
Abstract
Introduction: The objectives of this study were to examine if self-reported access to primary care is associated with actual patient wait times and use of telephone visits, and to assess whether this relationship differs by rural residence.
Methods: This study used 2016 administrative data from 994 primary care clinics within the Veterans Health Administration. Multiple-linear regression was used to examine relationships between patient perceptions of access and average actual patient wait time, use of telephone visits, and rural residence. Average panel size, clinic type, and panel severity were included as model covariates with cross-product terms for actual wait time, telephone use, and rurality to test for interactions.
Results: This study found patient perceptions of access aggregated at the clinic level to be conditional on the relationship between use of telephone visits, actual patient wait times, and rural residence. As actual wait time for routine appointments increases, Veterans served by clinics with a higher percent of rural Veterans perceive telephone visits more positively.
Discussion: These findings contribute to our understanding of factors associated with patient perceptions of access by highlighting complex interrelationships between strategies intended to improve access to care and how they can have differing impacts on perceptions among those living in rural or urban locations.
- Appointments and Schedules
- Rural Health
- Self Report
- United States Department of Veterans Affairs
- Veterans Health
Rural residents have identified several barriers to accessing care including distance, access to transportation, and availability of services.1 The use of telephone visits is 1 strategy being promoted to enhance access to primary care that does not require in-person visits.2,3 A recent study from the Veterans Health Administration (VHA) found that the use of telephone communication is strongly associated with higher patient perceptions of access.4 To our knowledge, no studies have specifically examined rural patients' perceptions of access associated with telephone visits, especially for clinics with longer wait times for in-person visits. Our objective was to examine whether self-reported access to primary care is associated with actual clinic wait times and use of telephone visits, and to assess whether this relationship differs between rural and urban settings.
Methods
In an observational study, we analyzed 2016 VHA administrative data from 994 VHA primary care clinics in the United States, representing data from 160,447 Veterans. Multiple-linear regression with clinics as the unit of analysis was used to examine relationships between patient perceptions of access (ie, percent of Veterans assigned to a clinic who reported they “always” received an appointment for routine primary care as soon as they needed) and 3 variables of interest: clinic wait time, use of telephone visits, and rurality defined by the proportion of patients classified as rural using the Rural-Urban Commuting Area codes corresponding with their home address.5 Average panel size, clinic type, and panel severity were included as model covariates with cross-product terms for clinic wait time, use of telephone visits, and rurality to test for interactions. This work is part of a larger quality improvement effort at the VHA and is not considered research activity subject to institutional review board review or waiver.
Results
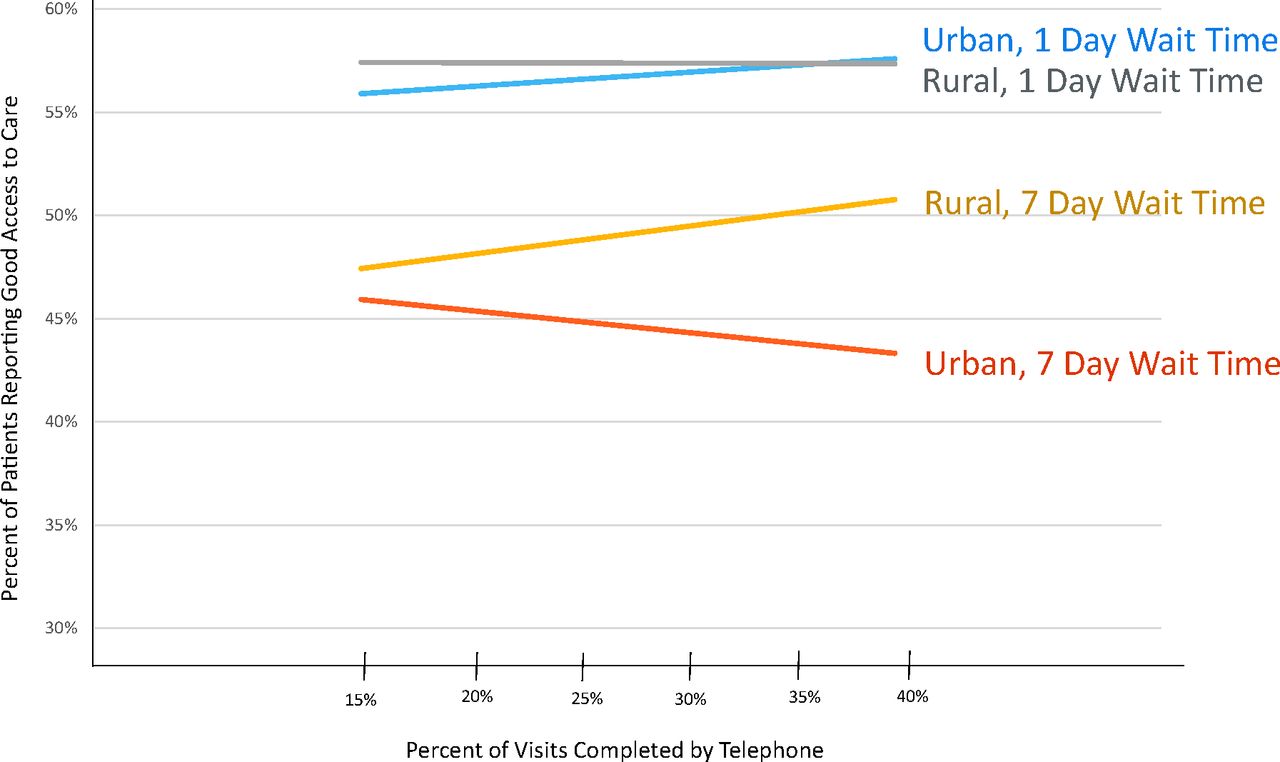
As shown in Table 1, on average 52% of the Veterans assigned to these clinics reported that they were “Always” able to schedule an appointment for a checkup or routine care with their provider as soon as they needed. Average clinic performance related to access indicated that veterans wait about 4 days for routine care, and telephone visits accounted for 28% of all primary care encounters. The mean proportion of rural patients among these clinics was 53%. Results from our regression analyses (Table 1) indicate a significant 3-way interaction between clinic wait time, use of telephone visits, and rurality, indicating that perceptions differed depending on proportion of rural Veterans and use of telephone visits (β = 0.071, P < .05). We illustrate this interaction in Figure 1. As clinic wait time for routine appointments increases, Veterans served by clinics with a higher percent of rural Veterans perceive greater use of telephone visits as improving their access to primary care, but Veterans served by clinics with a lower percent of rural Veterans perceive greater use of telephone visits as inhibiting their access to primary care.
Clinic Characteristics and Multivariable Analyses of Patient Perceptions of Access to Routine Care (n = 994)
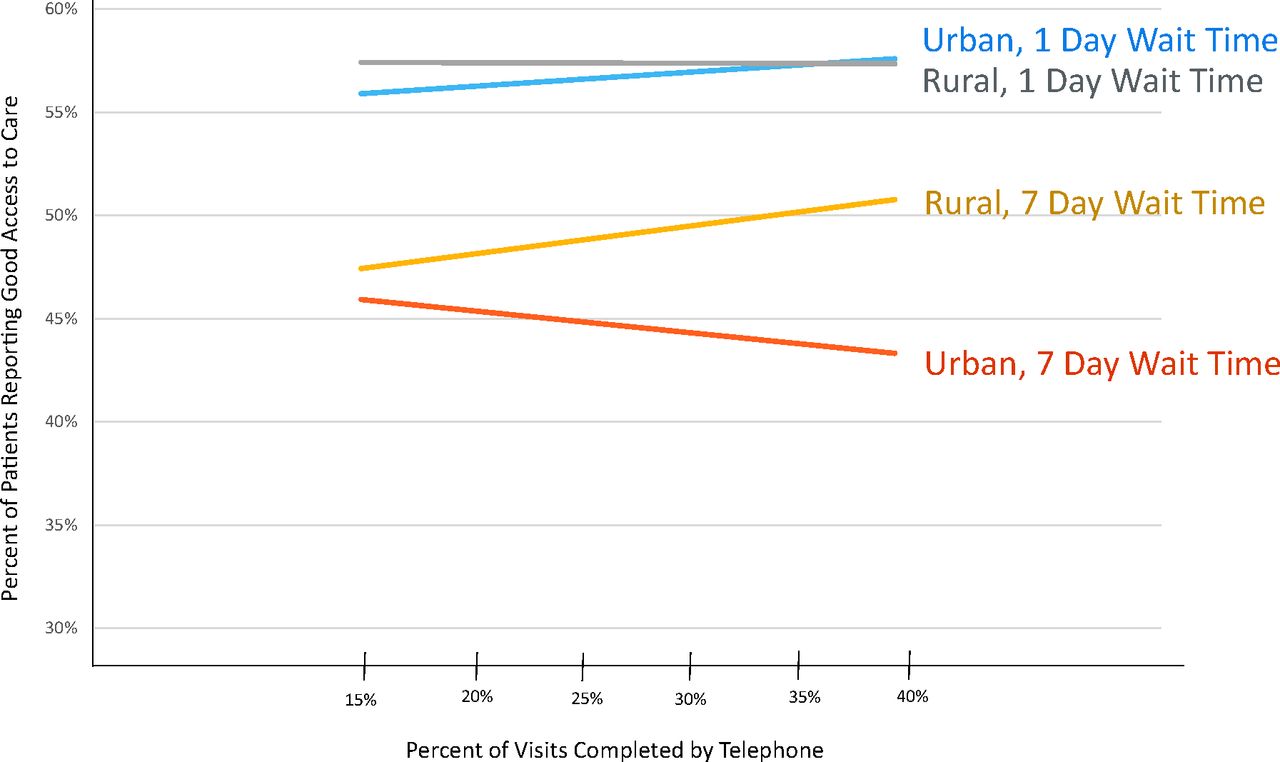
Comparison of Interaction between Clinic Wait Time and Use of Telephone Visits among Urban and Rural Clinics.
Discussion
This study found patient perceptions of access aggregated at the clinic level to be conditional on the relationship between use of telephone visits, clinic wait times, and rural residence. As actual wait time for routine appointments increases, Veterans served by clinics with a higher percent of rural Veterans perceive telephone visits more positively. While not focused specifically on rural, another study conducted in the VHA found favorable perceptions of telephone visits for routine care not requiring a physical from both Veterans and primary care providers.3 Relatedly, McKinstry et al6 found that telephone consultations were often used by rural patients and staff to maintain more regular contact and to avoid having to travel. They also reported that, unlike urban patients, rural patients were more likely to use telephone consultations to determine whether an in-person visit was necessary.6 Although more research is needed, these findings contribute to our understanding of factors associated with patient perceptions of access by highlighting complex interrelationships between strategies intended to improve access to care and how they can have differing impacts on perceptions among those living in rural or urban locations.
Notes
This article was externally peer reviewed.
Funding: This work was undertaken as part of the Veterans Administration's Primary Care Analytics Team (PCAT), supporting and evaluating VA's transition to a patient-centered medical home. Data for this report were developed by the national evaluation team of PCAT. Funding for PCAT is provided by the VA Office of Primary Care. The views expressed are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs.
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/32/5/749.full.
- Received for publication February 4, 2019.
- Revision received May 23, 2019.
- Accepted for publication May 24, 2019.




{kind=link}