
Article Figures & Data
Figures
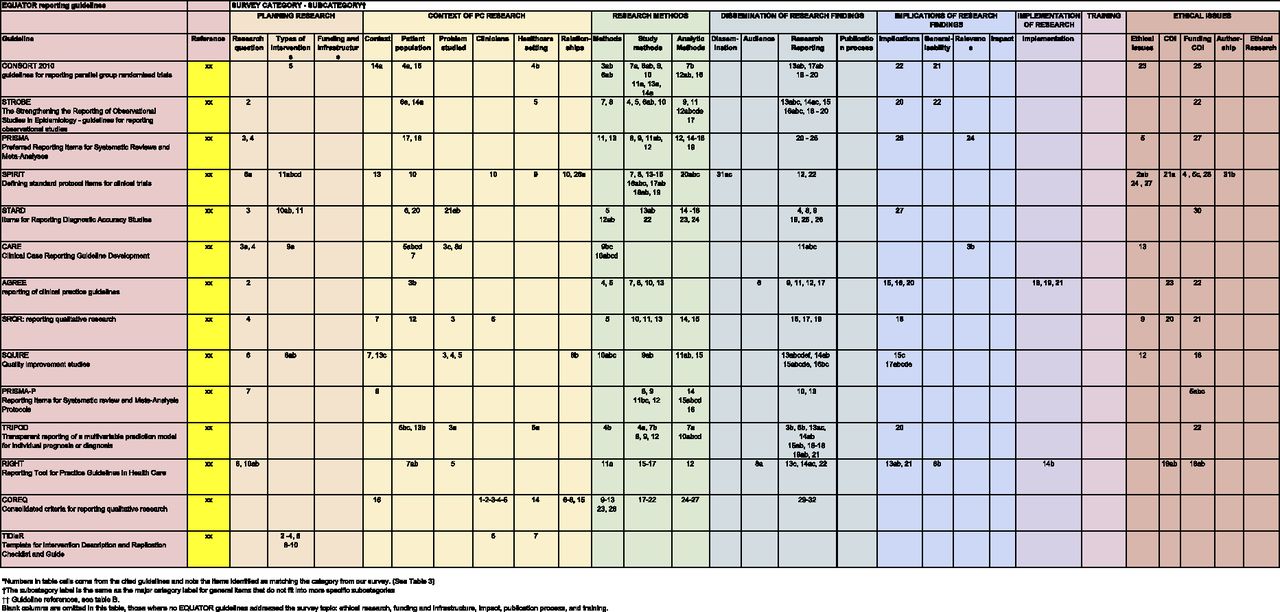
- Appendix 2.
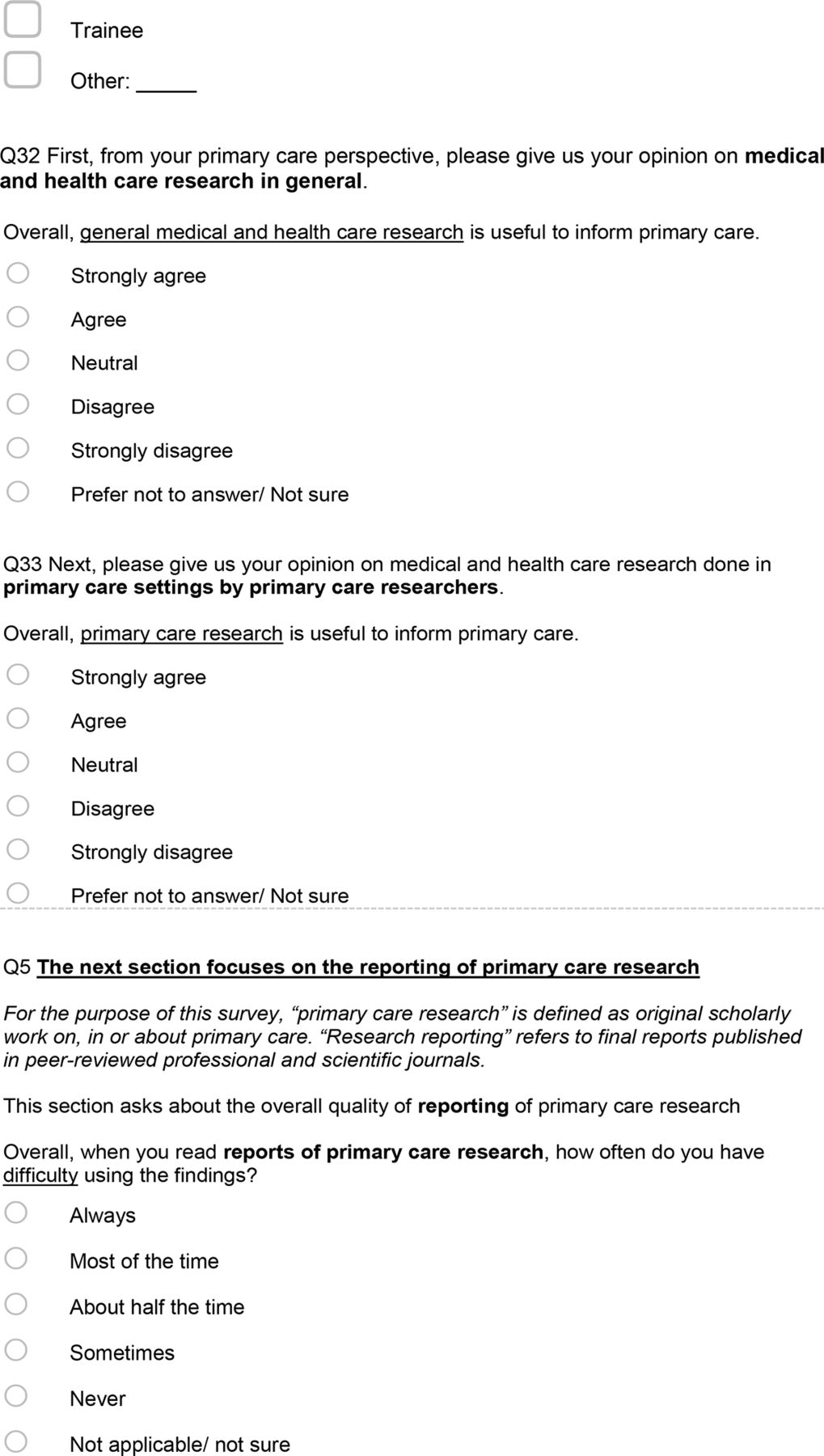
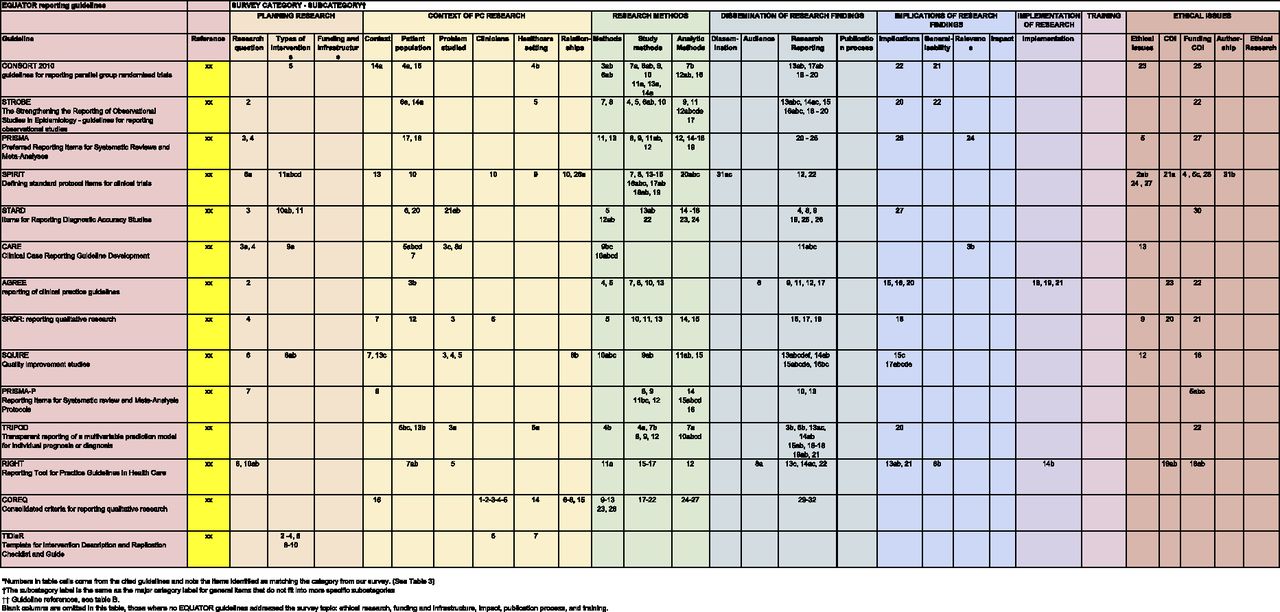
Table A. Comparison of published reporting guidelines with the categories of concern about primary care research reports expressed by survey respondents*




Tables
Characteristic Number % Total respondents 255 100 Gender (n = 255 answering) Male 114 45 Female 138 54 Other gender categories* 3 1 Nationality (n = 237 answering) United States of America 112 47 Australia 47 20 Canada 20 8 United Kingdom 13 5 Netherlands 12 5 Europe (other) 12 5 South America 11 5 Oceania (other) 5 2 Asia 5 2 Not answered 18 Primary profession (multiple options possible, n = 254 answering) Physician 169 67 Scientist 32 13 Educator 20 8 Public Health 18 7 Nursing and nursing practice 9 4 Other (eg, pharmacy, administration, dietitian, behavioral science) 34 13 Types of physicians (total physicians = 169; N = 168 answering) Family medicine/general practice 154 92 Internal medicine (including subspecialties) 6 4 Other (eg, obstetrics/gynecology, pediatrics, sports medicine) 8 5 Not answered 1 Level of research experience (n = 252 answering) Novice 39 15 Intermediate 103 41 Advanced 110 44 Not answered 3 Highest research degree obtained (n = 247 answering) Bachelor’s degree 10 4 Master’s degree 52 21 Doctoral degree (eg, PhD, MD) 159 64 None 21 9 Other 5 2 Not answered 8 Years since completion of professional training (n = 245 answering) 0 to 9 57 22 10 to 19 52 20 20 to 29 53 21 30 to 39 56 22 40 to 49 23 9 50 to 59 4 2 Not answered 10 4 Roles played in PC research (more than one option possible, n = 255) Research/investigator 205 80 Clinician 140 55 Journal reviewer 130 51 Educator 123 48 Editor 42 16 Manager 40 16 Methodologist 40 16 Community member/patient 20 8 Policymaker 16 6 Trainee 14 5 Other (eg, mentor, administrator) 12 5 PC, primary care.
Online survey October 2018 to 2019.
↵* Other gender category includes non-binary/third gender, prefer to self identify, and prefer not to answer.
- Table 2.
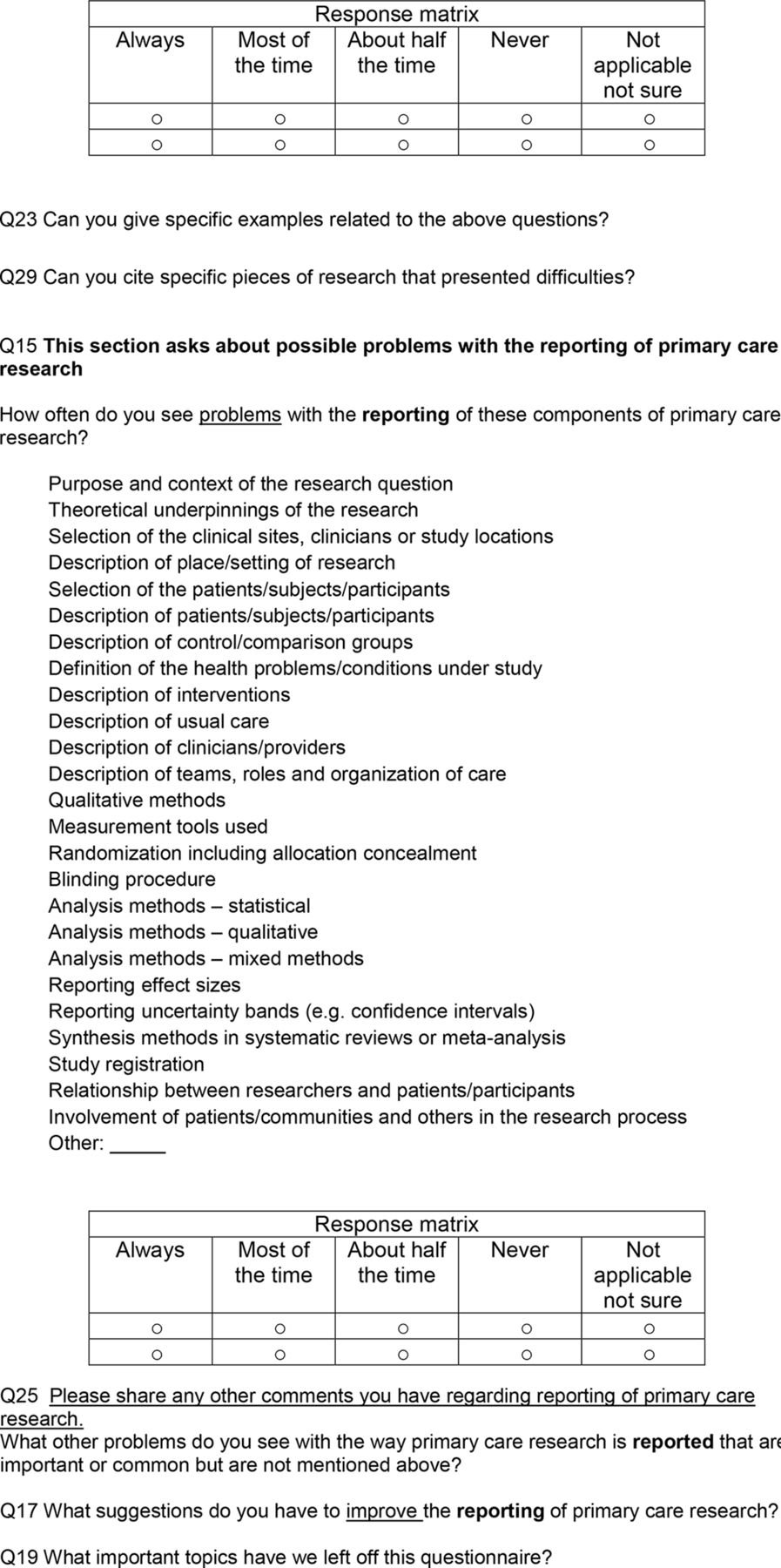
Areas of Primary Care Research Reports Where Respondents Encounter Problems “about Half or More of the Time”
Question* Respondents Answering† Encounter Problems†‡ N (%) Overall, how often does the reporting of PC research cause problems for your work? 198 74 (37.4) How often do reports of primary care research make it difficult for you to: Synthesize findings across studies 188 109 (58.0) Apply the findings to primary care policy 189 97 (51.3) Replicate research findings 168 83 (49.4) Assess the generalizability/transportability of the findings to my patients, practice or community 198 83 (41.9) Identify specific actions that apply to primary care patient care/practice 200 81 (40.5) Apply the findings to primary care education 194 74 (38.1) Apply the findings to further primary care research 193 60 (31.1) How often have you found reporting to be insufficient for these different types of PC research? Qualitative studies 170 84 (49.4) Mixed-methods studies 163 75 (46) Single-arm intervention trials 145 65 (44.8) Randomized controlled trials 164 71 (43.3) Surveys 158 65 (41.1) Cohort studies 171 65 (38) Meta-analysis 164 56 (34.1) Case study research 146 47 (32.2) Systematic reviews 169 53 (31.4) In general, how often is the reporting of PC research problematic in these areas? Authorship and relative contributions of research team members 157 45 (28.7) Role of funders in research and reporting 163 35 (21.5) Potential conflicts of interest of researchers/authors 158 29 (18.4) Ethical conduct of research and institutional approval 163 12 (7.4) How often do you see problems with the reporting of these components of PC research? Theoretical underpinnings of the research 162 87 (53.7) Description of teams, roles, and organization of care 161 86 (53.4) Involvement of patients, communities, others in the research process 148 78 (52.3) Reporting effect sizes 153 76 (49.7) Description of usual care 161 78 (48.4) Description of clinicians/providers 163 76 (46.6) Selection of the clinical sites, clinicians, or study locations 161 75 (46.6) Relationship between researchers and patients/participants 145 65 (44.8) Description of place/setting of research 160 62 (38.8) Analysis methods—mixed methods 151 58 (38.4) Selection of the patients/subjects/participants 163 62 (38) Qualitative methods 159 57 (35.8) Description of patients/subjects/participants 162 57 (35.2) Analysis methods—qualitative 155 53 (34.2) Measurement tools used 160 54 (33.8) Synthesis methods in systematic reviews or meta-analysis 143 47 (32.9) Blinding procedure 154 50 (32.5) Description of control/comparison groups 161 51 (31.7) Reporting uncertainty bands (eg, CIs) 152 46 (30.3) Description of interventions 162 48 (29.6) Purpose and context of the research question 166 48 (28.9) Study registration 135 37 (27.4) Randomization including allocation concealment 148 40 (27) Analysis methods—statistical 158 41 (25.9) Definition of the health problems/conditions under study 161 35 (21.7) Description of interventions 162 48 (29.6) Purpose and context of the research question 166 48 (28.9) Study registration 135 37 (27.4) Randomization including allocation concealment 148 40 (27) Analysis methods—statistical 158 41 (25.9) Definition of the health problems/conditions under study 161 35 (21.7) PC, primary care; CI, confidence interval.
Online survey October 2018 to 2019.
See Appendix 3 for more detailed results.
In each section, items are listed in rank order by percent, not in order of presentation on the questionnaire.
↵* Answers were on a five-point Likert scale with frequency measures. Responses were not compulsory to move forward in the survey.
↵† For each question, “Respondents Answering,” is the number of survey respondents who answered the question with Likert scale scores. “NA/Not Sure” responses are combined with no answers and are not shown. They total 255 – Respondents Answering.
↵‡ “About half or more than half of the time.”
Category
Sub-Category
Summary comment*
•“Respondent quotation.” (respondent characteristics†)PC RESEARCH IS DIFFERENT
Recognition and adaptation to the special character of PC practice and PC researchPLANNING RESEARCH
Description of the way clinicians, patients and community members are involved throughout the research process
•“Every study done in or on PC should have PC experts involved from the initial stages and throughout the process to the final report writing. The same might be proposed for patients or members of the communities studied or affected.” (FP; clinician, researcher; USA; M)†
Research question
Explanation of the origin of the research question
•“Failing to describe where the research question came from.” (FP; clinician, researcher; USA; M)
FUNDING AND INFRASTRUCTURE
Support of non-academic writing and reporting
•“Assure a research writer for clinicians.” (Behavioral scientist; educator, researcher; USA; F)CONTEXT OF PC RESEARCH
Description of the complex contexts of patients, problems and practice
•“It’s not so much the reporting but the many different contexts that family medicine can represent.” (FP; clinician, community member/patient, educator, reviewer, researcher; nation not stated; F)
•“PC has many contexts, types of practitioners and also takes patients into account – patient-centered care and factors in multimorbidities and preventative medicine. (Public health scientist; researcher; Australia, F)
Patient population
Description of patients and populations in practice and community-based research
“PC research includes a wide variety of patients and demographics which are oftentimes not directly applicable to larger studies conducted elsewhere.” (FP; researcher, trainee; USA; M)
Problem studied
Recognition and description of illness as it occurs in PC
•“Also the single disease single intervention is not always how patients present. A depressed childhood abuse survivor is not as interested in diabetic dietary guidelines when they are struggling with complex chronic trauma.” (FP; clinician, community member/patient, educator, reviewer, researcher; country not stated; F)
Clinicians
Description of clinicians, teams and how they are organized
“Types of clinicians, teams and how they are organized is impt and different. Clustering of pts, clinicians, teams and clinics is impt and often not reported adequately or accounted for in data analysis.” (FP; clinician, community member/patient, editor, educator, reviewer, researcher; USA; M)
Types of interventions
Description of pragmatic and complex interventions in PC
•“PC research tends to be more pragmatic and complex interventions and the reporting of methods is often less clear than in other settings.” (Pharmacy; reviewer, researcher; Australia; F)
Healthcare setting
Recognition and description of the complex settings of care and work in PC
•“Often the study is locale - and setting - specific, without much description of the ways in which protocol and implementation were shaped by these specifics.” (FP; clinician, editor, educator, reviewer; USA; F)
•“Health care setting is often not reported.” (FP; clinician, editor, educator, researcher; Norway; F)
•“Contextual factors are critical, yet not often reported. What kind of settings was the research performed in matter.”? (FP; journal reviewer, researcher; USA; M)
Relationships
Recognition and description of the relationships among patients, families, clinicians and other members of PC teams
•“Ideally I think relationship building is also important in both the research and the implementation and this should also be reported.” (FP; clinician, educator, reviewer, researcher; Australia; F)RESEARCH METHODS
Study methods
Presentation of the underlying theory behind the research
•“It would be helpful to allow a section for theoretical underpinnings. PC research often lacks theory, although researchers use theories, they may or may not be aware of them. Theories people draw on in designing a study, collecting and analysis data must be made explicit.” (Scientist; researcher; Canada, F)
Analytic Methods
Description of how findings and interpretation were checked with study participants
•“It would be great if those undertaking the research reported how they corroborated their interpretation of the findings with study participants. This is rarely reported.” (Nursing; educator, reviewer, researcher; New Zealand, F)DISSEMINATION OF RESEARCH FINDINGS
Presentation of findings in accessible and comprehensible way to patients and communities affected
•“Clinicians and researchers should strive to make their research accessible beyond their peer group, especially when patients and community members were involved in the research. We should strive to make our findings accessible and comprehensible to the communities we serve.” (Public health; educator, manager, community member/patient; USA; F)
Presentation of findings in accessible and comprehensible way to PC clinicians
•“The strengths and drawbacks of reporting depends on the audience. Is the reporting for a solo physician or small group, in which case the reporting is too technical, focusing on research and not practical implementation, and difficult to know how it applies to one’s own clinic population? If the audience is researchers, there’s different ways to improve the reporting more along the lines of methods and statistics. If the audience is large group practices looking for system or policy solutions, then it gets back to generalizability and implementation.” (FP; researcher; USA; F)
Research Reporting
Guidance from PC research reporting guidelines that are different than currently exist
•“We need standards for reporting mixed methods research which don’t currently exist (Equator does not have any) - PC research includes lots of mixed methods research. (Health services researcher; methodologist, reviewer, community member/patient; UK, F)
•“A checklist would be beneficial for both peer reviewers and authors. Provide authors a standardized checklist specific to PC research.” (Editor; educator, reviewer, methodologist, researcher; Australia, M)
Publication process
Adequate space to adequately space to describe PC research methods, results and context.
•“Good PC research often requires a larger word limit than the usual to describe things like the theoretical stance used, the context of the research setting, how qualitative analysis was undertaken, and in the case of qualitative or mixed methods - space to give results. The solution to this is for more on-line publications to prevail and the encouragement therefore of use of supplementary files.” (FP; educator, reviewer, researcher; Australia, F)IMPLICATIONS OF RESEARCH FINDINGS
Richer discussion of implications for research, practice, education and policy
•“Adding to research reporting, whatever is appropriate: Implications for future research, implications for practice, implications for policy.” (FP; researcher; Canada, M)
Generalizability
Description of the context in sufficient detail to assess generalizability to variety of PC contexts
•“It is important to have a good sense of context to assess whether the findings can be used in a different PC context, under which circumstances they can work and when not.” (Scientist; researcher; Canada, F)
Relevance
Demonstration that researchers and authors have grounded understanding of PC
•“…the SPRINT study and the hypertension guidelines that came from that: authored by specialists who had little understanding of PC.” (FP; editor, reviewer, researcher; USA, M)
•“Articles written by specialists for a PC audience are also often flawed because they at best only partially understand PC.” (FP; editor, reviewer, manager, researcher; Australia; M)IMPLEMENTATION OF RESEARCH
Description in details sufficient for implementation, application and translation
•[A major] “national demonstration project. Introduced a team-based approach hard to replicate without the additional support of the grant dollars and institutional infrastructure. Created a model of care that was formidable to the 80% of practices who did not have that infrastructure and are small 2 to 4 clinician practices. Offered no meaningful information about how to make the case with leadership to promote adoption of such a model. Why should a clinician take the risk to hire a full-time employee with no billable hours when already working close the profit line? Answers are actually easy… but not reported” (Health services researcher; educator, reviewer, methodologist; USA; F)ETHICAL ISSUES
Conflicts of interest
Information to help readers better assess potential conflicts of interest
•“It is very difficult to measure the conflict of interest.” (W, Hungary, Pharmacy, educator, journal reviewer, researcher)
•“La falta de financiación para este tipo de estudios, hace que los investigadores se asocien a empresas que tienen altos intereses.” (Google translation—“The lack of funding for this type of studies, makes researchers associate with companies that have high interests.) (Public health scientist; clinician; Argentina; M)
Authorship
Description of contributions among large, multidisciplinary collaborative author groups
•“PC research often involves collaboration of large groups of individuals from various backgrounds, who often don’t discuss or agree upon authorship before starting the research…. It becomes very unclear whether some of them actually made any contribution to the study design, analysis, interpretation or writing of the results” (Family Medicine Scientist; methodologist, researcher; Canada, F)Reference Number Guideline Reference 1 CONSORT 2010 guidelines for reporting parallel group randomised trials Moher D, Hopewell S, Schulz KF, Montori V, Gøtzsche PC, Devereaux PJ, Elbourne D, Egger M, Altman DG, for the CONSORT Group. CONSORT 2010 Explanation and Elaboration: updated guidelines for reporting parallel group randomised trial. BMJ. 2010;340:c869. 2 STROBE The Strengthening the Reporting of Observational Studies in Epidemiology - guidelines for reporting observational studies Vandenbroucke JP, von Elm E, Altman DG, Gotzsche PC, Mulrow CD, Pocock SJ, Poole C, Schlesselman JJ, Egger M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and Elaboration. PLoS Med. 2007;4(10):e297. 3 PRISMA Preferred Reporting Items for Systematic Reviews and Meta-Analyses Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. BMJ. 2009; 339:b2535. 4 SPIRIT Defining standard protocol items for clinical trials Chan A-W, Tetzlaff JM, Gøtzsche PC, Altman DG, Mann H, Berlin J, Dickersin K, Hróbjartsson A, Schulz KF, Parulekar WR, Krleža-Jerić K, Laupacis A, Moher D. SPIRIT 2013 Explanation and Elaboration: Guidance for protocols of clinical trials. BMJ. 2013;346:e7586. 5 STARD Items for Reporting Diagnostic Accuracy Studies Bossuyt PM, Reitsma JB, Bruns DE, Gatsonis CA, Glasziou PP, Irwig L, LijmerJG Moher D, Rennie D, de Vet HCW, Kressel HY, Rifai N, Golub RM, Altman DG, Hooft L, Korevaar DA, Cohen JF, For the STARD Group. STARD 2015: An Updated List of Essential Items for Reporting Diagnostic Accuracy Studies. 6 CARE Clinical Case Reporting Guideline Development Gagnier JJ, Kienle G, Altman DG, Moher D, Sox H, Riley D; the CARE Group. The CARE Guidelines: Consensus-based Clinical Case Reporting Guideline Development. BMJ Case Rep. 2013; doi: 10.1136/bcr-2013-201554. 7 AGREE reporting of clinical practice guidelines Brouwers MC, Kerkvliet K, Spithoff K, AGREE Next Steps Consortium. The AGREE Reporting Checklist: a tool to improve reporting of clinical practice guidelines. BMJ. 2016;352:i1152. 8 SRQR: reporting qualitative research O'Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89(9):1245-1251. 9 SQUIRE Quality improvement studies Ogrinc G, Davies L, Goodman D, Batalden P, Davidoff F, Stevens D. SQUIRE 2.0 (Standards for QUality Improvement Reporting Excellence): revised publication guidelines from a detailed consensus process. 10 PRISMA-P Reporting Items for Systematic review and Meta-Analysis Protocols Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1. 11 TRIPOD Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis Collins GS, Reitsma JB, Altman DG, Moons KG. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): The TRIPOD statement. Ann Intern Med. 2015;162(1):55-63. 12 RIGHT Reporting Tool for Practice Guidelines in Health Care Chen Y, Yang K, Marušić A, Qaseem A, Meerpohl JJ, Flottorp S, Akl EA, Schünemann HJ, Chan ESY, Falck-Ytter Y, Ahmed F, Barber S, Chen C, Zhang M, Xu B, Tian J, Song F, Shang H, Tang K, Wang Q, Norris SL; for the RIGHT (Reporting Items for Practice Guidelines in Healthcare) Working Group. A Reporting Tool for Practice Guidelines in Health Care: The RIGHT Statement. Ann Intern Med. 2017;166(2):128-132. 13 COREQ Consolidated criteria for reporting qualitative research Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349-357. 14 TIDieR Template for Intervention Description and Replication Checklist and Guide Hoffmann T, Glasziou P, Boutron I, Milne R, Perera R, Moher D, Altman D, Barbour V, Macdonald H, Johnston M, Lamb S, Dixon-Woods M, McCulloch P, Wyatt J, Chan A, Michie S. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. 2014;348:g1687. Respondent Ratings of Frequency of Encountering Problems with the Reporting of Primary Care Research
Question* R† Never
N (%)Sometimes
N (%)About Half the Time
N (%)Most of the Time
N (%)Always
N (%)Summary:
About half the time or more
N (%)A. Overall, how often does the reporting of primary care research cause problems for your work* 198 6 (3) 118 (59.6) 51 (25.8) 20 (10.1) 3 (1.5) 74 (37.4) B. How often do reports of primary care research make it difficult for you to:* Assess the generalizability/transportability of the findings to my patients, practice or community 198 5 (2.5) 110 (55.6) 43 (21.7) 38 (19.2) 2 (1) 83 (41.9) Identify specific actions that apply to primary care patient care/practice 200 10 (5) 109 (54.5) 41 (20.5) 37 (18.5) 3 (1.5) 81 (40.5) Apply the findings to primary care policy 189 6 (3.2) 86 (45.5) 54 (28.6) 37 (19.6) 6 (3.2) 97 (51.3) Apply the findings to primary care education 194 6 (3.1) 114 (58.8) 44 (22.7) 23 (11.9) 7 (3.6) 74 (38.1) Apply the findings to further primary care research 193 17 (8.8) 116 (60.1) 36 (18.7) 20 (10.4) 4 (2.1) 60 (31.1) Replicate research findings 168 6 (3.6) 79 (47) 37 (22) 39 (23.2) 7 (4.2) 83 (49.4) Synthesize findings across studies 188 3 (1.6) 76 (40.4) 53 (28.2) 47 (25) 9 (4.8) 109 (58.0) C. How often have you found reporting to be insufficient for these different types of primary care research? * Randomized Controlled Trials 164 6 (3.7) 87 (53.1) 37 (22.6) 29 (17.7) 5 (3.1) 71 (43.3) Qualitative studies 170 9 (5.3) 77 (45.3) 63 (37.1) 15 (8.8) 6 (3.5) 84 (49.4) Cohort studies 171 6 (3.5) 100 (58.5) 45 (26.3) 17 (9.9) 3 (1.8) 65 (38) Mixed methods studies 163 4 (2.5) 84 (51.5) 46 (28.2) 26 (16) 3 (1.8) 75 (46) Single arm intervention trials 145 5 (3.5) 75 (51.7) 35 (24.1) 24 (16.5) 6 (4.1) 65 (44.8) Systematic Reviews 169 12 (7.1) 104 (61.5) 34 (20.1) 14 (8.3) 5 (3) 53 (31.4) Meta-analysis 164 15 (9.2) 93 (56.7) 25 (15.2) 24 (14.6) 7 (4.3) 56 (34.1) Case study research 146 15 (10.3) 84 (57.5) 21 (14.4) 20 (13.7) 6 (4.1) 47 (32.2) Surveys 158 13 (8.2) 80 (50.6) 35 (22.2) 23 (14.6) 7 (4.4) 65 (41.1) D. In general, how often is the reporting of primary care research problematic in these areas?* Potential conflicts of interest of researchers/authors 158 27 (17.1) 102 (64.6) 18 (11.4) 9 (5.7) 2 (1.3) 29 (18.4) Role of funders in research and reporting 163 30 (18.4) 98 (60.1) 18 (11) 16 (9.8) 1 (0.6) 35 (21.5) Authorship and relative contributions of research team members 157 30 (19.1) 82 (52.2) 27 (17.2) 15 (9.6) 3 (1.9) 45 (28.7) Ethical conduct of research and institutional approval 163 67 (41.1) 84 (51.5) 7 (4.3) 4 (2.5) 1 (0.6) 12 (7.4) E. How often do you see problems with the reporting of these components of primary care research?* Purpose and context of the research question 166 15 (9) 103 (62.1) 37 (22.3) 10 (6) 1 (0.6) 48 (28.9) Theoretical underpinnings of the research 162 5 (3.1) 70 (43.2) 50 (30.9) 34 (21) 3 (1.9) 87 (53.7) Selection of the clinical sites, clinicians or study locations 161 11 (6.8) 78 (48.5) 43 (26.7) 26 (16.2) 3 (1.9) 75 (46.6) Description of place/setting of research 160 18 (11.3) 80 (50) 34 (21.3) 25 (15.6) 3 (1.9) 62 (38.8) Selection of the patients/subjects/participants 163 11 (6.8) 90 (55.2) 40 (24.5) 20 (12.3) 2 (1.2) 62 (38) Description of patients/subjects/participants 162 12 (7.4) 93 (57.4) 38 (23.5) 17 (10.5) 2 (1.2) 57 (35.2) Description of control/comparison groups 161 11 (6.8) 99 (61.5) 33 (20.5) 18 (11.2) 0 (0) 51 (31.7) Definition of the health problems/conditions under study 161 16 (9.9) 110 (68.3) 25 (15.5) 9 (5.6) 1 (0.6) 35 (21.7) Description of interventions 162 13 (8) 101 (62.4) 32 (19.8) 15 (9.3) 1 (0.6) 48 (29.6) Description of usual care 161 9 (5.6) 74 (46) 41 (25.5) 32 (19.9) 5 (3.1) 78 (48.4) Description of clinicians/providers 163 8 (4.9) 79 (48.5) 46 (28.2) 23 (14.1) 7 (4.3) 76 (46.6) Description of teams, roles and organization of care 161 4 (2.5) 71 (44.1) 48 (29.8) 33 (20.5) 5 (3.1) 86 (53.4) Qualitative methods 159 6 (3.8) 96 (60.4) 42 (26.4) 13 (8.2) 2 (1.3) 57 (35.8) Measurement tools used 160 10 (6.3) 96 (60) 42 (26.3) 11 (6.9) 1 (0.6) 54 (33.8) Randomization including allocation concealment 148 8 (5.4) 100 (67.6) 25 (16.9) 13 (8.8) 2 (1.4) 40 (27) Blinding procedure 154 7 (4.6) 97 (63) 33 (21.4) 15 (9.7) 2 (1.3) 50 (32.5) Analysis methods – statistical 158 9 (5.7) 108 (68.4) 32 (20.2) 8 (5.1) 1 (0.6) 41 (25.9) Analysis methods – qualitative 155 4 (2.6) 98 (63.2) 40 (25.8) 12 (7.7) 1 (0.7) 53 (34.2) Analysis methods – mixed methods 151 5 (3.3) 88 (58.3) 43 (28.5) 14 (9.3) 1 (0.7) 58 (38.4) Reporting effect sizes 153 5 (3.3) 72 (47.1) 49 (32) 26 (17) 1 (0.7) 76 (49.7) Reporting uncertainty bands (e.g. confidence intervals) 152 11 (7.2) 95 (62.5) 34 (22.4) 11 (7.2) 1 (0.7) 46 (30.3) Synthesis methods in systematic reviews or meta-analysis 143 6 (4.2) 90 (62.9) 34 (23.8) 12 (8.4) 1 (0.7) 47 (32.9) Study registration 135 18 (13.3) 80 (59.3) 22 (16.3) 14 (10.4) 1 (0.7) 37 (27.4) Relationship between researchers and patients/participants 145 11 (7.6) 69 (47.6) 38 (26.2) 26 (17.9) 1 (0.7) 65 (44.8) Involvement of pts/communities, others the research process 148 6 (4.1) 64 (43.2) 38 (25.7) 36 (24.3) 4 (2.7) 78 (52.7) Online survey October 2018 to 2019.
↵* Answers were on a five-point Likert scale with frequency measures. Responses were not compulsory to move forward in the survey.
↵† R = For each question, “Respondents Answering,” is the number of survey respondents who answered the question with Likert scale scores. “NA/Not Sure” responses are combined with no answers and are not shown. They total (Study n = 255) – Respondents Answering.
In each section, items are listed in rank order by percent, not in order of presentation on the questionnaire.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- CONSORT 2025 explanation and elaboration: updated guideline for reporting randomised trials
- Ameliorer les rapports de recherche en soins primaires: Presentation de la Liste de verification des elements de rapport detudes en soins primaires etablis par consensus
- Improving primary care research reporting: Introducing the Consensus Reporting Items for Studies in Primary Care checklist
- Improving the Reporting of Primary Care Research: Consensus Reporting Items for Studies in Primary Care--the CRISP Statement
- Key items for reports of primary care research: an international Delphi study
- International reflections on NAPCRG: celebrating 50 years of learning and connecting
- Clinician Use of Primary Care Research Reports
- Advancing Research Methods for Common Problems in Family Medicine and Family Medicine Practice Management