
Abstract
Although the fraction of family physicians (FPs) providing Long Acting Reversible Contraceptive (LARC) services increased between 2014 and 2017, the most recent estimates show that less than a quarter of family physicians include provision of LARC in their practice. Increasing the number of FPs providing LARC will help increase patients' access to the most effective forms of birth control currently available.
Long-acting reversible contraception (LARC), which includes intrauterine devices (IUDs) and etonogestrel single rod implants, is highly effective, is not user-dependent in its effectiveness, and is an extremely cost-effective method of birth control.1⇓–3 Allowing patients access to LARC is important to reproductive autonomy and to public health as unintended pregnancies result in health risks to the mother and child, significant direct health care costs, and long-term social and economic costs to women and families.4⇓⇓–7 LARC services can be provided to patients by family physicians (FPs). Women are increasingly opting for LARC with a growth in use from 6% of US women in 2008 to 14% of US women in 2014.8 As demand for LARC increases, it is important to ensure that an appropriate primary care workforce is available to provide these services, allowing all patients to have access to these valuable contraceptive methods.
We used data from the 2014 to 2017 American Board of Family Medicine (ABFM) demographic surveys to identify the percentage of FPs who regularly provide LARC services. This survey is a mandatory component of the Maintenance of Certification examination and is taken 3 months before testing. From 2014 to 2017 the percentage of FPs regularly providing UDs, implants, and both IUDs and implants each saw an absolute increase of 3% across the 3 years to 21.5%, 13.6%, and 11.4%, respectively by 2017 (Figure 1).
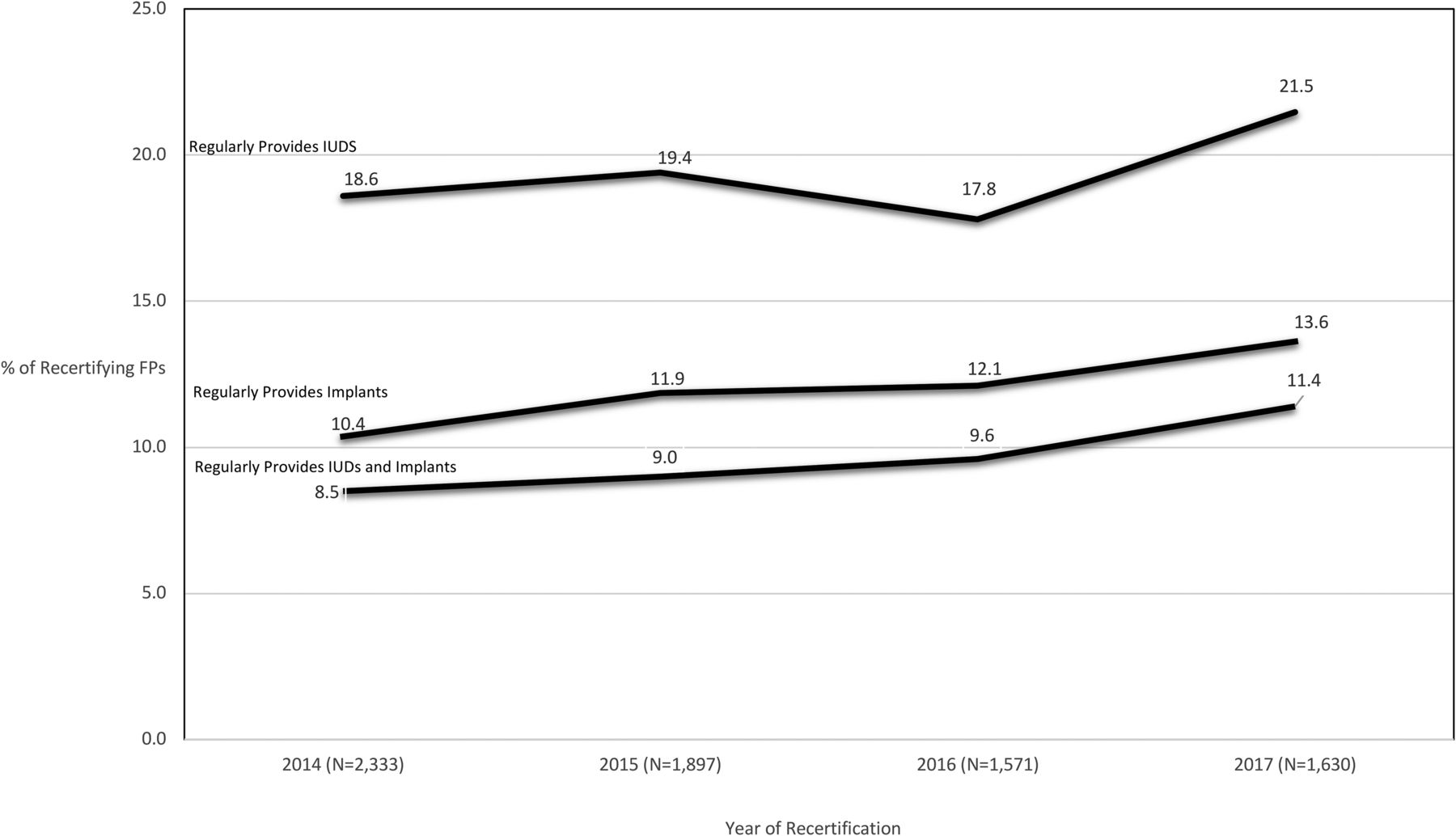
Percentage of Family Physicians Reporting Regularly Providing LARC Services, by Year of Recertification.
Although the percentage of FPs providing LARC services continues to rise, it still remains low with less than a quarter of FPs reporting that they provide any form of LARC. The relatively low provision of this form of reproductive care is in contrast to the fact that the vast majority of FPs self-report providing gender-specific care to women: in the most recent ABFM survey year available, 82% of FPs reported providing “women's health services.” This suggests that LARC is not considered part of the routine primary care offerings by a large segment of the FP workforce. Given that the majority of FPs endeavor to provide gender-appropriate services, and that the technical skills involved in IUDs and implants are within the scope of FP training, it is important to elucidate why provision of this increasingly popular contraceptive method remains low.
Though most FPs report training in family planning, FP residency training is less likely to include IUD insertion in comparison to obstetrician-gynecologist training programs, potentially leading to deficits in knowledge and comfort with this procedure among FPs post-residency.9,10 The Review Committee of the Accreditation Council on Graduate Medical Education has standards requiring comprehensive family planning training in residency,11 yet studies note great variability in the availability of this training in accredited FP training programs, with less than 25% of residencies reporting clinical training in implant insertion.12 Even for FPs with adequate LARC training and knowledge, complex reimbursement schemes and clinical environments that are not appropriately equipped for gynecological procedures can hinder a new graduate's ability to continue to provide these procedures.13,14
Given that reproductive planning and pregnancy are central to the physical health and the socioeconomic wellbeing of women and families, addressing barriers to LARC provision in primary care is important. Training and support to increase the fraction of FPs who deliver LARC services as well as promotion of policies which aim to create a more amenable practice environment for FPs to perform gynecological procedures in their primary care practice will ensure the full benefits of this most effective form of contraception are realized, and that patients' needs are fully met.
Notes
This article was externally peer reviewed.
Funding: MC was supported in part by the Department of Veterans Affairs, Veterans Health Administration, Office of Research and Development, and Health Services Research and Development.
Disclaimer: The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/32/1/10.full.
- Received for publication July 30, 2018.
- Revision received October 31, 2018.
- Accepted for publication November 2, 2018.
In this issue




{kind=link}
Related Articles
Cited By...
- No citing articles found.