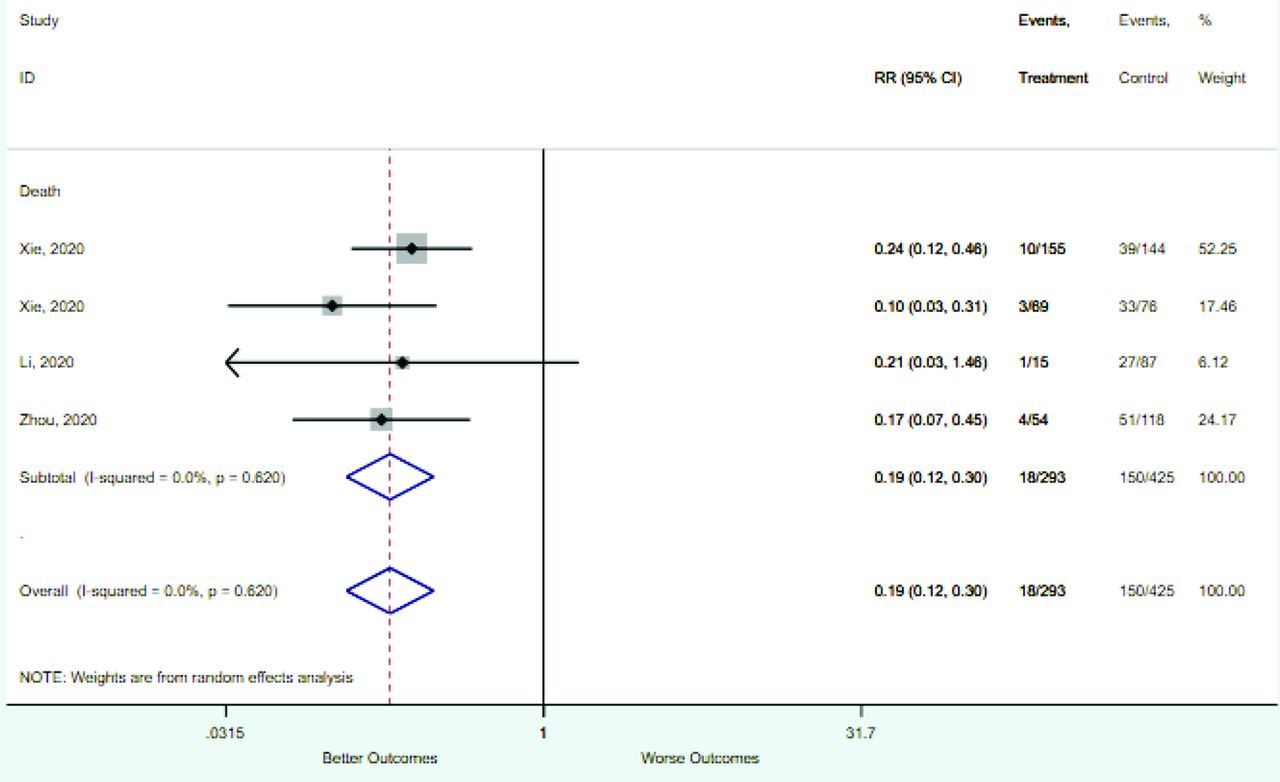
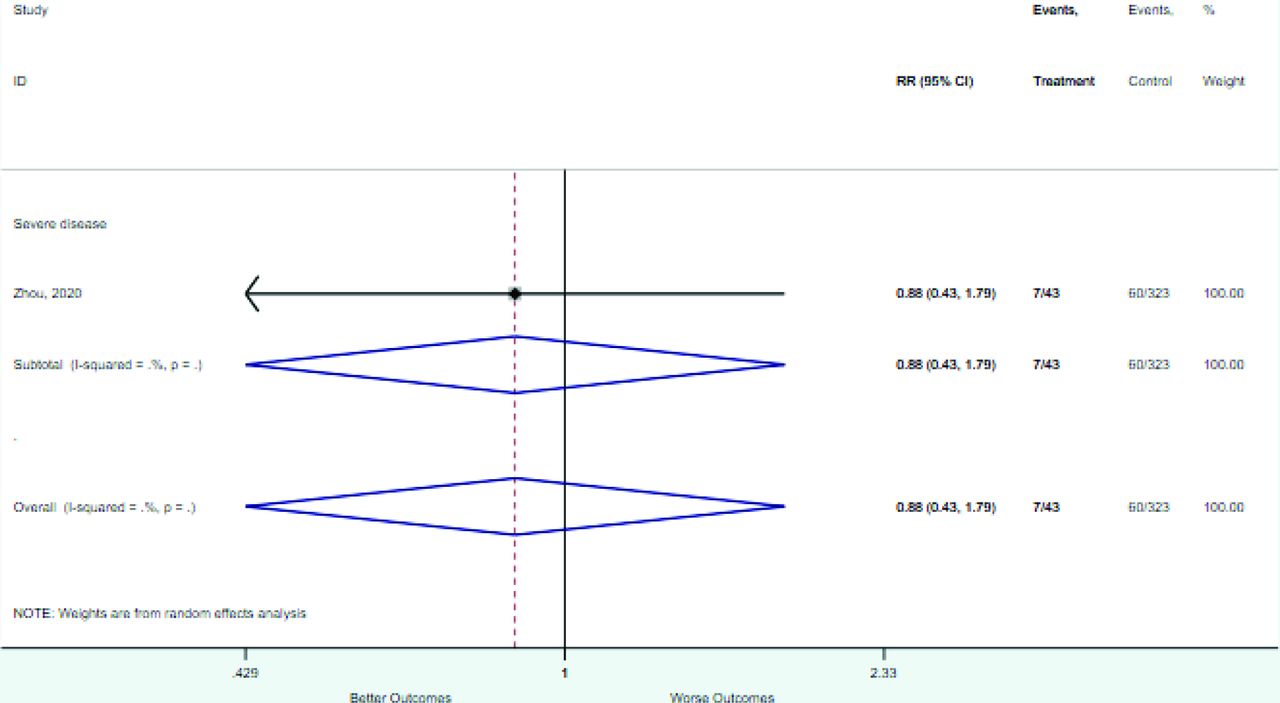
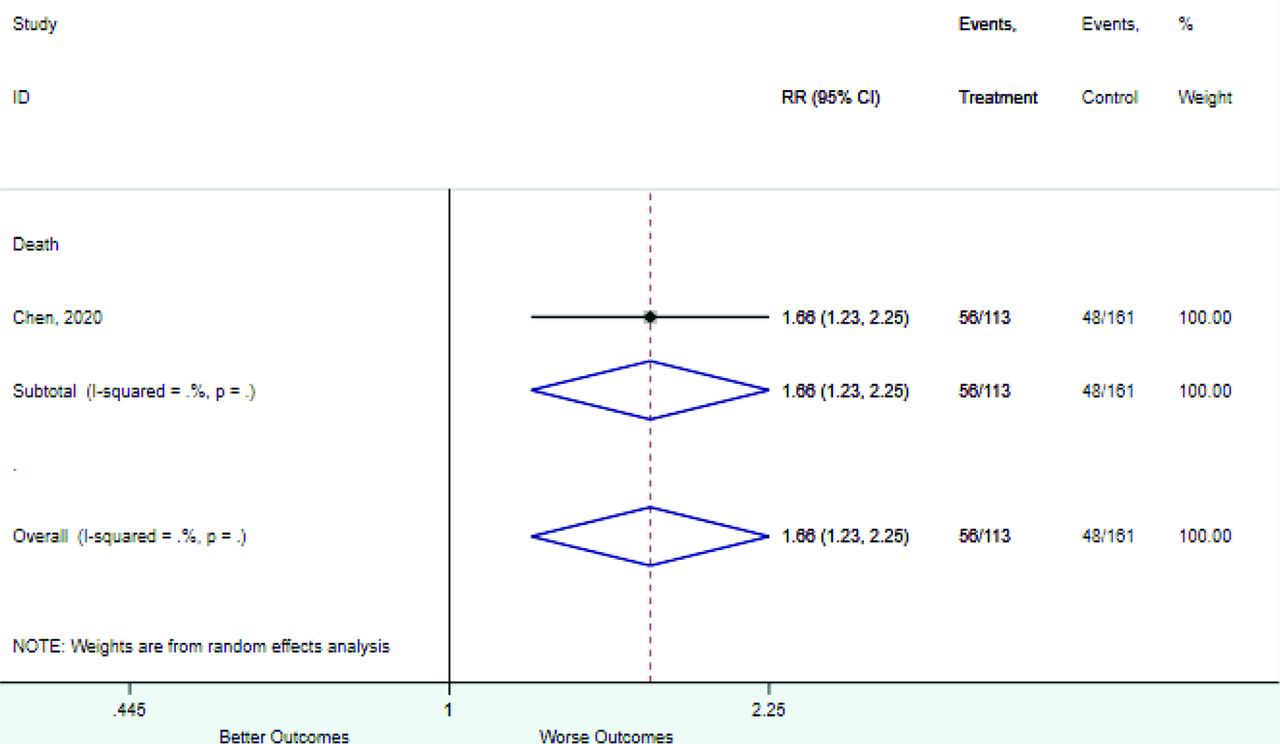
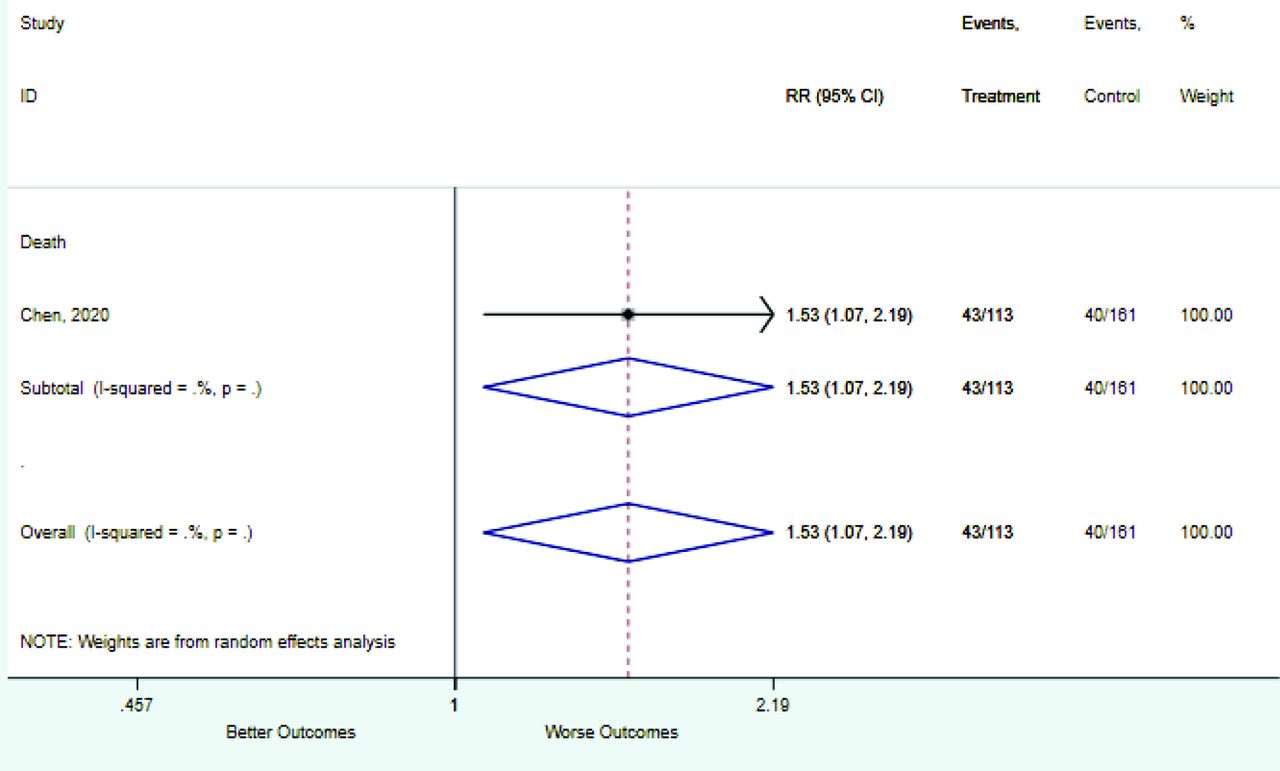
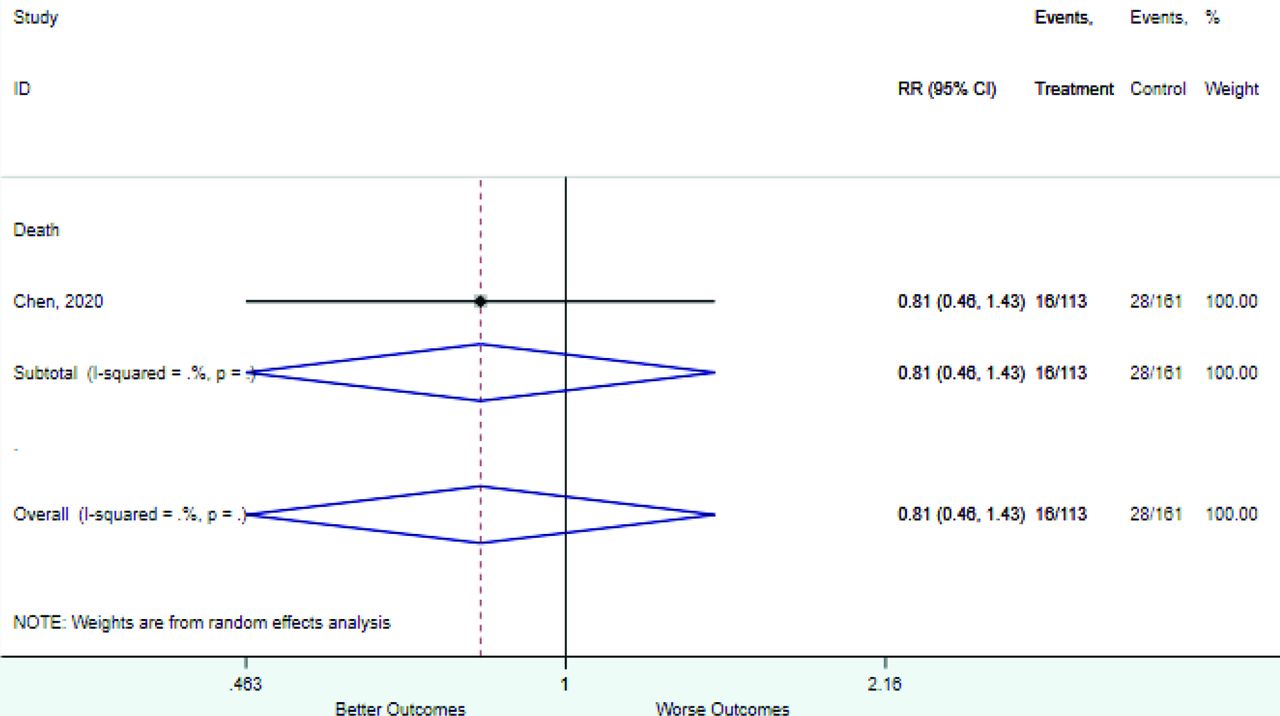
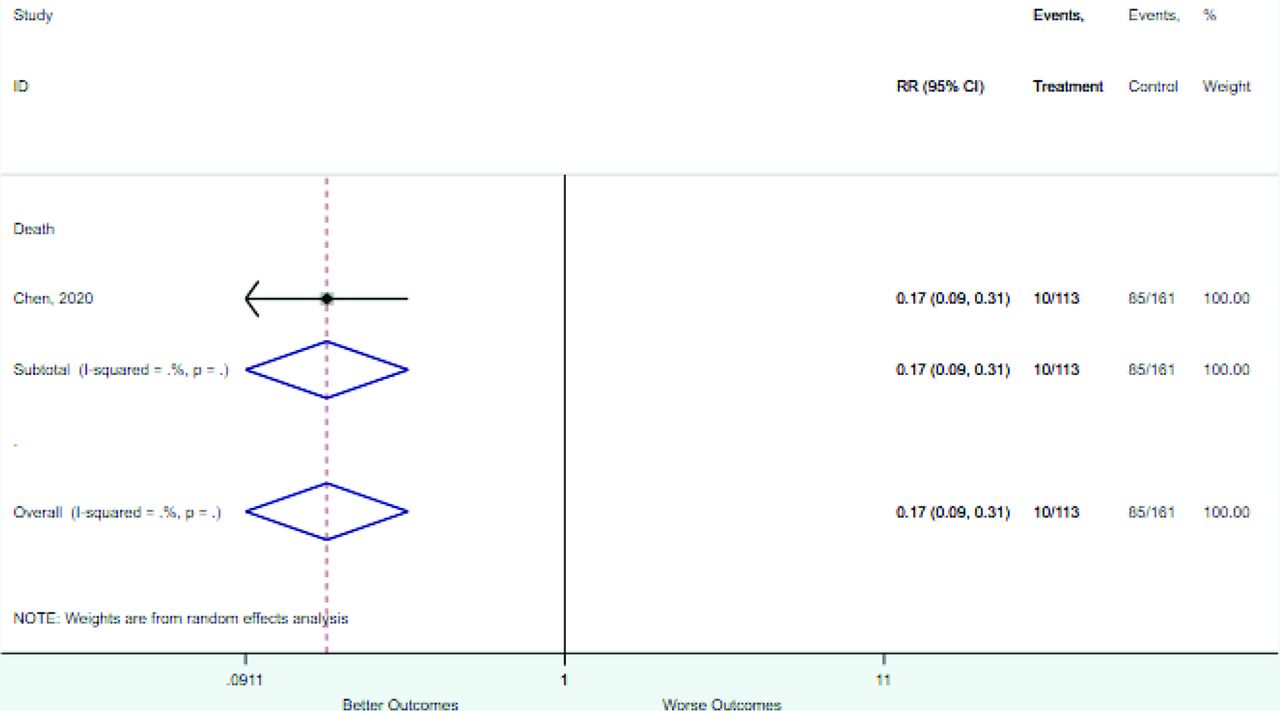
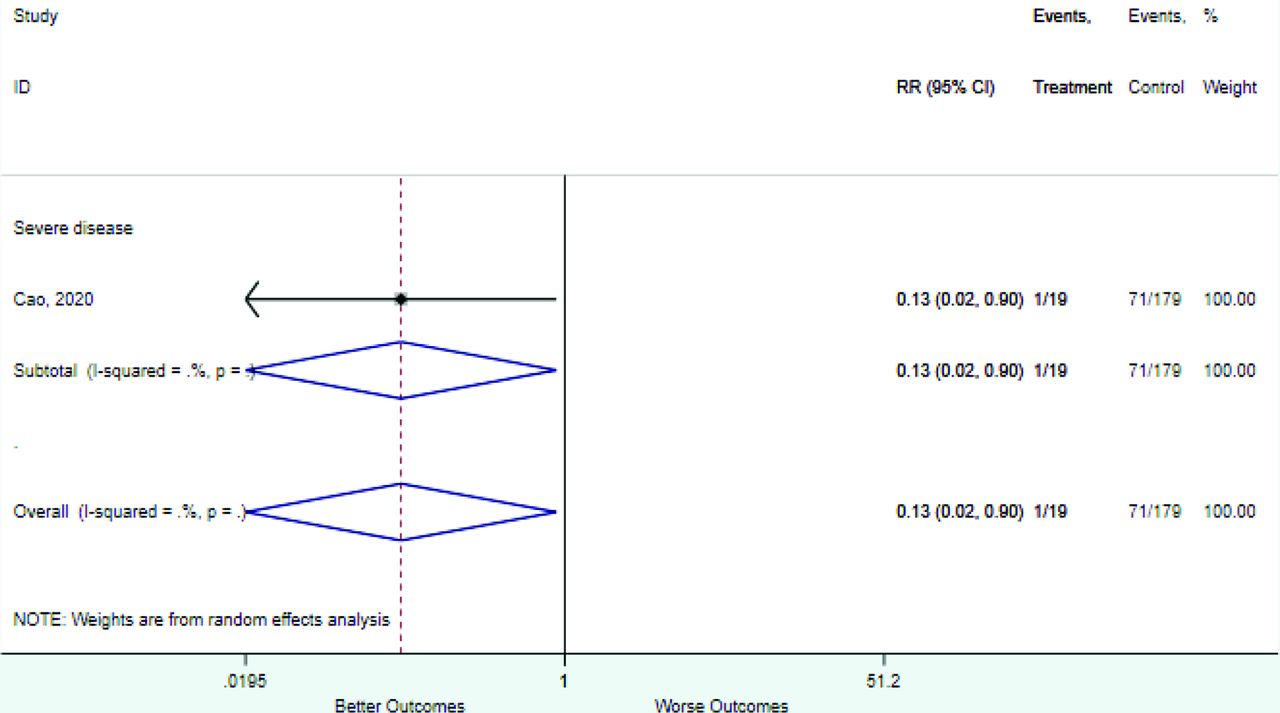
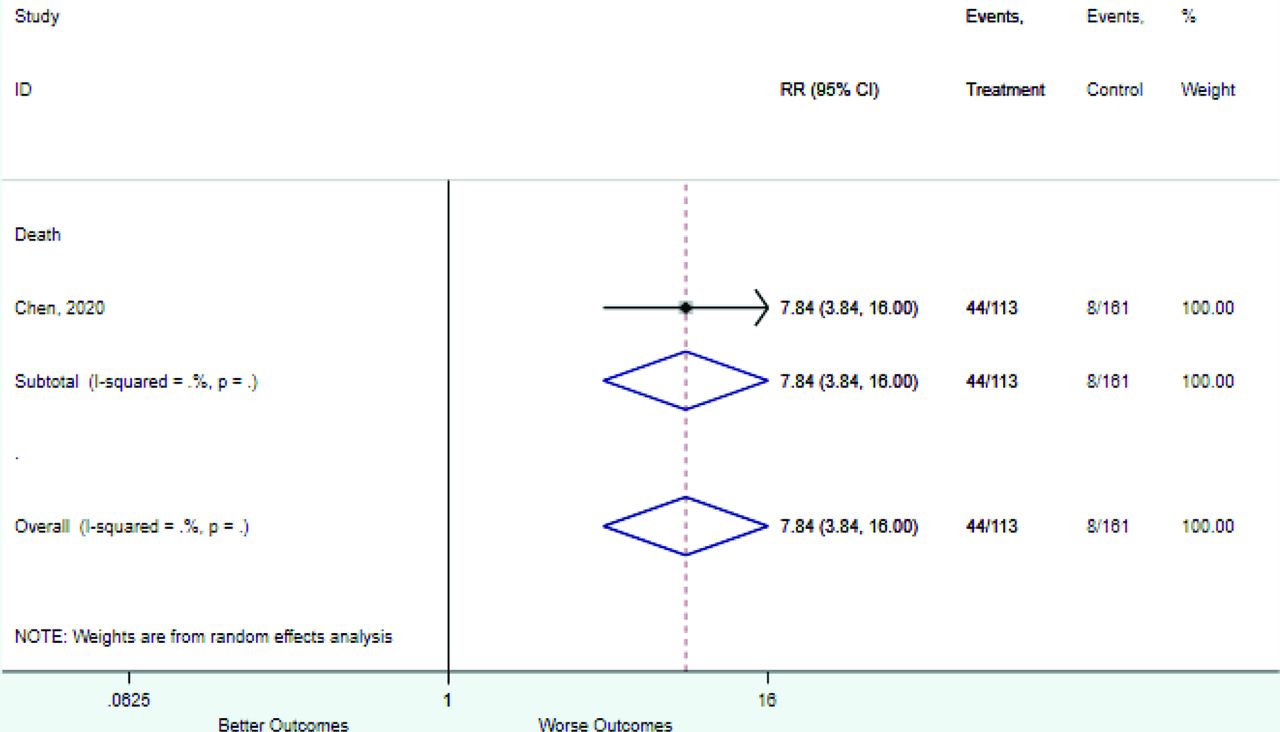
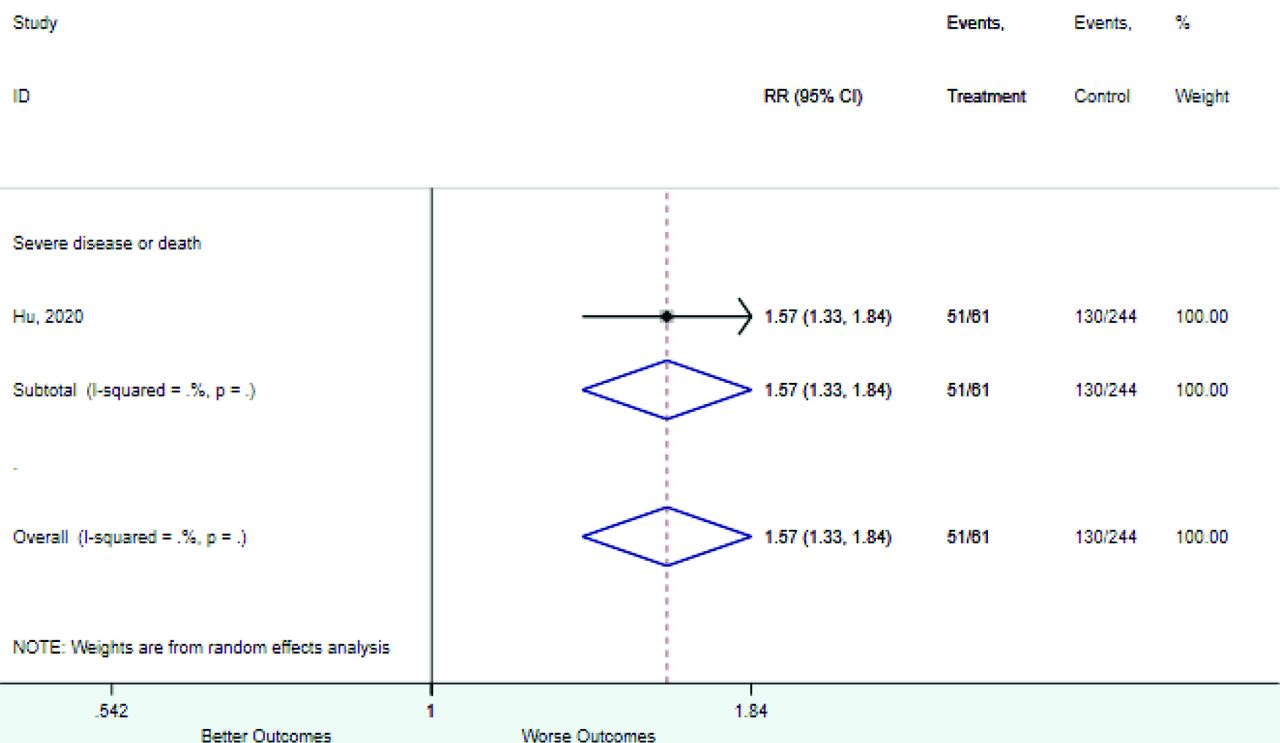
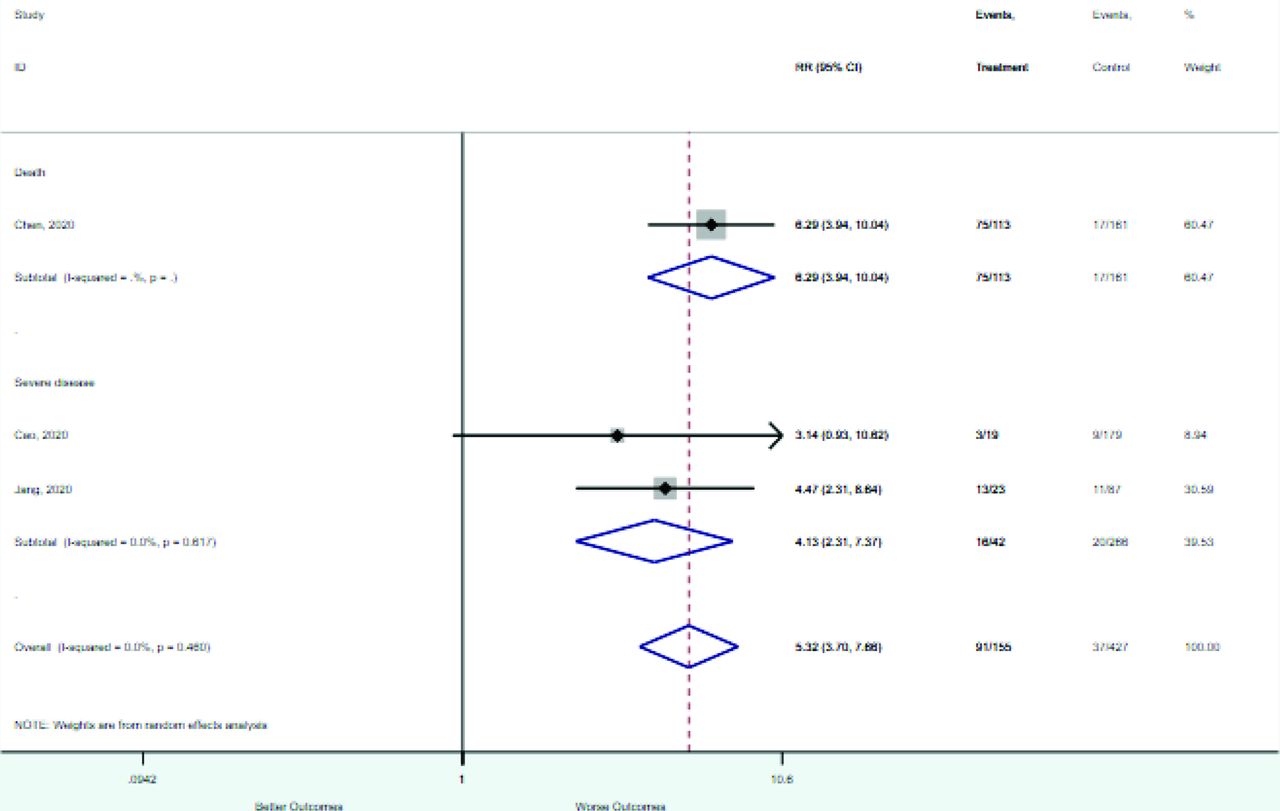
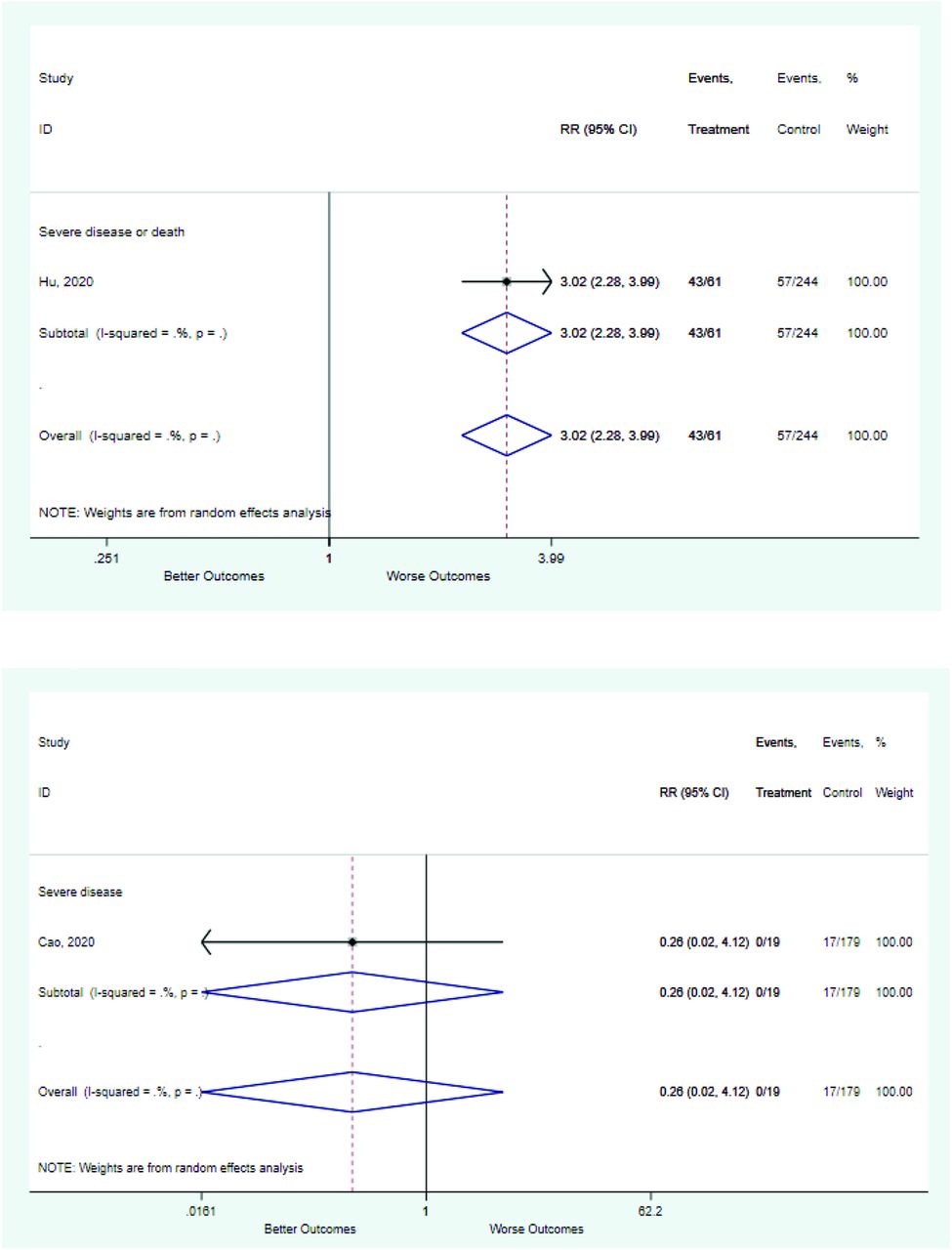
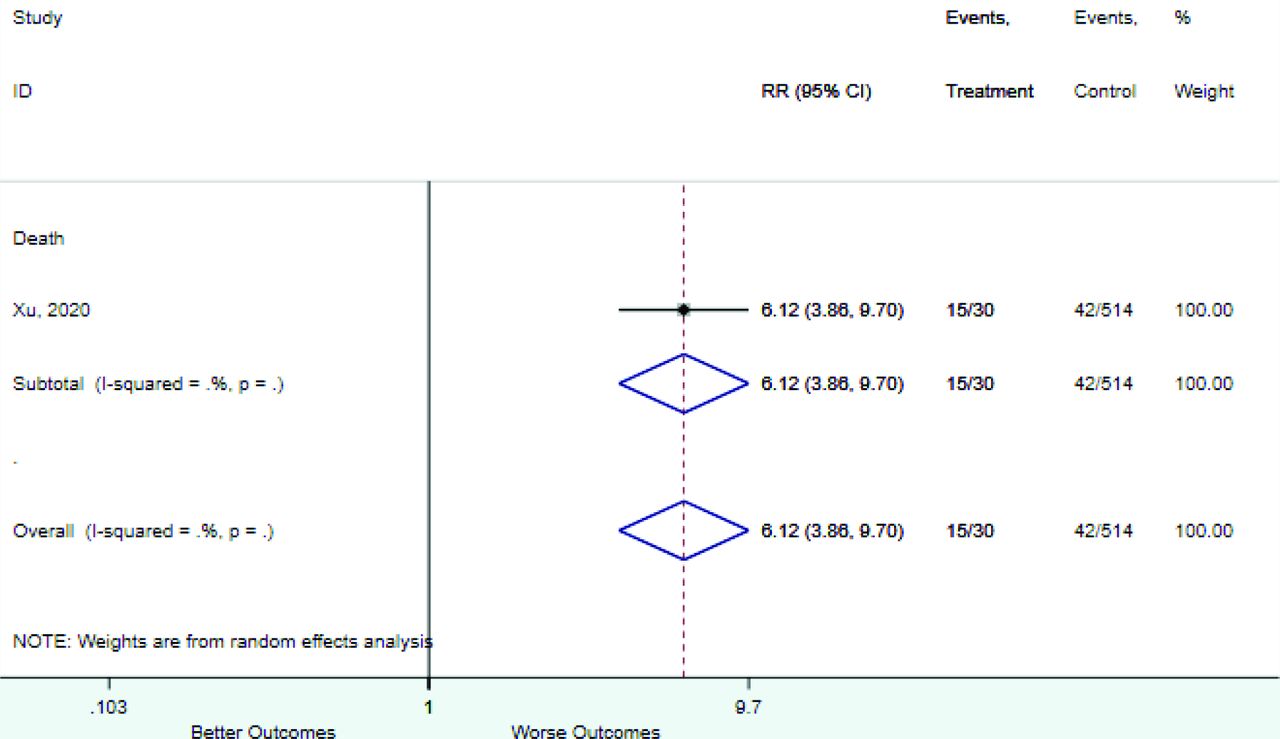
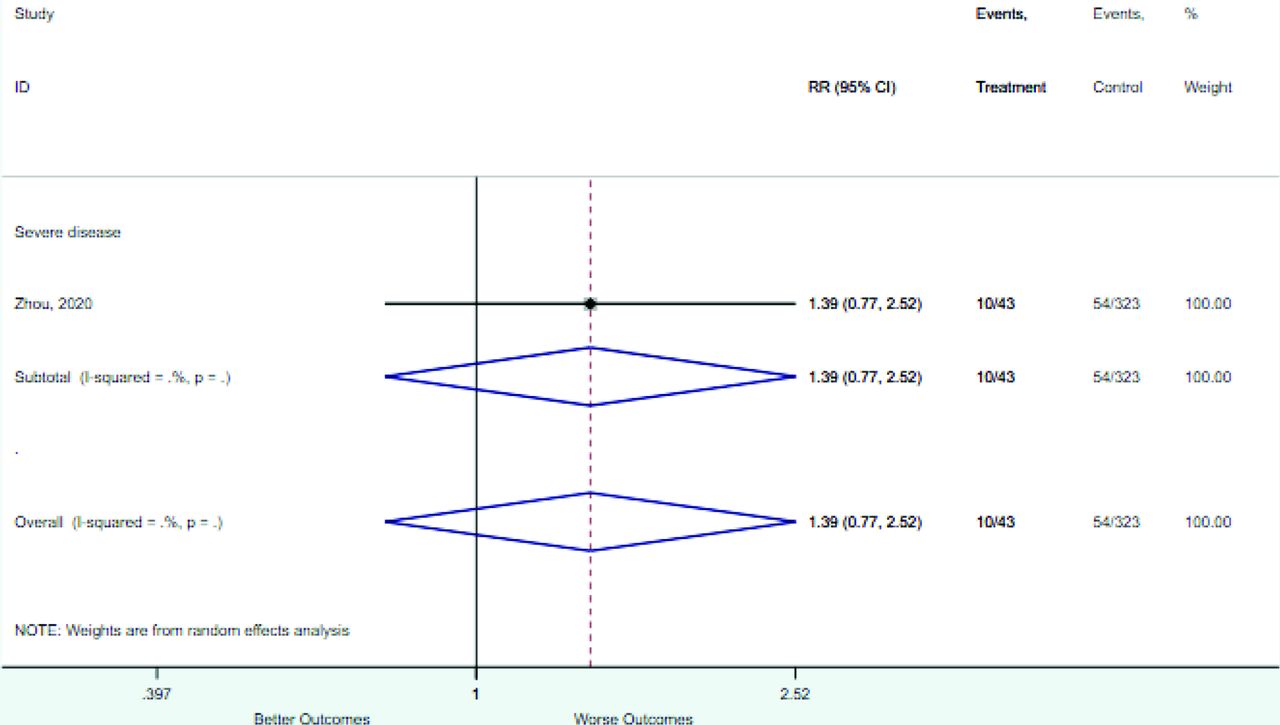
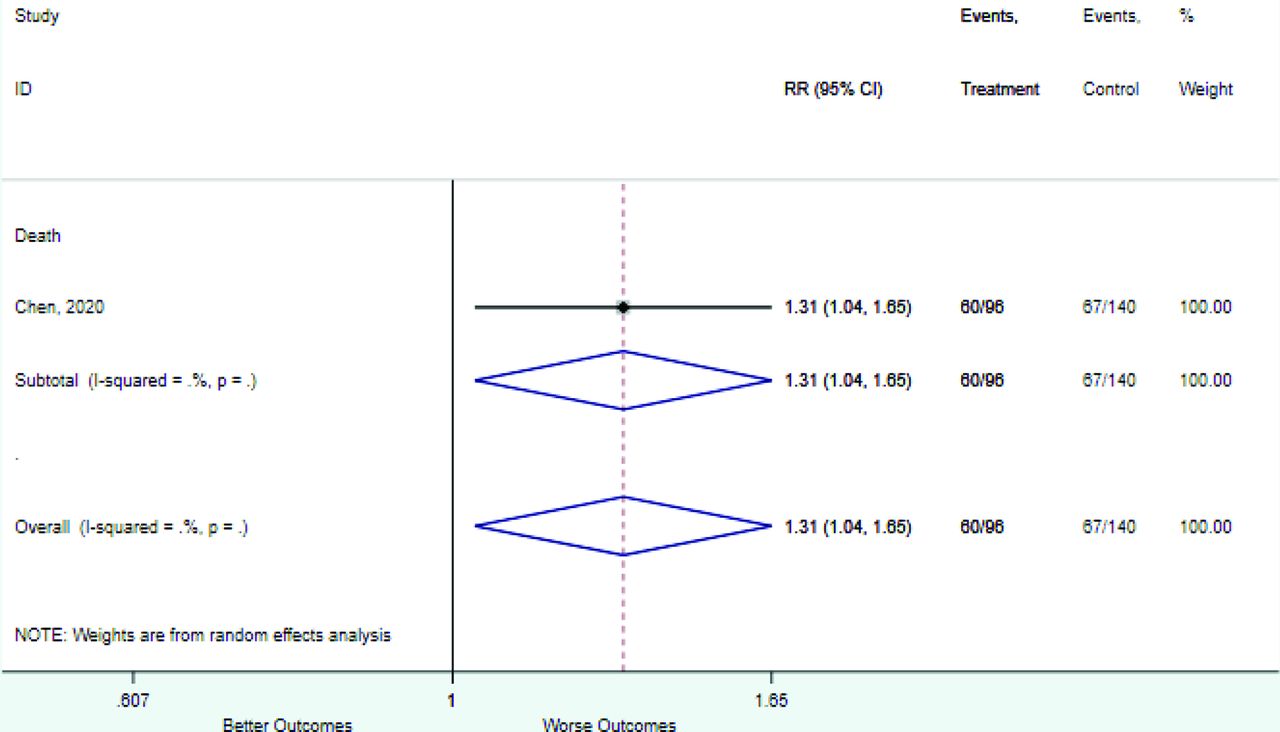
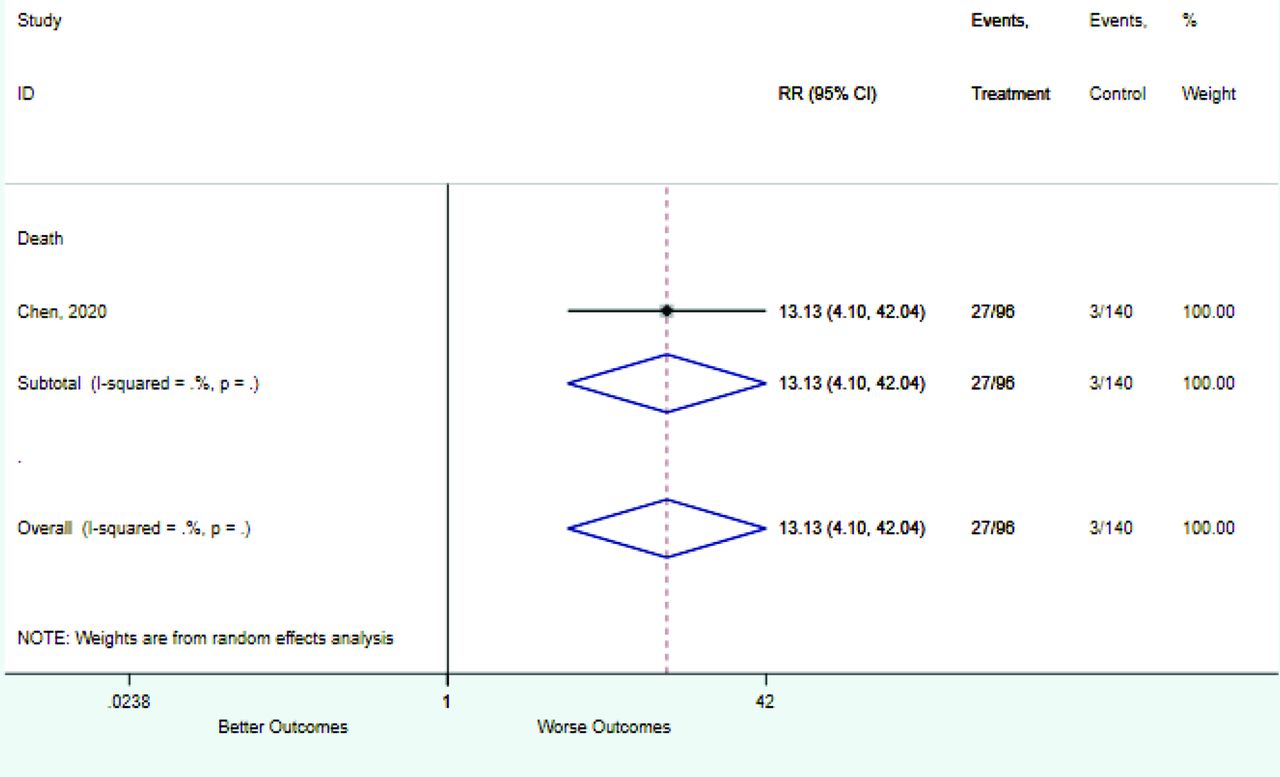
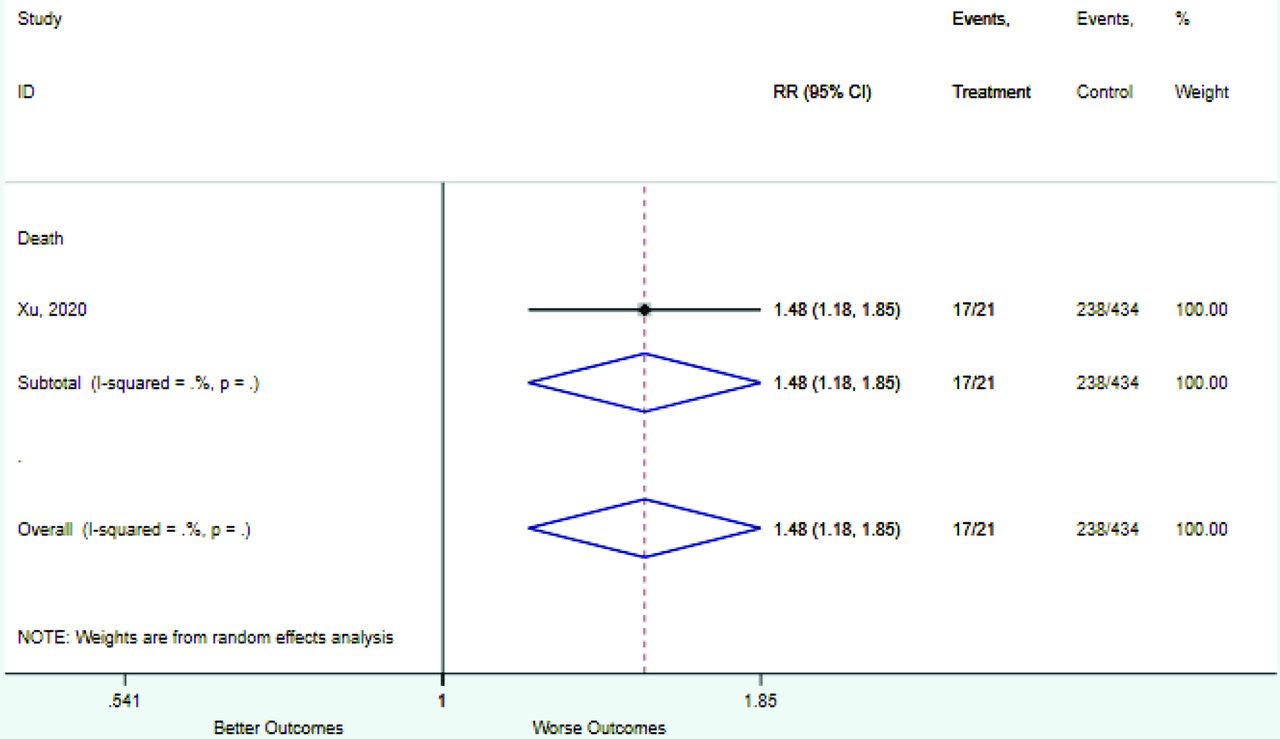
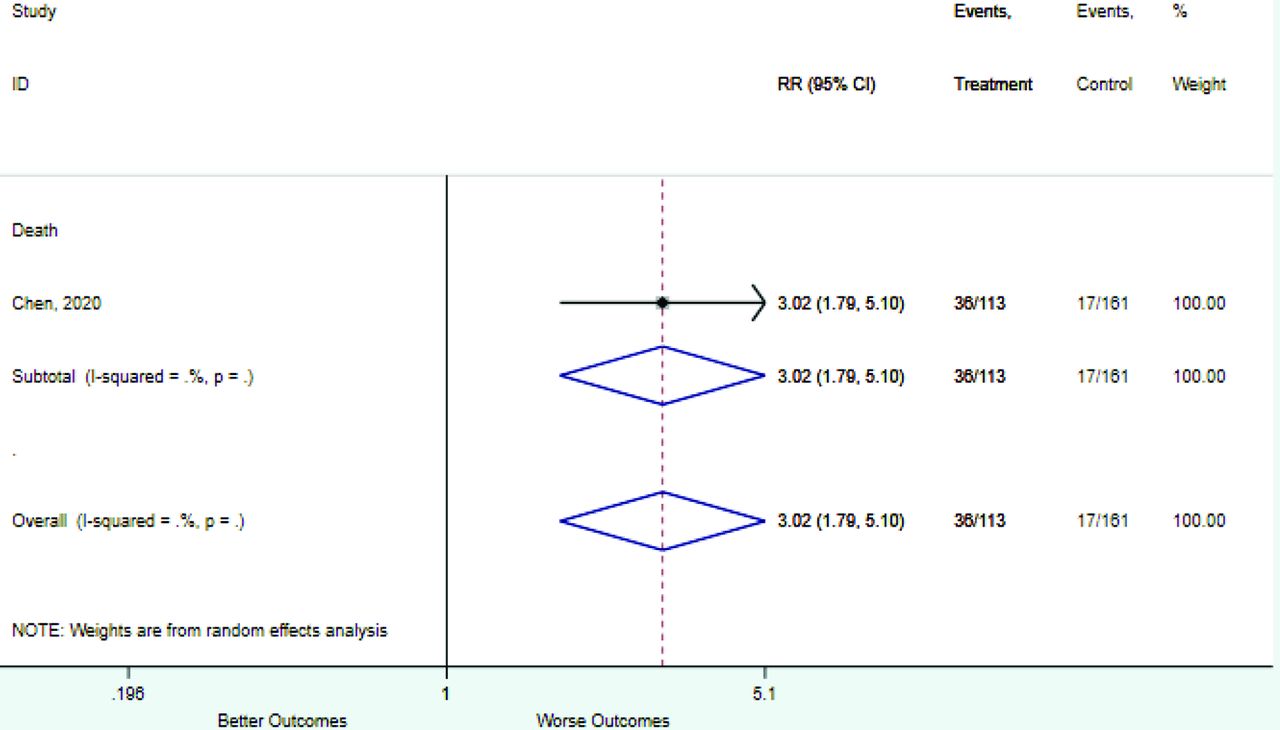
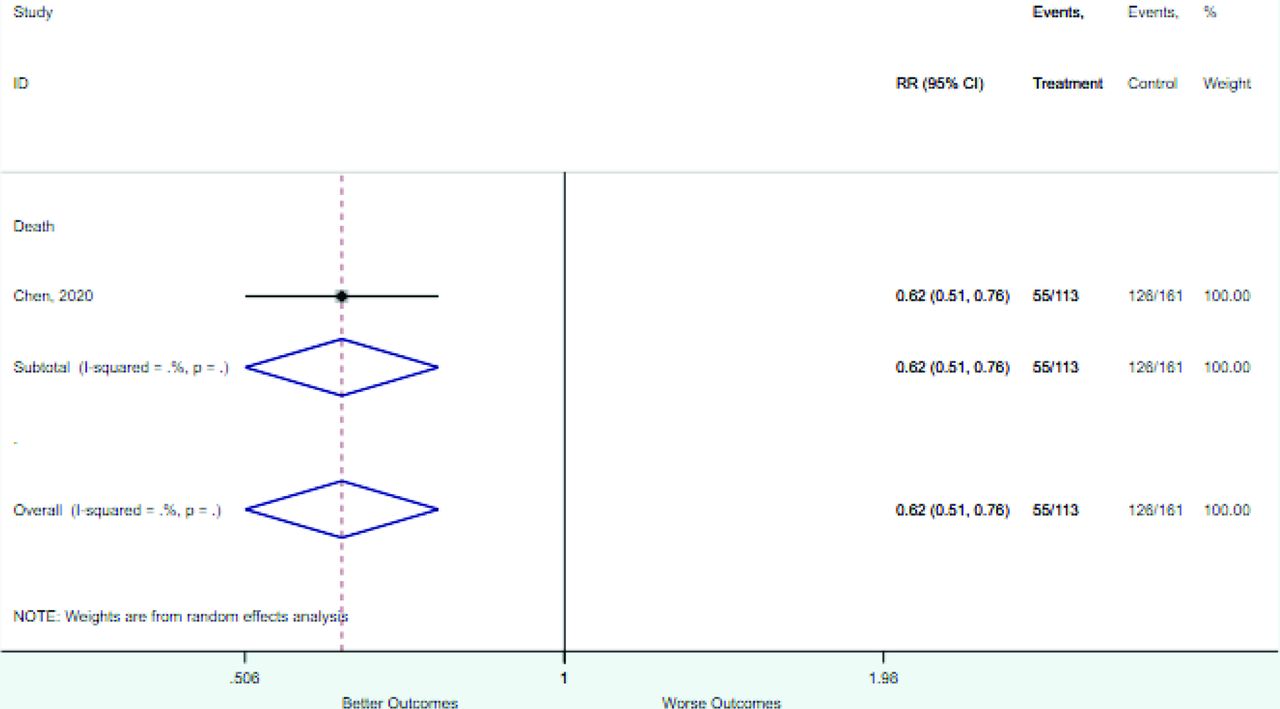
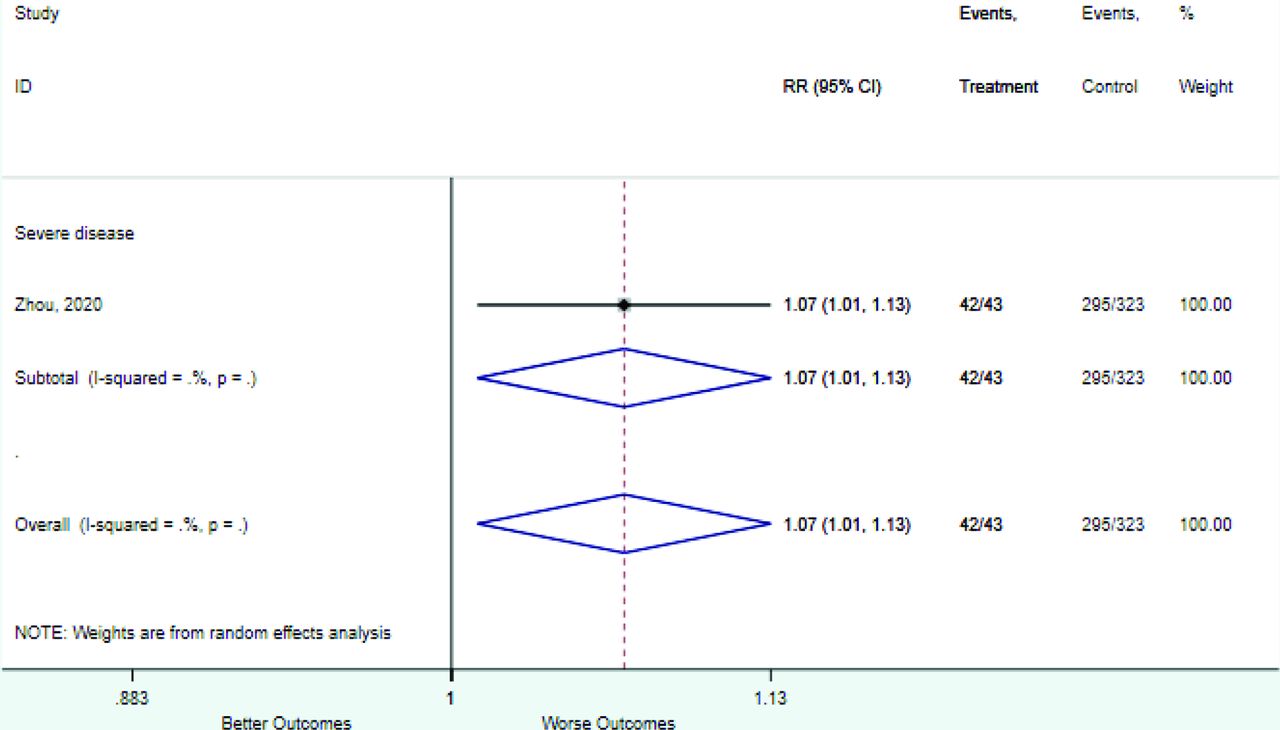
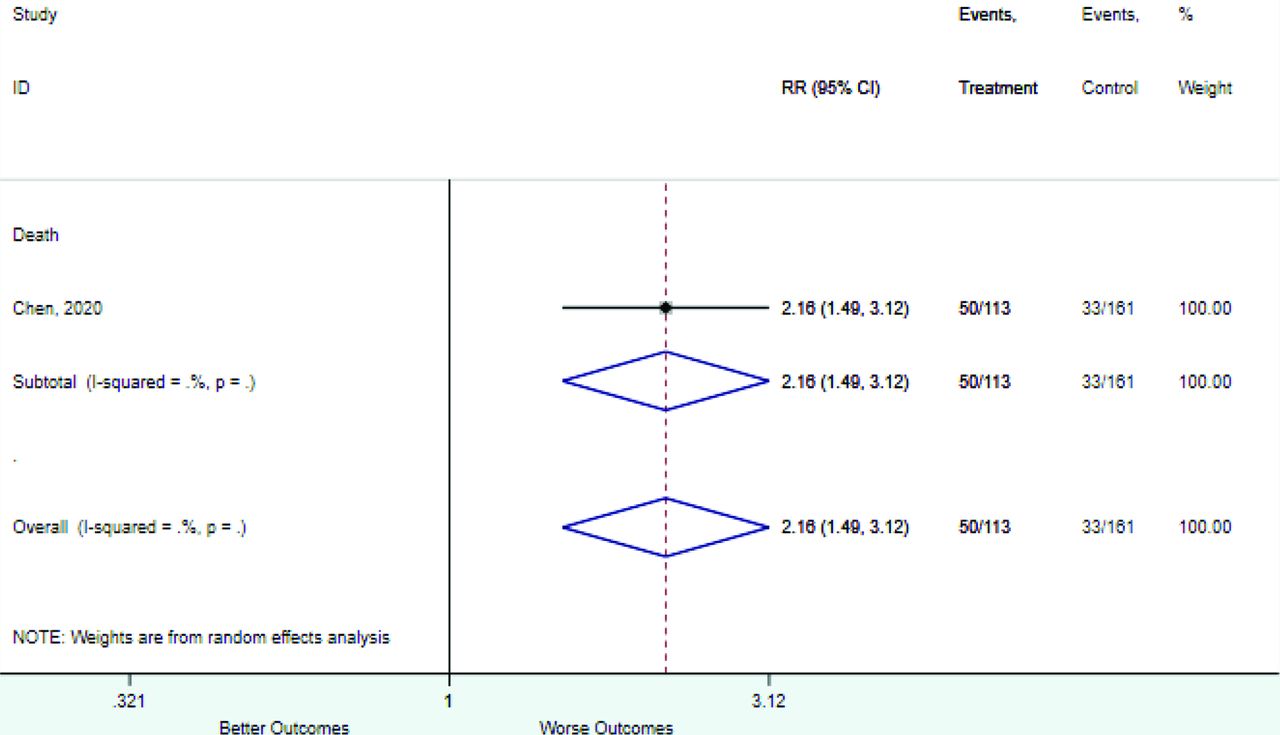
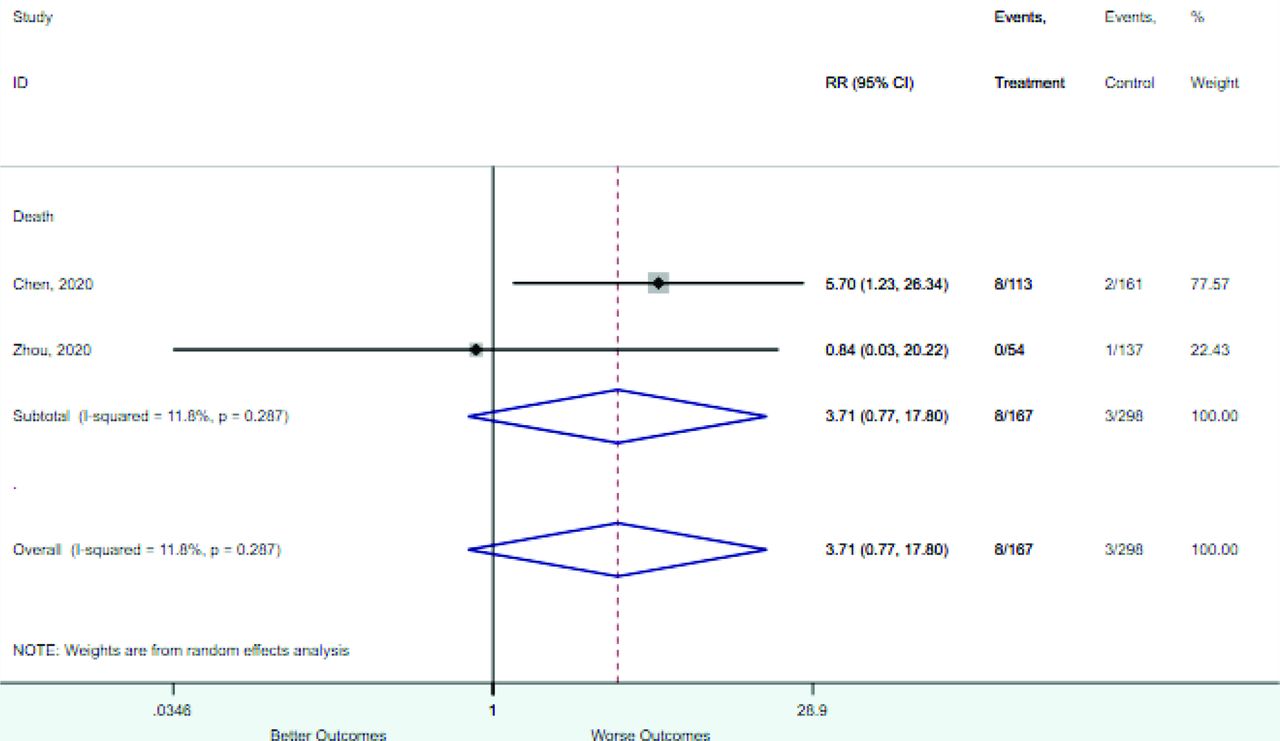
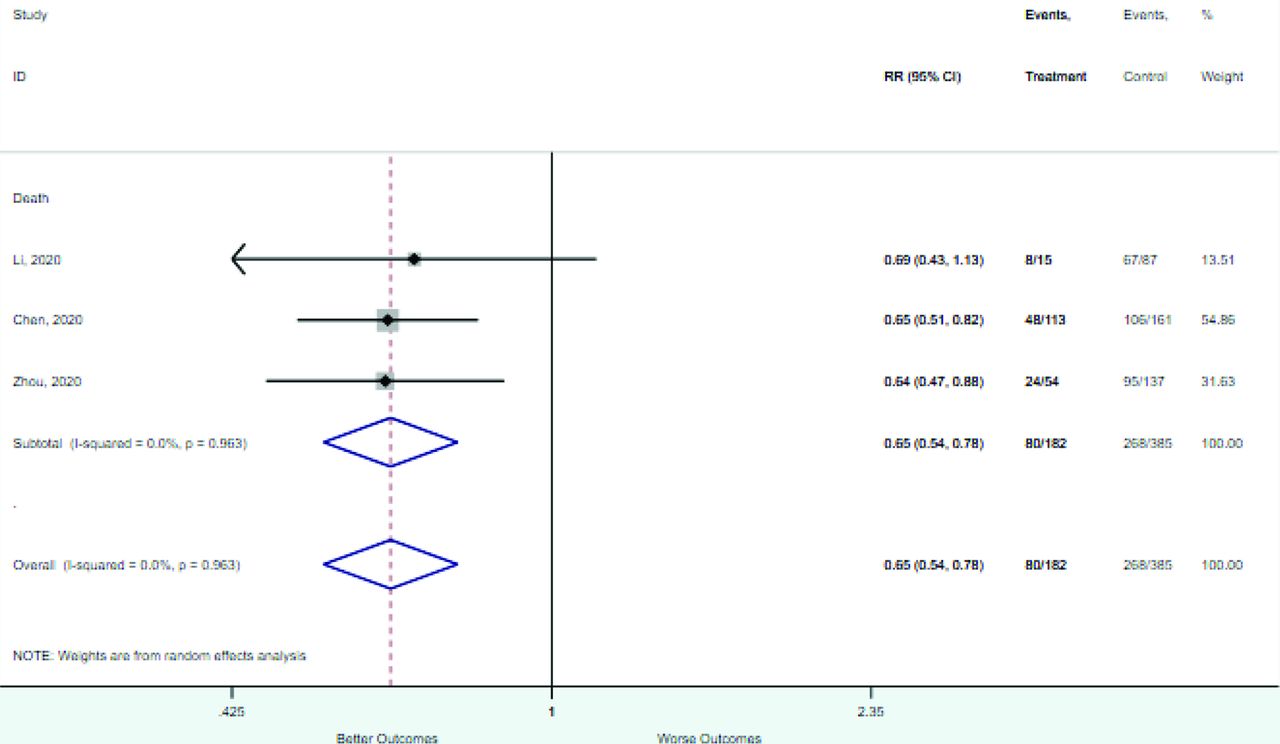
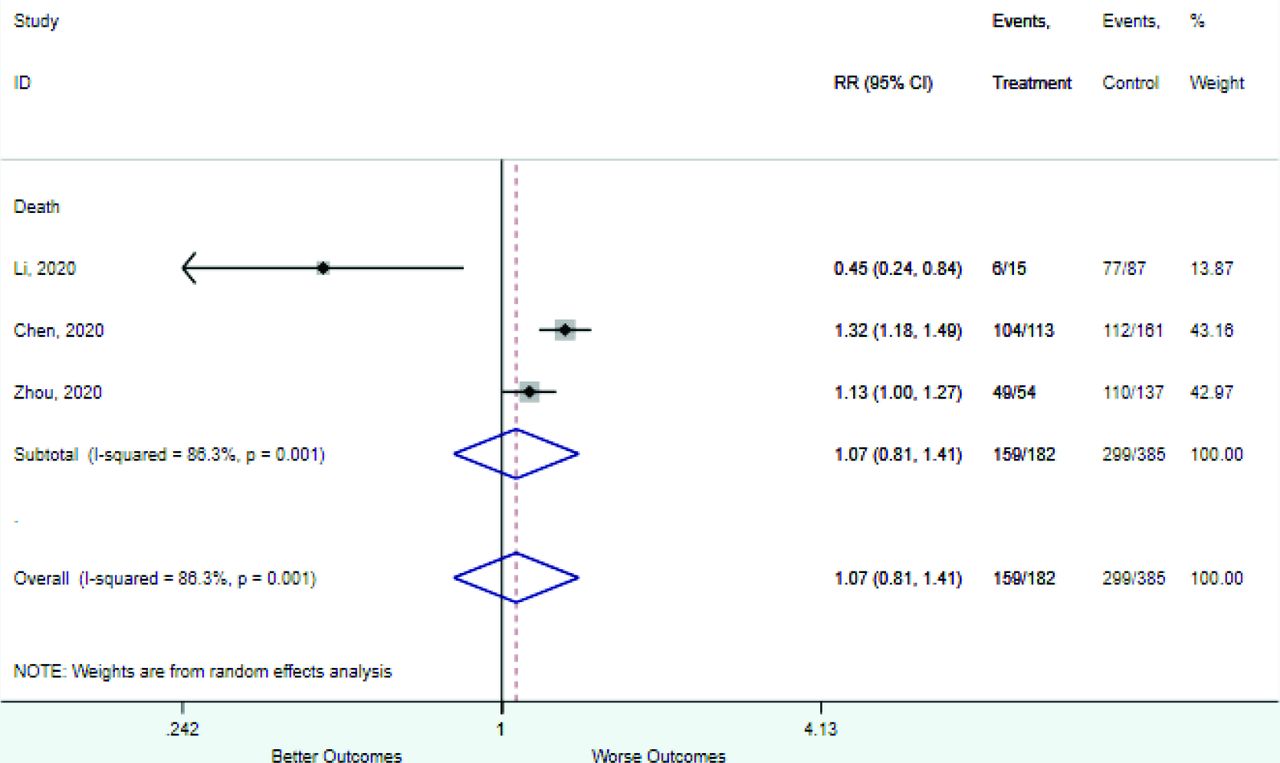
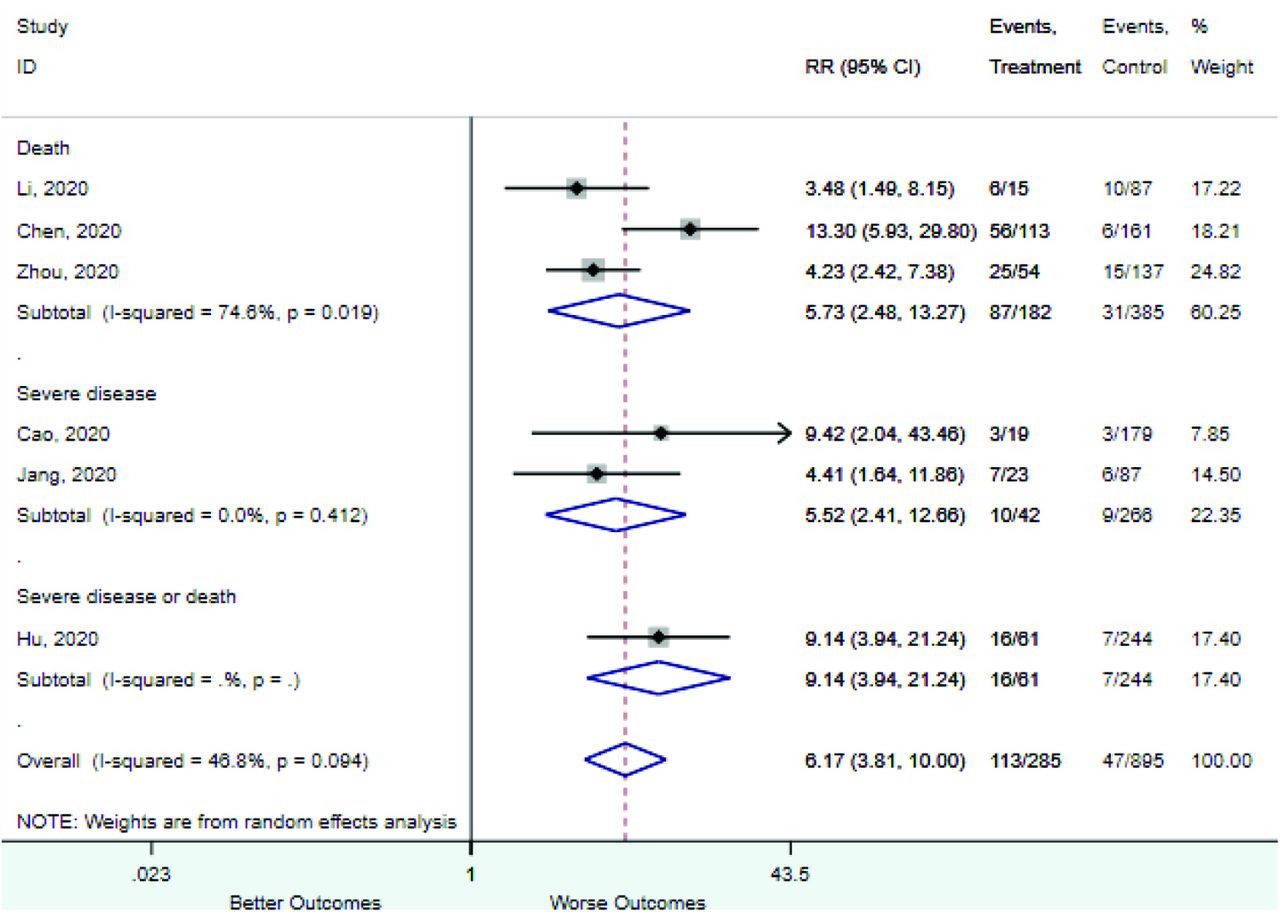
Risk Factor Studies Patients RR (95% CI) Outcome = Death Age <39 to 40 years 1 274 0.01 (0.00–0.21) Age <45 years 1 107 0.21 (0.06–0.79) Age >45 years 1 107 1.79 (1.38–2.32) Age >75 years 1 107 10.42 (3.58–30.33) Age ≥40 years 1 274 1.49 (1.33–1.66) Age ≥60 to 65 years 3 483 2.62 (1.91–3.58) Age 40–60 years 1 274 0.55 (0.34–0.89) Age 45–59 years 1 107 0.19 (0.03–1.34) Age 60–75 years 1 107 2.03 (0.97–4.23) Any comorbidity 1 692 2.99 (2.37–3.77) Chronic kidney disease 5 1562 5.11 (2.18–11.98) COPD 9 2213 3.79 (2.51–5.72) Coronary heart disease 9 2213 5.27 (2.89–9.58) Cough 5 1366 1.02 (0.93–1.13) CRP >100 mg/L 2 243 4.16 (2.71–6.37) CRP ≥3 mg/L 1 102 1.19 (1.04–1.36) CRP increased 1 581 1.42 (1.29–1.55) D-dimer ≤0.5 mg/L 4 718 0.19 (0.12–0.30) D-dimer >21 mg/L 1 247 17.53 (5.54–55.49) D-dimer ≥0.5 mg/L 3 569 1.54 (1.32–1.80) D-dimer ≥1.0 mg/L 4 718 2.56 (2.10–3.13) D-dimer 0.5–1.0 mg/L 4 718 0.45 (0.31–0.64) D-dimer increased 1 371 2.63 (1.91–3.63) Diabetes mellitus 9 2213 2.15 (1.46–3.15) Dyspnea 3 1073 3.47 (1.67–7.18) Fever 6 1530 1.10 (0.95–1.28) Heart rate >100 1 274 1.66 (1.23–2.25) Heart rate ≥125 1 191 12.55 (0.61–257.13) Hypertension 9 2213 2.34 (1.80–3.05) LDH increased 3 831 5.16 (0.72–37.09) Lymphocyte count <0.5 1 274 7.84 (3.84–16.00) Lymphocyte count <0.8 to 1.1 4 841 2.07 (1.51–2.84) Lymphocyte count ≥1 1 274 0.17 (0.09–0.31) Lymphocyte count 0.5–0.8 1 274 1.53 (1.07–2.19) Lymphocyte count 0.8–1 1 274 0.81 (0.46–1.43) Lymphocytes decreased 1 547 2.10 (1.87–2.36) Male sex 9 2213 1.24 (1.08–1.43) Neutrophil count >6.3 1 274 6.29 (3.94–10.04) Neutrophils increased 1 544 6.12 (3.86–9.70) Oxygen saturation <90 to 93 3 718 6.07 (4.27–8.63) Procalcitonin <0.05 ng/mL 1 236 0.02 (0.00–0.15) Procalcitonin <0.1 ng/mL 1 164 0.44 (0.31–0.64) Procalcitonin >0.05 ng/mL 1 102 1.79 (1.45–2.22) Procalcitonin ≥0.1 to 0.25 ng/mL 1 164 2.53 (1.34–4.79) Procalcitonin ≥0.25 to 0.5 ng/mL 4 728 9.59 (3.71–24.82) Procalcitonin ≥2.0 ng/mL 1 236 24.71 (1.44–423.13) Procalcitonin 0.05–0.5 ng/mL 1 236 1.31 (1.04–1.65) Procalcitonin 0.5–2.0 ng/mL 1 236 13.13 (4.10–42.04) Procalcitonin increased 1 455 1.48 (1.18–1.85) Respiratory rate <24 1 274 0.48 (0.38–0.60) Respiratory rate >20 to 30 4 841 3.80 (2.13–6.78) Respiratory rate 24–30 1 274 3.02 (1.79–5.10) SBP <90 mm Hg 2 274 5.70 (1.23–26.34) SBP ≥140 mm Hg 1 274 2.16 (1.49–3.12) SBP 90–140 mm Hg 1 274 0.62 (0.51–0.76) Troponin >34.2 1 101 6.96 (2.61–17.17) WBC < 3.5 to 4 3 567 0.34 (0.20–0.56) WBC ≥4 3 567 1.07 (0.81–1.41) WBC ≥9.5 to 10 3 567 5.73 (2.48–13.27) WBC 4–10 3 567 0.65 (0.54–0.78) WBC increased 1 630 16.08 (9.05–28.58) Outcome = severe disease or death Age ≥40 years 1 323 1.13 (1.07–1.19) Age ≥60 to 65 years 1 323 2.06 (1.56–2.74) Chronic kidney disease 1 1590 4.45 (1.76–11.29) COPD 2 1913 5.63 (1.07–29.69) Coronary heart disease 1 1590 3.15 (1.75–5.57) Cough 2 1821 1.06 (0.96–1.17) CRP ≥3 mg/L 1 306 1.13 (1.07–1.19) Diabetes mellitus 2 1913 3.24 (2.41–4.36) Dyspnea 2 1717 3.09 (2.59–3.68) Fever 2 1859 1.01 (0.96–1.07) Hypertension 2 1913 2.00 (1.06–3.78) LDH increased 1 87 3.32 (1.75–6.32) Lymphocyte count <2.0 1 305 1.57 (1.33–1.84) Male sex 2 1901 1.19 (1.06–1.33) Neutrophil count >7.5 1 305 3.02 (2.28–3.99) WBC ≥9.5 to 10 1 305 9.14 (3.94–21.24) Outcome = severe disease Age <39 to 40 years 1 198 0.29 (0.08–1.11) Age >75 years 1 2729 1.69 (1.49–1.93) Age ≥40 years 1 198 1.39 (1.15–1.68) Age ≥50 years 1 198 1.62 (1.23–2.14) Age ≥60 to 65 years 2 564 2.53 (1.89–3.40) Age ≥70 years 1 198 4.71 (2.33–9.53) Age 40–49 years 1 198 0.67 (0.17–2.61) Age 50–59 years 1 198 0.13 (0.01–2.11) Age 60–69 years 1 198 1.74 (0.90–3.33) Asthma or COPD 1 2729 1.05 (0.88–1.24) Chronic kidney disease 3 3516 3.02 (0.63–14.60) COPD 7 1033 2.47 (1.34–4.52) Coronary heart disease 9 4364 3.69 (1.75–7.77) Cough 9 1775 1.11 (0.87–1.42) CRP >5 to 10 mg/L 3 448 1.68 (1.47–1.93) D-dimer ≥0.5 mg/L 2 877 3.10 (1.45–6.64) Diabetes mellitus 11 4582 2.57 (1.59–4.17) spnea 7 1473 6.28 (3.10–12.74) Fever 10 4504 1.13 (1.05–1.22) Heart rate ≥90 1 366 0.88 (0.43–1.79) Hypertension 11 4582 2.29 (1.61–3.26) LDH increased 1 110 2.65 (1.93–3.63) Lymphocyte count <0.8 to 1.1 2 308 27.36 (0.96–778.27) Lymphocyte count >3.2 1 198 0.13 (0.02–0.90) Male sex 11 4582 1.30 (1.11–1.53) Neutrophil count <1.8 1 198 0.26 (0.02–4.12) Neutrophil count >6.3 1 308 4.13 (2.31–7.37) Oxygen saturation <88 1 2729 3.69 (3.06–4.46) Oxygen saturation <96 1 366 1.39 (0.77–2.52) Procalcitonin >0.05 ng/mL 3 448 4.06 (0.65–25.29) Respiratory rate >20 to 30 2 477 2.11 (0.20–22.05) SBP ≥110 mm Hg 1 366 1.07 (1.01–1.13) WBC <3.5 to 4 1 198 0.67 (0.17–2.61) WBC ≥9.5 to 10 2 308 5.52 (2.41–12.66) COPD = chronic obstructive pulmonary disease; RR, risk ratio; CI, confidence interval; CRP, c-reactive protein; LDH, lactate dehydrogenase; WBC, white blood count; SBP, systolic blood pressure.
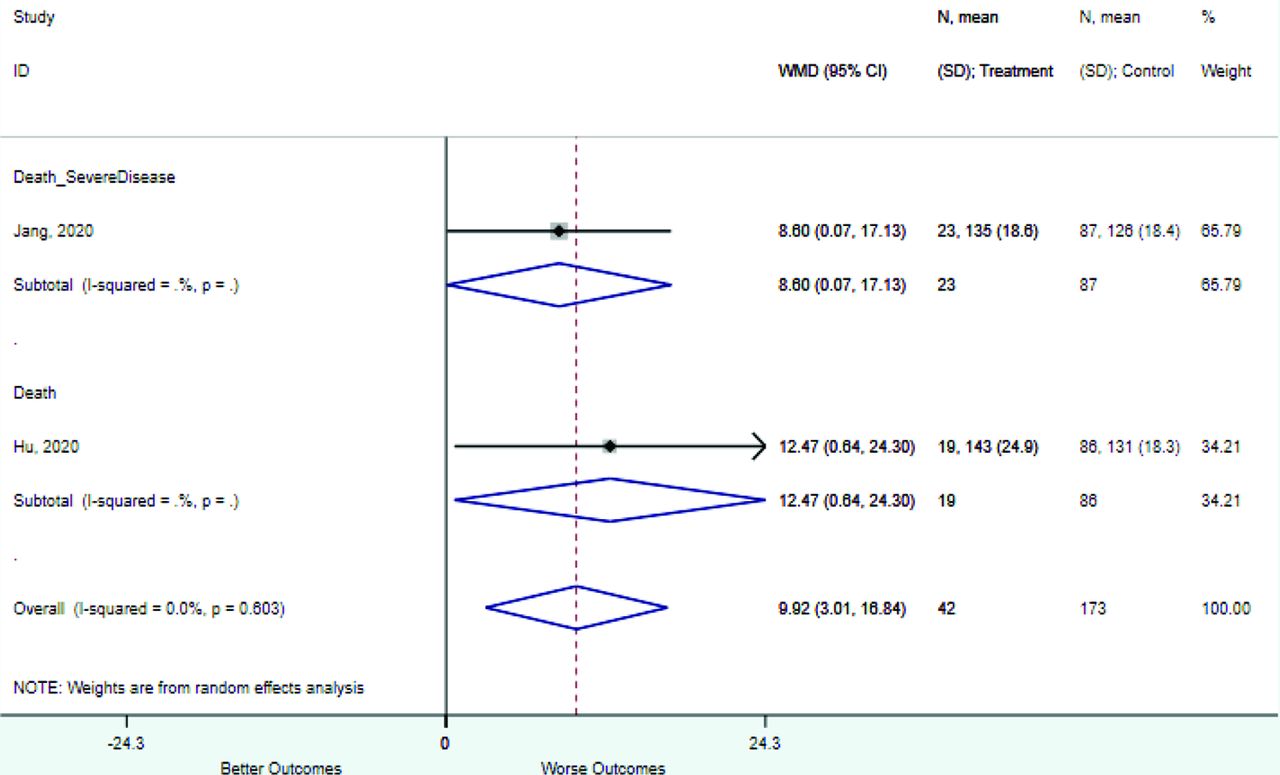
Association between Continuous Variables and Mortality, Severe Disease, or Both in Patients with COVID-19: Full Data Set
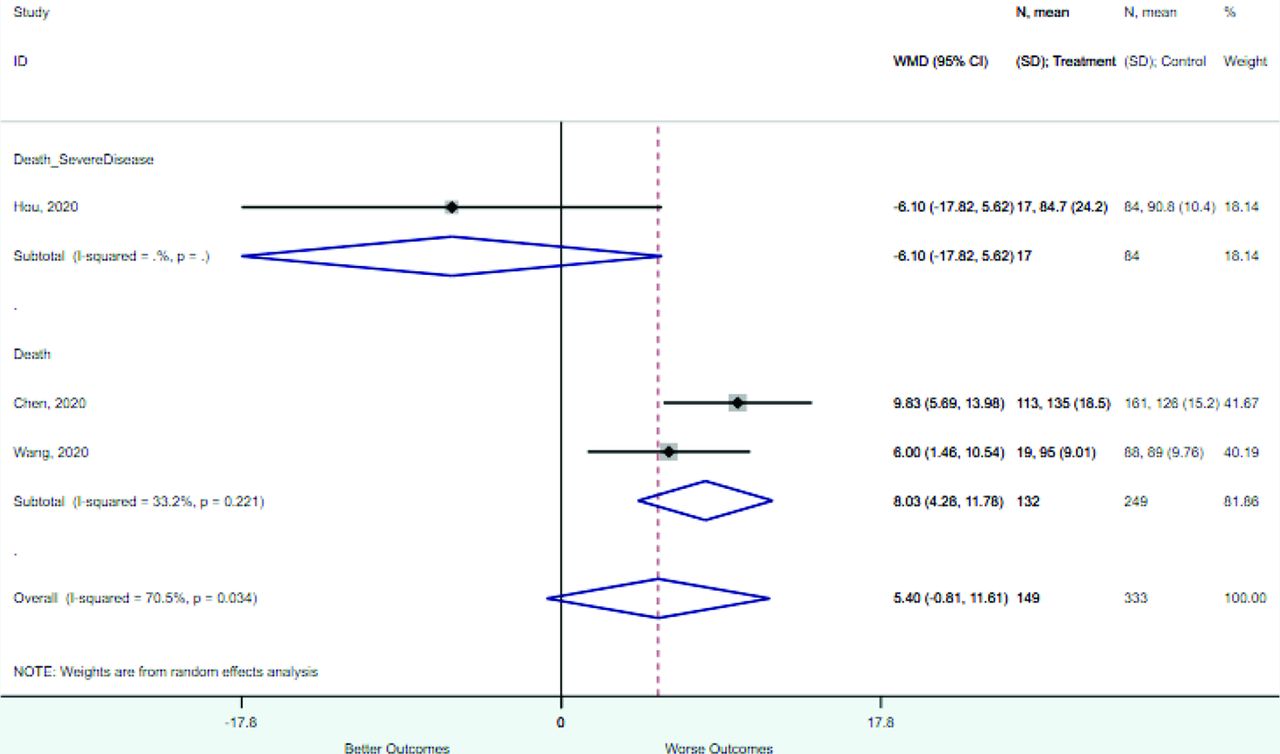
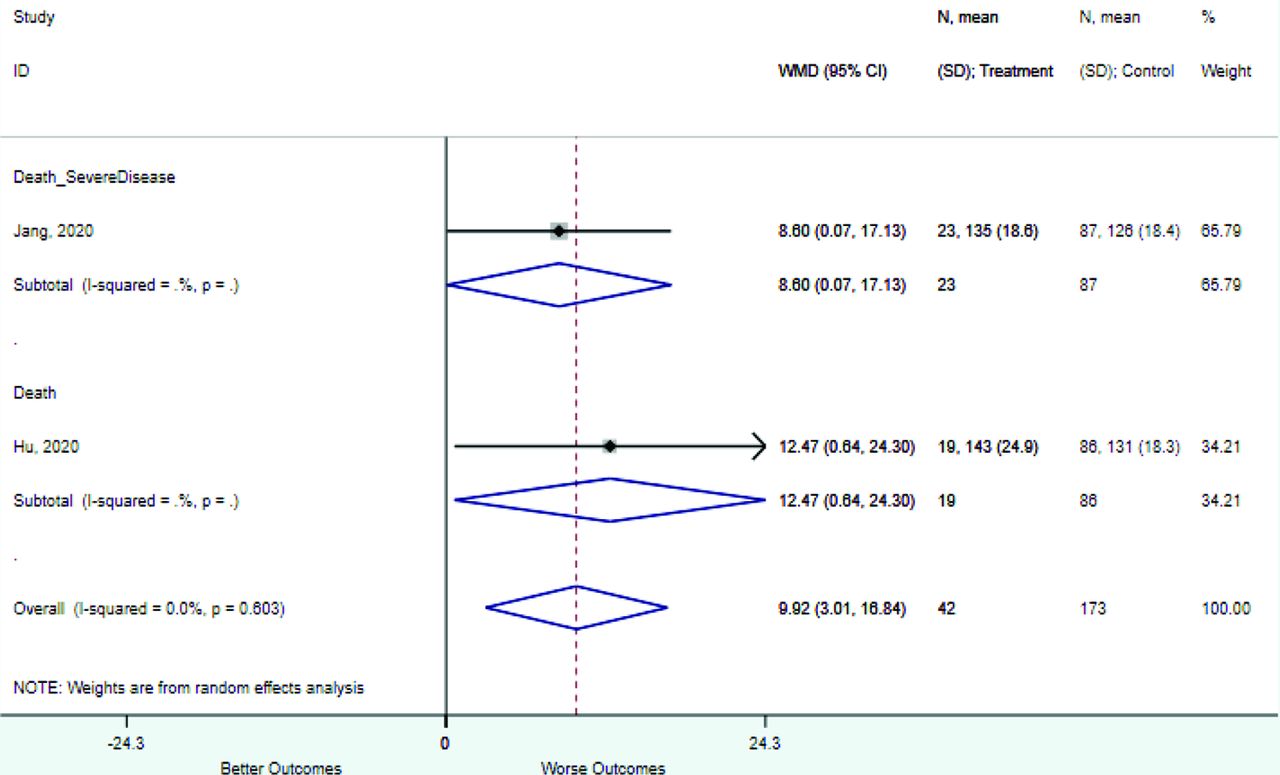
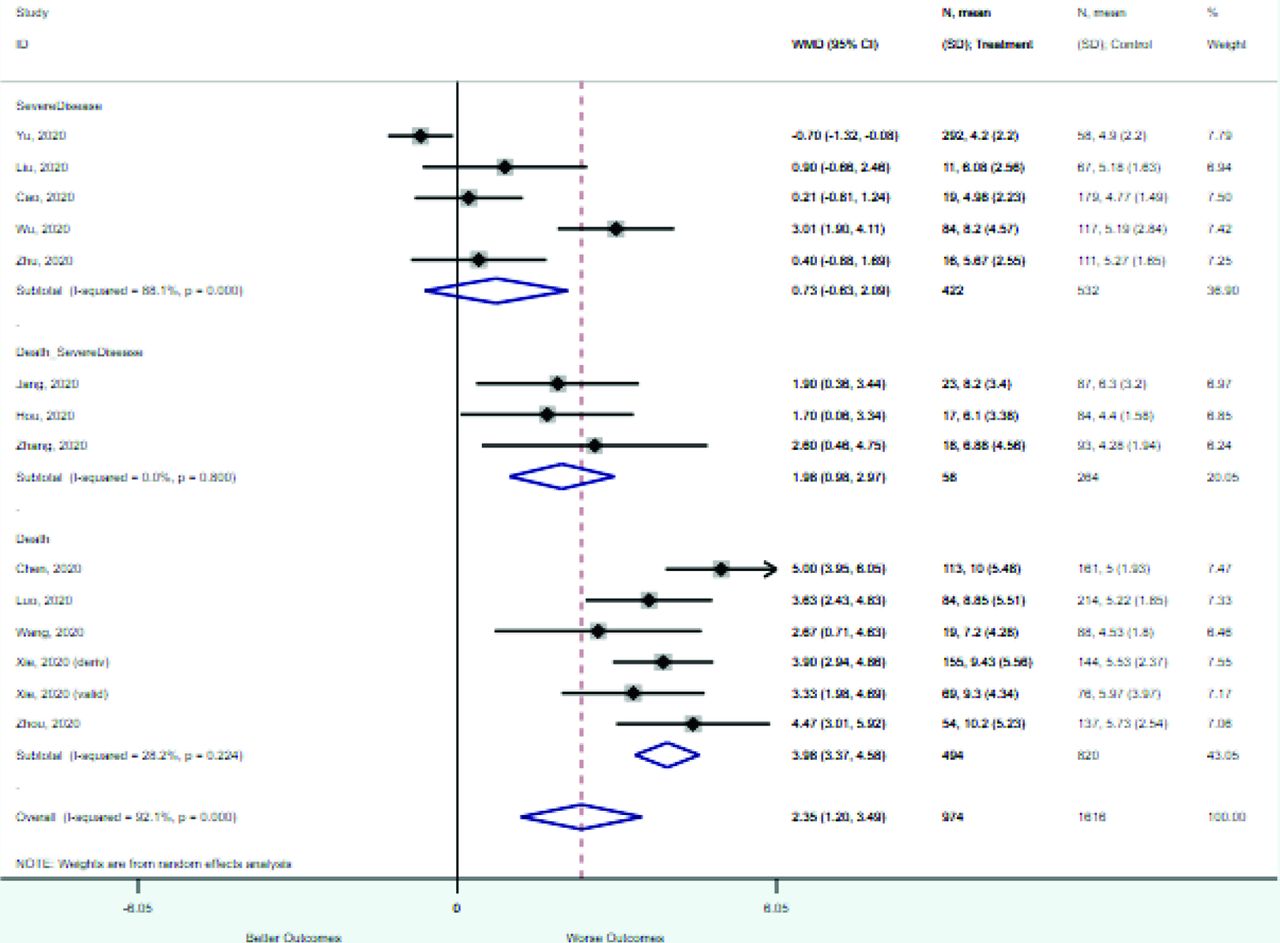
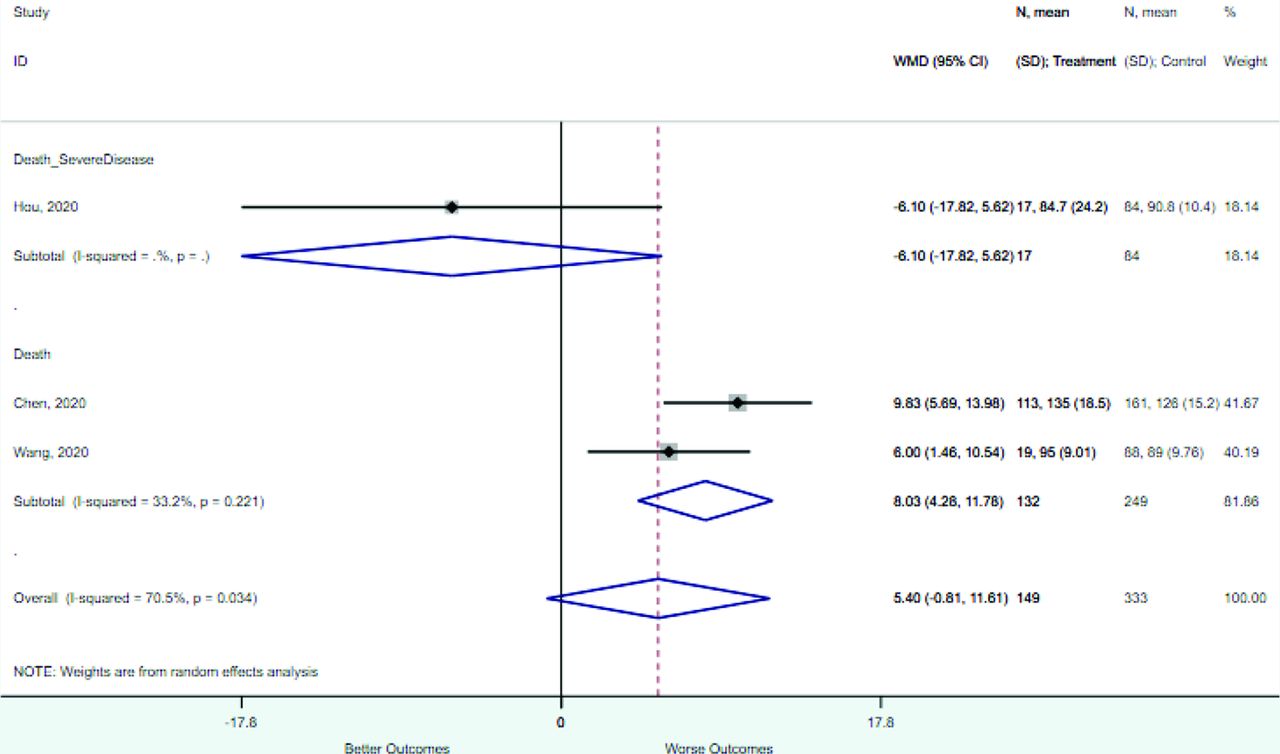
Risk Factor Studies Patients WMD (95% CI) Outcome = death Age 7 1418 18.5 (15.4–21.6) Systolic blood pressure 1 105 12.5 (0.64–24.3) Mean arterial pressure 2 381 8.0 (4.3–11.8) D-dimer (mg/L) 4 870 7.6 (6.1–9.4) Heart rate 3 486 5.3 (1.7–8.9) CRP (mg/L) 4 1016 40.4 (27.4–53.3) Neutrophil count 3 679 4.3 (2.7–5.8) WBC count 6 1314 4.0 (3.4–4.6) Respiratory rate 3 486 3.1 (1.5–4.7) Procalcitonin 3 763 0.34 (0.27–0.40) Oxygen saturation 4 823 −8.9 (−11.9 to −5.9) Lymphocyte count 6 1314 −0.4 (−0.5 to −0.3) Outcome = severe disease or death CRP (mg/L) 4 4531 60.5 (47.9–73.2) Age 5 4641 15.9 (10.4–21.3) Systolic blood pressure 1 110 8.6 (0.07–17.1) Neutrophil count 4 1912 2.6 (2.1–3.2) WBC count 3 322 2.0 (0.98–3.0) Respiratory rate 2 211 1.5 (0.02–3.3) Heart rate 2 211 0.99 (−3.7, 5.5) D-dimer (mg/L) 1 2729 0.31 (0.27–0.36) Procalcitonin 3 4420 0.13 (−0.30 to 0.56) Mean arterial pressure 1 101 −6.1 (−17.8 to 5.6) Oxygen saturation 3 2940 −4.4 (−7.3 to −1.4) Lymphocyte count 5 4641 −0.63 (−1.0 to −0.22) Outcome = severe disease CRP (mg/L) 4 731 34.2 (15.4–53.1) Age 8 2223 14.1 (10.9–17.6) Oxygen saturation 1 78 12.3 (2.6–22.1) Heart rate 1 78 7.3 (−21.4 to –36.0) Neutrophil count 5 752 0.94 (−0.42 to 2.3) WBC count 5 954 0.73 (−0.63 to 2.1) D-dimer (mg/L) 5 604 0.30 (0.06–0.55) Procalcitonin 2 276 0.05 (−0.08 to 0.19) Respiratory rate 1 78 0.00 (−15.6 to 15.6) Lymphocyte count 5 948 −0.44 (−0.52 to −0.36) WMD, weighted mean differences; COPD = chronic obstructive pulmonary disease; CI, confidence interval; CRP, c-reactive protein; LDH, lactate dehydrogenase; WBC, white blood count; SBP, systolic blood pressure.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Prospective Validation of a Simple Risk Score to Predict Hospitalization during the Omicron Phase of COVID-19
- Prognostic accuracy of triage tools for adults with suspected COVID-19 in a prehospital setting: an observational cohort study
- COVID-19 outcomes among adult patients treated with long-term opioid therapy for chronic non-cancer pain in the USA: a retrospective cohort study
- Gene Expression Risk Scores for COVID-19 Illness Severity
- Primary Care in the COVID-19 Pandemic: Essential, and Inspiring