
Article Figures & Data
Figures
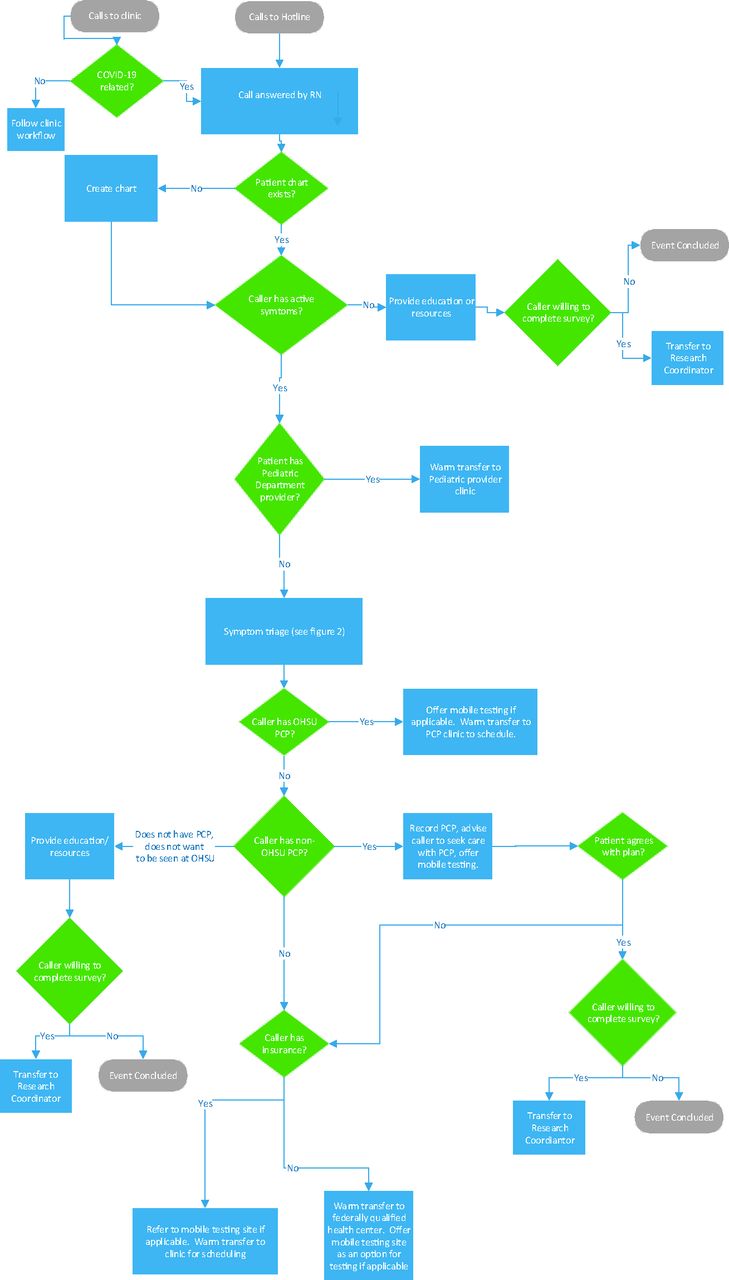
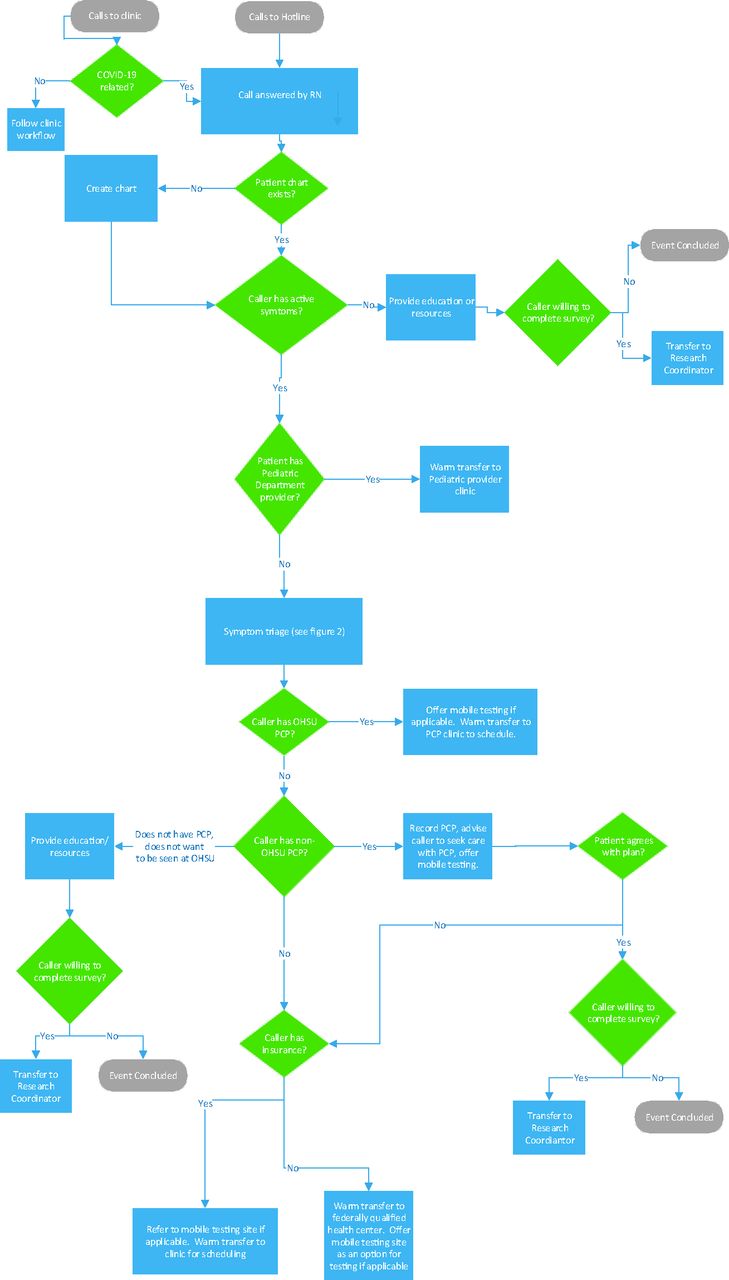
- Figure 1.
This workflow diagram illustrates how a nurse (RN) manages patient calls, which begin with a phone call to an Oregon Health & Science University (OHSU) clinic or to the hotline’s direct number. Patients with an OHSU Primary Care Provider (PCP) and with no PCP are managed within the system. Patients with a non-OHSU PCP are referred back to their provider after assessment.
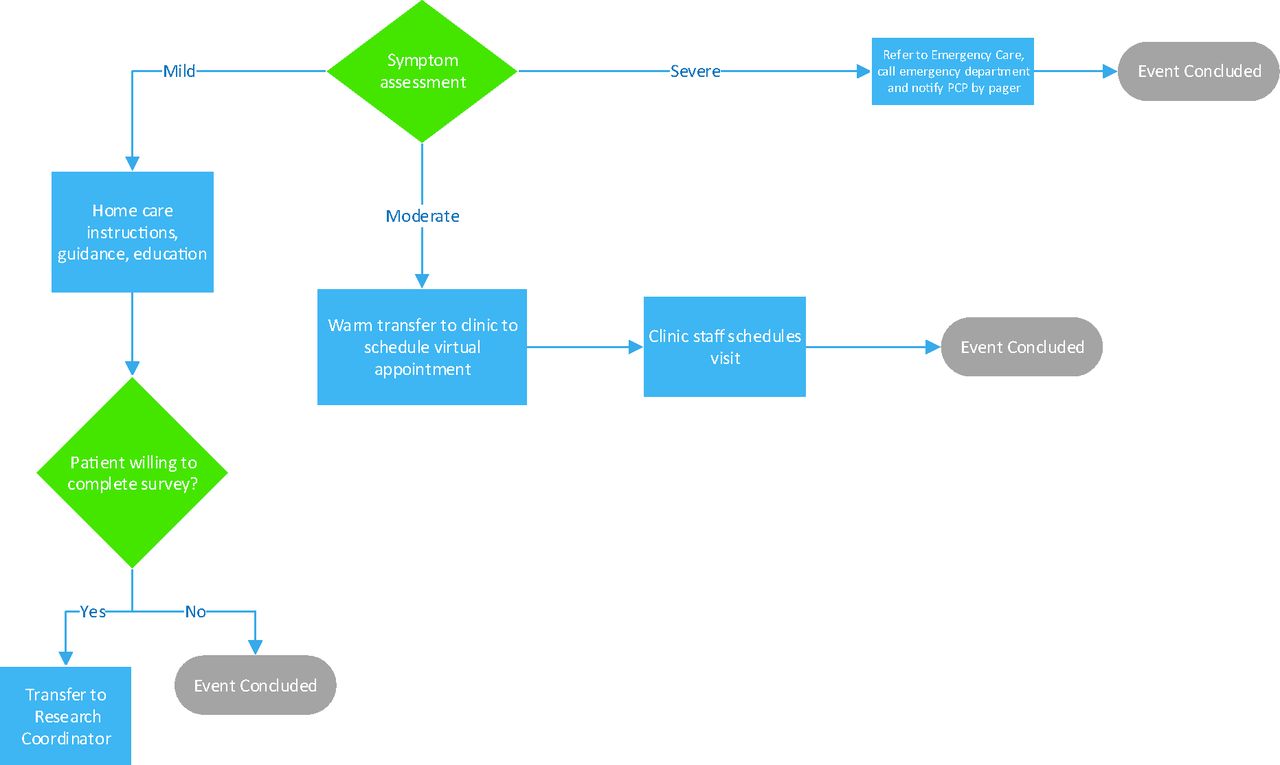
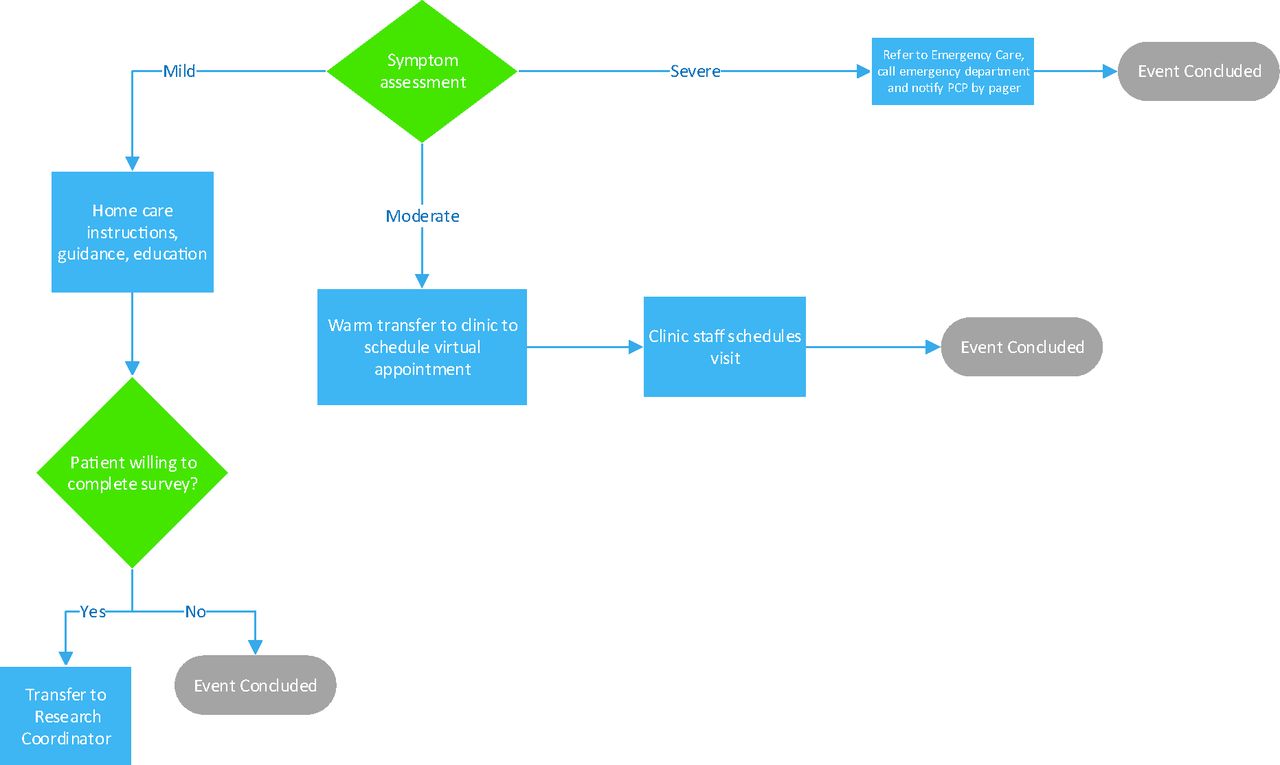
- Figure 2.
This diagram illustrates the management of calls after nurse triage of symptom severity as mild, moderate or severe. The primary care provider (PCP) is notified if a patient is referred to the emergency department.
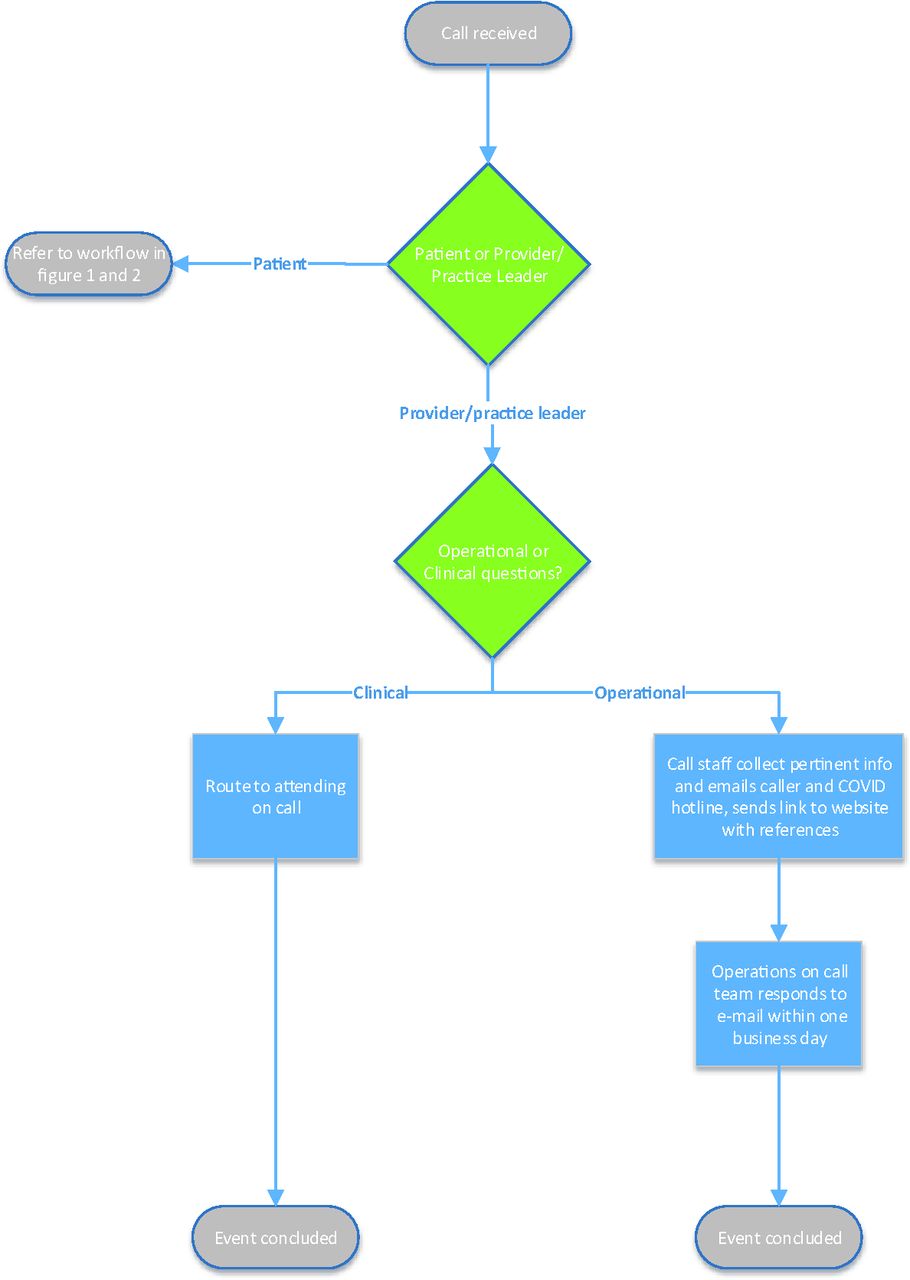
- Figure 3.
Provider or practice leaders also call the hotline. Clinical questions are answered by an on call physician. Operational questions are answered by practice leaders via email. Patient calls are managed as in Figure 1 and 2.

Tables
- Table 1.
COVID-19 Connected Care Center Hotline Work System: Description of the COVID-19 Connected Care Center Work System in Terms of SEIPS 2.0 Components, Including the Persons Involved, Their Tasks, the Tools and Technology They Used, and Processes Used for Adaptation
Persons Tasks Tools and Technology Adaptation Implementation team: a team of clinical, operations, and call center experts created and implemented the program. Workflow development sessions were led by internal performance improvement consultants. • Define and implement workflows.
• Produce resources needed to support standard work.
• Align work with institutional and statewide stakeholders.
Intensive workflow development sessions were conducted in person. The remainder of meetings were conducted remotely. • Institutional leaders were identified and convened into a daily steering committee to provide oversight of the implementation team and to rapidly identify and address barriers. This allowed us to navigate and influence the internal and external environment. For example, the steering committee helped us quickly develop health information technology tools within OHSU and identify areas for alignment with public health agencies.
• Daily huddles occurred for continuous process improvement.
COVID Inquiry Group: medical students were not able to participate in clinical rotations and were offered this COVID elective course. Residents on suspended clinical rotations also participated. Clinical and research faculty lead the group along with a project coordinator and administrative staff. Librarians and specialists provided consultative backing. • Continuous research to create and organize a library of materials that are accessible to all hotline teams as well as primary care and ambulatory specialty practices at OHSU and across the state.
• Update resource daily.
• Multiple tools were used to support the needs for large group, small group, and individual work with synchronous and asynchronous communication in both text-based and audiovisual formats.
• More information can be found about the inquiry group in a separate paper.10
Products were reviewed by the medical branch of the OHSU Emergency Operations Center through a delegated internal review process. Feedback was returned to the inquiry group. Triage nurses: the team is composed of nurses from across OHSU who were reassigned from other duties. • Assess severity of illness and arrange appropriate disposition for patients. Disposition options include mobile testing, home care, virtual visits, referral to primary care respiratory clinic, and referral to an emergency department.
• Answer phone calls and electronic messages directed to the hotline from OHSU clinics.
• Perform symptom assessments for patients with a positive COVID-19 test.
• A centralized phone number and e-mail address were created for the hotline. Phone trees were reprogrammed to provide access points to the hotline from ambulatory clinics. The phone tree was integrated into other existing phone trees across the university as appropriate.
• Nurses participated in an initial 2-hour virtual training.
• Nurses were given telephones, laptops, and headsets to allow them to work from home.
• Goals of care scripting are provided for rapid assessment of patients before referral to the emergency department.
• Dedicated electronic health record training teams and resources were made available in real time via conferencing software to support the nurses in the first 3 weeks after hotline implementation.
• Daily huddles occur for continuous process improvement.
• Conferencing software and secure instant messaging allow constant communication among the nurses to create a collaborative culture with rapid dissemination of knowledge and peer-to-peer learning.
• Quality assurance activities are ongoing, including review of live and recorded calls and operational data about the hotline (eg, hold times, abandonment rates), and patient experience surveys are collected. A more formal evaluation is also being developed (see Table 2 for more details).
Hotline attendings: OHSU physicians and advanced practice providers agreed to be on-call and performed this work in addition to their normal duties. • Provide consultation to triage nurses and support in navigating difficult clinical scenarios.
• Answer clinical questions from providers across the state.
• Provider onboarding was performed remotely.
• A dynamically updated frequently asked questions document was created through an internal peer-review process to provide evidence-based answers. This work was done by the OHSU School of Medicine COVID-19 Inquiry Group.
• This work was supported by the COVID-19 Connected Care Center Reference Guide which collates workflows and protocols from across the university. This resource is dynamically updated.
Development of expertise was encouraged by participation in institutional and statewide educational forums that occurred weekly. Ambulatory COVID-19 Operations Team: clinical managers and other medical operations experts representing medical delivery, front desk staff, and clinical support operations. • Create and update a guide with information about running an ambulatory clinic under the constraints of social distancing (eg, workflows to postpone visits, transition to virtual visits, provide education to patients and communities).
• Provide advice to statewide practice leaders navigating areas of uncertainty.
• Serve as a repository of best practices from outside institutions.
In addition to the hotline phone number, a dedicated e-mail address was created for primary care practices across the state to send questions to this group. Continuous review and updates to COVID-19 Connected Care Center Reference Guide. OHSU, Oregon Health & Science University.
- Table 2.
COVID-19 Connected Care Center Evaluation Research Questions, Measures, and Data Collection Approach
RE-AIM Element and Research Question (RQ) Measures/Data Collection Approach Reach—the absolute number, proportion, and representativeness of individuals who are willing to participate in a given initiativeRQ: To what extent does the hotline reach the intended target population? Numerators: number of target population for telephone hotline that called and spoke to someone; includes describing the following: trend in use over time, description of user (OHSU patient or not, sex, age), user patterns (time of the day), user location.Denominator: number of of OHSU patients and number of Oregonians without a primary care provider.Source: data from phone system, demographics for OHSU patients, statewide estimate of patients without a primary care provider. Effectiveness—the impact of an intervention on important outcomes, including potential negative effects.RQ: Does the telephone hotline impact key outcomes?Primary outcomes:Patient and provider experienceWere questions answered?Did patients feel reassured?Would patients/providers recommend this service?How much do patients value the service?Clinical outcomes and care use • Was testing offered when indicated.
• Follow-up rate.
• In-person visit/video visit—follow-up rate.
• Appropriate alignment of care level with severity—accuracy based on peer review.
• Infection prevention—adherence to quarantine, isolation, return to work recommendations.
• Emergency department—admission rates, total care cost.
Survey data: post-telephone surveys will be conducted with patients. Post-e-mail and post-telephone surveys will be conducted with providers.Qualitative interviews: these can be used to explore patient experiences more deeply and to try to understand variations in outcomes. Specifically, we will examine other information seeking and support seeking, access to services, alignment of the center with patients’ and providers’ needs, the community value of the call center, and access from both patients’ and providers’ perspectives.Source: electronic health records, Medicaid claims, statewide data. Adoption—willingness and experience of staff implementing the hotline. Source: semistructured interviews with staff to understand enjoyment of role, perceived readiness for role after training, responsibilities consistent with top of licensure, enjoyment of other nonclinical peers, perceived value of the hotline, confidence in the quality, and impact on well-being. Implementation—at the setting level, implementation refers to the intervention agents' fidelity to the various elements of an intervention's protocol. This includes consistency of delivery as intended and the time and cost of the intervention.RQ: How was the hotline implemented? What were the key elements of the “intervention” and what processes were put in place to ensure fidelity of the hotline? Source: qualitative data collection; interviews with key stakeholders: this will include understanding the staffing and functionality of the hotline, the staff full-time equivalent (FTE) and change in staff FTE over time, the type of staff involved, barrier/facilitators to implementation (eg, opportunities, technical issues, drop calls, hang up, hold times, and how these were resolved), partnership with the state and others that made this work possible. Maintenance—the extent to which a program or policy becomes institutionalized or part of the routine organizational practices and policies.RQ: Among key stakeholders, how would the hotline (if it is needed) be maintained, and what is needed to maintain it? Source: semistructured interviews with key stakeholders, after the active implementation phase of the pilot has ended, to assess factors related to maintenance. RE-AIM, Reach, Effectiveness, Adoption, Implementation, and Maintenance; OHSU, Oregon Health & Science University.




{kind=link}
{kind=link}
{kind=link}