
Abstract
Background: Prediabetes is increasing in prevalence and is associated with risk of developing diabetes, heart disease, stroke, and retinopathy. Clinicians have limited tools to facilitate prediabetes discussions within primary care visits.
Purpose: 1) Develop a Patient and Stakeholder Advisory Committee (PASAC) to design, evaluate, and revise a prediabetes shared decision aid, and 2) evaluate the feasibility and experience of implementing the tool within primary care practice.
Methods: A prediabetes decision aid (double-sided infographic with decision questions) was created by a PASAC that included patients, primary care clinicians, diabetes educators, endocrinologists, and pharmacists. Five clinicians within 3 primary care practices tested the prediabetes tool with 50 adult patients with prediabetes. Patients completed 2 surveys immediately after the office visit and 6 weeks later. Clinicians and PASAC members completed a postintervention survey.
Results: The prediabetes shared decision aid was created through a deliberative process over 3 PASAC meetings. Ninety-six percent of patients felt the tool prepared them to decide on a diabetes prevention plan, and 100% of clinicians would use the tool again and felt the tool did not extend visit length.
Discussion: It was feasible to cocreate a prediabetes shared decision aid within a PASAC and implement the tool within a primary care setting. Patients and clinicians reported a prediabetes discussion, which may mitigate rates of progression to diabetes and associated complications. Future research should evaluate which of the intervention components most effectively promotes discussion of prediabetes within a primary care setting.
- Decision Support Techniques
- Diabetes Mellitus
- Prediabetes
- Primary Health Care
- Surveys and Questionnaires
Introduction
Prediabetes is a condition involving elevated blood glucose (Hemoglobin A1c (A1c), 5.7% to 6.4%) below the diabetic range (A1c ≥ 6.5%). Approximately 38% of adults in the United States have prediabetes.1 Prediabetes is associated with risk of developing diabetes, in addition to macro- and microvascular complications.2⇓–4 Previous research has shown that intensive prevention strategies are effective at preventing or delaying diabetes,5–6 but are not available to all patients.7 Another study shows that patients simply notified that they had prediabetes experienced improvements in glucose tolerance compared with controls.8 Unfortunately, many people are unaware of their diagnosis8 or have not been presented with options to prevent or delay diabetes.
Shared decision making (SDM) is a process in which patients and clinicians collaborate to make health care decisions. SDM enhances communication, risk awareness, and patient engagement by providing evidence-based education and eliciting patient priorities. Effective SDM includes discussion of choices followed by values-based decision making.9 Previous research has shown that when patients understand their options, they are more likely to participate in making decisions for their care10 and to have accurate perceptions of the potential outcomes associated with those decisions.11 SDM may facilitate prediabetes conversations and prevent risk of progression to diabetes.11–12 Although there are brief tools for prediabetes SDM,13–14 evaluation of these tools are not yet available; additional tools should be developed that include infographics and are designed in collaboration with patients.
Internal and external stakeholders who are end users of health care innovations should be involved in the development, implementation, and dissemination of patient-centered outcomes research. Previous research has shown that their engagement facilitates balanced contributions, and15 meaningful involvement provides for retention and investment of patients, community members and health care stakeholders.16 Creating a Patient and Stakeholder Advisory Committee (PASAC) to cocreate a shared decision aid is an innovative approach that may increase likelihood of its utility for patients and clinicians.17
Study Purpose
This study aimed to 1) develop a PASAC to design, evaluate, and revise a prediabetes shared decision aid and, 2) evaluate the feasibility of implementation of the tool in primary care practice.
Methods
Aim 1
Plan-Do-Study-Act Study Design
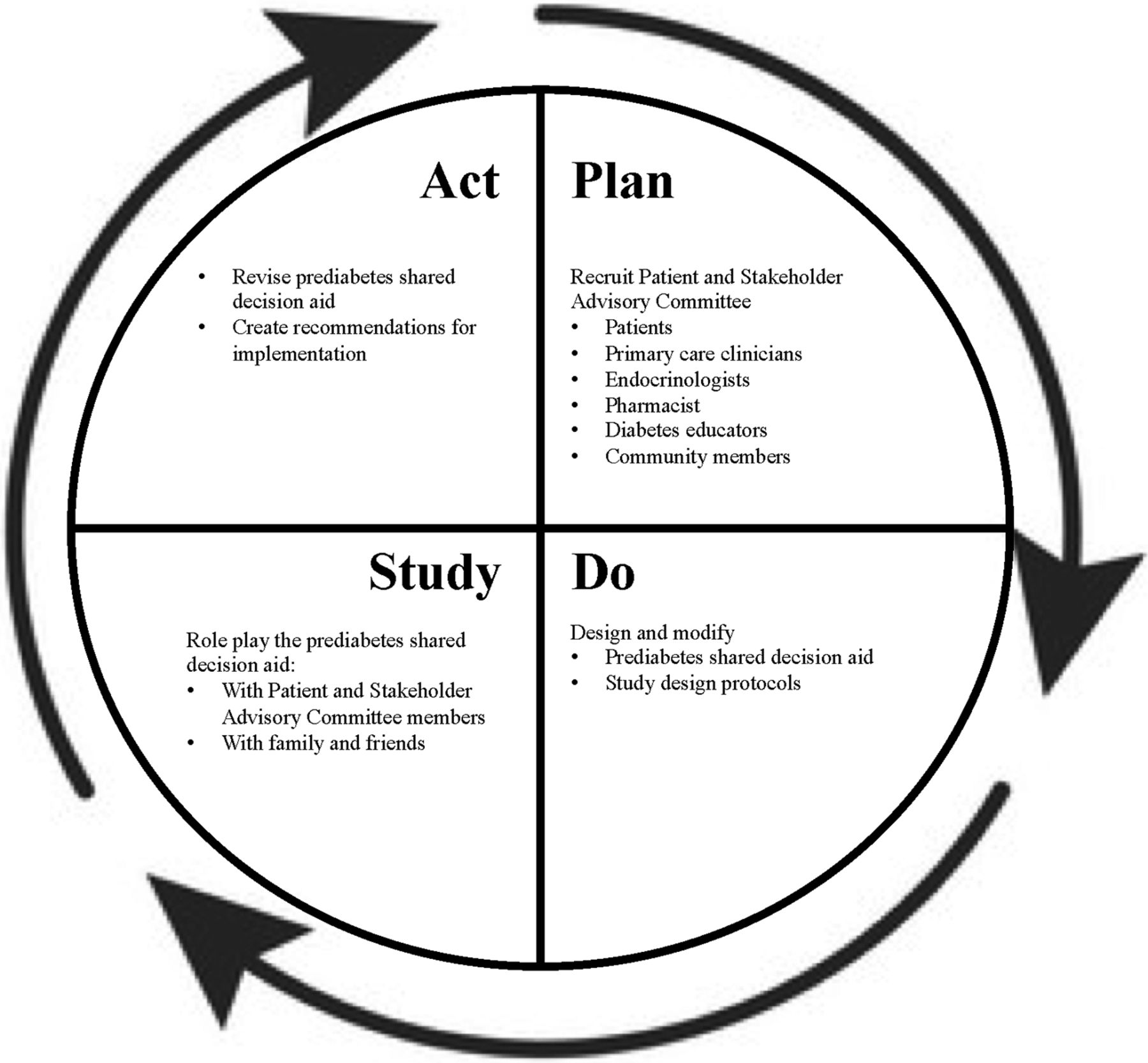
The PASAC conducted a Plan-Do-Study-Act (PDSA) cycle to create a prediabetes SDM tool, which was based on the PDSA model of improvement (Figure 1).18 Plan: A diverse group of PASAC members (n = 12) were recruited including patients, primary care clinicians, endocrinologists, a pharmacist, diabetes educators, and community members. The PASAC met 3 times to design and modify the shared decision aid and review the patient and clinician surveys using the deliberative method.19 Study: PASAC members engaged in role playing of the shared decision aid among each other as well as with family and friends. Act: The PASAC revised the prediabetes shared decision aid and created recommendations for implementation.

PDSA Cycle for Development of Prediabetes Shared Decision Aid.
Prediabetes Shared Decision Aid
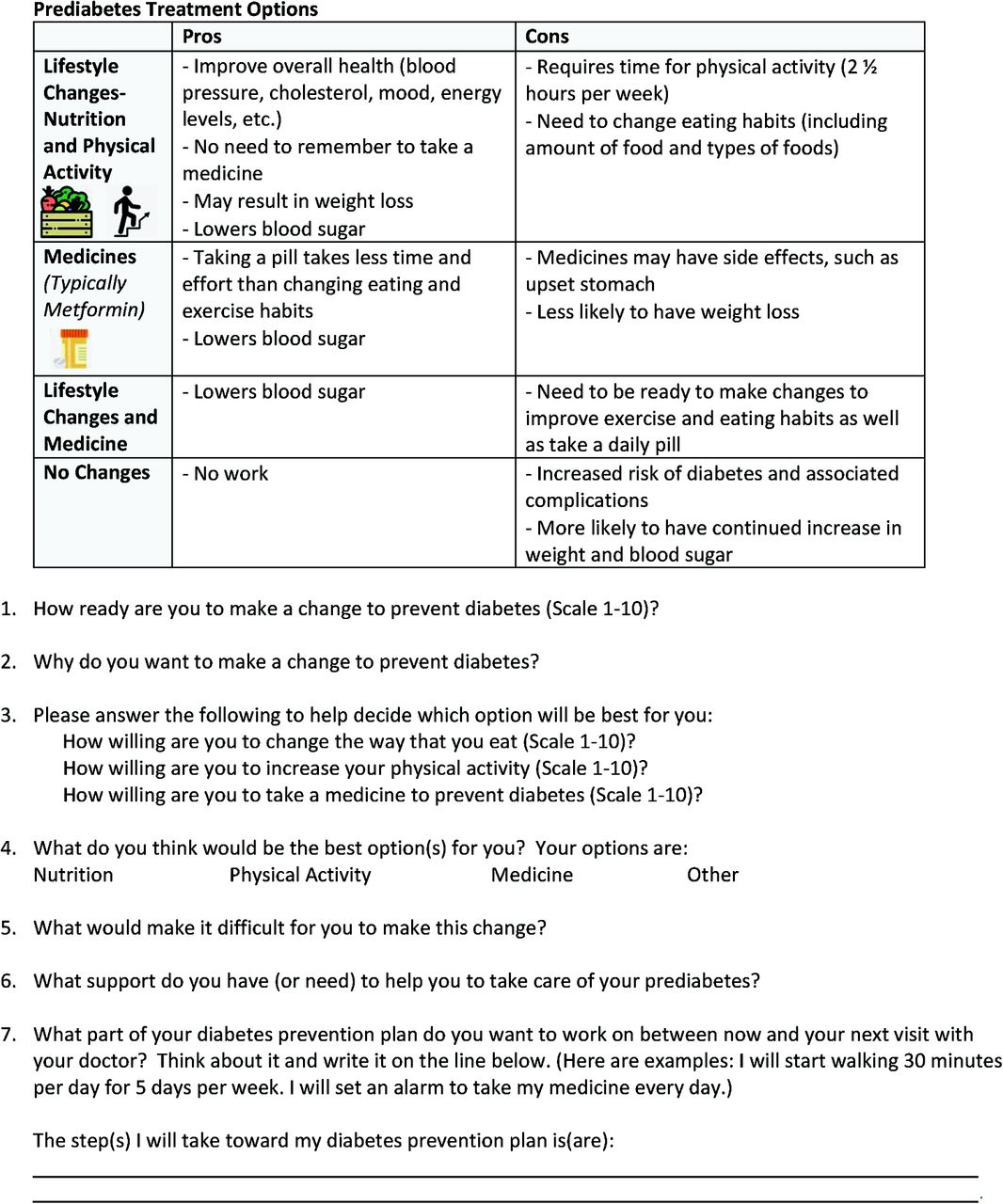
The prediabetes shared decision aid was 1 doubled-sided page with a prediabetes infographic and questions to prompt goal setting for diabetes prevention behaviors (Appendix). The infographic defined prediabetes and associated risk factors, delineated that prediabetes is reversible, and described strategies to decrease risk of developing diabetes including physical activity, nutrition, and medications. The decision aid component included a pro/con table for the diabetes risk reduction strategy, questions to elicit priorities and goals, and a prediabetes action plan.
Aim 2
Implementation of the Prediabetes Shared Decision Aid
The prediabetes shared decision aid was implemented in 50 clinical encounters across 3 primary care practices. Potential patients were identified through the electronic medical record, and clinical staff were alerted about patients through the electronic medical record. Patients and family medicine clinicians discussed prediabetes during the primary care appointment. Afterward, family medicine clinicians documented the preferred management selection (lifestyle, metformin, other, or none) in a standardized template.
Participants
Family medicine clinicians (n = 5) were recruited from 3 family medicine practices within a practice-based research network.
Patients (n = 50) were recruited from the 3 family medicine practices. Inclusion criteria were 1) A1c consistent with prediabetes in the preceding 24 months, 2) age between 18 and 75 years, 3) at least 1 visit with a participating family medicine clinician within the past 24 months, and 4) English speaking. Exclusion criteria included 1) current pregnancy, 2) resolved prediabetes, or 3) progression to type 2 diabetes.
Evaluation
A collaborative team of researchers developed content for both the patient and clinician surveys based on available tools for SDM.22⇓⇓⇓⇓–27
Patients completed a survey postintervention assessing their experience with the tool and a mailed survey after 6 weeks to assess short-term sustained behavior change. Patients were asked about information presented in the infographic, the process of using the tool with their clinician, and the decision-making process. The 6-week survey also asked patients about their experiences with their prediabetes prevention plan. All questions utilized a 5-point Likert scale.
Family medicine clinicians completed a survey at the conclusion of eligible patient encounters. The survey measured their experience using the tool, including frequency of decision making and decisional conflict, the process of using the tool, and impact on visit time.
Data Analysis
Descriptive statistics were conducted including frequencies and percentages for categorical variables and means and standard deviations for continuous variables. Statistical analyses were performed using SPSS (SPSS Inc., Chicago, IL).
Human Subjects Protection
This study was approved by the Institutional Review Board at Lehigh valley health network.
Results
Aim 1
Prediabetes Shared Decision Aid Feedback
PASAC members modified the and provided feedback on the shared decision aid. The original target audience for the shared decision aid was Hispanics; however, the PASAC expanded the audience to include non-Hispanic patients. The PASAC members reduced the number of questions included on the shared decision aid over time and increased the emphasis on action planning. The revised shared decision aid was cleaner, more organized, and contained more visuals and less text.
PASAC Partnership Self-Assessment Tool
After the fourth PASAC meeting, all responding members reported a clear agenda, appropriate objectives, productive meetings, and a clearly communicated follow-up plan (Table 1). In addition, all respondents reported that they are comfortable bringing new ideas to the meetings and that members respect each other’s opinions.
Patient and Stakeholder Advisory Committee’s Partnership Self-Assessment Tool Results (n = 8)
Aim 2
Implementation of the Shared Decision Aid
Patients were identified through the electronic medical record system. Clinicians reported that the shared decision aid was feasible within the context of a routine clinical office visit despite prediabetes not being the primary reason for the visit. Patients found the shared decision aid acceptable to complete; all consented patients completed the shared decision aid.
Patient Demographics Characteristics
Enrolled patients were predominantly female (66%), white (76%), non-Hispanic (80%), and over the age of 50 years (76%) (Table 2). Participants had an average A1c of 6.0%.
Patient Demographic Characteristics (n = 50)
Patient Postintervention and 6-week Surveys
Among participating patients, 92% reported that they decided together with their doctor about how to treat prediabetes (Table 3). Furthermore, 96% felt the SDM tool prepared them to decide on a diabetes prevention plan. After 6 weeks, 80% of responding patients said they had been following the diabetes prevention plan most days.
Patient Post-Intervention and 6-Week Survey
Clinician Survey
All family medicine clinicians reported that the prediabetes tool helped them provide more information to their patients than they had previously, with 80% (n = 5) stating that the SDM tool made it easier to include patients in the decision-making process. They reported that they would use the prediabetes shared decision aid again, and there was no change in the visit length due to using the tool. The clinicians thought the tool was beneficial because it provided a new framework for explaining prediabetes and a guided conversation about prediabetes management. Previously without the decision aid, they felt that prediabetes was challenging to express susceptibility.
Discussion
A prediabetes shared decision aid was cocreated in partnership with patients, clinicians, and key stakeholders. The shared decision aid facilitated conversations about diabetes prevention and logistically did not alter the primary care visit length. Patients felt the shared decision aid enabled them to create a diabetes prevention plan; all patients chose an intervention, and a majority of patients followed that plan after 6 weeks. Family medicine clinicians felt the shared decision aid was useful for communicating with their patients and would use it in the future.
Recommendations for PASAC Process
Primary care researchers who participate with a PASAC should consider the lessons learned during this study. Clinical members were more vocal during the initial meeting compared with patient members; the PASAC leader prompted patient members for their opinions with the goal of making them feel comfortable participating. At the end of the first meeting, the leader asked all members to provide final comments by systematically going around the room. Newsletters were used to maintain engagement with PASAC members in between meetings. These strategies increased participation from PASAC members in future meetings.
Recommendations for Implementing the Shared Decision Aid in Primary Care
Family medicine clinicians felt more comfortable addressing prediabetes with a shared decision aid. Primary care providers who aim to implement the prediabetes shared decision aid in clinical office visits will need to have a clear method of identifying patients with prediabetes. The study team used A1c lab values to identify eligible patients because the problem lists often lacked a diagnosis of prediabetes, impaired fasting glucose, or impaired glucose tolerance. In addition, the lab results did not specify whether or not glucose levels were fasting, making those results ineligible.
Limitations
One limitation of this study is the small pilot sample size of 50 clinical encounters in 3 clinical sites. Future research should include a larger sample in more diverse primary care settings with a control arm to measure the effectiveness of the tool. Only 30 patients completed the 6-week survey. More research is needed to understand long-term adherence to diabetes prevention plans. In addition, this patient population does not have adequate access to a local diabetes prevention program. Future iterations of this tool may include a diabetes prevention program as part of the menu of options for diabetes prevention. During the informed consent process, patients were informed about the prediabetes diagnosis, which sometimes led to more robust conversations on prediabetes. The impact of this process needs to be more fully understood. Furthermore, this study could have underestimated the number of prediabetics since inclusion criteria used A1c lab values, and some patients may not have been screened for A1c.
Conclusions
It was feasible to cocreate a prediabetes shared decision aid within a PASAC and implement the tool within a primary care setting. Patients and family medicine clinicians reported a prediabetes discussion, which may mitigate rates of progression to diabetes and associated complications. Future research should evaluate which intervention components most effectively promoted discussion of prediabetes within a primary care setting and the impact of clinical discussions of prediabetes.
Acknowledgments
The authors acknowledge the members of the Patient and Stakeholder Advisory Committee (PASAC): Edwin Colon; Nicole Defenbaugh, PhD; Roya Hamadani, MPH; Katarzyna Jabbour, PharmD; Mercedes Jerkiewics; Robert McCauley, MD; Joyce Najarian, RN; Franky Ortiz; Elia Ramirez; Alicia Rivera, Beatric Rosario, RN; and Janelle Sharma, DNP. The authors are particularly grateful to Susan Hansen, MA for facilitating PASAC meetings.
Appendix


Prediabetes Shared Decision Aid.
Notes
Conflicts of Interest: None.
This article was externally peer reviewed.
Funding: This project was supported in part by the Dorothy Rider Pool Trust Health Care Trust (award number 1573-011). The contents of this poster are solely the responsibility of the authors.
To see this article online, please go to: http://jabfm.org/content/33/2/262.full.
- Received for publication February 26, 2019.
- Revision received August 31, 2019.
- Accepted for publication September 3, 2019.




{kind=link}
{kind=link}
{kind=link}