
Abstract
To respond to the COVID-19 pandemic and recover from its aftermath, primary care teams will face waves of overwhelming demand for information and the need to significantly transform care delivery.
Innovation: Oregon Health & Science University’s primary care team envisioned and implemented the COVID-19 Connected Care Center, a statewide telephone “hotline” service.
Results: The hotline has taken more than 5825 calls from patients in 33 of Oregon’s 36 counties in less than 3 months. In preliminary survey data, 86% of patients said their questions were answered during the call, 90% would recommend this service, and 70% reported a reduction in stress levels about coronavirus. In qualitative interviews, patients reported their questions answered, short wait times, nurses spent time as needed, and appropriate follow-up was arranged.
Conclusion: Academic health centers may have the capacity to leverage their extensive resources to rapidly launch a multiphased pandemic response that meets peoples’ need for information and access to primary care, while minimizing risk of infection and emergency department use and rapidly supporting primary care teams to make the necessary operational changes to do the same in their communities. Such efforts require external funding in a fee-for-service payment model.
In March 2020, the large number of people who had symptoms and questions about COVID-19 and heightened psychological1 and physical distress2 suggested a need for increased access to primary care. At the same time, the United States had a shortage of primary care. Pandemic care requires sustained, rapid change.3,4 Initially, changes were needed to avoid in-person health care encounters for virtual care-sensitive conditions. Subsequently, primary care needed plans to continue telehealth and safe strategies to bring people back to the practice. Academic health systems may be in a position to augment less resource-rich primary care teams with regional telehealth services and facilitate information exchange for practice transformation.5
At the Oregon Health & Science University (OHSU), primary care nurses discontinued routine chronic disease management functions and answered thousands of COVID-related calls in the first weeks of the pandemic. Simultaneously, clinic leaders were rapidly adapting practice operations and population health activities. Practices across the state faced similar challenges; many had fewer resources to implement rapid change. Many community members lacked access to primary care. We wanted to help. The vision for the COVID-19 Connected Care Center, a statewide telephone “hotline,” was shared with philanthropic organizations and institutional leaders on March 20, 2020, funded on the March 23, and launched on March 30.
Innovation
Rapid policy changes provided financial support for the use of telemedicine platforms. The Centers for Medicare and Medicaid Services and many private payers increased payment rates for telehealth services and broadened the scope of covered services. This allowed us to link the hotline to an expanded range of digital health, primary care, and population health capabilities. The work systems and processes that we implemented are described using the SEIPS 2.0 Model, a human factors framework based on principles such as systems orientation, person-centeredness, and design-driven improvements (see Table 1).6,7 We maintained a strong evidence base, minimized handoffs in our workflows, offered virtual visits when appropriate, and arranged care to be provided by patients’ primary care clinicians whenever possible. We decided that clinic staff would schedule virtual visits to allow for local variations in workflows. Home care was supported by online patient education resources and secure patient messaging portals. Almost all work of the hotline was conducted by staff working from home.
COVID-19 Connected Care Center Hotline Work System: Description of the COVID-19 Connected Care Center Work System in Terms of SEIPS 2.0 Components, Including the Persons Involved, Their Tasks, the Tools and Technology They Used, and Processes Used for Adaptation
The hotline aligned efforts launched in response to the pandemic, including those to redeploy workforce and keep learners engaged. The willingness of staff and faculty to redeploy and community members’ volunteer efforts were critical. We also aligned our work with community and state partners, including the Oregon Health Authority (OHA), Oregon’s Poison Control Center, the Portland Fire Department, local public health departments, and 2-1-1, a nonprofit organization providing access to more than 7000 nonprofit, government, and faith-based health and social service programs.
Launch Timeline
OHSU’s COVID-19 Connected Care Center was launched in 3 phases.
Phase 1: OHSU Patient Hotline
On March 30, the hotline was opened to established OHSU patients, with hours 7 days a week from 8 am to 8 pm. Patients calling the hospital’s primary care and specialty clinics had the option to be routed to the hotline, where they would speak with a triage nurse who provided medical advice about clinical symptoms, scheduled virtual care, and referred to a mobile testing site, social worker, or the emergency department. Hotline nurses managed COVID-19 test results from OHSU sites, including its mobile testing sites, called patients with positive results, and provided education. Among patients positive for COVID-19, nurses called to reassess symptoms. A small percentage of patients referred to virtual visits were then referred to our respiratory clinic for in-person evaluation.8 Patients with questions pertaining to mental health care, social, and economic services were connected with an on-call social worker or social services.
Phase 2: Statewide Provider Hotline
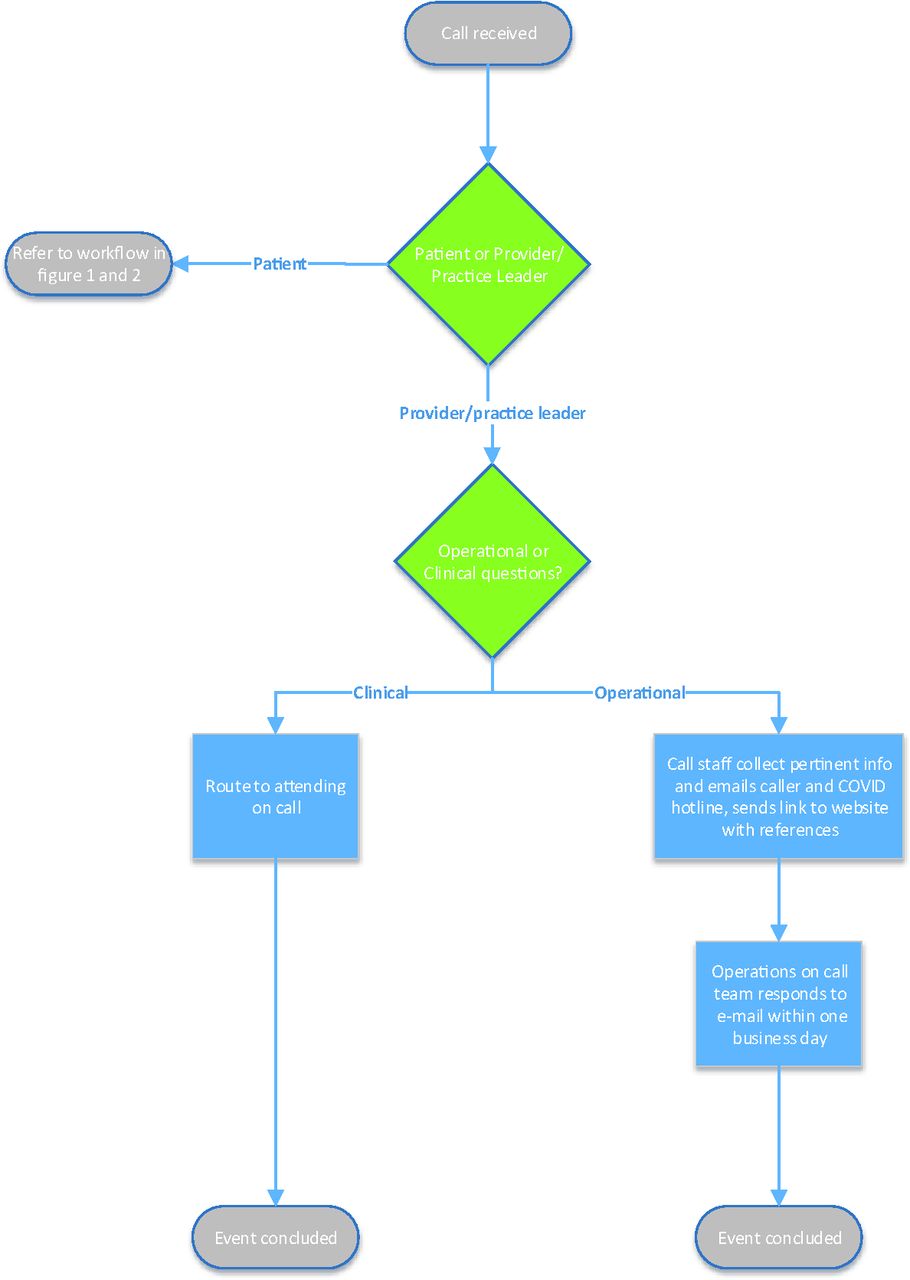
Beginning April 9, a central e-mail, website, and telephone consult line opened to primary care and specialty practices across Oregon. Clinicians were put in contact with an attending team, who answered symptom, testing, and operational questions.
Phase 3: Statewide Patient Hotline
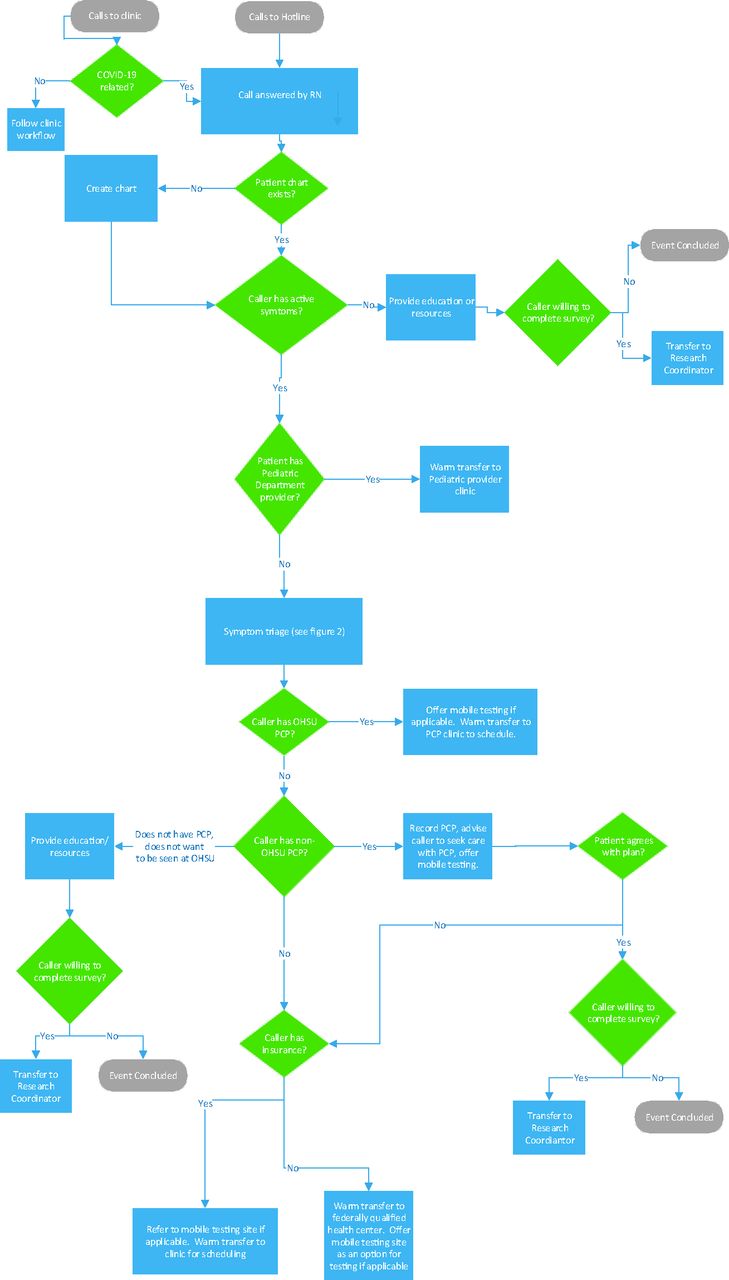
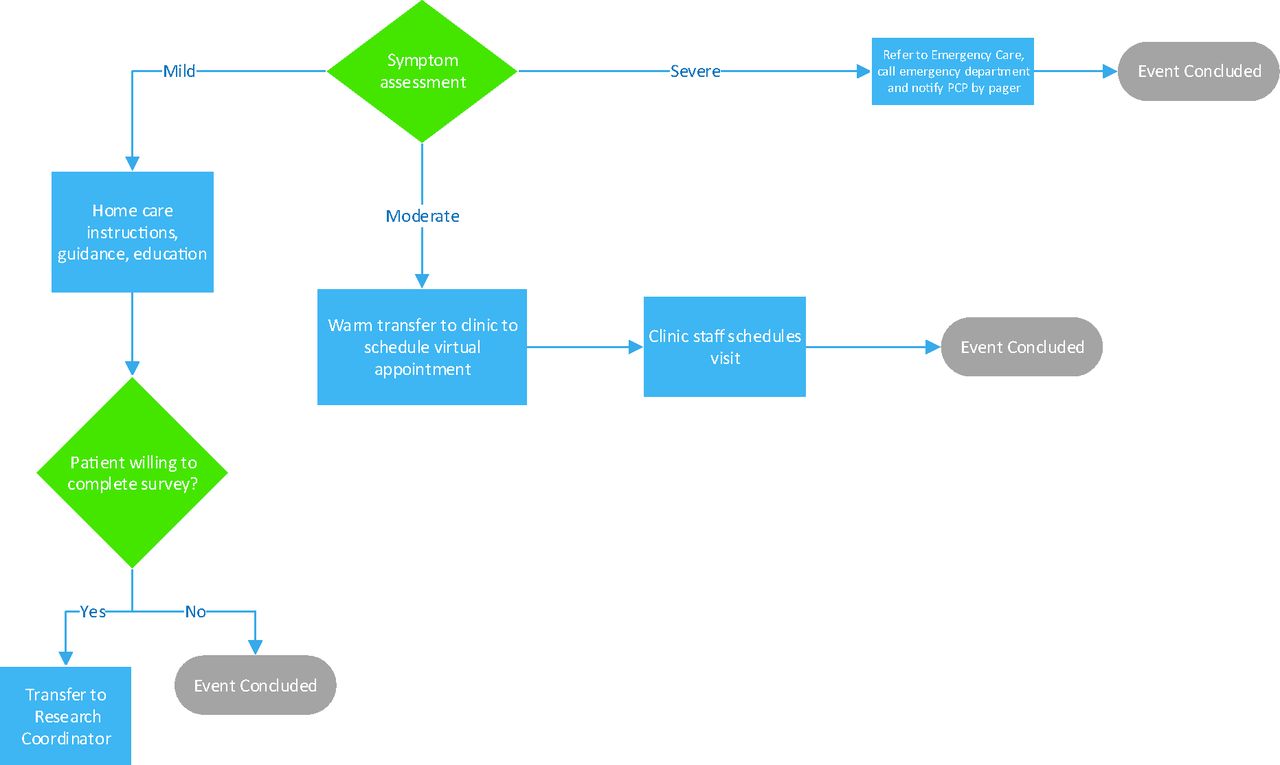
Beginning April 16, the patient hotline opened to Oregonians, with the target audience being people without access to primary care. Patients requiring a visit were referred to their primary care clinician, regional practices open to new patients, or OHSU clinics. COVID-19-related care was provided free of charge. Partnerships were leveraged to reach patients; the hotline was advertised on the OHA website as part of its health care partner resource and at c19.oregon.com, the Portland Metro Emergency Response for the Coronavirus Checker online tool. Figure 1 illustrates the flow of phone calls, Figure 2 management of symptoms, and Figure 3 the handling of calls from providers and practice leaders.
In all phases, call teams were supported by an attending, and nurses and attendings referred to a shared reference, the COVID-19 Connected Care Center Reference Guide, which was developed in real time by the School of Medicine COVID-19 Inquiry Group, an “intellectual engine” providing evidence-based recommendations using rapidly evolving data.9 This group consisted of volunteer clinical and research faculty, medical students, and residents. Medical students’ participation qualified as an elective. The group answered questions identified from hotline calls and clinicians participating in statewide Project ECHOs (Extension of Community Health Care Outcomes)10 on COVID-19. ECHOs had more than 1000 registrants, 25% of whom served rural or frontier communities. The inquiry group validated information through an internal peer-review process before dissemination.
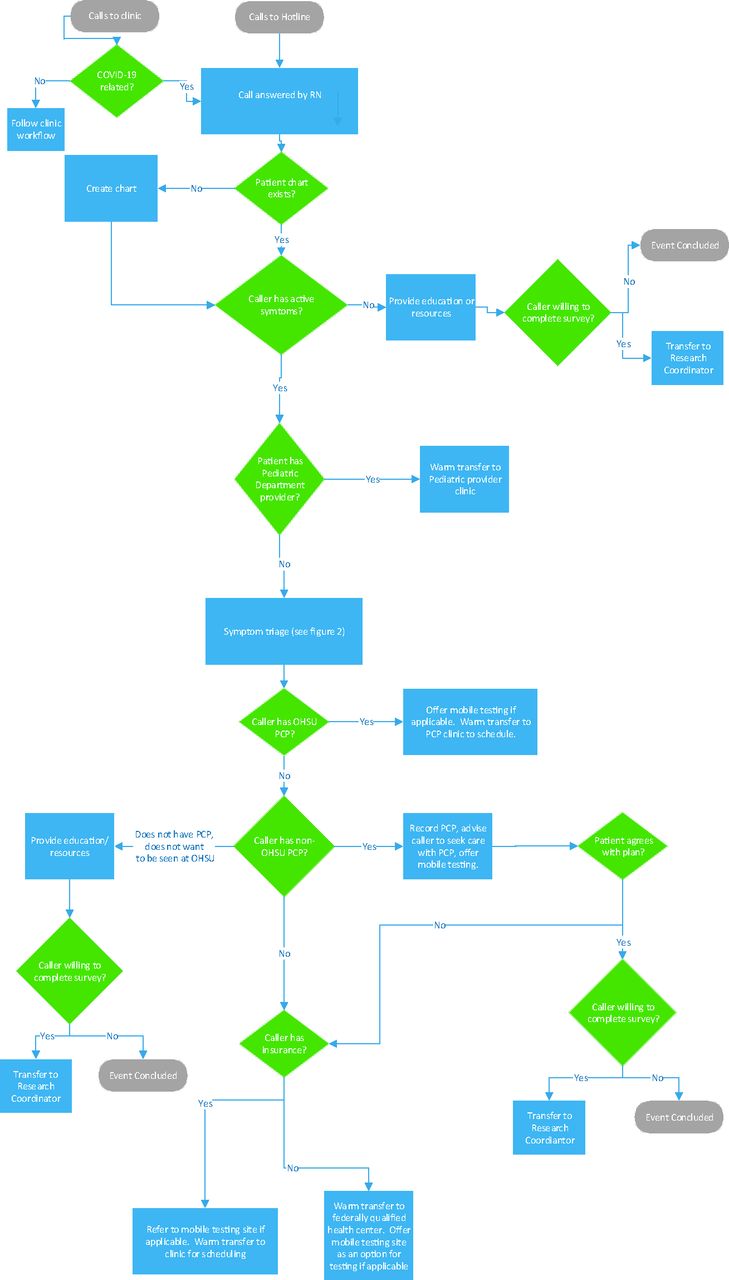
This workflow diagram illustrates how a nurse (RN) manages patient calls, which begin with a phone call to an Oregon Health & Science University (OHSU) clinic or to the hotline’s direct number. Patients with an OHSU Primary Care Provider (PCP) and with no PCP are managed within the system. Patients with a non-OHSU PCP are referred back to their provider after assessment.
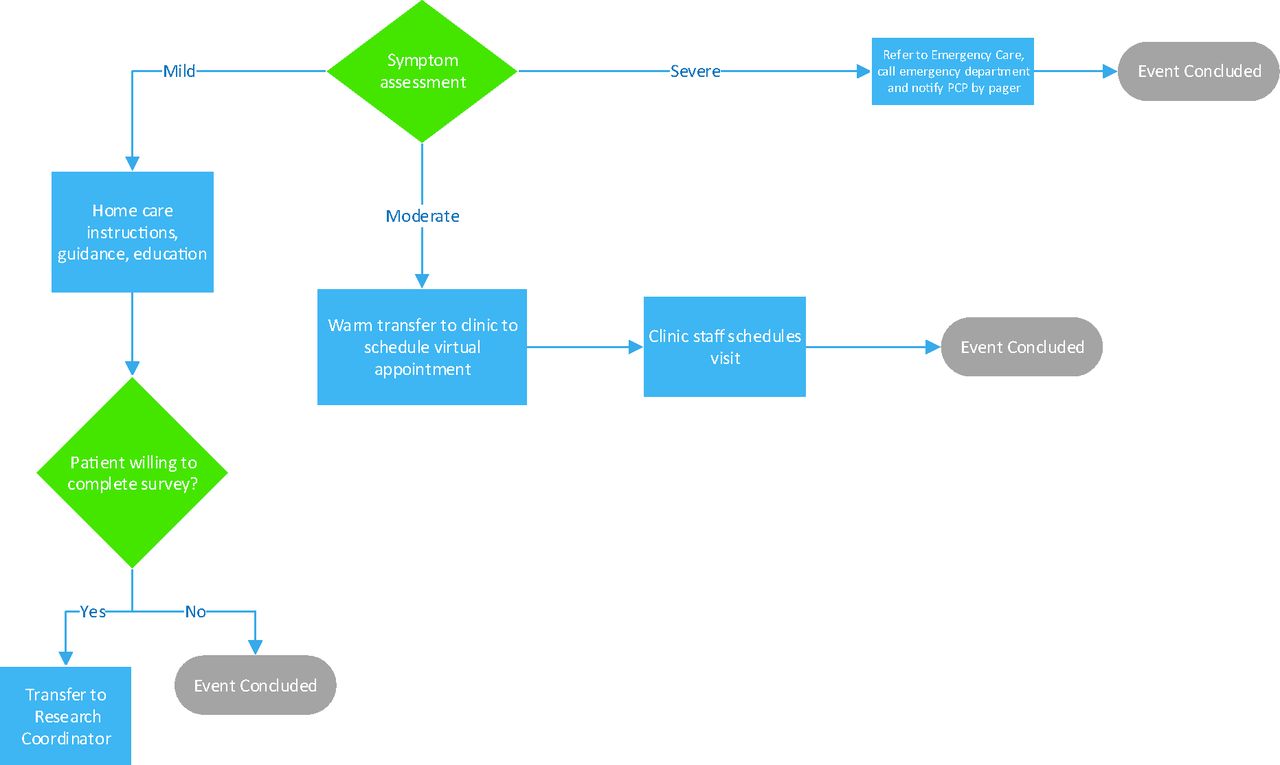
This diagram illustrates the management of calls after nurse triage of symptom severity as mild, moderate or severe. The primary care provider (PCP) is notified if a patient is referred to the emergency department.

Preliminary Results and Evaluation Plan
Between March 30 and June 1, 2020 the OHSU COVID-19 Connected Care Center took more than 5825 calls from patients and providers in 33 of Oregon’s 36 counties. There were an average of 141 triage calls and 68 results calls each weekday. The team also handled 9594 results and 916 patient e-mail messages. An average triage call was 6 minutes; an average results call was 30 minutes. Of the patient callers, approximately 36% received education; 49% had mild, 19% had moderate, and 1% had severe symptoms. In the first 2488 calls, only 7 resulted in an emergency care referral. Twenty-four full-time nurses staffed the hotline. In subsequent months, call volumes increased; total calls exceeded 60,000 by the end of the year.
To evaluate the Connected Care Center, we are using the RE-AIM Framework (Reach, Effectiveness, Adoption, Implementation, and Maintenance) to answer the following questions: (1) Did the Connected Care Center reach the intended target populations? (2) Was the Connected Care Center effective? (3) What can we learn about what worked and what did not to refine this effort? (4) What aspects of the Connected Care Center can and should be maintained, and how? To answer these questions, we are collecting quantitative and qualitative data as shown in Table 2. Data collection is ongoing.
COVID-19 Connected Care Center Evaluation Research Questions, Measures, and Data Collection Approach
Preliminary data show that patients called the hotline seeking personalized information to translate publicly available information to their own situation. As a result of their call, patients reported feeling their stress and anxiety about COVID-19 reduced, receiving information and access to care and testing and education that included help developing plans to social distance to protect coworkers and family members from transmission. When surveyed (n = 50), 86% of patients reported that their questions were answered during the call, and 90% said they would recommend this service to a friend or family member.
Discussion
Evaluation Plan
A nurse triage hotline to address patients concerns about the COVID-19 pandemic can relieve a substantial burden from primary care practices11 and contribute to efforts to prevent mildly sick but contagious people from seeking in-person care. The majority of patients that called our hotline required education only, and nurses talked to patients with mild symptoms, which were appropriately handled by a nurse telephonically.
In addition to patients, practice leaders from almost every Oregon county used the hotline to inform how they managed COVID-19. We shared resources, including almost 450 “frequently asked questions” and a reference guide, and have fielded 320 calls and 28 e-mails from primary care clinicians and practice leaders (through June 6, 2020). OHSU was a conduit for rapidly assimilating evidence and providing direct support to primary care practices across the state, helping them optimize patient care during this pandemic.12⇓⇓⇓⇓⇓⇓–19 Involving learners allows them to contribute to the pandemic response, safely. This centralized team of experts has also facilitated research and community based testing. Thus, the hotline served several of the functions envisioned for a primary care extension program, an unfunded mandate of the 2011 Patient Protection and Affordable Care Act. Where the federal government left a funding gap, the Andrew and Corey Morris-Singer Foundation stepped in and made a generous donation. Our experience demonstrates how a state-based primary care extension model, if funded, can support pandemic preparedness.
Our next step is to fully evaluate this effort, including identifying factors that led to implementation success (eg, alignment of institutional leadership, ability to adapt, visibility of the work across multiple levels of the institution) and determine which elements of this approach were most effective and why. Of particular interest is the impact of the hotline on primary care teams in community practice, particularly in rural and underserved areas, and to understand the impact on and the best strategies for reaching marginalized populations who suffer disproportionately from COVID-19. This includes taking steps to expand our partnerships to include community-based organizations and community leaders with diverse perspectives.20
Conclusion
With adequate resources and funding, it is possible to rapidly implement a multiphase coordinated approach to aid primary care teams on a statewide level to respond to a pandemic. The COVID-19 Connected Care Center addressed patients’, community members’, and providers’ COVID-related concerns. The hotline is an example of how an academic health center can support public health and statewide practice adaptation.
Acknowledgments
A generous donation from the Andrew and Corey Morris-Singer Foundation supported the establishment of an OHSU phone hotline and telemedicine service to enable many more Oregonians to access the COVID-19 primary care resources and information. We wish to thank the team of leaders, managers, and operations and logistics experts who worked 24/7 behind the scenes to make all of this happen. Those not already named include our executive sponsors John Hunter, MD, Bridget Barnes, MBA, MSEM, and Renee Edwards, MD. We also wish to thank steering committee cochair Kevin O’Boyle, MHA and lead for operations Debbie Lamberger, MPA. This work would not have been possible without the help of project managers Shilpa Kasukurthi, Ali Bruni, and Jessica Hoyt. We appreciate the guidance from steering committee members Johanna Warren, MD, Sarah Present, MD, MPH, Cat Livingston MD, MPH, Darren Malinowski, MD, Steve Kassakian, MD, Banning Hendriks, MBA, Betsy Boyd-Flynn, and Kelsey Huwaldt, MBA.
Notes
This article was externally peer reviewed.
Funding: This work was supported by the philanthropy of the Andrew and Corey Morris-Singer Foundation.
Conflicts of interest: None.
To see this article online, please go to: http://jabfm.org/content/34/Supplement/S170.full.
- Received for publication April 29, 2020.
- Revision received June 17, 2020.
- Accepted for publication June 18, 2020.




{kind=link}
{kind=link}
{kind=link}