
Article Figures & Data
Figures
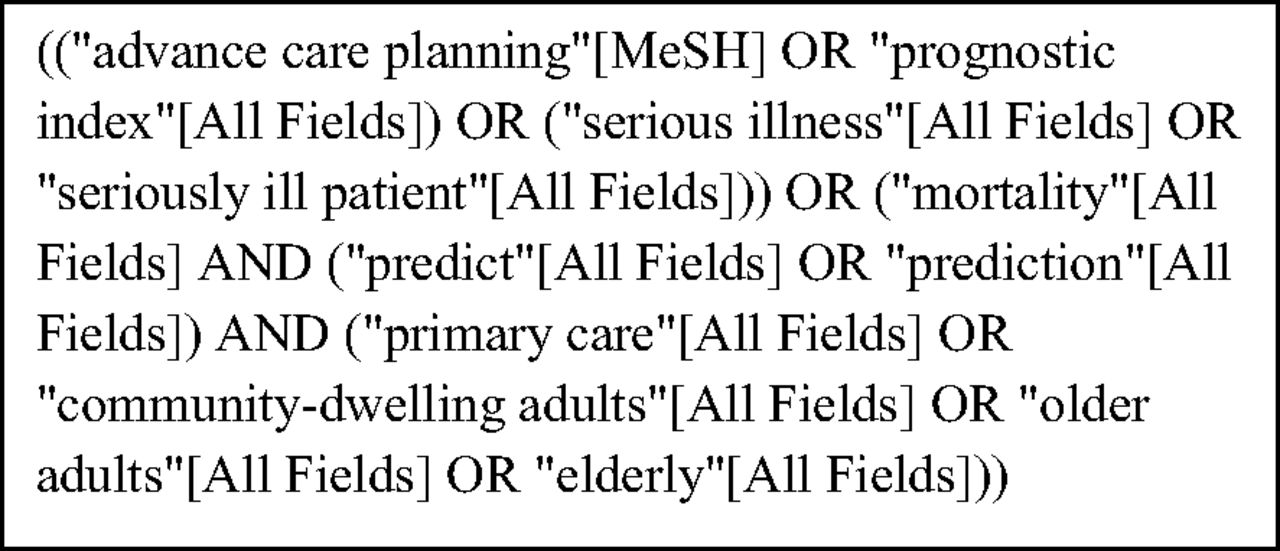
- Figure 1.
Final Search Query as displayed on PubMed.
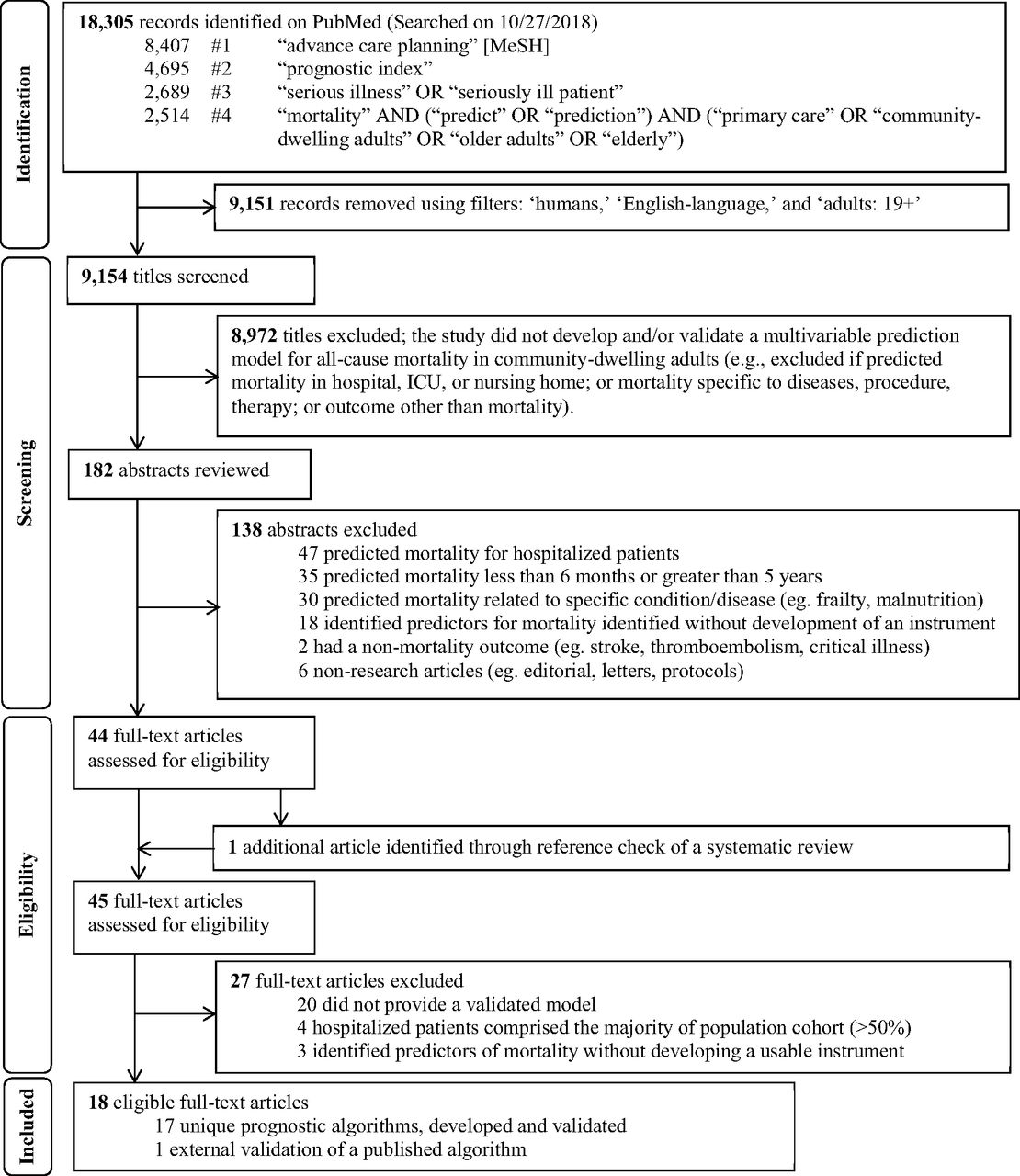
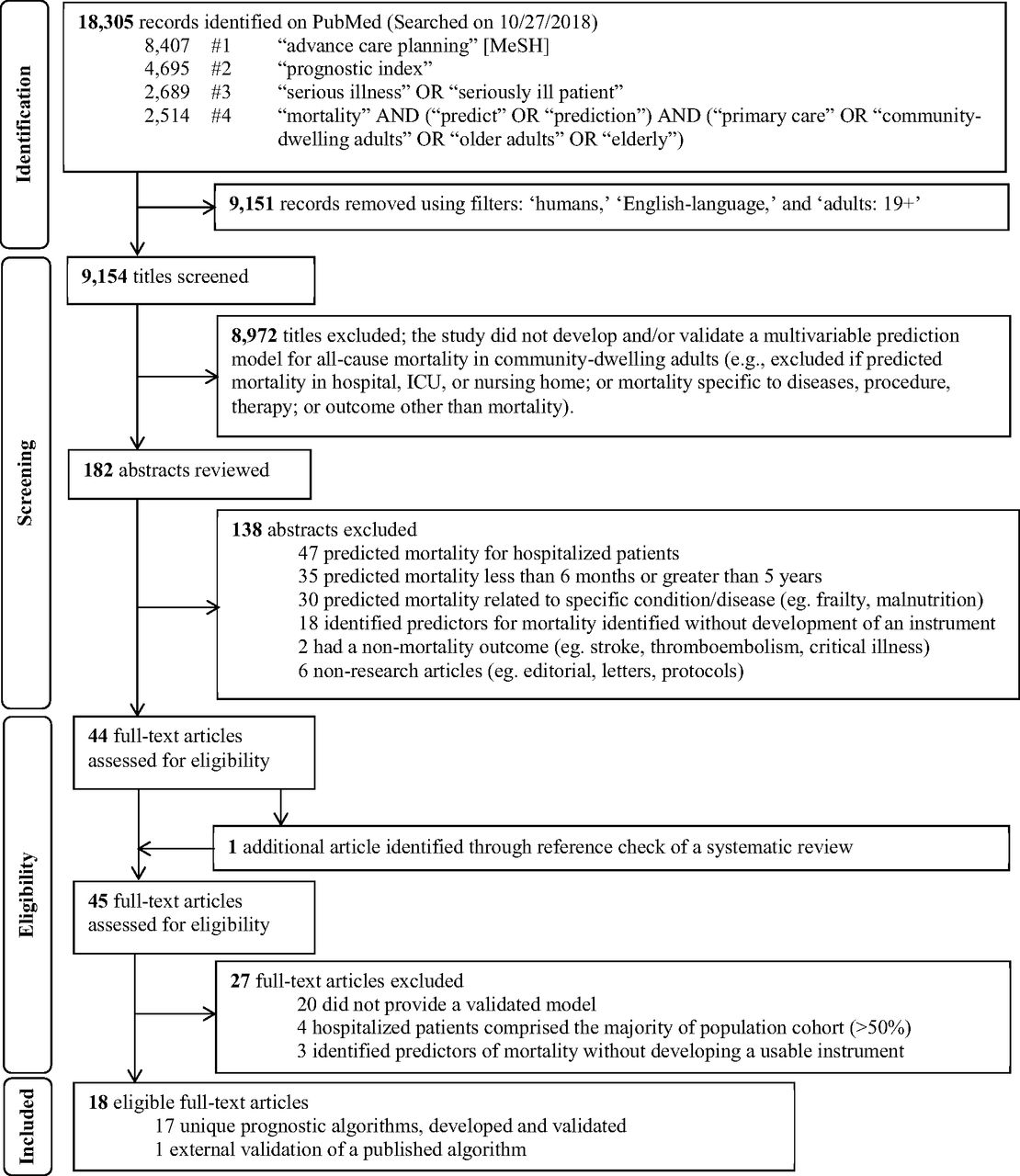
- Figure 2.
Flow diagram of study selection process to identify potentially useful prognostic indices in the primary care setting to help initiate advance care planning, adapted from the PRISMA statement.24 Abbreviations: MeSH, Medical Subject Headings; ICU, intensive care unit

Tables
n % Time Frame for Mortality 6 month20,21 1 5.9 1 year22–26 5 29.4 15 month27 1 5.9 2 year28 1 5.9 3 year29,30 2 11.7 4 year31 1 5.9 5 year32–37 6 35.3 Country United States20,21,25,26,28,30,31,34–37 10 58.8 United Kingdom22,23,33 3 17.6 Italy24,27 2 11.8 Russia29 1 5.9 South Korea32 1 5.9 C-statistics 0.50 to 0.59 (poor) 0 0 0.60 to 0.69 (moderate)29,30 2 11.7 0.70 to 0.79 (good)22,23,25,31–34,38 8 47.1 0.80 to 0.89 (very good)20,21,24,26–28,36,37 7 41.2 0.90 to 1.00 (excellent) 0 0 Calibration Well calibrated 13 76.5 <10% Difference22,24,26–28,30,31,34,35,37 10 58.8 Hosmer-Lemeshow P > .0533,36 2 11.8 Cox calibration regression25 (perfect calibration: α = 0, β = 1) 1 5.9 Poorly calibrated (>10% difference)32 1 5.9 Calibration curve only20,21 1 5.9 Not reported23,29 2 11.8 Usability† Clinically usable22,26–28,30,31,33,34,36,37 10 58.8 Not usable20,21,23–25,29,32,35 7 41.2 - Table 3.
Evaluation of Prognostic Indices according to Usability and Time Frame of Mortality Outcome
Reference by Tool Usability Population (Country) Outcome Where to Find Risk Tool and Scoring Variables Included in the Prognostic Index* Clinically Usable† Hippisley-Cox and Coupland (2017)22 Primary care patients aged 65 or older (England) 1-year all-cause mortality Instrument and scoring information not found in article.
QMortality−2017 risk calculator (https://qmortality.org/, accessed April 30, 2019)Demographics: age, ethnic group
Medications: antipsychotics, corticosteroids
Social history: alcohol intake, smoking status, living in a care home
Vital signs/labs: abnormal liver function test result, anemia, body mass index, high platelet count
Medical diagnosis: asthma or chronic obstructive pulmonary disease, atrial fibrillation, cancer, cardiovascular disease, chronic kidney disease, chronic liver disease or pancreatitis, congestive heart failure, dementia, diabetes type 1, diabetes type 2, epilepsy, learning disability, leg ulcer, Parkinson’s disease, rheumatoid arthritis, venous thromboembolism
Functional measures: Townsend deprivation score, poor mobility
Other: unplanned hospital admissions in the past 12 months, visits to a general practitioner in the past 12 months with either appetite loss, unexplained weight loss, or dyspneaGagne et al. (2011)26 Medicare enrollees aged 65 years or older (United States) 1-year all-cause mortality Instrument is presented in Table 3 and how to interpret score in bottom panel Figure 2.26
Gagne Index (https://eprognosis.ucsf.edu/gagne.php, accessed April 30, 2019)Medical diagnosis: alcohol abuse, deficiency anemia, any tumor, cardiac arrhythmias, chronic pulmonary disease, coagulopathy, complicated diabetes, congestive heart failure, dementia, fluid and electrolyte disorders, hemiplegia, HIV/AIDS, hypertension, liver disease, metastatic cancer, peripheral vascular disorder, psychosis, pulmonary circulation disorders, renal failure, weight loss Mazzaglia et al. (2007)27 Community-dwelling adults aged 65 years and older (Italy) 15-month all-cause mortality Instrument and how to interpret score are partially available in the article (Table 2 and Figure 1A).27 Authors do not state how to score the 7-item screening test (p. 1956).
Mazzaglia Index (https://eprognosis.ucsf.edu/mazzaglia.php, accessed April 30, 2019)Demographics: age, sex
Medications: ≥5 prescription medications
Functional measures: positive responses to a screening test45 (need help in performing basic ADL, need help in performing IADL, poor vision, poor hearing, weight loss, use of homecare services, and self-perceived inadequacy of income)
Other: hospitalization in the previous 6 monthsCarey et al. (2004)28 Frail community-dwelling adults aged 70 years and older (United States) 2-year all-cause mortality Instrument in Table 3 and interpretation of scoring in Table 4.28 Carey 2 Year Index (https://eprognosis.ucsf.edu/carey2.php, accessed April 30, 2019) Demographics: age, sex
Functional measures: dependence in bathing, dependence in shopping, difficulty walking several blocks, difficulty pulling/pushing heavy objectsCarey et al. (2008)30 Community-living patients aged 75 years and older enrolled in the Program of All-Inclusive Care for the Elderly (United States) 1-, 2-, and 3-year all-cause mortality Instrument in Table 3 and interpretation of scoring in Table 4.30 Carey 3 index available online (https://eprognosis.ucsf.edu/carey3.php, accessed April 30, 2019) Demographics: age, male sex
Medical diagnosis: congestive heart failure, chronic obstructive pulmonary disease, malignant neoplasm, renal failure or insufficiency
Functional measures: dependence in toileting, dependence in dressingLee et al. (2006)31 Community-dwelling adults aged 50 years and older (United States) 4-year all-cause mortality Instrument available in the article (Box on p. 807), score interpretation Table 4.31
Calculator online (https://eprognosis.ucsf.edu/lee.php, accessed April 30, 2019)Demographics: age, male sex
Social history: current smoker
Vital signs/labs: BMI < 25
Medical diagnosis: diabetes mellitus, cancer, lung disease, heart failure,
Functional measures: bathing, managing finances, walking several blocks, pushing/pulling heavy objectsGanna & Ingelsson (2015)33 Community-based participants aged 40 to 70 years (United Kingdom) 5-year all-cause mortality Instrument available online, but not in the article. (https://www.ubble.co.uk/risk-calculator/, accessed April 30, 2019) Women
Demographics: age, gender
Social history: financial assistance, smoking history
Medical diagnosis: cancer
Functional measures: disability or infirmity, usual walking pace
Other: number of live births, presence of long-standing illness, self-rated overall health, serious life events in the past 2 years, visit with a general practitioner for nerves, anxiety, tension or depression
Men
Demographics: age, gender
Social history: financial assistance, number of vehicles owned in a household, number of people living in house, relatedness of people living in house, smoking history
Medical diagnosis: diabetes, cancer, history of heart attack, angina, stroke, or high blood pressure
Functional measures: usual walking pace
Others: self-rated overall health, serious life events in the past 2 yearsMathias et al. (2013)34 Outpatients aged 50 years and older (United States) 5-year all-cause mortality Instrument available online, but not in the article. (http://info.eecs.northwestern.edu/FiveYearLifeExpectancyCalculator, accessed September 2019) Demographics: age, sex
Medications: digoxin prescription, loop diuretic prescription
Vital signs/labs: mean diastolic blood pressure, albumin—mean, median, standard deviation for the prior year, creatinine—mean, median, standard deviation for the prior year
Medical diagnosis: any vascular disease, heart failure, hypertension, chronic kidney disease, diabetes mellitus, dementia, HIV, anemia, any cancer, any liver disease
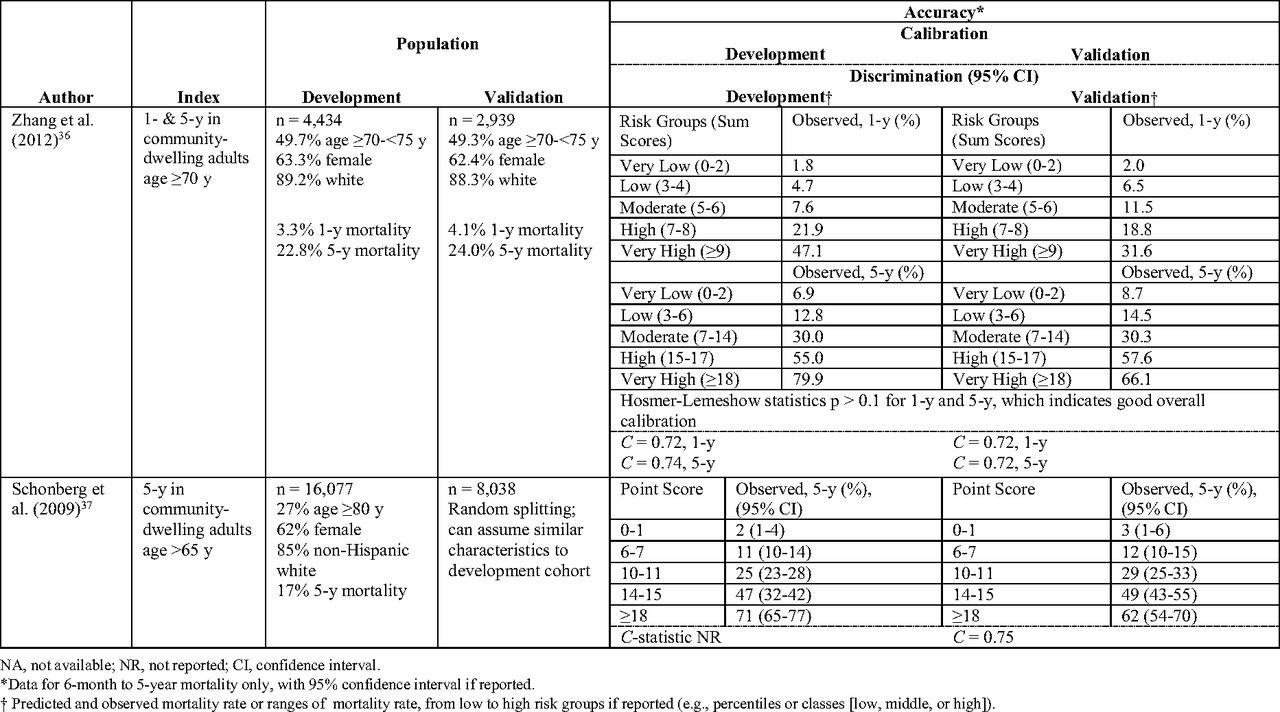
Functional measures: number of visits to primary care provider in the year before the index visit, number of hospitalizations 0 to 1 year prior, number of hospitalizations 1 to 2 years priorZhang et al. (2012)36 Community-dwelling elderly population aged 70 years and older (United States) 1- and 5-year all-cause mortality Instrument and scoring available in the article (Figures 1 and 2).36 1-year
Demographics: age, gender
Medical diagnosis: coronary artery disease
Functional measures: IADL stage
5-year
Demographics: age, gender
Medical diagnosis: cancer, coronary artery disease, diabetes, other heart disease
Functional measures: IADL stage
Other: self-rated health statusSchonberg et al. (2009)37 Community-dwelling adults aged 65 and older (United States) 5-year all-cause mortality Instrument available in the article (Table 2) and scoring in Table 3.37
Available online (https://eprognosis.ucsf.edu/leeschonberg.php, accessed April 30, 2019)Demographics: age, male sex
Social history: smoking status
Vital signs/labs: body mass index < 25
Medical diagnosis: cancer, emphysema/chronic bronchitis, diabetes mellitus
Functional measures: needs help of other persons handling routine needs, difficulty walking
Others: overnight hospitalizations in past year, perceived healthNot usable‡ Duarte et al. (2015)21 Primary and tertiary care patients aged 65 years and older (United States) 6-month all-cause mortality Instrument available in the Appendix (self-reported patient questionnaire)21; scoring not shown. Demographics: age, sex
Social history: proxy status, smoking status
Medical diagnosis: any cancer, congestive heart failure, chronic obstructive pulmonary disease
Functional measures: activities of daily living, health-related quality of lifeHan et al. (2012)20 Medicare Health Outcomes Survey respondents aged 65 years or older (United States) 6-month all-cause mortality Not in article or online. See Duarte et. al (2015)21 Crooks et al. (2016)23 Primary and secondary care patients aged 20 years and older (England) 1-year all-cause mortality Not in article or online. Social history: alcohol or illegal drug use
Medical diagnosis: burns, chromosomal anomalies, cerebrovascular disease, chronic obstructive pulmonary disease, cirrhosis, dementia, diabetes, epilepsy, esophageal, heart conduction disorders, heart failure, interstitial lung disease, liver disease, lung disease due to external agents, malignancy of respiratory tract and intrathoracic organs, malignancy of lymphatic and hematopoietic tissue, metastases, neoplasm histology, nephritis, nephrosis and nephrotic syndrome, nondeficiency and nonhemolytic anemias, nonmalignant white cell, nonorganic psychoses, other central nervous system disorders, platelet and splenic disorders, paralysis, Parkinson’s disease, spinal disease, peripheral vascular disease, pleural disease, stomach and duodenal diseasesPilotto et al. (2013)24 Community-dwelling adults aged 65 years and older (Italy) 1-year all-cause mortality A link to download free software program in Italian available in the article but must know Italian.
(http://www.operapadrepio.it/impi/svamasetup.exe, accessed April 2019)Demographics: age, sex
Social history: nursing care needs, social support network
Functional measures: Barthel Index (activity of daily living and mobility)
Others: Short Portable Mental Status Questionnaire, Exton-Smith Scale for pressure ulcerWang et al. (2013)25 Primary care patients of the Veterans Health Administration aged 18 to 110 years (United States) 1-year all-cause mortality Not in article or online. Demographics: age, sex
Medications: alpha-blockers, Antidepressants, antiplatelet, angiotensin converting enzyme inhibitor/angiotensin receptor blocker, anticholinergics, antipsychotics, benzodiazepines, beta-agonists, beta-blockers, bumetanide, calcium channel blockers, digoxin, furosemide, HMG-CoA inhibitors, other hypertension drugs, insulin, metformin, metolazone, nitrate long lasting, nitrate short lasting, opioid narcotics, nonsteroidal antiinflammatory drug, nonstatin lipid lowering agents, thiazolidinediones, potassium-sparing diuretic, oral steroids, sulfonylureas, diuretic combinations, torsemide, warfarin
Social history: substance abuse
Vital signs/labs: albumin, blood pressure (diastolic), blood pressure (systolic), blood urea nitrogen, BMI, creatinine, diastolic blood pressure, systolic blood pressure, heart rate, respiration, potassium, white blood cell count
Medical diagnosis: acute myocardial infarction, old myocardial infarction, unstable angina, stroke, hemiplegia, Atherosclerosis, depression, heart failure, respiratory failure, valvular heart disease, diabetes, hypertension, chronic obstructive pulmonary disease, pneumonia, peripheral vascular disease, metastatic cancer, psychotic disorder, liver disease, atrial fibrillation, post-traumatic stress disorder, mental disorder
Other: malnutrition, function disease, trauma, coronary artery bypass graft surgery, enrollment priority group 1 to 8, Deyo-Charlson index, emergency room visits in the past year, cardiology visit in the past year, service connection ≥50%, number of providers, primary care visits in the past year, phone visits in the past year, other nonface visits in the past year, outpatient visits in the past year, mental health hospitalization in the past year, all hospitalization, number of medication refillsTurusheva et al. (2017)29 Community-dwelling adults aged 65 years and older (Russia) 3-year all-cause mortality Instrument in Box 1.29
Interpretation unclear.Model 1
Demographics: age, male sex
Vital signs/labs: anemia, forced expiratory volume in 1 second/Height3, mid-arm muscle area
Functional measures: Short physical performance battery
Model 2
Demographics: age, male sex
Vital signs/lab: brain natriuretic peptide, anemia, C-Reactive Protein, mid-arm muscle area, forced expiratory volume in 1 second/Height3
Functional measures: Short physical performance batteryJung et al. (2016)32 Community-dwelling adults aged 65 years and older (South Korea) 3- and 5-year all-cause mortality Application for mobile devices is available for download in Korean (personal communication with authors). Demographics: age, gender
Functional measures: activities of daily living, instrumental activities of daily living
Other: Charlson Comorbidity Index or Cumulative Illness Rating Scale for Geriatrics, Korean version of the Geriatric Depression Scale, Korean Mini-Mental State Examination, Mini Nutritional Assessment or Nutrition Screening InitiativeTan et al. (2013)35 Medicare beneficiaries aged 66 to 90 years (United States) 1- and 5-year all-cause mortality Not in article or online. Demographics: age
Social history: alcohol abuse, drug abuse
Medical diagnosis: acquired immunodeficiency syndrome, cardiac arrhythmia, chronic pulmonary disease, chronic blood loss anemia, coagulopathy, congestive heart failure, deficiency anemia, depression, diabetes without chronic complications, diabetes with chronic complications, fluid and electrolyte disorders, hypertension (uncomplicated), hypertension (complicated), hypothyroidism, liver disease, lymphoma, metastatic cancer, neurological disorders other than paralysis, obesity, paralysis, peptic ulcer disease excluding bleeding, peripheral vascular disease, psychoses, pulmonary circulation disease, renal failure, rheumatoid arthritis/collagen vascular disease, solid tumor without metastasis, valvular disease, weight lossBMI, body mass index; HMG-CoA, β-hydroxy β-methylglutaryl-CoA. ADL, activities of daily living; IADL, instrumental activities of daily living.
↵* Not shown if the prognostic index did not have variables in one of the major categories (demographics, medications, social history, vital signs/labs, medical diagnosis, functional measures, and other).
↵† Clinically usable if the mortality risk can be calculated using the instrument and interpreted using tables and/or figures in the paper without referring to the main text in the article, and not usable otherwise or if risk calculator is in a language other than English.

In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Can Electronic care planning using AI Summarization Yield equal Documentation Quality? (EASY eDocQ)
- Using Primary Health Care Electronic Medical Records to Predict Hospitalizations, Emergency Department Visits, and Mortality: A Systematic Review
- Evaluation of a process to implement advance care planning conversations in primary care: uptake and patient experience
- Development of a Histopathology Informatics Pipeline for Classification and Prediction of Clinical Outcomes in Subtypes of Renal Cell Carcinoma
- Advance Care Planning During the COVID-19 Pandemic
- Many Family Medicine Successful Interventions and Clinical Reviews for Common Illnesses