
Article Figures & Data
Figures
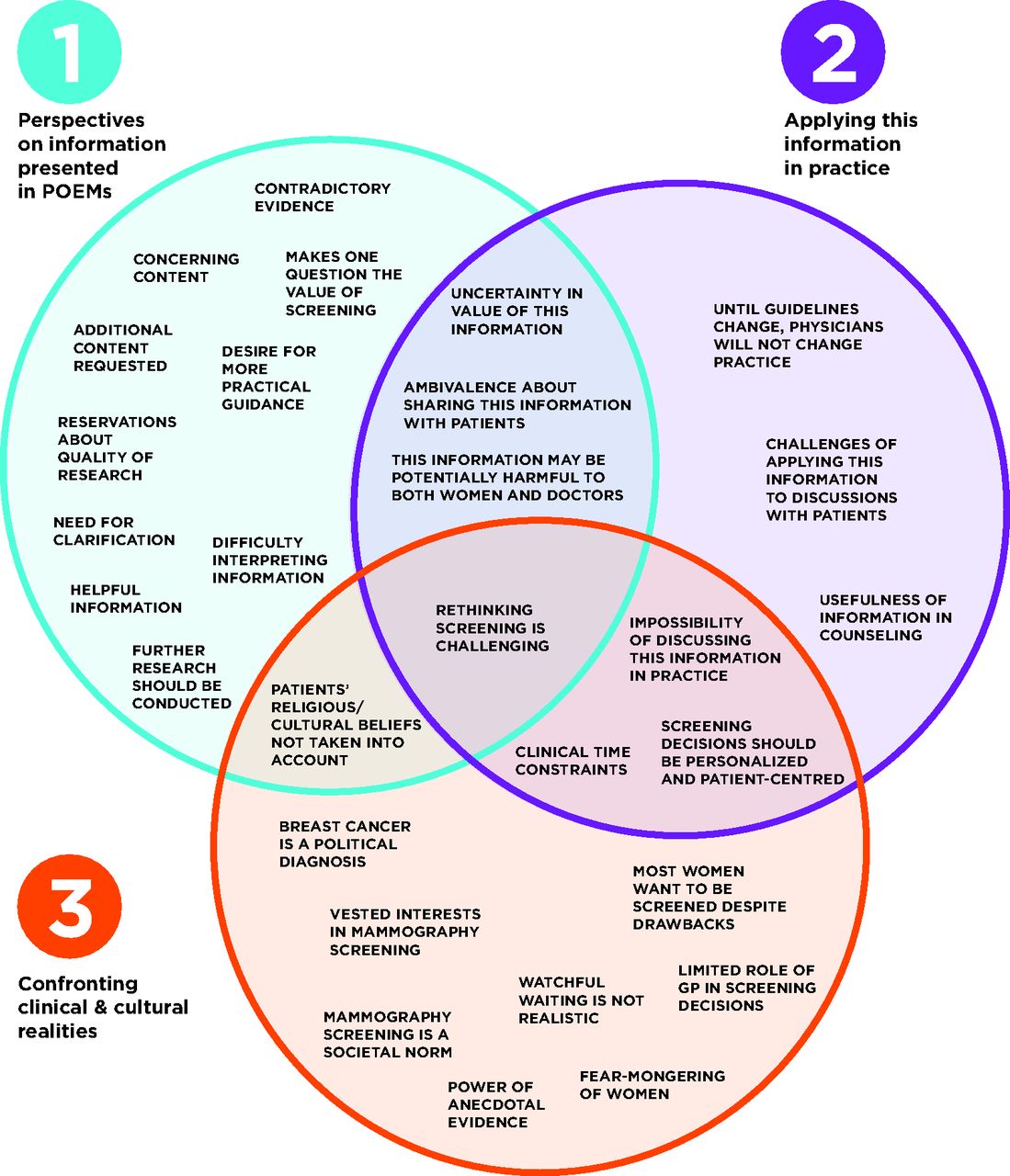
- Figure 1.
Themes and subthemes that emerged from physician comments.

Tables
Domain Question Sub-Item of Interest Q1: What is the impact of this information on you or your practice? o. I disagree with the content of this information
o. This information is potentially harmful
Q3: Will you use this information for a specific patient? If YES, then: o. As a result of this information I will manage this patient differently
o. I had several options for this patient, and I will use this information to justify a choice
o. I thought I knew what to do, and I used this information to be more certain about the management of this patient
o. I used this information to better understand a particular issue related to this patient
o. I will use this information in a discussion with this patient, or with other health professionals about this patient
o. I will use this information to persuade this patient, or to persuade other health professionals to make a change for this patient.
Q4: For this patient, do you expect any health benefits as a result of applying this information? If YES, then: o. This information will help to avoid unnecessary or inappropriate treatment, diagnostic procedures, preventative interventions or a referral, for this patient
IAM, Information Assessment Method.
- Table 2.
Key Characteristics of Four Retrieved POEMs Relevant to Mammography Screening, Decision Making, and Overdiagnosis
POEM Title and Date Study Design Publication Date Clinical Question Bottom Line 1. Overdiagnosis of breast cancer is common 2013-01-2942 Cohort (prospective) 2012 What proportion of breast cancer is overdiagnosed? In the past 30 years we have seen a large increase in the detection of early-stage cancers, but little corresponding decline in late-stage cancers. The authors conclude that approximately 1 in 4 breast cancers has been overdiagnosed, and was unlikely to have ever harmed the woman. 2. Numbers to help women understand the benefits/harms of screening mammography 2014-02-144 Special Communication 2014 What are the trade-offs of benefits and harms for women considering a mammogram to screen for breast cancer? The authors suggest that balanced discussions about the benefits and harms of screening mammography should focus not only on the possibility of breast cancer deaths avoided but also the possibility of false alarms and overdiagnosis (the detection of abnormalities that will never progress enough to cause symptoms or death during a patient’s lifetime). The numbers for women of different ages are outlined in the synopsis. Although some women are comfortable with a high rate of false positive results, some women will experience lasting consequences43 and should know the risk of harm when making the decision whether to screen. 3. Mammography doesn’t decrease cancer-related deaths long term 2014-04-1644 Randomized controlled trial (non-blinded)2014 Over the long term, does screening mammography decrease the likelihood of a woman dying of breast cancer? Over an average follow up of 22 years in almost 90,000 women, there was a clinically insignificant difference of 5 deaths due to breast cancer (500 vs 505) in women who received 5 annual screening mammograms instead of usual care. Over more than 2 decades, only 1.1% of women died of breast cancer, much lower than the 12.5% (1 in 8) often cited. 4. Mammogram decision aid slightly increases informed decisions by women 2015-08-1345 Randomized controlled trial (double-blinded)2015 Does a decision aid that incorporates data on breast cancer overdiagnosis increase informed decision making in women? Decisions aids, regardless of whether they contain information about breast cancer overdiagnosis, have a modest influence on a woman’s ability to make informed choices about screening. POEM, Patient-Oriented Evidence that Matters.
Number of Physicians Endorsing Item (%) POEM 1 POEM 2 POEM 3 POEM 4 IAM Question n = 1293 n = 1351 n = 1308 n = 1243 Q1.I disagree with the content of this information. 19 (1.5) 7 (0.5) 15 (1.15) 4 (0.3) This information is potentially harmful. 24 (1.9) 4 (0.3) 13 (1.0) 0 Q3.Will you use this information for a specific patient? 139 (10.8) 214 (15.8) 156 (11.9) 79 (6.4) Answering ‘Yes’ to Q3 enables the following sub-items: n = 139 n = 214 n = 156 n = 79 As a result of this information I will manage this patient differently. 22 (15.8) 19 (8.9) 19 (12.2) 6 (7.6) I had several options for this patient, and I will use this information to justify a choice. 33 (23.7) 50 (23.4) 44 (28.2) 19 (24.1) I thought I knew what to do, and I used this information to be more certain about the management of this patient. 18 (12.9) 33 (15.4) 24 (15.4) 16 (20.3) I used this information to better understand a particular issue related to this patient. 52 (37.4) 61 (28.5) 49 (31.4) 34 (43.0) I will use this information in a discussion with this patient, or with other health professionals about this patient. 78 (56.1) 134 (62.6) 99 (63.5) 43 (54.4) I will use this information to persuade this patient, or to persuade other health professionals to make a change for this patient. 21 (15.1) 16 (7.5) 14 (9.0) 8 (10.1) Q4. For this patient, do you expect any health benefits as a result of applying this information? 121 (87.1) 186 (86.9) 129 (82.7) 61 (77.2) Answering ‘Yes’ to Q4 enables the following sub-item: n = 121 n = 186 n = 129 n = 61 This information will help to avoid unnecessary or inappropriate treatment, diagnostic procedures, preventative interventions or a referral, for this patient. 105 (86.8) 163 (87.6) 122 (94.6) 45 (73.8) POEM, Patient-Oriented Evidence that Matters.
POEM 1 2 3 4 Number of ratings 1293 1351 1308 1243 Number of comments 29 125 93 63 POEM, Patient-Oriented Evidence that Matters.




{kind=link}