
Abstract
Background: Exponential increases in nonindicated, low-value vitamin D testing have been reported over the past 15 years. Downstream effects of such testing have not been well quantified.
Methods: The purpose of this study was to describe patterns of vitamin D testing within primary care of a large regional health system and to explore downstream health service utilization subsequent to nonindicated testing. Instances of vitamin D testing in 2015 were obtained by an electronic health record-automated search. A subset of patients for whom vitamin D testing was classified as nonindicated was identified, and vitamin D-related service utilization was tracked for 24 months.
Results: Of the 77,836 adult primary care patient records identified in 2015, vitamin D tests were conducted on 8,042 (10.3%), with 24.3% of tests yielding abnormal results. In the nonindicated test subset (n = 574), substantial clinical variability was illustrated by 85 care pathways and 26 vitamin D prescriptions. Forty-five percent of abnormal vitamin D lab tests were not followed up with repeat vitamin D tests. Vitamin D-related services (laboratory tests, imaging, and prescriptions) occurred at an average rate of 1.6 services per patient during the 24 months following nonindicated vitamin D testing. Some of these services were also classified as nonindicated.
Conclusions: Evidence of a health service cascade following nonindicated vitamin D testing exists. Opportunities for improved consistency and quality of care related to vitamin D were observed in our health system. These results may inform clinical pathways related the prevention, evaluation, and treatment of low vitamin D.
- Electronic Health Record
- Low Value Care
- Overuse
- Primary Health Care
- Quality Improvement
- Uncertainty
- 25-hydroxyvitamin D
Introduction
Over 25% ($760 to $932 billion annually) of US health care spending is considered unnecessary and wasteful.1 Low value care, which is defined as clinical services that confer minimal or no benefit or may cause harm, is a substantial component of unnecessary health care expenditures.2,3 The Choosing Wisely Campaign is an initiative aimed at reducing low value care and highlighting clinical practices inconsistent with the evidence.4,5 Initially founded in 2012 by the American Board of Internal Medicine Foundation, Choosing Wisely includes recommendations from over 80 professional medical societies.4
Three medical societies have identified a Choosing Wisely recommendation of Do not order population-based screening for vitamin D.6 This recommendation aligns with a 2014 US Preventive Services Task Force recommendation statement that advises against vitamin D screening in asymptomatic community-dwelling adults due to insufficient evidence of benefits and harms.7 The US Endocrine Society and the National Academy of Medicine (formerly known as the Institute of Medicine) also recommend against vitamin D testing in low-risk populations.8,9 Choosing Wisely and others do recognize, however, that vitamin D testing is indicated in patients at high risk for abnormal vitamin D or related complications (ie, osteoporosis or osteopenia, parathyroid or calcium-related disorder, or chronic kidney disease of ≥ stage 3) (Table 1).6,10
Indicators for Vitamin D Testing
At $100 to $300 per test, vitamin D testing is itself a low to moderately priced laboratory test.11 However, the large volume of tests regularly conducted makes vitamin D testing a significant economic investment.10,12 It has been estimated that over 1 billion vitamin D tests are ordered annually worldwide13 and that test ordering has increased substantially over the past 15 years.14⇓⇓⇓–18 Between 25% and 77% of these tests follow a pattern of nonindicated screening rather than targeted testing of high-risk patients.11,19⇓⇓–22 Six million vitamin D tests labeled as “low value” were conducted in commercial and Medicare-insured Americans in 2014, tallying over $800 million. In addition, $24 million was spent on vitamin D testing considered nonindicated just in the state of Virginia in 2016.23 Recently, insurance providers have implemented stricter guidelines on vitamin D test reimbursement.24
Along with financial burden, overuse of screening and diagnostic tests has been associated with increased risk of patient harm.25⇓⇓–28 Further research is needed to examine downstream effects and consequences of nonindicated vitamin D testing. The purpose of this study was to describe vitamin D test ordering patterns and explore downstream consequences of nonindicated vitamin D test ordering within primary care of a regional health system.
Methods
Study Design
An automated search of the electronic health record (EHR) database for a regional health system was performed to identify instances of vitamin D testing in adult, continuous care patients in 2015. Vitamin D testing was defined as a single 25-hydroxyvitamin D [25(OH)D] test. We also identified a subset of vitamin D tests that were ordered without clinical indication and tracked vitamin D-related laboratory testing, imaging services, and prescriptions incurred during the 24 months following the index vitamin D test. For the purpose of this study, nonindicated vitamin D testing was defined as vitamin D tests that do not meet Choosing Wisely criteria for indicated services (Table 1).6 This study was approved by the institutional review board of Carilion Clinic (IRB-18-274). The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement checklist for observational studies was used in the preparation of this manuscript.29
Setting
Carilion Clinic is a nonprofit comprehensive health care system that serves over 1 million patients in Southwest Virginia. Adult primary care services at Carilion Clinic are delivered by 226 family medicine clinicians and 22 internal medicine clinicians (physicians, physicians assistants, and nurse practitioners) in 54 different facilities. Epic (Epic Systems, Wisconsin, US) has served as the EHR platform for Carilion Clinic since 2008, and Quest Diagnostics (New Jersey, US) has served as the laboratory services provider for Carilion Clinic since 2014. Vitamin D test analyses are conducted using an immunoassay methodology certified by the Centers for Disease Control and Prevention Vitamin D Standardization Certification Program. Carilion Clinic assigns 30 to 100 ng/mL as the normal reference range for 25(OH)D (Table 2). Within our health system, ICD-10 codes are assigned at the time that laboratory tests are ordered.
Vitamin D Test Result Reference Range
Data Extraction
From Carilion Clinic's EHR, we identified adult patients (≥18 years of age) who received ongoing care (≥1 visit annually) from 1 or more primary care clinicians between January 1, 2013 and December 31, 2017. Data were extracted for any of these continuous primary care patients for whom an outpatient initial vitamin D test (ie, first test within 12 months) was conducted between January 1, 2015 and December 31, 2015. In addition to vitamin D test date and test results, we also extracted the following data: age, gender, race/ethnicity, body mass index (BMI), insurer, and diagnoses code(s) associated with the vitamin D test.
A subset of patients for whom the initial vitamin D test was considered nonindicated was established through the identification of patients who did not have diagnoses shown in Table 1, had no previous vitamin D test(s) documented anywhere in their history, and had not received a vitamin D prescription in the 12 months before their index vitamin D test. The following additional vitamin D-related service data documented in the 24 months subsequent to the nonindicated vitamin D test were extracted for this subset: laboratory tests [25(OH)D, 1,25(OH)2D, calcium, phosphorus, alkaline phosphatase, and parathyroid hormone (PTH)], prescriptions (vitamin D preparations >400 IU, osteoporosis medications, and calcimimetic medications), imaging services (bone mineral density), and diagnoses.
Data Analysis
Data were analyzed using IBM Statistical Package for the Social Sciences (SPSS) version 26.0 (Chicago, IL). Descriptive statistics (means, standard deviation, and frequencies) were calculated on all data. Differences between means were evaluated using the unpaired t test or one-way analysis of variance with Tukey's multiple comparisons test. For categorical data, χ2 and Fisher's exact tests were used. Multivariate linear regression analysis was used to evaluate the contribution of patient factors to vitamin D test results. Poisson regression analysis was used to evaluate the contribution of patient factors to number of services incurred.
Statistical significance was set at an α level of 0.05. Plotly R Package version 4 (Quebec, Canada) was used to create an alluvial diagram.
Results
We identified 77,836 continuously enrolled adult primary care patient records for 2015. Vitamin D tests were conducted on 8042 of these patients (10.3%). The nonindicated vitamin D test subset included 574 patients. Patients in the nonindicated vitamin D test subset were younger, more likely to be male, more likely to be commercially insured or self-pay, and less likely to be insured by Medicare compared with all patients who had vitamin D testing (Table 3).
Demographic and Clinical Characteristics of Patients Who Had Vitamin D Testing in 2015
Vitamin D Test Results
Vitamin D test results were similar among the nonindicated and indicated vitamin D test groups (Table 4), but the nonindicated vitamin D test subset included a greater proportion of abnormal test results (39.5%) than those who had indicated tests (24.3%) (P < .001) (Table 4). Vitamin D test results did not differ by patient age. White patients had 18% higher vitamin D test results than black or African American, Asian, and Hispanic patients (P < .001). Patients with underweight (<18.5 kg/m2) or normal BMI (18.5 to 25 kg/m2) had higher (17% and 15%, respectively) vitamin D test results than patients with a BMI of >25 kg/m2 (P < .001) as did those with commercial insurance or self-pay status compared with other insurers (Medicare, Medicaid, and other) (P < .001).
Results of Initial Vitamin D Tests in Primary Care Patients in 2015
Downstream Services following Nonindicated Vitamin D Testing
A total of 4437 vitamin D-relevant laboratory, prescription, and imaging services were ordered for patients who had nonindicated vitamin D testing over the 24-month observation period. Because the volume of calcium (n = 2184) and alkaline phosphatase (n = 1412) tests ordered was disproportionate to other laboratory tests and because they are part of common test panels (basic metabolic panel and comprehensive metabolic panel, respectively), they were omitted from primary analyses. Thus, we observed a total of 841 vitamin D-relevant laboratory (n = 466), prescription (n = 344), and imaging (n = 31) services during the 24 months following a nonindicated vitamin D test. The provision of these services followed 85 different clinical pathways (ie, steps and timing of vitamin D-related care; data not shown).
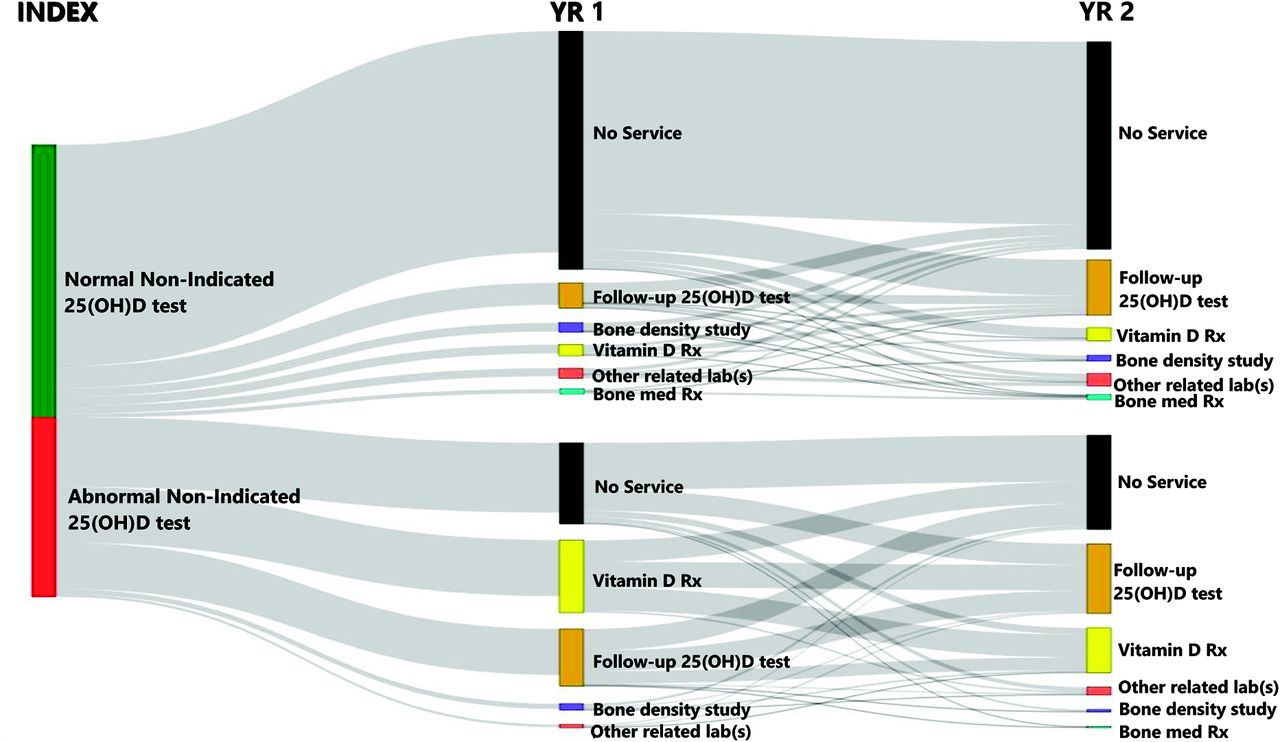
Based on Poisson analysis, gender, race, age, insurer, month of test, and index vitamin D test result category (deficient, insufficient, normal, and high) did not predict the number of services incurred. Figure 1 shows the flow of vitamin D-relevant services observed in the nonindicated vitamin D test subset based on results of the index vitamin D test.

Vitamin D-relevant services incurred in the 24 months following a nonindicated vitamin D test. An alluvial diagram showing the flow of vitamin D-relevant service utilization for 2 years following a nonindicated vitamin D test in 2015.
Laboratory Testing Subsequent to Nonindicated Vitamin D Testing
Follow-up vitamin D testing was conducted in 200 patients (34.8%) in the nonindicated vitamin D test subset. The time lapse between initial and follow-up test(s) varied broadly (2 to 718 days), but 19 (5.9%) follow-up vitamin D tests took place sooner than 8 weeks after the nonindicated test. The number of follow-up tests conducted over 24 months was 1 (129 patients), 2 (37 patients), 3 (23 patients), 4 (9 patients), 5 (1 patient), or 7 (1 patient). No follow-up vitamin D testing was conducted in 61.7% of patients with abnormal vitamin D test results. Of the 320 total follow-up vitamin D tests conducted, 194 (60.6%) occurred in patients with normal vitamin D test results in their most recent vitamin D test. Patients with insufficient initial vitamin D test results had a 2-fold greater likelihood of follow-up vitamin D tests than patients with deficient test results and a 5-fold greater likelihood than those with normal test results (P = .022).
Other vitamin D-relevant laboratory tests included PTH (n = 281), phosphorus (n = 123), and 1,25(OH)2D (n = 62). Abnormal test results were observed with 33.3% (PTH), 23.6% (phosphorus), and 20.0% [1,25(OH)2D] of these tests. There was no relationship between initial vitamin D test result and likelihood of having a 1,25(OH)2D test. Most 1,25(OH)2D tests (92%) were conducted in patients who did not have abnormal PTH or elevated calcium test results.
Prescriptions Subsequent to Nonindicated Vitamin D Testing
A total of 275 prescriptions for oral vitamin D supplements were provided to 112 (20%) patients. Nine different vitamin D prescriptions were provided in a total of 26 different treatment regimens (Table 5). Seventy-three (65%) prescriptions were for ergocalciferol (vitamin D2) and 39 (35%) were for cholecalciferol (vitamin D3). There was no relationship between vitamin D test result and type or dosage of vitamin D prescribed. For example, there were 11 25(OH)D test results of <12 ng/mL. The following vitamin D prescriptions were provided to these patients: high-dose vitamin D2 (n = 2), high-dose vitamin D3 (n = 2), moderate-dose vitamin D3 (n = 2), and no vitamin D prescription (n = 5).
Vitamin D Prescriptions Provided to the Subset of Patients Who Had Nonindicated Index Vitamin D Tests in 2015
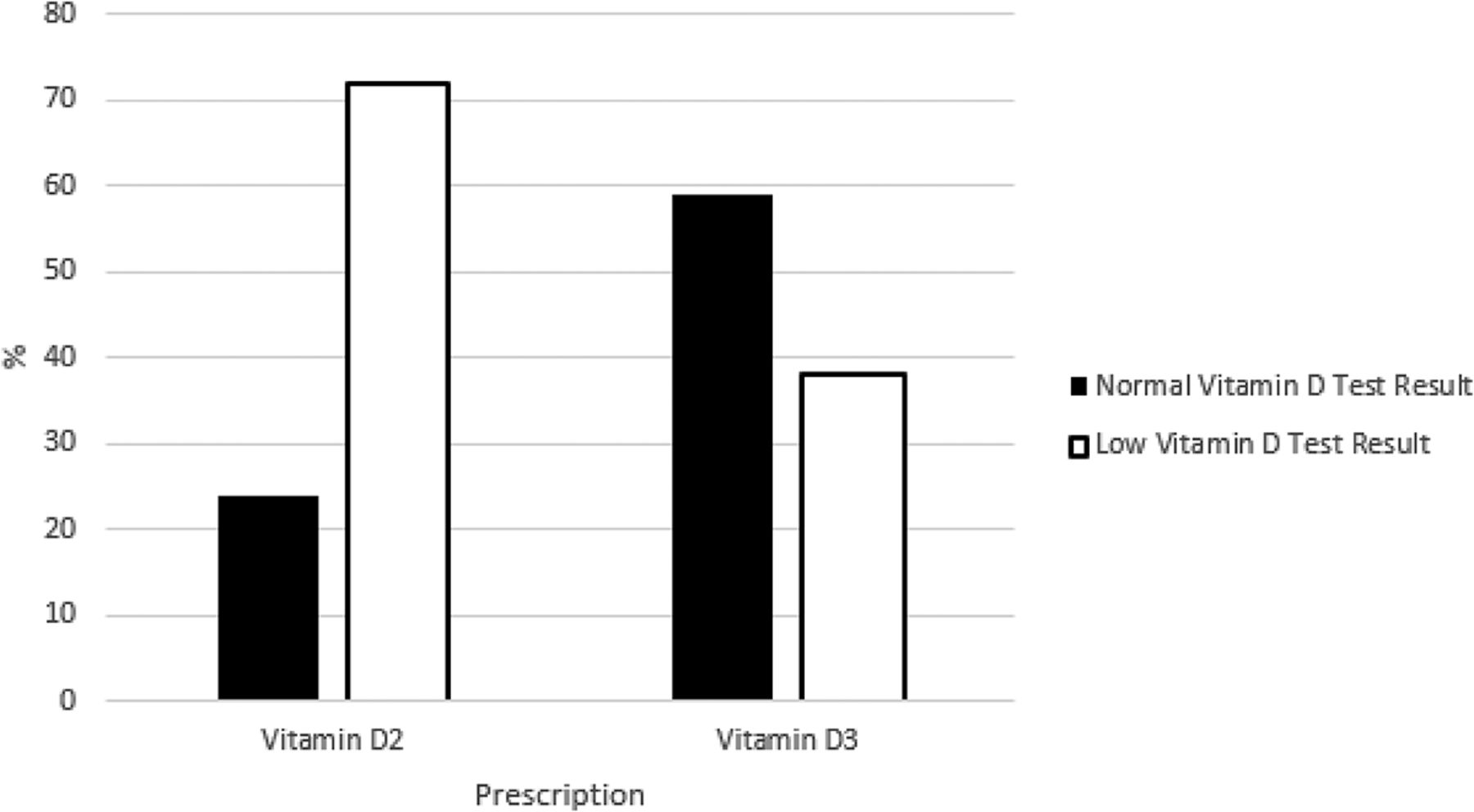
Of the 112 patients who received a vitamin D prescription, 82 (73%) had at least 1 follow-up vitamin D test. The type of vitamin D prescription (vitamin D2 or D3) was a significant predictor of change in vitamin D test result (R2= 0.854, P < .001) (Figure 2). Patients prescribed vitamin D2 experienced a 68% decline in vitamin D test results (range, −710% to 48% change), whereas patients prescribed vitamin D3 experienced a 43% improvement in vitamin D test results (range, −180% to 430%). There was no significant interaction between type of prescription and time. Half (50%) of patients with low initial vitamin D test results achieved normal test results during the 24-month observation. The likelihood of achieving normal vitamin D results was significantly higher in patients prescribed moderate-dose (1000 to 2000 IU/day) or high-dose (≥2000 IU/day) vitamin D3 than in those prescribed low-dose (400 to 1000 IU/day) vitamin D3 (P = .030). There were no high (>100 ng/mL) vitamin D test results following the provision of vitamin D prescriptions.

Proportion of low and normal vitamin D test results following vitamin D2 and vitamin D3 prescriptions *The highest vitamin D test result attained during the 24 months following a nonindicated index vitamin D test.
Calcium (without vitamin D) was prescribed to 21 patients (5%), and bone resorption inhibitors were prescribed to 15 patients (3%) who had nonindicated vitamin D tests. Calcimimetic medications (eg, cinacalcet) were not prescribed to any patients in the subset.
Imaging Subsequent to Nonindicated Vitamin D Testing
Vitamin D-related imaging studies were conducted on 30 patients (5%) during the 24 months following nonindicated vitamin D testing. One patient underwent 2 imaging studies, whereas the remainder had a single imaging study. The majority of imaging studies (83%) consisted of multisite dual energy radiograph absorptiometry (DXA), and the remainder consisted of axial-only DXA.
Diagnoses Subsequent to Nonindicated Vitamin D Testing
During the 24 months following a nonindicated vitamin D test, a new diagnosis of vitamin D deficiency or vitamin D insufficiency was documented for 356 patients (62%). Of these patients, 107 (21%) had only normal vitamin D test results during the 24-month observation period. Other vitamin D-related diagnoses documented were osteoporosis (8%), osteopenia (1%), osteoporotic fracture (1%), pathologic fracture (0.5%), stress fracture (0.5%), inflammatory bowel disease (5%), malabsorption (2%), and parathyroid/calcium/phosphate disorder (1%). There was no difference in the likelihood of receiving these diagnoses based on initial vitamin D status.
Discussion
Amid controversy in vitamin D research and clinical guidelines, vitamin D testing and prescribing have increased substantially in the past 15 years.10 Nonindicated testing has been shown to represent a substantial proportion of this testing and is considered a source of low value health care.6 One purpose of this study was to explore downstream consequences of nonindicated vitamin D testing within primary care of our Southwest Virginia health system. Overall, we observed inconsistency in care, opportunities to improve care, and evidence of a low-value service cascade during the 24 months following a nonindicated vitamin D test.
Patterns of Care
Inconsistency in vitamin D-related care has been reported previously30⇓–32 and existed in the current study. Numerous care pathways and vitamin D treatment regimens were observed. In addition, the number of follow-up vitamin D tests, time between vitamin D tests, and the 25(OH)D concentration associated with a vitamin D deficiency diagnosis were highly variable.
We observed the highest inconsistency in care following insufficient vitamin D test results. Defined as 25(OH)D of 20 to 29.9 ng/mL in the present study (Table 2), insufficient test results were associated with the highest rate of follow-up vitamin D tests (double that of low test results). However, few patients with insufficient test results were given vitamin D prescriptions. It is possible that over-the-counter vitamin D supplements were recommended for patients with insufficient test results, but because only one-third of these patients showed improved vitamin D test results within the 24-month observation period, issues of documentation, adherence, and effectiveness are all possible. Of note, the definition of vitamin D insufficiency is controversial and not even recognized by all practice guidelines. For instance, the Endocrine Society recognizes 25(OH)D of 20 to 29.9 ng/mL as insufficient,8 but the National Academy of Medicine does not recognize a vitamin D insufficient category and states that 25(OH)D of 20 ng/mL meets the needs of 97.5% of the population.9 It is also important to consider that many professional organizations have highly variable recommendations related to indicators for vitamin D testing,10 which is challenging for clinicians to navigate.33⇓–35 We observed higher average vitamin D test results (41.1 ± 9.3 ng/mL) and a lower prevalence of severe vitamin D deficiency (<1%) than previous reports.36⇓–38 As there are numerous factors that influence vitamin D status, these differences could be based on variability in geography, age, race, adiposity, medication use, socioeconomic status, overall health status, or other factors. For example, our cohort included almost exclusively white patients (who typically have higher vitamin D than individuals with darker skin pigmentation) and patients with lower BMI than other cited studies (higher BMI is associated with lower vitamin D).24,25,39,40
A few differences in characteristics of patients who had nonindicated initial vitamin D tests compared with those who had indicated vitamin D tests were identified. The difference in age (nonindicated test patients were younger and less likely to be insured by Medicare) may be due to the exclusion of patients who were recorded as already taking vitamin D supplements. More than 50% of Americans over 60 years of age have been reported to take vitamin D supplements.41 The greater proportion of self-pay and commercially insured patients in the nonindicated test cohort is likely a factor of this younger age-group that is less likely to be insured by Medicare. The higher rate of abnormal vitamin D test results in the nonindicated test subset may reflect clinicians' clinical instinct related to the possibility of low vitamin D. However, it is unclear if identification and treatment of low vitamin D is clinically valuable in patients without specific indications.7
Quality of Care
We identified some potential opportunities to improve quality of care related to vitamin D. For example, nearly half of low vitamin D test results were not followed up by repeat vitamin D testing (Figure 1). Monitoring 25(OH)D following low test results and at least 12 weeks of treatment is a common practice recommendation.8,42,43 In addition, two-thirds of vitamin D prescriptions were for vitamin D2 rather than vitamin D3, which has greater bioavailability than vitamin D2 and is more effective in raising 25(OH)D.44,45 As this finding is somewhat recent, it is not reflected in major vitamin D guidelines, which describe both forms as suitable treatment options.8,9
One-fifth of patients given a new diagnosis of vitamin D deficiency or insufficiency did not have low vitamin D test results. This may reflect the existing controversy around 25(OH)D values.33 Clinicians may have also assigned such a diagnosis to obtain insurance reimbursement for tests, which has been reported previously.34
Health Services Cascade
Abnormal test results have been described as triggering a cascade process by which a number of referrals and additional investigations arise.46 The volume of vitamin D-relevant services (an average of 1.6 services per patient) that followed a nonindicated vitamin D test suggests that a similar cascade occurs within our health system. Another consideration is that, during 2015, our health system had a limited endocrinology service and did not have a nephrology service, so referrals for these services were made outside of our health system. Thus, we are likely missing vitamin D-relevant health services that were not documented in our EHR.
Some of the services provided subsequent to a nonindicated vitamin D test can themselves be described as low value. For example, more than half of the 320 follow-up tests ordered (up to 7 follow-up tests in 24 months) did not meet our criteria (based on Choosing Wisely) for an indicated vitamin D test. In addition, the majority of 1,25(OH)2D tests were conducted in patients who did not fulfill the Choosing Wisely indications for this test (hypercalcemia and/or abnormal PTH).4
The financial impact of nonindicated vitamin D testing can be significant. Based on the charge for an outpatient vitamin D test at Carilion Clinic (∼$278 in 2015), the sum of all vitamin D charges for tests ordered by primary care clinicians in this health system in 2015 is estimated at $2,946,800. Over $240,000 was charged for vitamin D testing within the nonindicated test subset. Downstream health services and associated resources for these nonindicated tests may result in additional financial burden. In addition, the overall culture of low-value care is in itself considered harmful. Consequences such as increased false-positive test results, enhanced health risk related to follow-up services, emotional impact to patients, increased resources required to administer services, and decreased opportunity for higher value care have been observed following low-value health services.26,29
A strength of this study is the use of EHR data to explore downstream impacts of a common nonindicated laboratory test within a large health system, similar to that which has been performed with other low-value care services.47,48 We are not aware of other published studies that have examined downstream consequences of low-value vitamin D tests. Although individual chart review was not performed in this study, Isaac et al.40 recently observed only minor differences in low-value care services identified via automated EHR search and individual chart review.
We acknowledge some limitations in the current study. By nature, EHR research makes assumptions about clinician behavior without necessarily knowing intent. To that end, our results provide a broad description of health service patterns without consideration of details that may have factored into clinician decisions and behaviors. Some tests that we classified as nonindicated may actually have been indicated, and vice versa. We were also unable to account for over-the-counter vitamin D supplements (unless reported in patients' medication list), diet, and sun exposure. Finally, we acknowledge that service chronology does not necessarily reflect downstream effects but instead interprets the high volume of vitamin D-relevant services as suggestive of a causal association. Overall, our results provide one of the first attempts to capture downstream health service use following nonindicated vitamin D testing. The broad patterns we observed generate hypotheses for future investigations.
Conclusions
In 2015, vitamin D tests were ordered for 10% of adult primary care patients within our Southwest Virginia health system, with approximately one-quarter yielding abnormal results. In a subset of these patients who had nonindicated vitamin D tests, there seems to be high variability in care pathways and some opportunities to improve care quality. We also observed evidence of a low-value service cascade during the 24 months following a nonindicated vitamin D test. Taken together, these results provide insight into primary care clinicians' practice patterns in light of evolving research and conflicting guidelines related to the clinical management of vitamin D status. Possible interventions to improve care and reduce inconsistency related to vitamin D services could include clinician education and feedback, development of clinical pathways related to the identification and treatment of vitamin D-related abnormalities, modifications to EHR default settings and prompts, and patient education. Further research on the downstream impacts of nonindicated vitamin D testing is needed.
Notes
This article was externally peer reviewed.
Conflicts of interest: The authors have no conflicting or competing interests to disclose.
Funding: The project was supported by the Center for Transformative Research on Health Behaviors, Fralin Biomedical Research Institute at Virginia Tech Carilion, Roanoke, VA.
To see this article online, please go to: http://jabfm.org/content/33/4/569.full.
- Received for publication January 6, 2020.
- Revision received April 3, 2020.
- Accepted for publication April 8, 2020.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Reduire les dosages systematiques inutiles de la vitamine D
- Reduce unnecessary routine vitamin D testing
- Health, financial and environmental impacts of unnecessary vitamin D testing: a triple bottom line assessment adapted for healthcare
- Do not routinely test for vitamin D
- Retrieving Family Medicine's Lost Literature: The Journal of Family Practice 1974-1999 Archive
- Medications, Medicating, and Medicated--When, Where, and How--Opioids and Others