
Article Figures & Data
Figures
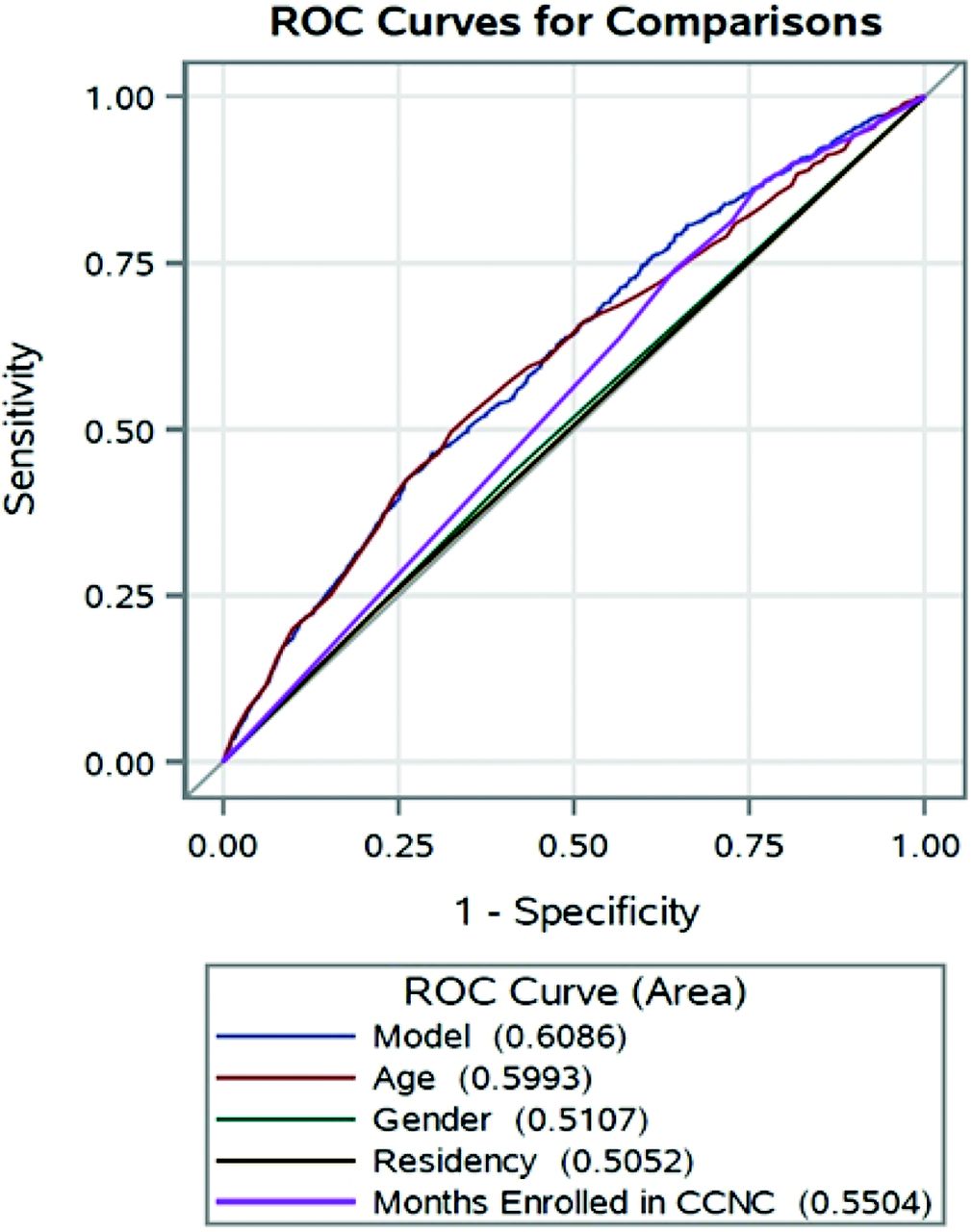
- Figure 1.
Area under the curve–receiver operating characteristics (AUC-ROC) curve for comanagement. Performance of predictor measures and a combined model including age, gender, residency, and months enrolled in Community Care of North Carolina (CCNC) for comanagement with area under the curve values for each.
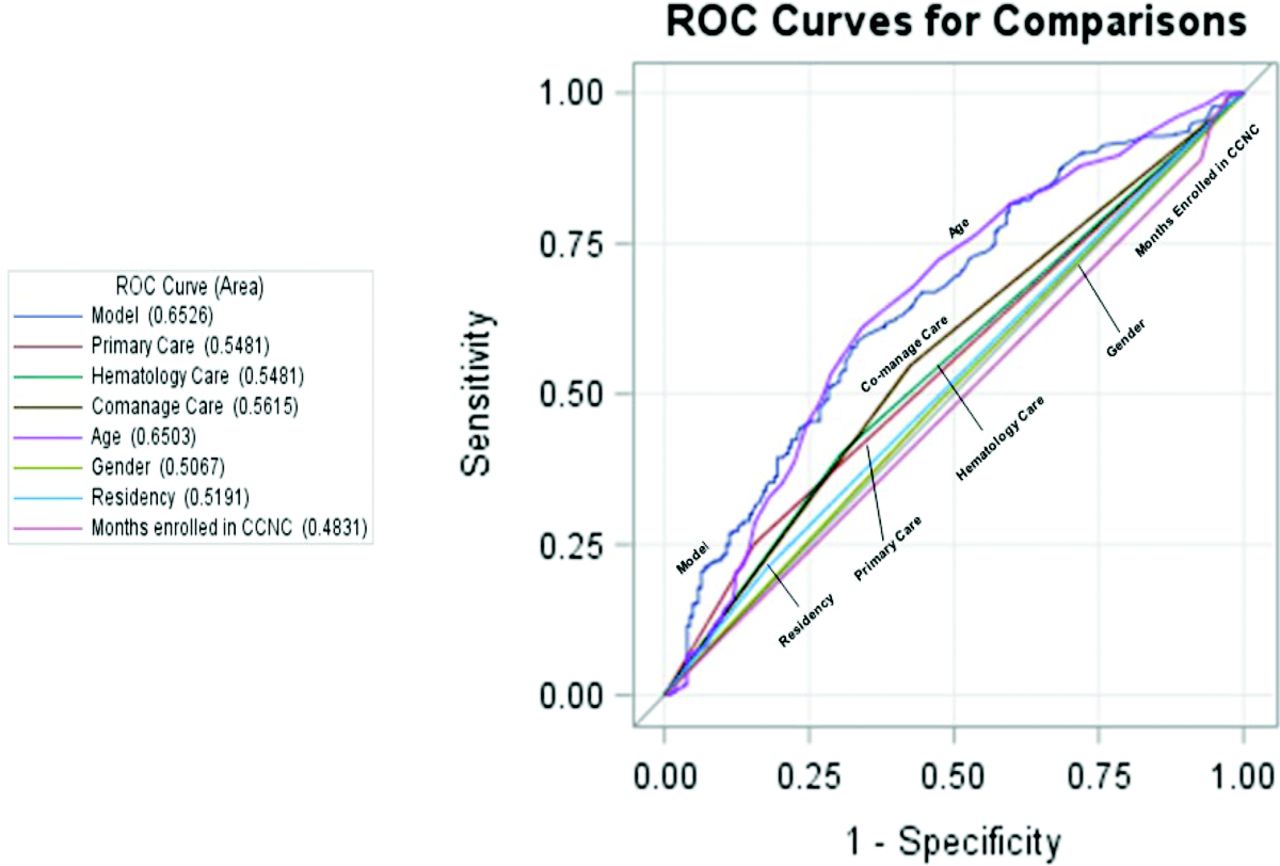
- Figure 2.
Performance of predictor measures and a combined model including Primary Care visit alone, Hematology visit alone, Co-management, age, gender, residency and months enrolled in Community Care of North Carolina (CCNC) for good versus fair or poor hydroxyurea adherence with area under the curve values for each.
Tables
Characteristics Statistic Sex, n (%) Female 1162 (56.82) Male 883 (43.18) Age, mean (SD) 22.87 (16.41) N (%) 1 to 9 years old 499 (24.40) 10 to 17 years old 436 (21.32) 18 to 30 years old 537 (26.26) 31 to 45 years old 347 (16.97) 46 to 64 years old 194 (9.49) ≥65 years old 32 (1.56) CCNC program months enrolled*, mean (SD) 10.67 (3.43) Dual eligible Medicare and Medicaid, n (%) Yes 417 (20.39) No 1628 (79.61) Residence†, n (%) Metro 1558 (76.19) Non-Metro adjacent to Metro 440 (21.52) Non-Metro un-adjacent to Metro 47 (2.30) CCNC network, n (%) Access East 390 (19.07) Access Care 180 (8.80) Carolina Collaborative Community Care 125 (6.11) Carolina Community Health Partnership 30 (1.47) Community Care Partners of Greater Mecklenburg 320 (15.65) Community Care of Southern Piedmont 66 (3.23) Community Care of Wake/Johnston Counties 217 (10.61) Community Care of Western North Carolina 20 (0.98) Community Care of the Lower Cape Fear 112 (5.48) Community Care of the Sandhills 102 (4.99) Community Health Partners 37 (1.81) Northern Piedmont Community Care 133 (6.5) Northwest Community Care Network 134 (6.55) Partnership for Community Care 179 (8.75) - Table 2.
List of Non-Hematology Specialist by Type and Visit Frequency for Age 1 to 65+ (Sample N = 2045)
Specialty Type Frequency Primary care visits 6251 Hematology specialty visits 2792 Non-hematology specialty visits 8827 Acute care* 2743 Physician assistant (unidentified specialty or family practice) 1477 Nurse practitioner (unidentified specialty or family practice) 1144 Unidentifiable (null)† 458 Obstetrician/gynecologist 383 Other specialty visits‡ 377 Orthopedic medicine 295 Ophthalmology/optometry 282 Surgery 235 Cardiology 191 Neurology 178 Pulmonary 174 Oncology 161 Nephrology 122 Otolaryngology 116 Anesthesiology 103 Gastroenterology 96 Physical and rehabilitation medicine 91 Foot & ankle surgery/podiatric medicine 87 Urology 82 Psychology 32 ↵* Acute care visit—a visit that occurred in an out-patient acute setting.
↵† Unidentifiable (Null) category includes office visits with a billing provider code for “multi-specialty” or “single specialty” with no rendering provider information.
↵‡ Other specialty visits include outpatient visits not historically linked to SCD care or a frequency of visits within the specialty category ≤ 1% of the total number of specialty visits. Excludes SCD and general NP or PA visits. Includes addiction medicine, allergy and immunology, anatomic pathology, critical care medicine, dermatology, development behavior, diagnostic radiology, endocrinology, geriatric medicine, infectious disease, special hospital, neonatal-perinatal medicine, neuro-development, rheumatology, sleep medicine, sports medicine, vascular and interventional.
- Table 3.
Emergency Department Encounters, In-Patient Stays, Out-Patient Visits, Emergency Department Reliance and Co-Management for North Carolina Medicaid Enrolled 12 Months and Age 1 to 65+ (Sample = 2045)
Age Total ED Encounters Within 7-day Re-Encounters Within 14-day Re-Encounters Within 30-day Re-Encounters Participants, n (%) Encounters, n (mean) Median (IQR) Participants, n (%) Encounters, n (mean) Median (IQR) Participants, n (%) Encounters, n (mean) Median (IQR) Participants, n (%) Encounters, n (mean) Median (IQR) 1 to 9 (n = 499) 348 (69.74) 930 (1.86) 1 (0, 3) 75 (15.03) 102 (0.20) 0 (0, 0) 96 (19.24) 146 (0.29) 0 (0, 0) 114 (22.85) 220 (0.44) 0 (0, 0) 10 to 17 (n = 436) 268 (61.47) 643 (1.47) 1 (0, 2) 47 (10.78) 61 (0.14) 0 (0, 0) 60 (13.76) 84 (0.19) 0 (0, 0) 74 (16.97) 128 (0.29) 0 (0, 0) 18 to 30 (n = 537) 423 (78.77) 2801 (5.22) 2 (1, 6) 166 (30.91) 934 (1.74) 0 (0, 1) 189 (35.20) 1253 (2.33) 0 (0, 1) 229 (42.64) 1663 (3.10) 0 (0, 2) 31 to 45 (n = 347) 258 (74.35) 1804 (5.20) 2 (0, 4) 84 (20.49) 703 (2.03) 0 (0, 0) 105 (30.36) 914 (2.63) 0 (0, 1) 125 (36.02) 1176 (3.39) 0 (0, 2) 46 to 64 (n = 194) 132 (68.04) 607 (3.13) 1 (0, 4) 37 (19.07) 148 (0.76) 0 (0, 0) 44 (22.68) 209 (1.08) 0 (0, 0) 55 (28.35) 297 (1.53) 0 (0, 1) 65+ (n = 32) 22 (68.75) 49 (1.53) 1 (0, 2) 1 (3.13) 1 (0.03) 0 (0, 0) 2 (6.25) 2 (0.06) 0 (0, 0) 6 (18.75) 9 (0.28) 0 (0, 0) All (n = 2045) 1451 (70.95) 6834 (3.34) 1 (0, 4) 410 (20.05) 1949 (0.94) 0 (0, 0) 496 (24.25) 2608 (1.28) 0 (0, 0) 603 (29.49) 3493 (1.71) 0 (0, 1) Age Total IP Hospitalizations Within 7-Day Rehospitalization Within 14-Day Rehospitalization Within 30-Day Rehospitalization Participants, n (%) Stays, n (mean) Median (IQR) Participants, n (%) Stays, n (mean) Median (IQR) Participants, n (%) Stays, n (mean) Median (IQR) Participants, n (%) Stays, n (mean) Median (IQR) 1 to 9 (n = 499) 176 (35.27) 312 (0.63) 0 (0, 1) 13 (2.61) 13 (0.03) 0 (0, 0) 16 (3.21) 20 (0.04) 0 (0, 0) 26 (5.21) 43 (0.09) 0 (0, 0) 10 to 17 (n = 436) 133 (30.50) 324 (0.74) 0 (0, 1) 10 (2.29) 10 (0.02) 0 (0, 0) 20 (4.59) 25 (0.06) 0 (0, 0) 30 (6.88) 56 (0.13) 0 (0, 0) 18 to 30 (n = 537) 318 (59.22) 1211 (2.26) 1 (0, 2) 45 (8.38) 84 (0.16) 0 (0, 0) 73 (13.59) 234 (0.44) 0 (0, 0) 100 (18.62) 479 (0.89) 0 (0, 0) 31 to 45 (n = 347) 184 (53.03) 618 (1.78) 1 (0, 2) 22 (6.34) 34 (0.10) 0 (0, 0) 32 (9.22) 81 (0.23) 0 (0, 0) 46 (13.26) 208 (0.60) 0 (0, 0) 46 to 64 (n = 194) 88 (45.36) 225 (1.16) 0 (0, 1) 4 (2.06) 7 (0.04) 0 (0, 0) 9 (4.64) 22 (0.11) 0 (0, 0) 17 (8.76) 55 (0.28) 0 (0, 0) 65+ (n = 32) 17 (53.13) 19 (0.59) 1 (0, 1) 0 (0) 0 (0) 0 (0, 0) 0 (0) 0 (0) 0 (0, 0) 0 (0) 0 (0) 0 (0, 0) All (n = 2045) 916 (44.79) 2709 (1.32) 0 (0, 1) 94 (4.60) 148 (0.07) 0 (0, 0) 150 (7.33) 382 (0.19) 0 (0, 0) 219 (10.71) 841 (0.41) 0 (0, 0) Age Total Outpatient Visits PCP Visits Hematology Specialty Visits Non-Hematology Specialty Visits Participants, n (%) Visits, n (mean) Median (IQR) Participants, n (%) Visits, n (mean) Median (IQR) Participants, n (%) Visits, n (mean) Median (IQR) Participants, n (%) Visits, n (mean) Median (IQR) 1 to 9 (n = 499) 486 (97.39) 4044 (8.10) 6 (4, 11) 437 (87.58) 1853 (3.71) 3 (1, 5) 257 (51.50) 761 (1.53) 1 (0, 2) 345 (69.14) 1430 (2.87) 2 (0, 4) 10 to 17 (n = 436) 410 (94.04) 3299 (7.57) 5 (3, 9) 344 (78.90) 1101 (2.53) 2 (1, 3) 209 (47.94) 667 (1.53) 0 (0, 2) 329 (75.46) 1531 (3.51) 2 (1, 4) 18 to 30 (n = 537) 482 (89.76) 4174 (7.77) 6 (2, 11) 332 (61.82) 1226 (2.28) 1 (0, 3) 214 (39.85) 668 (1.24) 0 (0, 2) 406 (75.61) 2280 (4.25) 2 (1, 6) 31 to 45 (n = 347) 319 (91.93) 3708 (10.69) 8 (4, 16) 254 (73.20) 1214 (3.50) 2 (0, 5) 134 (38.62) 459 (1.32) 0 (0, 1) 271 (78.10) 2035 (5.86) 3 (1, 8) 46 to 64 (n = 194) 180 (92.78) 2286 (11.78) 9 (4, 17) 140 (72.16) 716 (3.69) 2 (0, 5) 72 (37.11) 222 (1.14) 0 (0, 1) 162 (83.51) 1348 (6.95) 4 (2, 10) 65+ (n = 32) 30 (93.75) 359 (11.22) 9 (4.5,14) 26 (81.25) 141 (4.41) 4 (1.5, 6) 6 (18.75) 15 (0.47) 0 (0, 0) 27 (84.38) 203 (6.34) 4.5 (1, 8) All (n = 2045) 1907 (93.25) 17870 (8.74) 7 (3, 12) 1533 (74.96) 6251 (3.06) 2 (0, 4) 892 (43.62) 2792 (1.37) 0 (0, 2) 1540 (75.31) 8827 (4.32) 2 (1, 6) Age ED Reliance Score Co-management % of Sample with EDR ≥ 0.33 Mean (SD) n (Row %) 1 to 9 (n = 499) 21.84 0.19 (0.21) 224 (44.88) 10 to 17 (n = 436) 23.17 0.19 (0.24) 171 (39.22) 18 to 30 (n = 537) 44.69 0.35 (0.31) 153 (28.49) 31 to 45 (n = 347) 34.01 0.27 (0.28) 105 (30.26) 46 to 64 (n = 194) 24.23 0.20 (0.25) 53 (27.32) 65+ (n = 32) 12.50 0.14 (0.20) 6 (18.75) All (n = 2045) 30.27 0.25 (0.27) 712 (34.82) ED, emergency department, EDR, emergency department reliance; PCP, primary care physician; IQR, interquartile ranges; IP, In-Patient; SD, standard deviation.
- Table 4.
Hydroxyurea (HU) Prescription (Rx) Fills and Adherence for North Carolina Medicaid Enrolled at least 12-monthnths Age 1 to 64 (N = 2013)
Medicaid Enrolled for 12-monthnths by Age Group 1 to 9 (n = 499) 10 to 17 (n = 436) 18 to 30 (n = 537) 31 to 45 (n = 347) 46 to 64 (n = 194) All (n = 2013) Participants with a HU Rx Filled N (% of eligible sample) 200 (40.08) 201 (46.10) 183 (34.08) 43 (12.39) 22 (11.34) 649 (32.24) Description of usage for participants with at least one HU Rx Enrolled in Medicaid for 12-months 1 to 9 (n = 200) 10 to 17 (n = 201) 18 to 30 (n = 183) 31 to 45 (n = 43) 46 to 64 (n = 22) All (n = 649) Number of HU Rx Filled Median (IQR) 7 (4, 10) 6 (4, 8) 4 (1, 7) 4 (2, 7) 5.5 (2, 10) 5 (2, 8) Number of Days Supplied† Median (IQR) 221 (104.5, 319) 180 (105, 270) 110 (30, 210) 120 (58, 210) 165 (90, 300) 159 (85, 270) Duration of HU Treatment (days)‡ Median (IQR) 340 (301, 349) 334 (285, 350) 322 (266, 345) 336 (305, 347) 334 (287, 357) 334 (284, 349) Number of Days between breaks in treatment§ Median (IQR) 14.21 (0, 50.75) 22.8 (7.75, 51.50) 49.33 (19.67, 139) 40.40 (21.60, 103.50) 35.45 (0, 89.67) 29.6 (7, 72.5) HU Adherence¶, n (%) Good 95 (47.50) 60 (29.85) 33 (18.03) 9 (20.93) 8 (36.36) 205 (31.59) Fair 30 (15.00) 48 (23.88) 23 (12.57) 8 (18.60) 2 (9.09) 111 (17.10) Poor 75 (37.50) 93 (46.27) 127 (69.40) 26 (60.47) 12 (54.55) 333 (51.31) IQR, interquartile ranges
* There were zero participants on HU in the 65+ age group so they were excluded from this analysis.
↵† Number of days supplied is the sum of the days of supply on the Rx (eg, 30-day supply) in a 12-month period per person.
↵‡ Duration of HU treatment days is the number of days between the first HU Rx filled and February 28, 2017.
↵§ Number of days between breaks in treatment is the sum of days of no HU coverage divided by the number of gaps (missing next HU Rx fill) per person.
↵¶ HU adherence is considered Good—if number of days supplied is ≤80% of duration of HU treatment; Fair or Moderate—if number of days supplied is 60% to 79% of duration of HU treatment; Poor—if number of days supplied is >60% of duration of HU treatment.




{kind=link}
{kind=link}