
Abstract
Background: Family physicians provide a sizable portion of emergency care in the United States. However, there is limited work characterizing this population.
Methods: We completed a cross-sectional analysis of the 2020 American Medical Association Physician Masterfile that was inclusive of all clinically active physicians who designated emergency medicine as their primary or secondary specialty and had family medicine residency training and/or family medicine board certification. We used Accreditation Council for Graduate Medical Education information to determine family medicine residency training and data from the American Board of Medical Specialties to determine family medicine board certification status. We calculated physician density using US Census Bureau estimates; urban-rural assignments were based on Urban Influence Codes.
Results: We identified 4354 clinically active emergency physicians (9% of the overall emergency physician workforce). Of these, a majority were male (88%) and completed their training at least 20 years ago (84%), and a majority (59%) reported emergency medicine as their primary specialty. There is notable variation in physician density per 100,000 US population, and these densities declined compared with prior estimates from 2008.
Conclusions: We find that family physicians represent a sizable portion of the overall emergency physician workforce despite decreases in physician densities across the United States.
- Cross-Sectional Studies
- Delivery of Health Care
- Emergency Medicine
- Family Medicine
- Family Physicians
- Workforce
Introduction
The United States currently has a shortage of emergency physicians (EPs),1 particularly in rural areas.2,3 We recently completed an analysis of all clinically active EPs in the United States. We found more EPs compared with 2008 but a decrease in the density of EPs in rural areas.2,3 Further, we found that nearly a third of rural EPs reported prior family medicine (FM) residency training;3 FM-trained EPs—who we will refer to as FM EPs—play an important role in emergency care in the rural United States,4,5 but this population has not been well characterized. Our goal was to characterize the 2020 population of clinically active FM EPs and identify their geographic distribution.
Methods
We performed a cross-sectional, secondary analysis of the 2020 American Medical Association (AMA) Physician Masterfile as reported previously;2,3 the AMA Masterfile is a comprehensive database that includes every physician with a medical license.2,3,6 The FM EP population of interest was all clinically active physicians who designated emergency medicine (EM) as their primary or secondary specialty and had FM residency training and/or FM board certification. Residents and those not clinically active (eg, primarily researchers, teaching faculty, nonclinical administrators, or physicians who retired or semiretired) were excluded given our interest in clinically active EPs.2,3 We used Accreditation Council for Graduate Medical Education (ACGME) information to determine FM residency training and American Board of Medical Specialties (ABMS) data to determine FM board certification status.
As described previously, physician location was classified into US Census divisions.2,3 Corresponding population sizes were classified using US Office of Management and Budget groups.2,3 Urban Influence Codes were used to assign each EP's county location (urban, large rural, or small rural); FM EP population density was calculated using county-level 2019 Census Bureau population estimates.2,3
Data were analyzed using Stata 15.1 (StataCorp; College Station, TX). First, we grouped FM EPs by board certification status: FM board certification with or without EM board certification, EM board certification, board certification but not in FM or EM, and no board certification. In the primary analysis, those with both FM and EM board certification (n = 736) were classified under the FM board certification group. In a sensitivity analysis, we split the FM board certification group by those with isolated FM board certification versus those with dual FM and EM board certification. Second, we examined FM EPs' characteristics by sex. Physician population density was mapped using ArcMap 10.6.1 (ESRI; Redlands, CA). The MassGeneral Brigham (Boston) Institutional Review Board determined that this study met criteria for exemption. This study followed the Strengthening in the Reporting of Observational Studies in Epidemiology guidelines for observational studies.7
Results
We identified 4354 EPs with FM training and/or FM board certification (9% of the overall EP workforce). The majority (83%) were FM board certified, but a small subset lacked either FM or EM board certification (1%) or had no board certification (7%) (Table 1). Overall, a majority were male (88%) and located in urban areas (79%). Most (84%) completed their training at least 20 years ago, and a majority (59%) reported EM as their primary specialty. EPs in small rural areas were similarly aged (median age of 65 years [interquartile range (IQR) 60 to 69 years]) as EPs in large rural areas (65 [58 to 69]) and urban areas (65 [58 to 69]) but more often FM trained (small rural: 92%, large rural: 87%, urban: 82%, P <.001), had completed their training at least 20 years ago (small rural: 89%, large rural: 87%, urban: 84%, P = .003), and more frequently reported FM board certification (small rural: 87%, large rural: 86%, urban: 82%, P <.001). The majority of all groups reported EM as their primary specialty (small rural: 53%, large rural: 58%, urban: 60%, P = .04).
Comparison of Family Medicine Trained and/or Board Certified Emergency Physicians by Board Certification
FM EPs with isolated FM board certification (compared with those with dual FM and EM board certification) were younger (63 [58 to 67] vs 69 [66 to 72]), more often female (13% vs 9%), more often in rural (both large [14% vs 10%] and small rural [10% vs 3%]) areas, and less likely to report EM as their primary specialty (49% vs 82%) (Appendix Table 1). Stratified by sex, female EPs (compared with male EPs) were younger (62 [54 to 67] vs 65 [59 to 69]) but had similar geographic distribution (eg, by US Census division) and were similarly located in urban (77% vs 79%) and rural (large rural [14% vs 13%] and small rural [9% vs 9%]) areas. Additional comparisons of FM EPs stratified by sex are presented in Table 2.
Comparison of Family Medicine Emergency Physicians by Sex, n = 4354
We also identified notable variation in FM EP density by area per 100,000 US population (total [1.3], urban [1.2], large rural [2.1], and small rural [2.0]). Given prior 2008 data, this represents FM EP density decreases in all areas (total [−0.5], urban [−0.4], large rural [−0.5], and small rural [−0.4] areas).3 Physician density is presented in Figure 1 (EPs per 100,000 population by county) and Figure 2 (percent FM EPs among all EPs by county) for all clinically active FM EPs. Although the panels demonstrate FM EPs across the country, they seem most prevalent at the edges of our previously reported band of underserved states (from North Dakota to Texas)—the “EP desert.”3
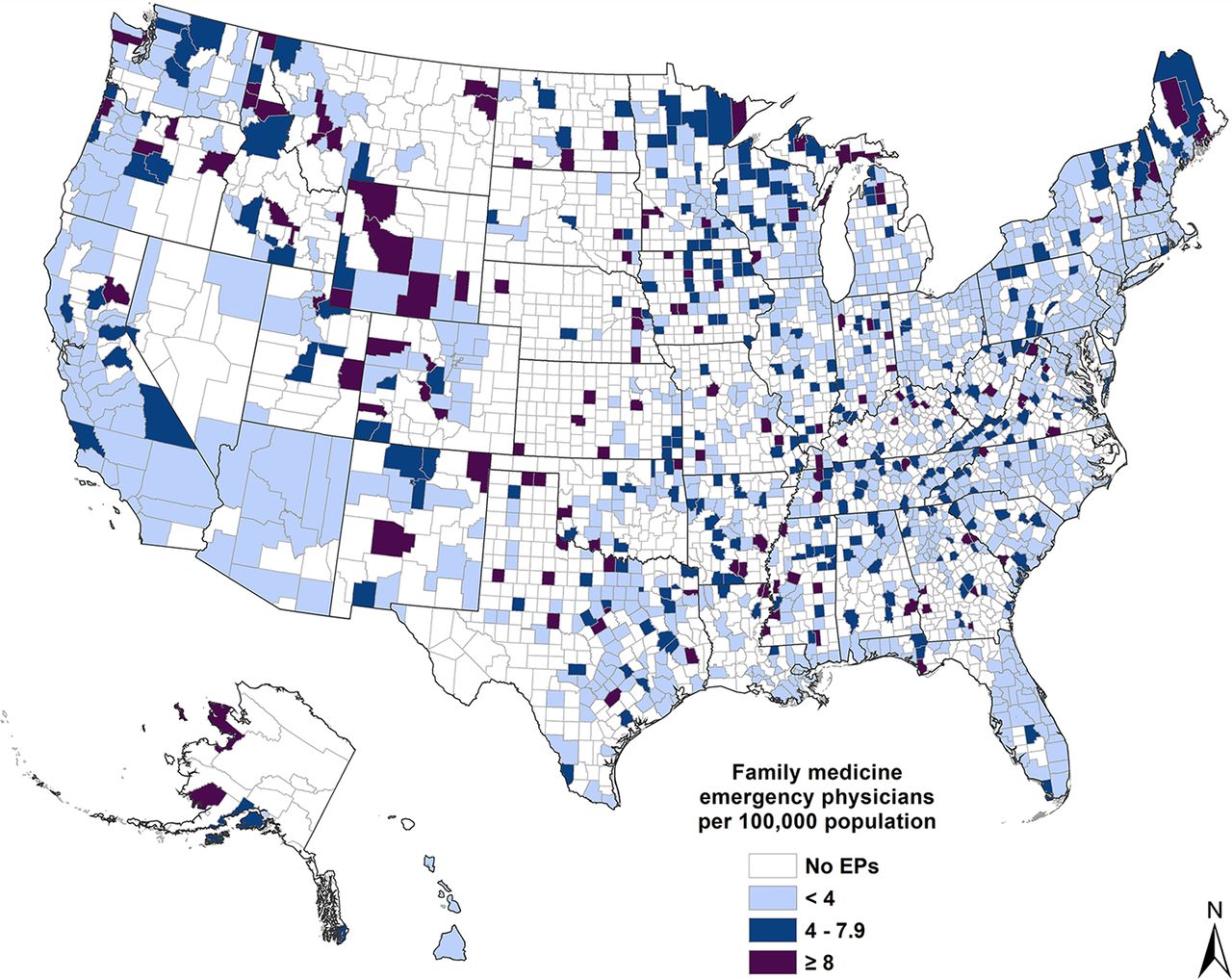
Family medicine emergency physician density per 100,000 population by county.

Family medicine emergency physician percent among all clinically active emergency physicians by county.
Discussion
We find that FM EPs represent a sizable portion of the clinically active EP workforce and most are male and in urban areas. Although less than a quarter were located in rural areas, the rural proportions presented here are higher than those of the overall EP population (we recently reported that only a minority of all EPs are in either large [6%] or small [3%] rural areas).3 We also found that FM EPs are older than the overall EP workforce and FM EPs in small and large rural areas are older than counterparts from the overall EP workforce.3 Further, compared with 2008,3 we find decreases in FM EP density across the United States (overall, urban, large rural, and small rural). Our findings characterize a rural, predominately male subpopulation of older FM EPs, who more often have isolated FM board certification, and who provide care in already underserved areas of the country where overall EP density is declining—“EP deserts.”3
However, our work has limitations.2,3 First, our study was limited to physicians who self-designated EM as their primary or secondary specialty. Family physicians who provide emergency care in the United States may not necessarily identify as EPs. As such, we likely slightly underestimate the number of actual FM EPs.4,5 Second, we are unable to account for the contributions of osteopathic EPs. Data are linked only to ACGME and ABMS; there is no equivalent osteopathic database.2,3 This is a previously noted limitation.2,3 Despite this, our work is still the most current and comprehensive study on clinically active FM EPs in the United States. Third, we are unable to account for the impact graduating EM residents will have on the FM EP workforce. We recently demonstrated increasing densities of EPs in urban areas;3 EM resident graduates have historically not taken jobs in rural areas.8 This absence of EM residency-trained EPs has likely contributed to the large share of FM EPs providing emergency care in more remote areas.
COVID-19 has significantly impacted the EP workforce.9 Fewer jobs,9 an increase in the number of EM residency programs,10 and a potential surplus of EPs by 203011 may collectively mean that new graduates joining the workforce will now relocate to areas and work in rural settings where FM EPs predominate.
Efforts that promote an increased physician presence in rural America are required. As FM EPs leave the workforce, “EP deserts” will persist and likely expand. However, addressing the need for rural EPs will require concerted effort.2,3 Incentivizing relocation efforts through loan repayment and expanding the number of rural EM rotations have been suggested.12,13 In the absence of any significant change, we anticipate that declining EP densities (both all EPs and FM EPs) in rural America will contribute to an accelerated used of nonphysician models of care with an increased presence of nurse practitioners, physician assistants, and/or telehealth.14,15
Appendix
Comparison of Family Medicine Emergency Physicians with Isolated Family Medicine or Dual Family Medicine and Emergency Medicine Board Certification, n = 3596
Notes
This article was externally peer reviewed.
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/34/6/1221.full.
See Related Commentary on Page 1265.
- Received for publication April 16, 2021.
- Revision received July 5, 2021.
- Accepted for publication July 8, 2021.




{kind=link}
{kind=link}