
Abstract
Background: Cardiovascular disease (CVD) is the leading cause of death among breast cancer (BC) survivors. BC survivors are at increased risk of CVD due to a higher prevalence of risk factors. Current data are limited on the cardiovascular screening practices and lipid management in this population in primary care settings.
Methods: A retrospective case control study was performed with 105 BC survivors and 210 matched controls (based on age and medical comorbidities of diabetes, hypertension, and hyperlipidemia). BC survivors were established with primary care practices within a large academic institution and had completed primary cancer treatment. Data on screening for CVD and lipid management were collected via a retrospective chart review.
Results: The average BC survivor was 63 years old, with 9 years since diagnosis. Compared with matched controls, BC survivors had more cholesterol screening (88% vs 70%, P < .001) and active statin prescriptions (63% vs 40%, P < .05) if indicated by the Atherosclerotic Cardiovascular Disease Calculator. There were no differences in CVD screening in White and African American BC survivors. However, African American BC survivors were more likely to have hypertension (P < .01) and have a body mass index in the overweight and obese category (P < .001) than White BC survivors. Older BC survivors were more likely to receive cholesterol screening.
Discussion: This study demonstrates that BC survivors who have an established primary care provider have improved cholesterol screening and statin therapy based on their risk of developing chronic diseases.
- Cardiovascular Diseases
- Case-Control Studies
- Hyperlipidemias
- Obesity
- Prevalence
- Retrospective Studies
- Risk Factors
- Statins
- Survivorship
Introduction
In 2016, there were over 3.5 million women living in the United States with a history of breast cancer (BC).1 Cardiovascular disease (CVD) is the most common cause of death in older BC survivors.2,3 Furthermore, BC survivors are at increased risk of CVD when compared with individuals without history of cancer.4⇓⇓⇓⇓⇓⇓–11 The etiology of CVD in BC survivors is multifactorial. BC and CVD share common risk factors, including activation of inflammatory pathways.12⇓⇓⇓–16 Management of comorbid medical conditions has also been shown to be suboptimal during active cancer treatment, and cancer disease processes themselves may cause subclinical myocardial damage.2 Cancer therapies, including radiotherapy, chemotherapy, and endocrine therapies, can negatively impact cardiovascular health in 3 domains: vascular conditions, structural problems, and cardiac dysfunction.17⇓⇓⇓⇓⇓–23 The risk of CVD increases with additional risk factors and exposures, as the “multi-hit hypothesis” has proposed.2,22
There are limited guidelines for screening for CVD in BC survivors; however, studies are ongoing regarding the use of biomarkers, imaging modalities, and preventive medications for cardiovascular risk reduction.2,23⇓–25 Current strategies for risk factor reduction in BC survivors include aggressive management of comorbid conditions, including hypertension, diabetes, hyperlipidemia, and promotion of lifestyle factors such as smoking cessation, maintaining an appropriate body weight, and increased physical activity.3,19,23,26⇓–28
BC survivors are followed by multiple specialists, which often includes oncology, primary care, and cardiology. Communication between primary care and oncology is often insufficient with poor differentiation of roles in the care of cancer survivors.29⇓⇓⇓⇓⇓–35 Cancer survivors who see both cancer specialists and primary care received a wider range of appropriate clinical services as compared with those seeing cancer specialists alone.36⇓⇓–39
Limited studies have evaluated cardiovascular screening practices in BC survivors and have focused predominantly on those over the age of 65 years, an age at which there is decreased benefit to preventive interventions. BC survivors self report increased cholesterol screening compared with the general population, although claims-based data demonstrate decreased receipt of preventive health services and screenings, including cholesterol screening.16,38 Empirical data are not available on the type of provider who is likely to screen BC survivors for CVD risk. Chidwick et al40 demonstrated similar initiation of statin therapy in BC survivors with high cardiovascular risk as compared with a control population. However, when evaluating statin use 1-year following initiation, cancer survivors had increased rates of discontinuation.
Despite increased risk of CVD and cardiovascular mortality for BC survivors compared with the general population, cardiovascular screening practices and risk reduction through statin therapy has not been evaluated and has, in particular, not been evaluated to our knowledge in a cohort that includes individuals under the age of 65 years. Investigation has also not been conducted regarding the specialty providing this care. In this study, we sought to evaluate cholesterol screening and management in BC survivors compared in a retrospective case-control study with further analysis regarding differences between African American and White BC survivors.
Methods
Study Design
A retrospective case-control study with 105 BC survivors and 210 matched controls was conducted at the Medical University of South Carolina (MUSC). The project received MUSC Institutional Review Board approval with a waiver of informed consent. Inclusion criteria for BC survivors were individuals between 40 and 75 years old with previous diagnosis of BC not currently receiving active cancer therapy. Endocrine therapy (ie, aromatase inhibitors, tamoxifen, ovarian suppression) was not considered active therapy for the purpose of this study. BC survivors included had identified MUSC Primary Care as their primary care provider with a primary care visit between December 2017 and February 2018. There are 20 outpatient clinics that comprise MUSC Primary Care, composed of internal medicine (26%) and family medicine (51%) physicians and advanced practice providers (23%). Exclusion criteria included individuals who were currently receiving active primary treatment or hospice care. History of CVD was not considered an exclusion criterion; however, disease incidence is documented. Cancer diagnosis outside of superficial skin cancer was not found in cases or controls. BC survivors were matched with individuals without history of malignancy seen at the same primary care clinics within 3 months at a 2:1 ratio of controls to cases to improve the power of the study.41 Matching criteria included age and the presence or absence of the medical comorbidities of diabetes, hypertension, and hyperlipidemia. These comorbidities were selected based on their impact on screening parameters and statin use. An electronic medical record inquiry was conducted among individuals seen by the associated primary care clinics with ICD codes consistent with diagnosis of BC. A random number generator was used to assign a number to each of the eligible individuals identified. The first 105 individuals study criteria were included to meet the sample size established through power analysis. A list of control individuals was generated, when greater than 2 individuals met matching criteria each match was assigned a random number and those receiving the lowest 2 numbers were selected. In 5 cases, a match meeting the criteria of age and comorbidities was unavailable so a match consistent with at least 1 comorbidity was used.
Data Collection
Data extraction was initially conducted by a research data warehouse inquiry and then subsequently by manual chart review for the data unable to be extracted through the initial query. Demographic data obtained included age and race/ethnicity. Clinic variables obtained included date of last primary care provider visit. Cancer-related variables for cases included year of diagnosis, stage, treatments received, and receptor status. Comorbidity data included the presence or absence of hypertension, hyperlipidemia, diabetes, myocardial infarction, cerebrovascular accident, and coronary artery disease. Outcome variables included last blood pressure, body mass index, date and ordering provider of last lipid panel, statin therapy and ordering provider, atherosclerotic cardiovascular disease (ASCVD) risk, and hemoglobin A1c. Chart review was conducted by the principal investigator and subsequently verified in a population of 10% of randomly selected participants by our data analyst for manually extracted data with a Cohen’s kappa value of 0.933 for inter-rater reliability. Individuals with a diagnosis of hypertension were determined to have controlled blood pressure if their most recent blood pressure reading was <140/90 based on the Eighth Joint National Committee recommendations.42 An individual was considered to have received screening for hyperlipidemia if a lipid panel or its component pieces had been obtained within 3 years. ASCVD risk was calculated for each individual (ages 40 to 75 years based on inclusion criteria) without history of diabetes, coronary artery disease, or known cardiovascular event based on the most recent blood pressure and lipid panel.43 Indications for statin therapy included a 10-year ASCVD greater than 7.5%, current diagnosis of diabetes, or previous major cardiovascular event which includes myocardial infarction or cerebrovascular accident. All individuals with documented coronary artery disease on their problem list had a statin indication based on the criteria above. The specialty of the ordering provider was determined by review of the electronic medical record of the ordering provider for the test or medication. For the purposes of this study, potentially cardiotoxic therapies received included radiation therapy, anthracyclines, endocrine therapies, and trastazumab.
Statistical Considerations
A power calculation was conducted to determine the sample size needed to detect a 15% difference in cholesterol screening with α of 0.05 and β 0.85 and an enrollment ratio of 2:1. IBM SPSS v25 was used for statistical analyses. Descriptive statistics were calculated for all variables. Group means and standard deviations are presented for continuous variable. Counts and percentages are presented for categorical values. Comparisons were made between groups using the Student’s t-test and Pearson’s c2 analysis as applicable. P < .05 was considered statistically significant for all analyses. Binary logistic regression was conducted for lipid screening and statin use for cancer survivors and controls and based on race with use of categories of White as compared with other races which was predominantly African American.
Results
Study Population
The average age of BC survivors was 63 years, with an average time of diagnosis 9.4 years prior and median time of diagnosis 6 years prior. The racial distribution of individuals included in the study as well as the incidence of medical comorbidities in shown in Table 1. Clinical information related to BC for the study sample is provided in Table 1. Of the BC survivors, 6.7% were found to have had a previous heart attack or stroke, compared with 1.4% of controls (P < .05). Minor differences in the incidence of hyperlipidemia and diabetes were found due to limitations in matching all participants with an equivalent age and comorbidity matched control. ASCVD risk was calculated for those individuals for whom it was appropriate to calculate and is shown in Table 1. Body mass index was the same between BC survivors and matched controls. Primary care provided 93.7% of the cholesterol screening and prescribed 93.6% of statins to BC survivors (Table 1). Cardiology was the next most common specialty providing cholesterol screening and statin therapy.
Demographic Data
Cardiovascular Screening and Lipid Management in BC Survivors
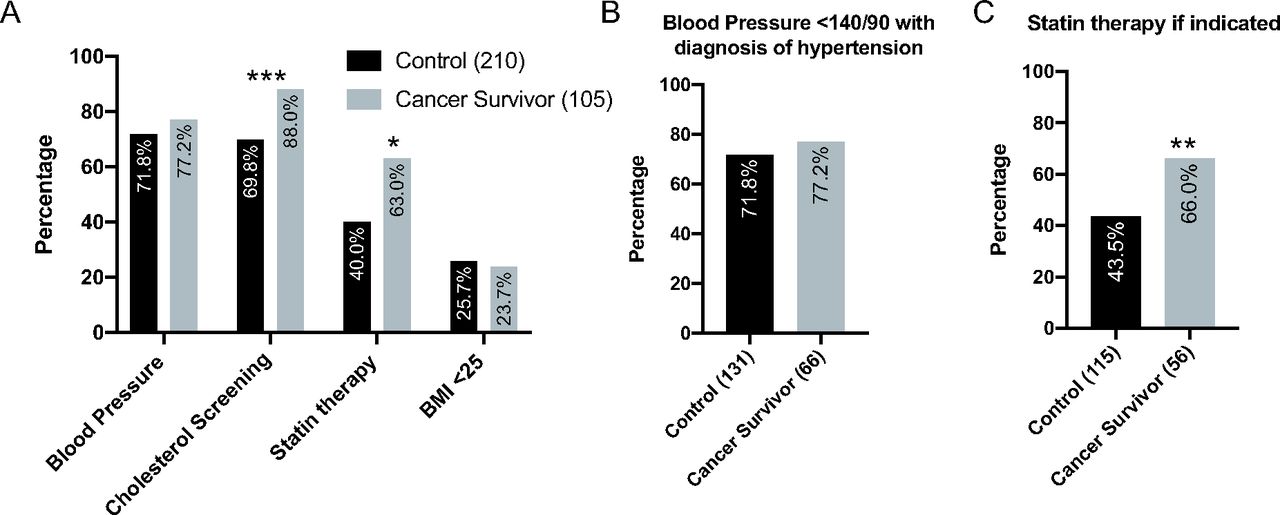
BC survivors were more likely than controls to receive cholesterol screening (P < .001) and statin therapy (P < .05) than age and comorbidity matched controls (Figure 1A). There was no significant difference in blood pressure control in cancer survivors and controls or the percentage of individuals who were overweight or obese based on body mass index (Figure 1A). No significant differences between cardiovascular screening and lipid management were observed based on time of diagnosis with BC, stage at time of diagnosis, or treatments received (data not shown). When blood pressure control was assessed in individuals with a diagnosis of hypertension, no significant differences were observed in the percentage of individuals with controlled blood pressure (Figure 1B). In individuals with an indication for statin therapy, cancer survivors were more likely to have a current prescription for statin therapy (P < .05) (Figure 1C). Multivariate analysis for statin therapy (Nagelkerke R-squared value was 0.08 for the model) showed that BC survivors were more likely to be on statin therapy (P = .001). For lipid screening the Nagelkerke R-squared value was 0.06. Cancer survivors were more likely to receive lipid screening within 3 years (P = .017).
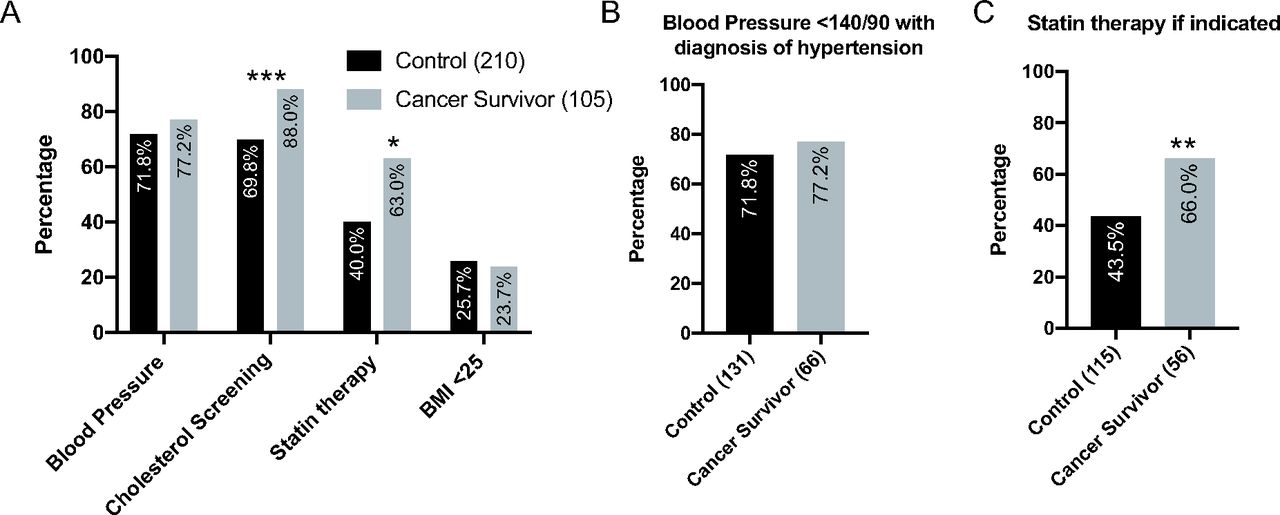
Cardiovascular screening and statin therapy in breast cancer (BC) survivors. A, BC survivors are more likely to have received cholesterol screening and statin therapy than matched controls. B, Subgroup analysis of BC survivors with a diagnosis of hypertension have no differences in blood pressure control compared with comorbidity matched peers. C, Subgroup analysis of BC survivors are more likely than matched controls to have an active statin prescription if indicated. Sample size is indicated in parentheses for each group. Abbreviation: BMI, body mass index. *P < .05, ** P < .01, ***P < .001.
Cardiovascular Screening and Lipid Management in BC Survivors by Race
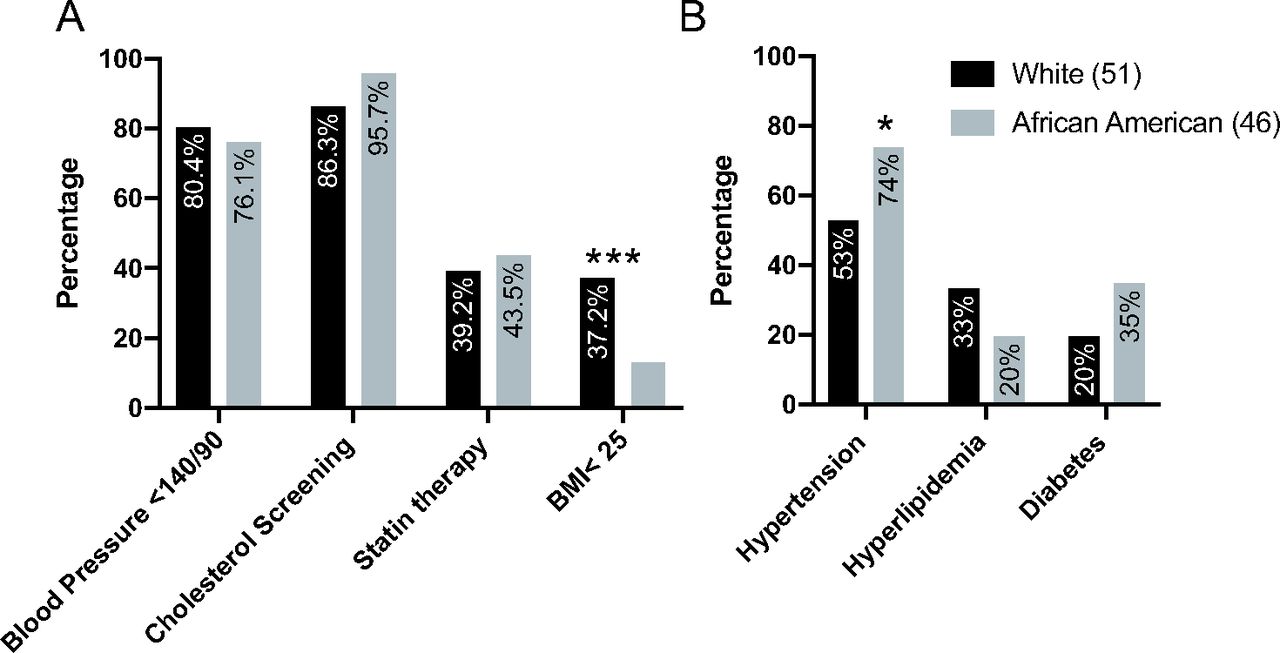
African American BC survivors were found to have no differences in cardiovascular screening, blood pressure control and statin use as compared with White BC survivors (Figure 2A). African American BC survivors were less likely to have a body weight in the appropriate range (Figure 2A, P < .01). African American women were noted to have a higher incidence of hypertension (Figure 2B). African American BC survivors did not have a higher incidence of diabetes than White BC survivors in our study (35% vs 20%, P = .09).

Cardiovascular screening, management, and comorbidities in African American and White breast cancer (BC) survivors. A, No differences in cardiovascular screening and management were observed between White and African American BC survivors; however, African American BC survivors were found to have a decreased incidence of having a body mass index less than 25 kg/m2. B, African American BC survivors are more likely to have a diagnosis of hypertension. Sample size is indicated in parentheses for each group. Abbreviation: BMI, body mass index. *P < .05, ***P < .001.
Older BC Survivors Have Increased Cholesterol Screening
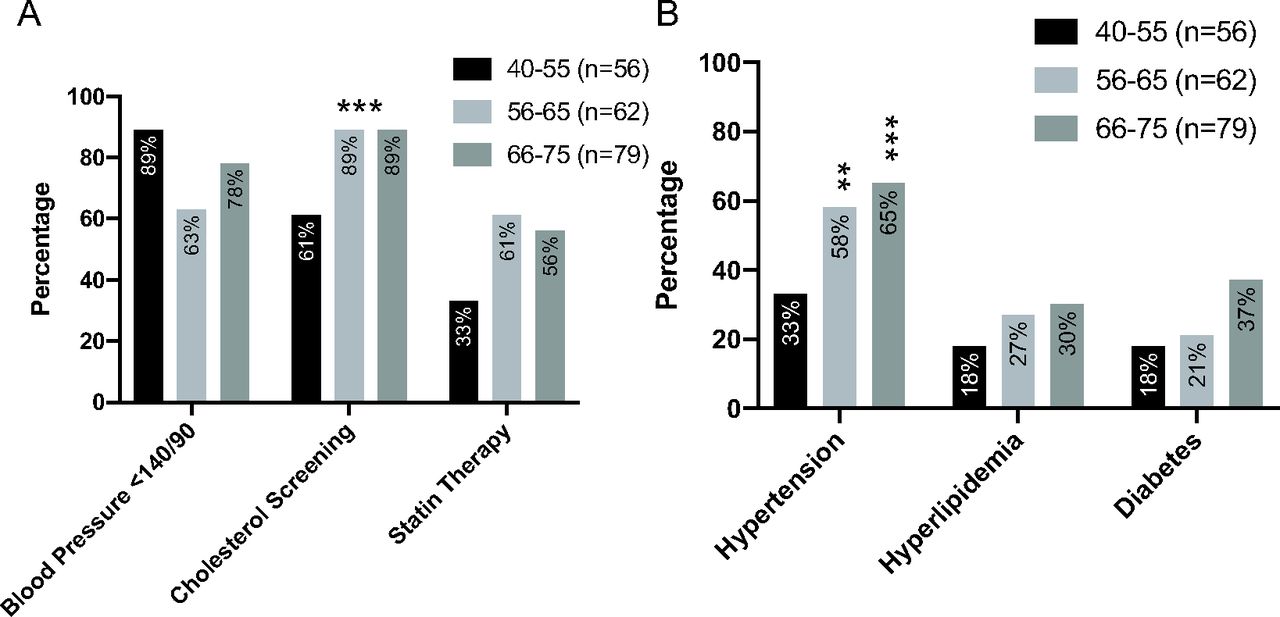
Older BC survivors have increased cholesterol screening as compared with those 40 to 55 years old (P < .001) (Figure 3A). Individuals aged 66 to 75 years old had an increased incidence of hypertension and diabetes compared with younger BC survivors (Figure 3B).
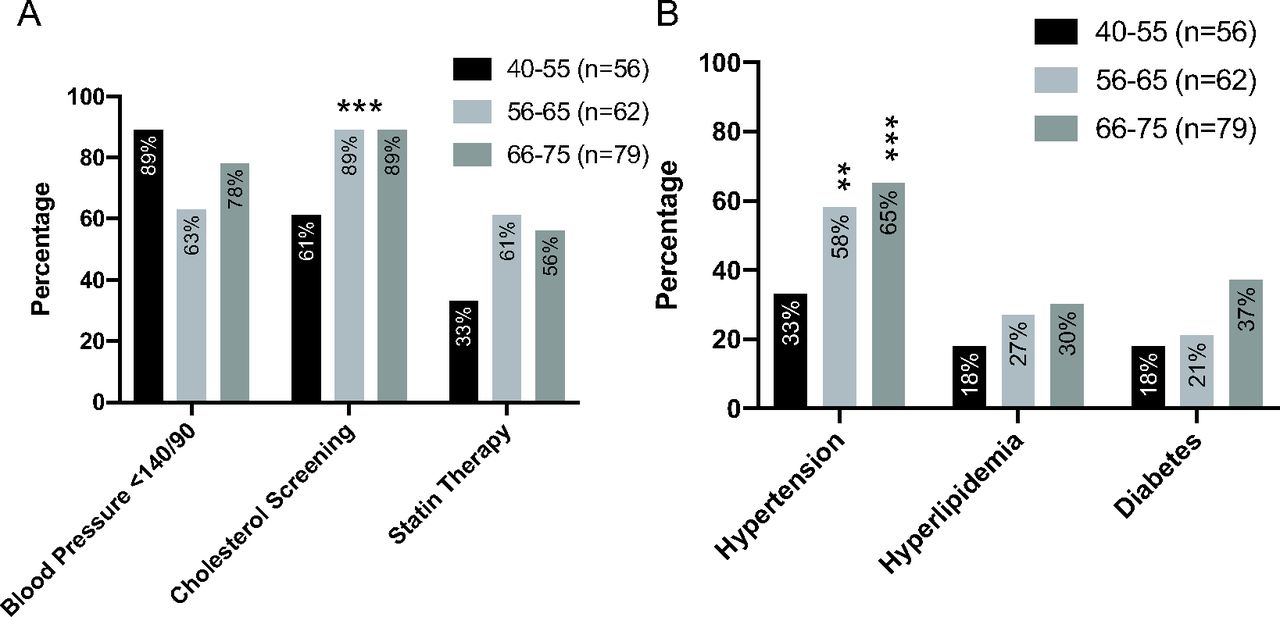
Impact of age on cardiovascular screening breast cancer (BC) survivors. A, Cardiovascular screening and management of BC survivors stratified by age. Older individuals are more likely to have received cholesterol screening than younger counterparts. B, Incidence of comorbidities based on age in BC survivors. Older BC survivors have a higher incidence of hypertension. Sample size is indicated in parentheses for each group. *P < .05, **P < .01, ***P < .001.
Discussion
Cardiovascular morbidity and mortality disproportionately impact BC survivors compared with women who do not have a personal history of the disease, in part due to previous cancer treatments received. CVD is often a late effect of treatment, with the onset of this disease often occurring several years after primary cancer treatment has been completed. In this article, we characterized the CVD screening practices among BC survivors who had an established primary care provider. Our study demonstrates that BC survivors received improved cardiovascular screening and statin therapy when appropriate as compared with peers. Primary care predominantly provides cardiovascular screening and management in this population with the majority of patients seeing primary care more recently than cancer specialists.
Our study demonstrates increased use of cholesterol screening and statins in cancer survivors as compared with matched controls. Blood pressure control for individuals with a diagnosis of hypertension did not differ between cancer survivors and controls. Based on the time of data extraction, guidelines from the Eighth Joint National Committee for blood pressure control were utilized in this study.44 The finding of comparable blood pressure control in cancer survivors is a significant finding given that endocrine therapies, antiangiogenic therapies, and other cancer therapies have been associated with elevated blood pressures.45⇓–47
Previous studies regarding the receipt of preventive health screenings and in particular cholesterol screening have been limited and have had conflicting results. Synder et al conducted a longitudinal study and multi-cohort study evaluating cholesterol screening and other preventive health services in Medicare recipients compared with matched controls using claims-based data and found decreased rates of screening in cancer survivors compared with controls except when a comorbidity-based cohort analysis was conducted.48⇓–50 Other studies focused on Medicare BC survivors and cancer survivors using both claims-based and interview data have demonstrated increased preventive health services including cholesterol screening.16,39 When individual cancers types have been studied, there is variation in the receipt of recommended acute and chronic care that cancer survivors receive.50 In these studies, the frequency of cholesterol screening was suboptimal. When we examine a population of patients with an identified primary care provider with associated recent visit to their primary care provider, cholesterol screening was increased in BC survivors compared with controls. Based on our findings, we concluded that BC survivors with an identified primary care provider are more likely to received cholesterol screening and statin treatment. Although not directly evaluated in this study, we believe that this is a result of both patient and provider factors. BC survivors may be more likely to pursue recommended preventive health given previous history of surviving cancer diagnosis as a focus on improved ongoing health. Health care providers may be more likely to conduct cholesterol screening in BC survivors due to the increasing awareness of their cardiovascular risk. It would be beneficial for future qualitative work to examine the factors that contribute to this increased screening on a patient, provider, and system level.
African American women have a lower incidence of BC compared with White women; however, African American women have a higher mortality when diagnosed with BC even when matched with White women with the same stage at time of diagnosis.51,52 As BC treatment has improved and cancer survivors are having improved treatment outcomes, this has disproportionally benefited White women. In this study, we found that there were no differences between African American women and White women regarding screening. African American BC survivors were more likely to have a diagnosis of hypertension than White BC survivors, but this was consistent with the incidence in the general population.
The current study has some advantages compared with previously conducted studies. In addition to focusing on cholesterol screening, we have further included a cardiovascular risk evaluation and inclusion of statin therapy when appropriate based on risk, major cardiac event, or diagnosis of diabetes. For this reason, we have focused on a younger population of BC survivors with average age of 63 years compared with 75 years for previous studies.16,48,50 Although the benefit of statin use for primary prevention for individuals at high cardiovascular risk has been established, insufficient evidence is available for its use in individuals over the age of 75 years.53 In addition, in comparison with previously conducted studies, this study has a higher percentage of African American women. More than 42% of our sample were African American whereas these women made up 10% or less of the samples examined in previous reports.16,54
The current study has several limitations. Although the primary care practices included employed both internal and family medicine physicians and advanced practice providers, the study population was a population of BC survivors seen at a single academic institution. To further evaluate screening practices in those with a usual source of care, individuals with a primary care provider were selected for inclusion and as such the data cannot be extrapolated to those without a primary care provider. The screening rates reported are likely to be higher than for a cohort of all BC survivors. Our data are limited by information that can be extracted from the electronic health record and does not include screening or management obtained from other sources. Data including dietary habits, physical activity, aspirin use, and socioeconomic status could not be included.
BC survivors are at increased risk of CVD, for which screening and management is conducted predominantly in the primary care setting. The results of this study demonstrate that BC survivors are more likely than matched controls to be screened for CVD risk. Future research may benefit from investigation as to whether development of cardiovascular risk assessment and management guidelines that consider an individual’s cancer diagnosis and treatment history would improve cardiovascular outcomes for BC survivors. As majority of cardiovascular screening and management is conducted in the primary care setting, communication between cancer specialists and primary care regarding an individual’s treatment history and associated cardiovascular risk is essential to the care of cancer survivors.
Notes
This article was externally peer reviewed.
Conflict of interest: None.
Funding: This project was supported in part by the National Center for Advancing Translational Sciences of the National Institutes of Health under Grant Number UL1 TR001450. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
To see this article online, please go to: http://jabfm.org/content/33/6/894.full.
- Received for publication December 19, 2019.
- Revision received May 19, 2020.
- Accepted for publication May 20, 2020.




{kind=link}
{kind=link}
{kind=link}