
Article Figures & Data
Figures
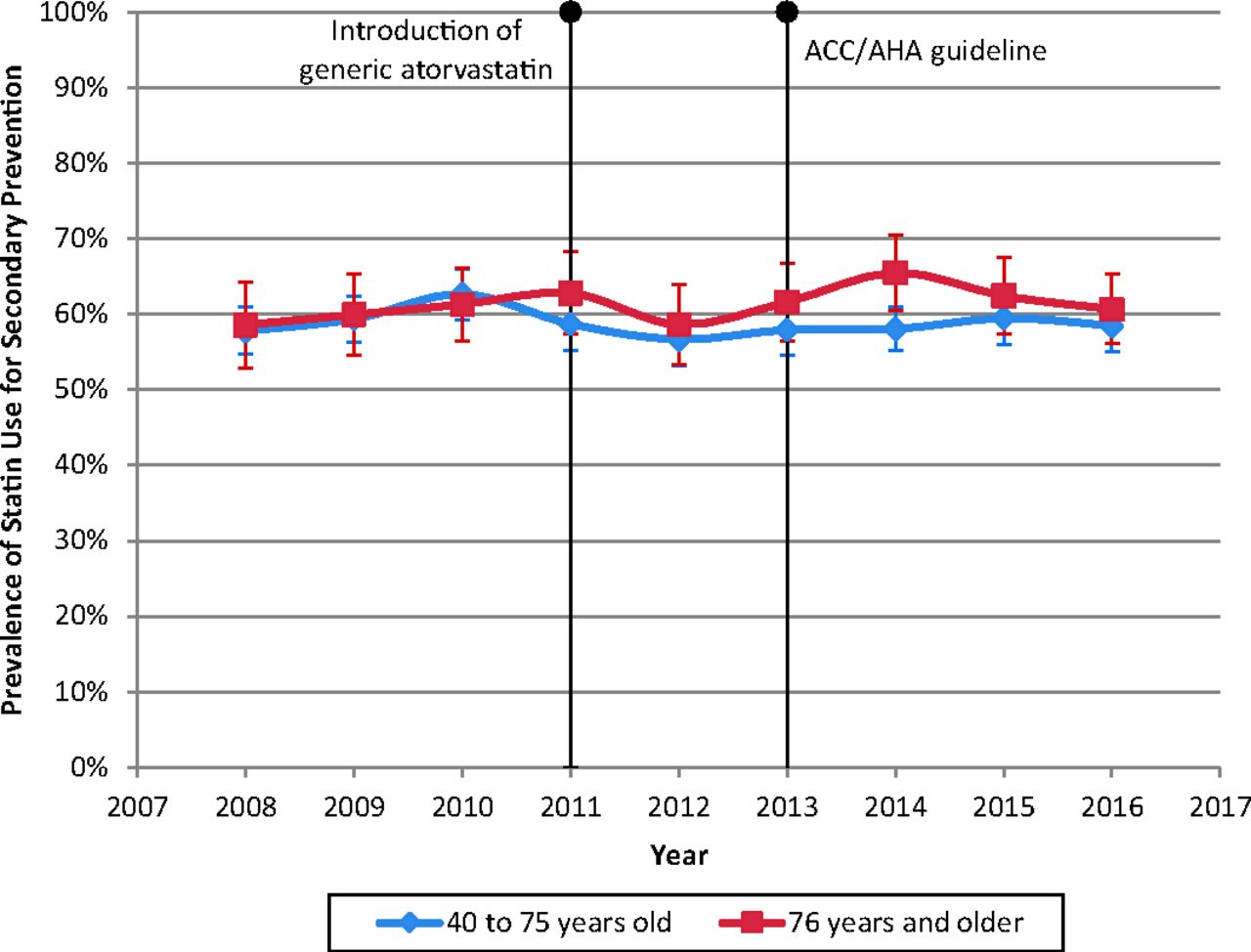
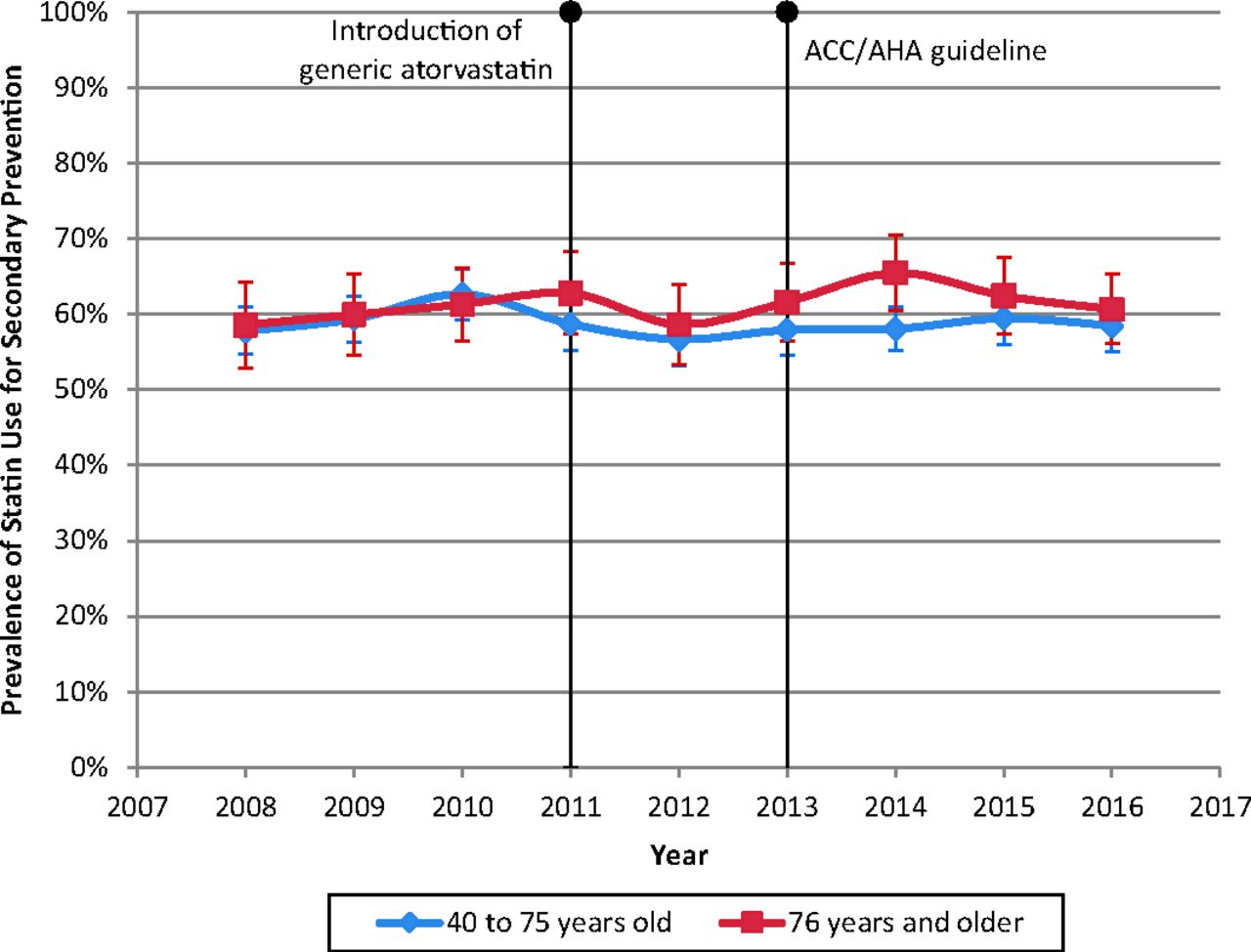
- Figure 1.
Statin use among adults with history of diagnosed Ascvd, 2008 to 2016. Source: Agency for Health Care Research and Quality, Medical Expenditure Panel Survey, Full-Year Consolidated Files, 2008 to 2016. Note: All years were age-adjusted to match the 2016 age distribution.
Tables
- Table 1.
Demographic and Health Characteristics of Adults Aged 40 Years and Older with History of Diagnosed ASCVD, 2014 to 2016
Characteristic n Weighted % 95% CI Age.in years 40 to 49 595 8.7 (7.6 to 9.8) 50 to 59 1,247 17.3 (15.9 to 18.7) 60 to 64 804 12.6 (11.4 to 13.7) 65 to 69 871 15.2 (13.7 to 16.7) 70 to 75 946 17.4 (15.8 to 19.0) 76 to 79 513 9.2 (8.1 to 10.2) 80 to 84 562 9.9 (8.9 to 10.9) 85 and above 546 9.8 (8.6 to 11.0) Sex Women 3,039 46.3 (44.5 to 48.1) Men 3,045 53.7 (51.9 to 55.5) Race/ethnicity Hispanic 1,124 9.5 (8.0 to 11.0) Non-Hispanic, white 3,198 73.5 (71.3 to 75.7) Non-Hispanic, African American 1,320 11.1 (9.7 to 12.6) Non-Hispanic, Asian 254 2.7 (2.0 to 3.5) Non-Hispanic, Other 188 3.1 (2.2 to 4.0) Marital status Unmarried 3,159 44.5 (42.3 to 46.7) Married 2,925 55.5 (53.3 to 57.7) Education Did not complete high school 2,322 31.1 (29.3 to 32.8) High school graduate or GED 1,304 22.4 (20.7 to 24.1) Some college 1,407 24.9 (23.1 to 26.7) College degree or higher 991 21.0 (19.2 to 22.9) Insurance coverage Medicare 4,064 69.7 (67.8 to 71.6) Private 1,124 20.4 (18.7 to 22.1) Medicaid 568 6.0 (5.1 to 6.9) Uninsured 328 3.9 (3.2 to 4.6) Census region Northeast 1,003 17.8 (15.8 to 19.8) Midwest 1,231 22.5 (20.2 to 24.9) South 2,628 40.8 (38.1 to 43.5) West 1,222 18.8 (17.0 to 20.7) MSA MSA 5,024 81.3 (78.1 to 84.6) Non-MSA 1,060 18.7 (15.4 to 21.9) History of cardiovascular disease CHD to MI to or angina 4,555 76.2 (74.6 to 77.9) Stroke 2,538 39.5 (37.8 to 41.2) ASCVD risk factors Doctor ever told high cholesterol 4,504 75.1 (73.4 to 76.8) Doctor ever told had hypertension 4,982 80.9 (79.4 to 82.4) Doctor ever told had diabetes 2,122 31.7 (29.8 to 35.6) Current smoker 1,020 16.8 (15.1 to 18.4) Usual source of care No 531 7.9 (6.8 to 8.9) Yes 5,553 92.1 (91.1 to 93.2) Source: Agency for Healthcare Research and Quality, Medical Expenditure Panel Survey 2014 to 2016.
ASCVD, atherosclerotic cardiovascular disease; CHD, coronary heart disease; CI, confidence interval; ED, emergency department; GED, General Equivalency Diploma; MI, myocardial infarction; MSA, Metropolitan Statistical Area.
Total Population Statin Users N Weighted Population, Millions (95% CI) Weighted Users, Millions (95% CI) Weighted % (95% CI) Age 40 years and older 6,084 23.4 (22.1 to 24.6) 13.9 (13.0 to 14.8) 59.4 (57.4 to 61.5) Age 40 to 75 years 4,463 16.6 (15.7 to 17.6) 9.7 (9.0 to 10.4) 58.3 (55.9 to 60.6) Age 76 years and older 1,621 6.7 (6.2 to 7.3) 4.2 (3.8 to 4.7) 62.3 (59.0 to 65.7) ASCVD, atherosclerotic cardiovascular disease; CI, confidence interval.
Source: Agency for Healthcare Research and Quality, Medical Expenditure Panel Survey, 2014 to 2016.
- Table 3.
Odds of Current Statin Use and Sociodemographic Characteristics, Adults Aged 40 Years and Older with History of Diagnosed ASCVD, 2014 to 2016 (n = 6,039)
Characteristic Odds Ratio (95% CI) P-Value Age, in years 40 to 49 (reference) 1.00 — — 50 to 59 1.60 (1.14 to 2.26) .007 60 to 64 2.43 (1.66 to 3.56) <.001 65 to 69 3.36 (2.15 to 5.22) <.001 70 to 75 3.09 (2.02 to 4.74) <.001 76 to 79 3.43 (2.14 to 5.49) <.001 80 to 84 3.03 (1.93 to 4.74) <.001 85 and above 2.03 (1.27 to 3.24) .003 Female 0.65 (0.55 to 0.77) <.001 Race/ethnicity Non-Hispanic, white (reference) 1.00 — — Hispanic 0.69 (0.52 to 0.92) .011 Non-Hispanic, African American 0.81 (0.63 to 1.04) .102 Non-Hispanic, Asian 1.25 (0.82 to 1.90) .297 Non-Hispanic, other 0.70 (0.40 to 1.21) .201 Has a usual source of care 1.87 (1.37 to 2.56) <.001 Doctor ever told high cholesterol 6.22 (5.02 to 7.72) <.001 Doctor ever told had high blood pressure 1.33 (1.08 to 1.65) .009 Doctor ever told had diabetes 1.51 (1.24 to 1.85) <.001 Current smoker 0.90 (0.70 to 1.14) .375 SF-12 Physical Component Score 1.01 (1.00 to 1.02) .022 Married 1.26 (1.02 to 1.57) .033 Education Did not complete high school (reference) 1.00 — — High school graduate or GED 1.23 (1.00 to 1.52) .055 Some college 1.39 (1.08 to 1.80) .011 College degree or higher 1.15 (0.87 to 1.51) .339 Insurance coverage Private (reference) 1.00 — — Medicare 1.05 (0.76 to 1.44) .781 Medicaid 1.13 (0.78 to 1.63) .527 Uninsured 0.90 (0.60 to 1.35) .607 Census region Northeast (reference) 1.00 — — Midwest 1.17 (0.88 to 1.55) .271 South 0.82 (0.62 to 1.08) .165 West 0.90 (0.67 to 1.22) .504 MSA 1.11 (0.85 to 1.44) .451 Constant 0.04 (0.02 to 0.08) <.001 ASCVD, atherosclerotic cardiovascular disease; CI, confidence interval; GED, General Equivalency Diploma; MSA, metropolitan statistical area; SF-12, 12-Item Short Form Health Survey (SF-12).
Source: Agency for Healthcare Research and Quality, Medical Expenditure Panel Survey, 2014 to 2016.
Year Prevalence Per 1000 95% CI 2008 161.0 151.3 to 170.6 2009 157.5 148.8 to 166.3 2010 153.7 145.5 to 162.0 2011 149.5 140.7 to 158.3 2012 147.6 138.7 to 156.6 2013 155.3 146.9 to 163.7 2014 156.6 147.9 to 165.3 2015 153.4 144.6 to 162.2 2016 152.6 144.6 to 160.6 ASCVD, atherosclerotic cardiovascular disease.
Adjusted Wald test to Prob > F = 0.1931.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Discharge prescription patterns for antiplatelet and statin therapy following carotid endarterectomy: an analysis of the vascular quality initiative
- Effects of statin therapy on coronary plaque volume by decreasing CRP/hsCRP levels: A meta-regression of randomized controlled trials
- New Research on Back Pain, Diet and Diabetes, Advanced Care Planning, and Other Issues Frequently Seen in Family Medicine