
Abstract
Background: The percentage of adults achieving hemoglobin A1c goals less than 7% remains a challenge. The study objective was to evaluate effects of a multidisciplinary approach on behavioral outcomes and mean change in A1c in immediate start (intervention) versus 6-month delay (control) groups at 6 months.
Methods: The study assessed 111 patients recruited from a safety-net primary care clinic with a pharmacist-led multidisciplinary team and found that the intervention improved mean A1c outcomes for patients with type 2 diabetes. A1c values were measured every 3 months, and a self-efficacy scale to measure behaviors was evaluated at baseline and 6 months.
Results: After 6 months from baseline, the intervention group showed an A1c decrease of 2.4 compared with the control group’s 1.1 decrease. Mean increase in self-efficacy score in the intervention group at baseline versus after 6 months showed a statistically significant change (P = .01) compared with the control group (P = .26). Results revealed a post hoc association between A1c and PHQ-9 such that patients with higher baseline PHQ-9 scores experienced greater mean decrease in A1c. In the immediate start arm, mean A1c values decreased from 10.6 at baseline to 7.7 at month 12. For the delayed intervention group, mean A1c values decreased from 10.2 at baseline to 9.0 after 6 months.
Conclusions: Use of a multidisciplinary clinic team in a safety-net primary care practice improved mean A1c control and behavioral outcomes for patients with type 2 diabetes as compared to control group.
- Behavioral Medicine
- Depression
- Family Medicine
- Patient Care Team
- Patient Health Questionnaire
- Primary Health Care
- Self-Efficacy
- Shared Decision Making
- Telemedicine
- Type 2 Diabetes Mellitus
Introduction
If recent trends in diabetes prevalence rates continue over the next 50 years, future demographic characteristics of the US population will lead to dramatic increases in the number of Americans with diagnosed diabetes. The projected number of adults with diagnosed diabetes would increase from 22.3 million in 2014 to 60.6 million in 2060.1
This increased number can further contribute to the disproportionate amount of health care costs linked to care of patients with multiple chronic diseases. One of 4 total health care dollars spent in the United States goes to the medical cost of diabetes.2 Cost is complicated by comorbid conditions such as depression, where people with type 2 diabetes have a 24% increased risk of developing depression. Those with diabetes and depression have 4.5 times higher the health care expenditures than individuals without depression.3⇓–5 Discordance exists between money spent and the percentage of patients who maintain glycemic control. The percentage of adults achieving A1c goals less than 7% only increased from 44.3% in 1999 to 2002 to 52.2% in 2007 to 2010,6,7 highlighting a need to implement more effective health care strategies to improve glycemic control. One probable strategy involving implementation of self-efficacy-focused education may lead to reduced A1c, enhanced self-efficacy, and regulation of self-management behaviors.8
The use of multidisciplinary teams is widely recommended to improve diabetes management. To date, there are limited studies evaluating the feasibility and efficacy of this team care approach,9 especially in safety-net clinics that serve a greater number of patients who are uninsured.10 According to the 2020 Standards of Medical Care in Diabetes, the use of multidisciplinary teams including primary care physicians, nurses, dietitians, pharmacists, and mental health professionals ranks only as an expert consensus because of limited clinical data.11 Preliminary studies have shown that treatment of diabetes in multidisciplinary teams with pharmacists or behavioral health professionals is associated with decreased A1c concentrations12⇓⇓–15 and more rapid attainment of associated goals. Despite these data, gaps in evidence remain, especially with respect to long-term outcomes and intervention sustainability.
This article describes a multidisciplinary clinic approach to improving glycemic control and behavioral outcomes in a family medicine safety-net academic practice. The study objective was to evaluate the effects of a multidisciplinary approach on behavioral outcomes and mean change in A1c in patients with type 2 diabetes.
Methods
Study Design and Setting
This single-site, single-blind, prospective study used a randomized delayed-start design with 2 parallel arms. Randomization was done in a simple sequence where patients were randomly assigned to immediate start versus the 6-month delay group based on the random order in which they were referred to the clinic. This study took place at an urban family medicine practice housing a family medicine residency program, affiliated with a level 1 trauma center and teaching hospital that is part of Atrium Health, a large vertically integrated health care system with care locations in North Carolina, South Carolina, and Georgia. The patient population attending the practice had the following demographics: 70% African American, 20% Caucasian, and 10% Hispanic/other. Approximately 1200 patients with diabetes visit this site, with 45% Medicare, 35% commercial insurance, 14% Medicaid, and 6% self-pay or sliding scale. The Atrium Health Institutional Review Board approved this study.
Intervention
This clinic was held at most 3.5 days per month and virtual (interim care) took approximately 8 hours per week. Members of the multidisciplinary team included a clinical pharmacist, rotating physician champions, clinical care nurse coordinator, social worker, behavioral health counselors, nurses, family medicine and pharmacy residents, and a research assistant.16 The clinical pharmacist, who is a certified diabetes care and education specialist and board certified in advance diabetes management, served as team lead. Standard 5 of the National Standards of Diabetes Self-Management Education and Support was used to appoint members of the multidisciplinary team.17
Participants
Providers referred practice patients who were nonpregnant, ≥ 18 years old with type 2 diabetes, with at least 1 of the following criteria: A1c greater > 8, A1c < 8 but with wide blood glucose variability, newly diagnosed, and/or new to diabetes injection therapy. Patients being followed by an outside endocrinologist or on insulin pump therapy were excluded. After a provider referral, a research assistant contacted the patient to assess readiness and obtain consent. Using a 10-point self-reported motivation score, patients were asked, “How motivated are you in getting better control of your diabetes?” Patients scoring 5 or higher were included in the study and received a $10 gift card for participation.
Outcomes
The primary outcome was the mean change in A1c in the intervention versus the control group during the 6 months of follow-up. Because all follow-up visits did not occur exactly at 6 months, a window of 5 to 10 months was used to capture outcomes. Per protocol, after 6 months the delayed-start group was exposed to the intervention. A1c values were assessed at baseline and every 3 months during the study period. Baseline A1c values were obtained from the medical record using the value closest to the time of randomization if that time frame was less than 3 months. If greater than 3 months had elapsed, the A1c was measured at the first diabetes clinic appointment. The secondary outcome was change in self-efficacy scores from baseline to month 6 of follow-up. Self-efficacy was measured using the Stanford Self-Efficacy for Diabetes Scale.18
Procedures
The study was powered to detect a mean difference of 1 percentage point in A1c between the intervention and control groups.19 To achieve 80% power, a sample of 104 (52 per arm) was required based on a 2-sample t-test with a standard deviation of 1.8.20 A sample size of 28 was required to achieve 80% power to detect a 2-point difference in the secondary outcome of self-efficacy (range 1 to 10) with a standard deviation of 1.76.18 The target sample size was set at 140 to accommodate an anticipated attrition rate of 20%.
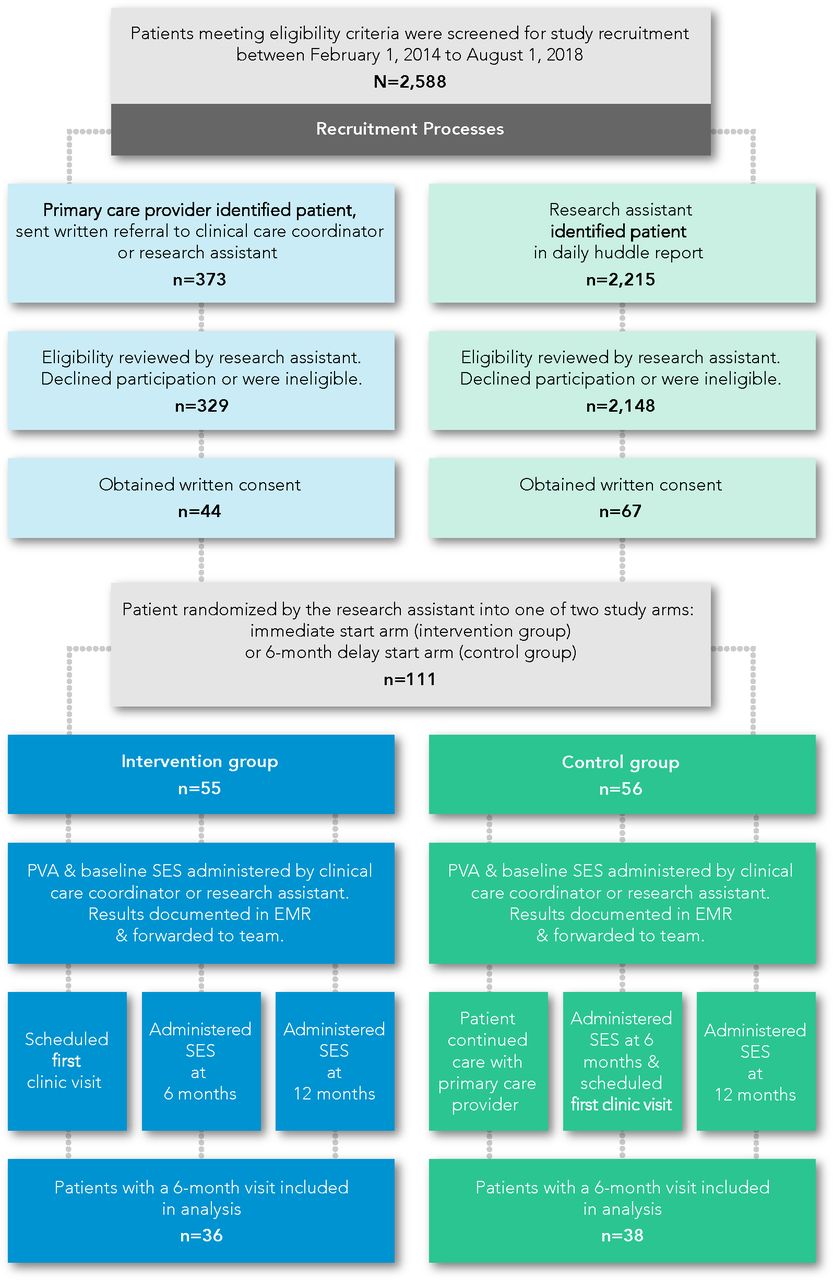
Patients were randomized 1:1 to the immediate start or the 6-month delay arm using a randomization schedule. Immediate start patients (intervention group) were scheduled in the first available appointment in the multidisciplinary diabetes clinic. Patients assigned to the 6-month delay arm (control group) continued to receive standard of care from their primary care provider for a period of at least 6 months before being scheduled for the first available multidisciplinary diabetes clinic appointment (see Figure 1).
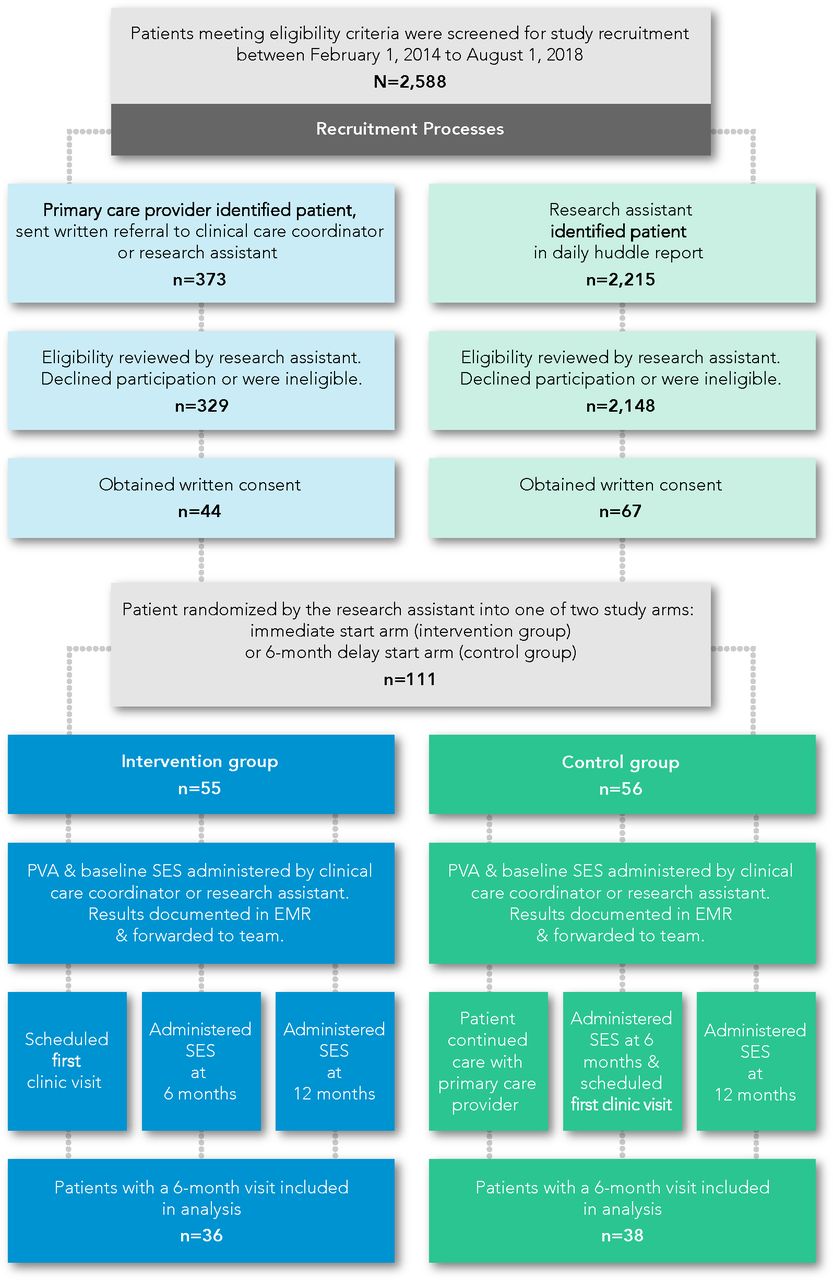
Study design flow chart. EMR, electronic medical record; PVA, previsit assessment; SES, self-efficacy scale.
Previsit Evaluations
Two previsit evaluations, termed previsit assessments (PVAs), were designed to identify barriers to disease management such as nonadherence, treatment complications, and a patient's perception of quality of life.21 The first PVA identified barriers in medication adherence, access to care, social support, depression symptoms, food acquisition, nutritional education, and self-care behaviors (see Table 1). The second PVA assessed patient self-efficacy using a validated, modified, self-efficacy scale (SES), where questions measuring self-confidence in self-management behaviors were modified to be more diabetes-specific.22 Answers to both PVAs allowed visits to be tailored to patient-specific needs to strengthen confidence, problem-solving skills, and self-management. The SES was administered at the first visit and again at 6 and 12 months (see Table 2).
Previsit Assessment
Self-Efficacy Survey
Initial Visit
Two business days before the scheduled appointment, a reminder call was placed to patients asking them to bring a completed nutrition, glucose, and exercise log to the visit.23 To promote patient engagement and empowerment, eligible patients with A1c < 9% were introduced to shared decision making (SDM)24 and motivational interviewing,16 to emphasize the importance of patient preferences for treatment. SDM is a process in which the patient and provider are equally involved in determining a treatment plan based on the individual patient's preferences of prioritizing medication cost, symptom control, side effects, and frequency of medication usage. During the clinic visit, specific patient treatment goals were shared and discussed so both patients and providers were involved in each treatment step of diabetes management.25 Patients not meeting the A1c ≤ 9% eligibility criteria for SDM were reassessed throughout the study period for inclusion and continued to receive all other aspects of the study interventions.
The diabetes clinic visits incorporated depression screening and diabetes education with an emphasis on healthful eating and exercise. To assess the presence and severity of depression, the 9-item Patient Health Questionnaire (PHQ-9) was administered by a behavioral health counselor at the initial visit and periodically thereafter based on the baseline score.26 To promote self-care, a packet of educational materials highlighting specific components of the National Standards for Diabetes Self-Management Education and Support were explained.17 All patients received nutrition education tailored to individual cultural customs, current A1c, blood glucose trends and variability, body mass index, activity level, financial status, and food stability. Different variations of education included, but were not limited to, the plate method, Mediterranean diet, and an intensive lifestyle intervention based on the LOOK AHEAD study.27 Detailed information on healthful eating from the American Diabetes Association's position statement on nutrition was referenced when applicable.28 Nutritional education, with an emphasis on accountability and sustainable healthy eating habits for maintaining glycemic control, was provided at multiple visits.
The following disease markers were measured when clinically appropriate: blood glucose, A1c, nonfasting lipid panel, basic or complete metabolic panel, urine microalbumin, and thyroid panel.11 Additional items addressed included foot examination, influenza vaccine, pneumococcal vaccines, hepatitis B vaccine, and screening for retinopathy and neuropathy.
Follow-Up Visits
Follow-up visits included repeat measurement of PHQ-9 every 4 to 8 weeks, clinically appropriate labs, vital signs, and office blood glucose as well as assessment of the patient's blood glucose recordings, exercise, and food logs. Medication therapy regimens were assessed at each follow-up visit for effectiveness, safety, tolerability, degree of weight neutrality, and affordability. Refill histories were obtained from community pharmacies to verify patients' self-report of adherence to the medication regimen. Behavioral therapy with a behavioral health counselor was offered. Patients started on or currently taking antidepressant medication were scheduled for frequent follow-up by the behavioral health counselor and the patient's primary care provider.
Interim Virtual Care
Interim virtual care for select patients, designed to improve access to care and provide frequent assessments and therapy intensification in between scheduled diabetes clinic visits, was coordinated by the clinical care nurse coordinator and executed by the clinical pharmacist. Inclusion criteria included patients with transportation challenges and at least 1 of the following characteristics: symptoms of hypoglycemia or hypoglycemia unawareness, wide blood glucose variability, and/or newly diagnosed or largely uncontrolled diabetes needing weekly insulin intensification. Each patient was called to obtain blood glucose values, and phone management for each patient continued until blood glucose and/or A1c values were within 1% of goal.
Statistical Analyses
Baseline demographic characteristics of patients in the 2 study arms were analyzed using Student's t-test, the χ2 test, or Fisher's exact test, as appropriate. Within groups, change from baseline to 6 months was analyzed using the paired t-test for weight, A1c, systolic blood pressure, and self-efficacy scores. McNemar's test was used for the binary results of the PHQ-9 score, while the Wilcoxon signed-rank test was used for self-rated health.
Analysis of covariance (ANCOVA) was used to assess between-group comparisons of baseline to 6-month change for weight, A1c, systolic blood pressure, self-efficacy, and self-rated health. The 6-month measure was the dependent variable. Group assignment (intervention and control) was the primary independent variable, and the baseline measure was the covariate. For PHQ-9 (binary), the Breslow-Day test was used. The self-efficacy composite score was calculated as the average of items 1 to 8 (see Table 2). All analyses were performed using SAS Enterprise Guide 7.1 (SAS Institute Inc., Cary, NC). A P value less than 0.05 was considered statistically significant.
Results
One hundred and eleven patients were enrolled between February 2014 and August 2018. The average patient age was 55 years; greater than 60% of the patients ranged in age from 45 to 64 years old. Sixty-six percent of the patients were female; greater than 80% were African American (see Table 3). A1c values were similar in the intervention and 6-month delay (control) groups at baseline: 10.6% and 10.2%, respectively (see Table 4). After 6 months from baseline, the intervention group showed a decrease in A1c of 2.4 compared with a decrease of 1.1 points in the control group, which was statistically significant (P = .02). Mean self-efficacy scores increased 0.8 points to 8.0 in the intervention group (P = .01), while there was a nonsignificant increase of 0.3 points in the control group (P = .26) at 6 months. The effect of the intervention on self-efficacy scores did not reach statistical significance when compared with the observed change in the control group (P = .05). A post hoc analysis showed mean decrease in A1c was greater in the intervention group among patients who had baseline PHQ-9 scores > 10. Fifty-three out of 74 patients met the criteria for the SDM intervention. The average number of weeks over 6 months that patients received the SDM intervention was 14, with a standard deviation of +/-7.4 weeks. Data analyses were completed to determine the impact of the clinical interventions on patients randomized to the 6-month delayed-start arm. After 6 months of receiving the multidisciplinary approach, mean A1c values decreased from 10.2 at baseline to 9.0 (P ≤ 0.1) at month 12. In the immediate start arm, mean A1c values decreased from 10.6 at baseline to 7.7 (P ≤ 0.01) at month 12 (see Table 5).
Patient Demographics
Comparison of Clinical and Behavioral Outcomes at Baseline and 6-Month Visit Among Patients Enrolled in Diabetes Clinic Study
Comparison of A1c at Baseline and 12-Month Visit Among Patients Enrolled in Diabetes Clinic Study
Discussion
The use of a multidisciplinary team approach in diabetes care was associated with a statistically significant improvement in mean A1c control and behavioral outcomes. This finding of a greater decrease in A1c is consistent with studies evaluating the role of interdisciplinary members in improving diabetes care.29,30 The design of our clinic used multiple disciplines along with techniques of SDM and motivational interviewing to address the many facets of diabetes management.16 The study showed a clinically significant difference in the change of A1c values after 6 months between the 2 groups. Self-efficacy scores in the intervention group at baseline versus 6 months were both clinically and statistically significant compared with those in the control group. An association was found between A1c and PHQ-9. The more depressed a person was at baseline in the intervention group, the more improvement he or she experienced in A1c at 6 months.
In addition to using the multidisciplinary team approach, successful implementation and sustainability of the diabetes clinic is due in part to the resources used to identify patient needs. By using a diabetes-specific PVA and SES to identify psychosocial and medication management needs, our multidisciplinary diabetes clinic team was able to minimize barriers and incorporate patients' needs as treatment goals. The SES provided a measurable method of understanding patients' self-management behaviors. Although we did not achieve our sample size goal based on a power calculation for the A1c outcome, and the intervention group did not achieve a 2-point difference from baseline to month 6, the final sample size of 74 provided enough power to detect a difference as small as 1.2. Notably, the power analysis was based on a 2-sample t-test, and the final analysis was an ANCOVA. The SES increase of 0.8 led to a statistically significant increase in the intervention group. The between-group difference in SES for the intervention and control groups was not statistically significant. However, the clinical significance of improving confidence and behaviors in self-care was achieved.
In line with previous studies, these data highlight the usefulness of a long-term multidisciplinary diabetes clinic on A1c reduction and improved behavioral outcomes. Our pharmacist-led program showed A1c improvement, similar to a study showing patients not only lowering A1c but reaching their A1c goal faster.31 In addition, our study integrated behavioral health into treatment of poorly controlled type 2 diabetes, in line with a similar study that also found lower A1c values with behavioral health integration, as well as systolic blood pressure, compared with controls.32 In addition, a systematic review of multidisciplinary management found there was overall statistically improved A1c values as well as improvement in health-related quality of life, patient self-care abilities, and patient knowledge of diabetes.33 Practices that have a different mix of health care professionals may benefit from reviewing standard 5 of the National Standards for Diabetes Self-Management Education and Support.17 This standard discusses how to assemble a successful team using available clinical resources. Collaborative practice agreements may also be a great cost-neutral strategy for improving skills within a team. Literature highlights the clinical usefulness of collaborative practice agreements between clinical pharmacists and physician practices.32,34 Primary care practices not yet collaborating with professional health care programs can easily begin a symbiotic partnership. Universities with health care professional programs are frequently looking for patient care sites where faculty can practice in their respective specialty area while providing continuous learning experiences for learners. In exchange for providing a practice site for health professional students to complete their supervised training, licensed faculty work under a collaborative agreement to implement beneficial clinical services while serving as the core preceptor for their learners.
Limitations
This strategy of using a multidisciplinary diabetes clinic to manage chronically uncontrolled patients is not without limitations. One limitation was the strong teaching component embedded within the multidisciplinary diabetes study that allowed potential cross contamination where provider exposure to both the control and intervention groups may have led to improved management in the delayed arm patients. Resident physicians who rotated through the diabetes clinic may have also served as the primary care providers for patients randomized to the delayed-start arm. Loss to follow-up was also higher than expected; our complete case analysis included only 74 of the 111 patients who were randomized. Common reasons for loss to follow-up included change in insurance or primary care provider, transportation challenges, and scheduling conflicts. Comparisons between patients with 6-month follow-up data and those without showed that these patients did not differ significantly on measured variables. The intervention and control groups in our final analysis sample also did not differ significantly on measured variables. However, loss to follow-up may have led to differences in unmeasured characteristics between the study groups, or between participants with 6-month follow-up data and those without such data, so selection bias remains a possibility.
Conclusions
Organizing a multidisciplinary approach to diabetes care can provide a much-needed resource for managing diabetes. This study provides a strategy for implementing a multidisciplinary approach to diabetes management in any primary care practice using a pharmacist, social worker, physicians, behavioral health counselors, clinical care coordinator, and nurse. Despite these data, gaps in evidence remain, especially with respect to long-term outcomes and intervention sustainability.
Acknowledgments
We would like to thank all of the members of the multidisciplinary diabetes clinic team for their support and contributions to the clinic design; Lakesha Beasley, Laura Staton, Steven Greenberg, Kenniesha Spencer, Dellyse Bright, Jewell Carr, Allison Bickett, and Rebecca Hayes.
Notes
This article was externally peer reviewed.
Funding: This study was funded by Atrium Health.
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/34/3/579.full.
- Received for publication June 23, 2020.
- Revision received December 19, 2020.
- Accepted for publication December 21, 2020.




{kind=link}