
Article Figures & Data
Figures
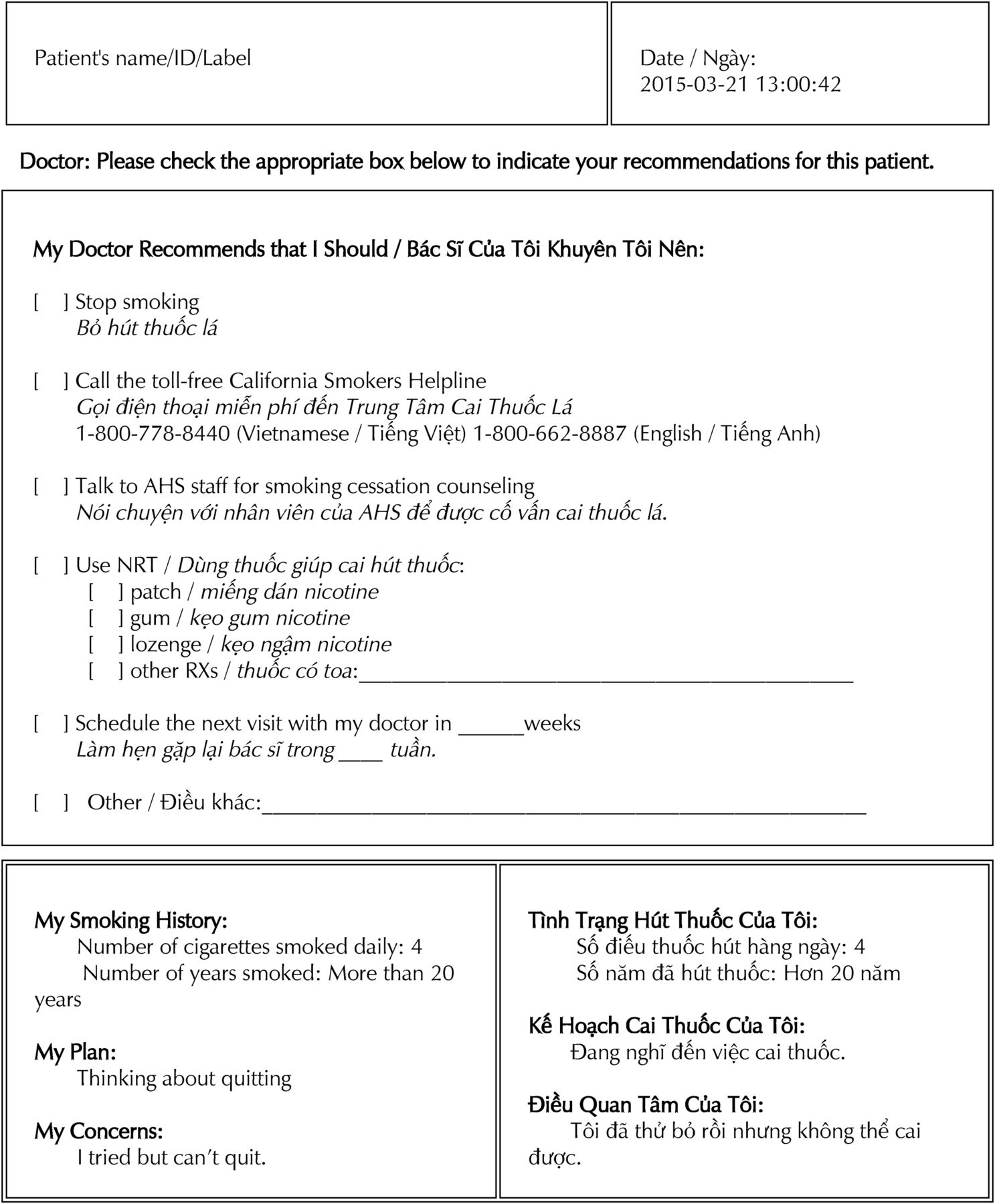
- Figure 1.
Sample bilingual summary (English/Vietnamese) printout generated by the Interactive Mobile Doctor (iMD) intervention.
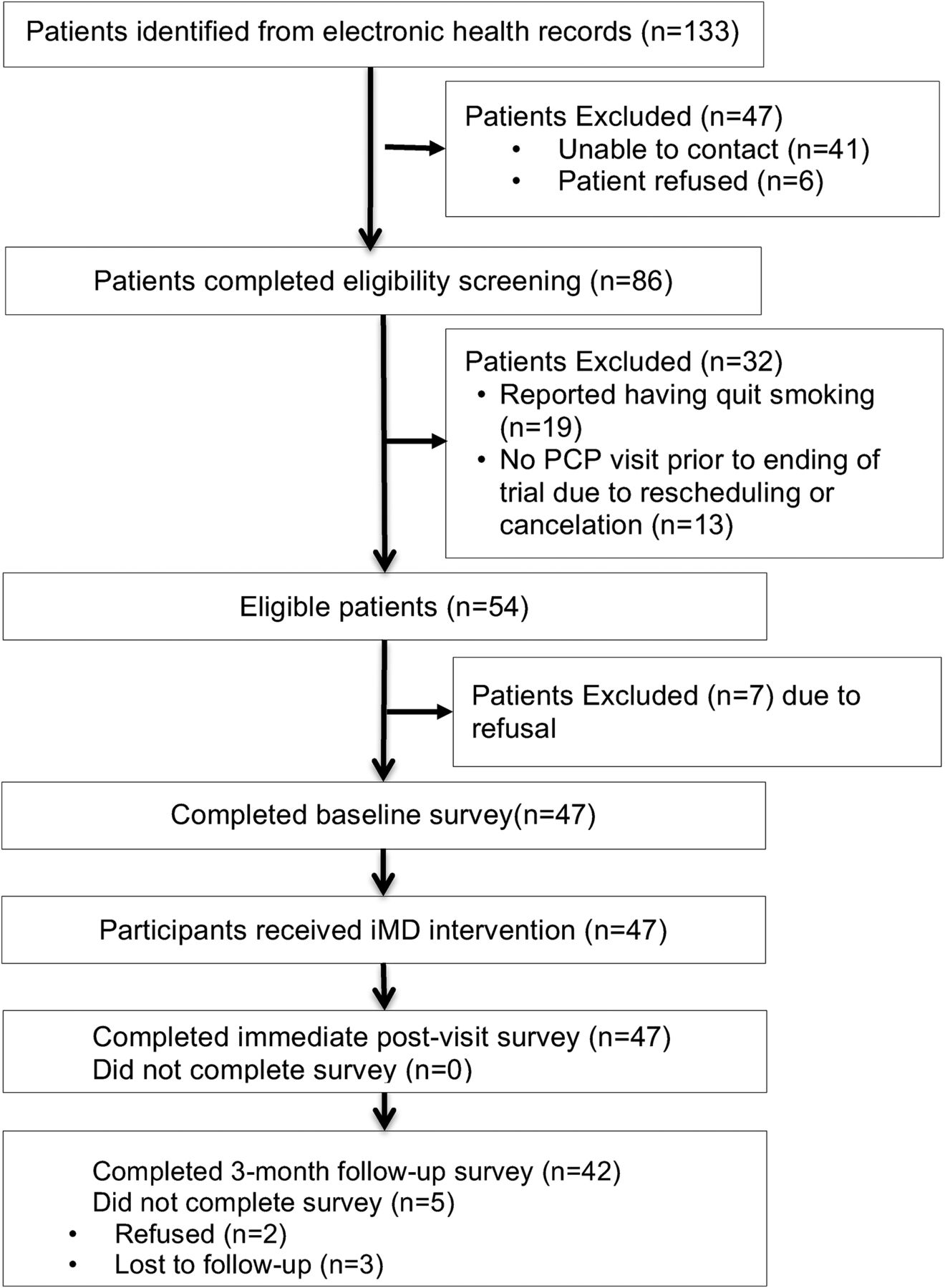
- Figure 2.
Participant flow diagram. PCP, primary care provider.
- Figure 3.
Documented primary care providers' delivery of the 5As (Ask, Advise, Assess, Assist, and Arrange) to 47 study participants across 3 consecutive primary care visits at preintervention, intervention, and postintervention based on 141 progress notes extracted from electronic health records.


Tables
- Table 1.
Coding Definitions of 5As to Quantify Primary Care Providers' Delivery of 5As as Documented on Electronic Health Record Progress Notes
Code Definitions Progress Note Examples Ask Any statement mentioned about patient's use of tobacco or smoking status. Examples: diagnosis codes, smoking status updates, mentions of tobacco use. Tobacco abuse
Still smoking 5 to 6 cigarettes per day
Advise Statements advising patient to quit or to reduce. Tobacco use: encouraged cessation
Access Statements reflecting patient's readiness to quit; examples: patient's intent, motivation or effort at quitting. Trying to cut down
Precontemplative, does not want to set date, will try to decrease number of cigarettes for next visit by 1/2.
Assist Statements addressing commitment to a method to achieve quitting (ordering, planning or provision of information relating to smoking cessation medications) Plan quit date 3/8/15. 800-778-8440 call smoker's helpline Vietnamese. Use Nicotine 21 mg/24 hr daily × 6 weeks #42, then 14 mg/24 hr daily × 6 weeks, then 7 mg/24 hr daily × 6 weeks …
Arrange Statements document specific plans for follow-up with a patient's effort to quit Tobacco smoking cessation discussed … He is to schedule a follow-up visit 2 to 3 months
Values† Demographics Male 47 (100) Ethnicity Vietnamese 29 (61.7) Korean 18 (38.3) Age, years <50 9 (19.1) 50 to 59 17 (36.2) >60 21 (44.7) Married 31 (66.0) Lived in United States <15 years 17 (36.2) Education < High school 21 (44.6) Graduated high school or beyond 16 (55.3) Income (% of federal poverty level) 100% to 200% 24 (51.1) <100% 11 (23.4) Unknown 12 (25.5) Health status Self-rated health Fair to poor 34 (72.3) Tobacco-related diseases‡ Hypertension 27 (57.4) Diabetes 11 (23.4) COPD 10 (21.3) Others (CVD, stroke, or cancer) 6 (12.7) Behavioral health conditions‡ Depression 13 (27.7) Anxiety disorders (including PTSD) 9 (19.1) Others (alcohol use or sleep disorders) 5 (10.6) Smoking status and history Number of cigarettes smoked per day, mean (SD) 9.3 (4.5) Time to first cigarette after waking Within 30 minutes 33 (70.2) >30 minutes 14 (29.8) Years smoked regularly >10 years 3 (6.4) 11 to 20 years 3 (6.4) >20 years 41 (87.2) Intended to quit in the next 6 months 22 (46.8) Had 24-hr quit attempt past year 18 (38.3) Attempted to quit in the past year 28 (59.6) COPD, chronic obstructive pulmonary disease; CVD, cardiovascular disease; PTSD, posttraumatic stress disorder; SD, standard deviation.
↵* Column percent for mutually exclusive categories may not be summed to 100% due to rounding.
↵† Values are n (%) except where indicated.
↵‡ Participants may endorse one or more categories for tobacco-related diseases, and behavioral conditions.
- Table 3.
Feasibility and Acceptability Outcomes of Interactive Mobile Doctor Intervention (N = 47)*
Values† Feasibility Measures Length of iMD administration (minutes) Mean (SD) 12.9 (3.7) Range 10 to 25 Needed staff assistance during administration No assistance needed 30 (63.8) Once 17 (36.2) More than once 0 (0.0) Completion of iMD prior to seeing PCP Yes 45 (95.8) No 2 (4.2) Acceptability Measures Please tell us what you think of the length of the video intervention? Would you say the length was… Too long 0 (0.0) Just right 46 (97.9) Too short 1 (2.1) What did you think of the messages from the videos? Were they… Too difficult to understand 0 (0.0) Somewhat difficult to understand 1 (2.1) Not too difficult to understand 6 (12.8) Quite easy to understand 40 (85.1) How helpful or not helpful do you think the video program was in your decision about quitting cigarettes? Not at all helpful 1 (2.1) Somewhat helpful 5 (10.6) Moderately helpful 13 (27.7) Very helpful 28 (59.6) In terms of enhancing the quality of the communications between you and your doctor in the clinic visit you just had, how helpful or not helpful do you think the video program was… Not at all helpful 1 (2.1) Somewhat helpful 5 (10.6) Moderately helpful 6 (12.8) Very helpful 35 (74.5) iMD, Interactive Mobile Doctor; PCP, primary care provider; SD, standard deviation.
↵* Feasibility data were obtained by research staff's observation. Acceptability data were obtained by participants' self-report from an in-person assessment immediately after the primary care visit after the iMD administration.
↵† Values are n (%) except where indicated.
- Table 4.
Multivariable Logistic Model Results for Electronic Health Record-Documented Outcomes*
EHR-Documented Outcomes Time Points† Intervention Visit AOR (95% CI), P Value Postintervention Visit AOR (95% CI), P Value Ask 2.26 (0.94–5.46), .07 1.49 (0.62–3.57), .37 Advise 1.44 (0.66–3.13), .36 1.44 (0.54–3.79), .47 Assess 4.49 (1.62–12.49), .004 3.34 (1.32–8.44), .01 Assist 17.63 (4.67–66.57), < .001 2.02 (0.54–7.56), .30 Arrange 10.28 (2.92–36.23), < .001 1.80 (0.44–7.39), .42 AOR, adjusted odds ratio; EHR, electronic health record; 95% CI, 95% Confidence Interval.
↵* All models used generalized estimating equations (GEE) to adjust PCP clusters. Multivariable logistic regression models included the following as covariates: ethnicity (Korean vs. Vietnamese), age (<60 vs 60 or older), education (<high school vs. high school or beyond), presence vs. absence of a tobacco-related disease condition (hypertension, diabetes, chronic obstructive pulmonary disease, cardiovascular diseases, stroke, or cancer), and number of cigarettes smoked per day (<10 vs 10 or more). Bold text denotes significant AOR, 95% CI, and P-value (P < 0.05).
↵† Referent is preintervention visit. Three time points were included in this study: (1) at preintervention, one primary care (PCP) visit prior to the intervention; (2) intervention visit with participants receiving the interactive Mobile Doctor (iMD) intervention; and (3) at postintervention, one PCP visit after the intervention visit.




{kind=link}
{kind=link}
{kind=link}