
Article Figures & Data
Figures
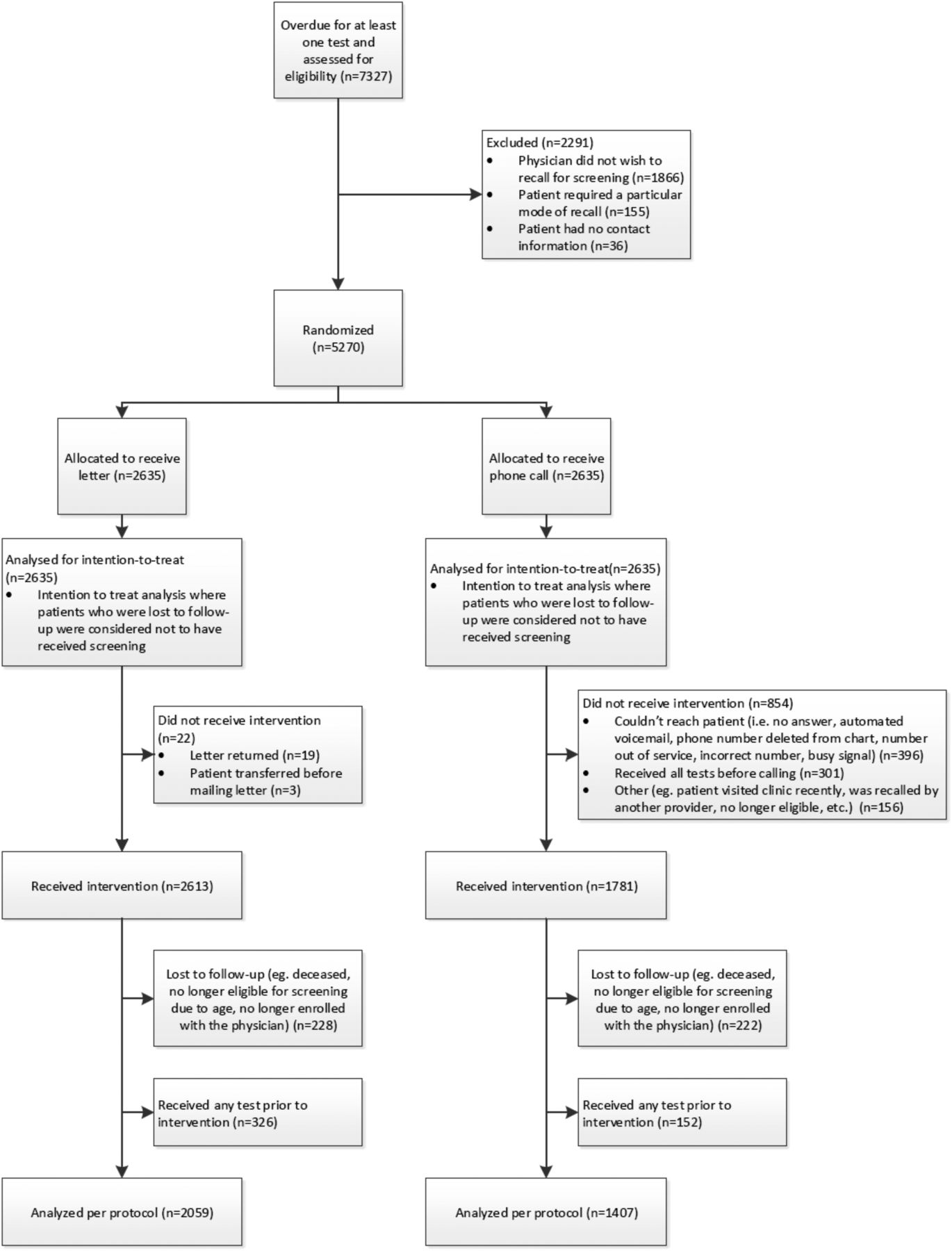
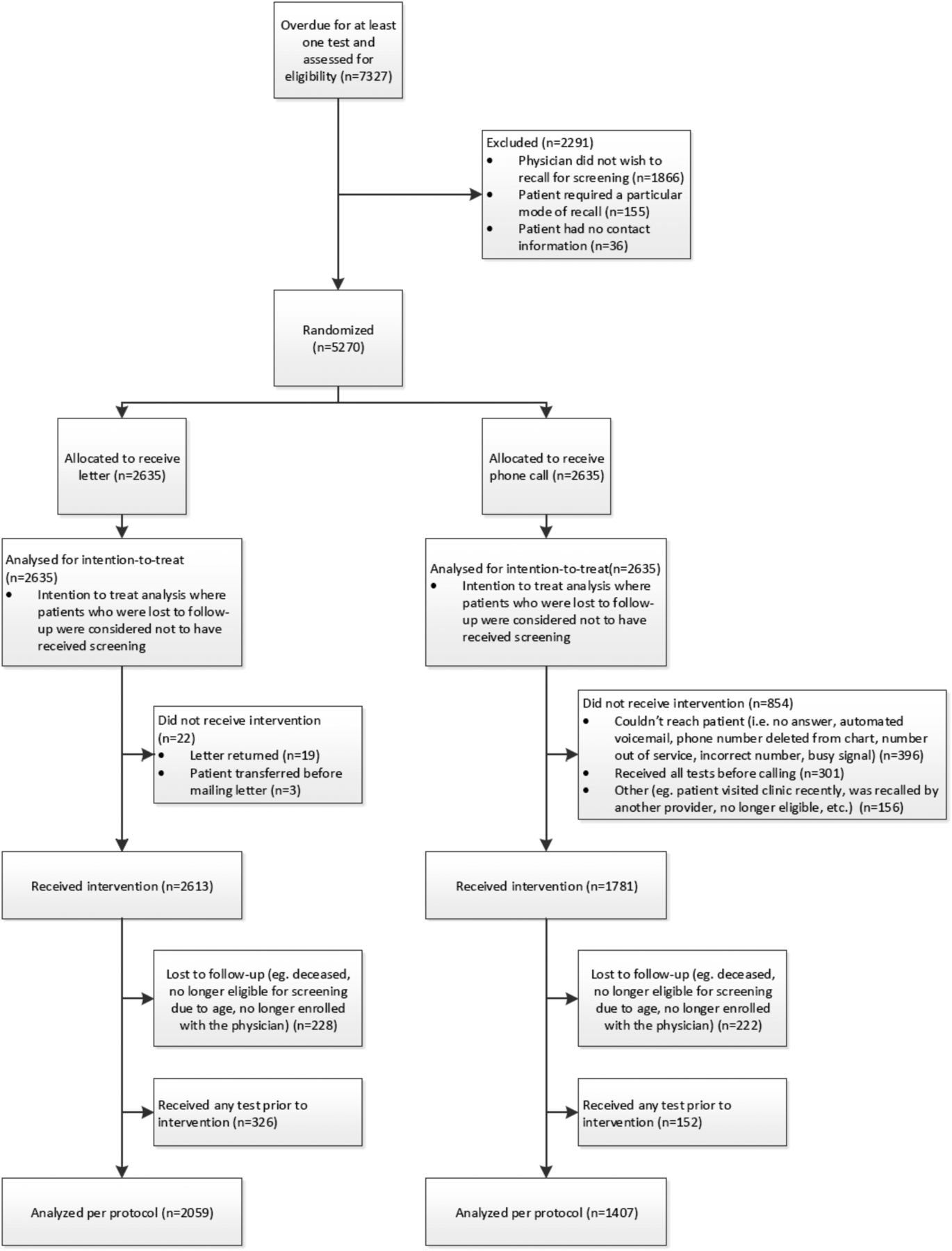
- Figure 1.
Summary of patients randomized and included in intention-to-treat and per protocol analysis.

Tables
- Table 1.
Baseline Characteristics of Patients Randomized to Receive a Reminder Letter or Phone Call as of March 31, 2015
Patient Characteristics Female Male Randomized to Receive Letter (n = 1896) Randomized to Receive Phone Call (n = 1837) P value† Randomized to Receive Letter (n = 739) Randomized to Receive Phone Call (n = 798) P Value† Age, years [n (column %)] 21 to 29 214 (11.3) 190 (10.3) .3225 — — .5404 30 to 39 353 (18.6) 380 (20.7) — — 40 to 49 317 (16.7) 271 (14.8) — — 50 to 59 558 (29.4) 565 (30.8) 487 (65.9) 516 (64.7) 60 to 69 357 (18.8) 335 (18.2) 195 (26.4) 228 (28.6) 70 to 74 97 (5.2) 96 (5.2) 57 (7.7) 54 (6.8) Income quintile [n (column %)] Q1 (lowest) 504 (28.6) 480 (27.9) .3449 198 (29.3) 236 (32.2) .6854 Q2 304 (17.2) 321 (18.6) 110 (16.3) 116 (15.9) Q3 288 (16.3) 305 (17.7) 124 (18.3) 119 (16.3) Q4 278 (15.8) 277 (16.1) 116 (17.1) 117 (16.0) Q5 (highest) 390 (22.1) 340 (19.7) 129 (19.1) 144 (19.7) Missing 132 114 62 66 Overdue for cancer screening [n (column %)] Pap test only 1036 (54.6) 967 (52.6) .7235 — — n/a Mammogram only 190 (10.0) 175 (9.5) — — CRC screen only 214 (11.3) 214 (11.7) 739 (100) 798 (100) Pap test and mammogram 62 (3.3) 75 (4.1) — — Mammogram and CRC screen 171 (9.0) 181 (9.9) — — Pap test and CRC screen 62 (3.3) 65 (3.5) — — Pap test, mammogram, CRC screen 161 (8.5) 160 (8.7) — — ↵† χ2 test.
CRC, colorectal cancer.
- Table 2.
Outcomes 6-Months Postintervention (Intention-to-Treat Analysis), Female Patients
Outcomes* No./Total No. (%) Absolute Difference, % (95% CI) P Value† Reminder Letter (n = 1896) Reminder Phone Call (n = 1837) Patients who received at least one screening test for which they were due 626/1896 (33.0) 756/1837 (41.2) 8.1 (5.1–11.2) <.001 Patients overdue for a Pap test who received a Pap test 386/1321 (29.2) 479/1267 (37.8) 8.6 (5.0–12.2) <.01 Patients overdue for a mammogram who received a mammogram 138/584 (23.6) 164/591 (27.8) 4.1 (−0.9 to 9.1) .106 Patients overdue for CRC screening who received a CRC screen 156/608 (25.7) 186/620 (30.0) 4.3 (−0.7 to 9.4) .090 Patients overdue for CRC screening who receive an FOBT 123/608 (20.2) 163/620 (26.3) 6.1 (1.4–10.8) .012 Patients overdue for CRC screening who receive a colonoscopy 41/608 (6.7) 30/620 (4.8) −1.9 (−4.5 to 0.7) .153 ↵* Patients in the phone call arm who did not receive the intervention but were up to date with screening at the time of outcome ascertainment were only considered screened if they received the screening test within 6 months of the date that letters were sent.
↵† χ2 test.
CI, confidence interval; CRC, colorectal cancer; FOBT, fecal occult blood test.
Outcomes* No./Total No. (%) Absolute Difference, % (95% CI) P Value† Reminder Letter (n = 739) Reminder Phone Call (n = 798) Patients overdue for CRC screening who received a CRC screen 183/739 (24.8) 230/798 (28.8) 4.1 (−0.4 to 8.5) .073 Patients overdue for CRC screening who receive an FOBT 156/739 (21.1) 198/798 (24.8) 3.7 (−0.5 to 7.9) .085 Patients overdue for CRC screening who receive a colonoscopy 34/739 (4.6) 41/798 (5.1) 0.5 (−1.6 to 2.7) .625 ↵* Patients in the phone call arm who did not receive the intervention but were up to date with screening at the time of outcome ascertainment were only considered screened if they received the screening test within 6 months of the date that letters were sent.
↵† χ2 test.
CRC, colorectal cancer; CI, confidence interval; FOBT, fecal occult blood test.
Outcomes No./Total No. (%) Absolute Difference, % (95% CI) P Value* Reminder Letter (n = 1459) Reminder Phone Call (n = 977) Patients who received at least one screening test for which they were due 370/1459 (25.4) 395/977 (40.4) 15.1 (11.3–18.9) <.001 Patients overdue for a Pap test who received a Pap test 241/1029 (23.4) 269/653 (41.2) 17.8 (13.2–22.4) <.001 Patients overdue for a mammogram who received a mammogram 72/441 (16.3) 72/315 (22.9) 6.5 (3.0–12.3) .024 Patients overdue for CRC screening who received a CRC screen 84/464 (18.1) 81/339 (23.9) 5.8 (0.1–11.5) .045 Patients overdue for CRC screening who receive an FOBT 69/464 (14.9) 72/339 (21.2) 6.4 (0.9–11.8) .019 Patients overdue for CRC screening who receive a colonoscopy 18/464 (3.9) 14/339 (4.1) 0.3 (−2.5 to 3.0) .858 ↵* χ2 test.
CRC, colorectal cancer; CI, confidence interval; FOBT, fecal occult blood test.
Outcomes No./Total No. (%) Absolute Difference, % (95% CI) P Value* Reminder Letter (n = 600) Reminder Phone Call (n = 430) Patients overdue for CRC screening who received a CRC screen 109/600 (18.2) 105/430 (24.4) 6.3 (1.2–11.4) .015 Patients overdue for CRC screening who receive an FOBT 98/600 (16.3) 92/430 (21.4) 5.1 (0.2–9.9) .039 Patients overdue for CRC screening who receive a colonoscopy 16/600 (2.7) 16/430 (3.7) 1.1 (−1.2 to 3.3) .336 ↵* χ2 test.
CRC, colorectal cancer; CI, confidence interval; FOBT, fecal occult blood test.
- Table 6
Logistic Regression Results Examining the Effect of Income Quintile on the Likelihood of Patients Receiving at Least 1 Screening Test for Which They Were Due Within 6-Months Postintervention (Intention-to-Treat Analysis), Adjusted for Age, Female Patients
Income Quintile Subgroup No. of patients No./Total No. (%) Odds Ratio (95% CI) P value for Interaction Reminder Letter and Received at Least 1 Screening Test for Which They Were Due Reminder Phone Call and Received at Least 1 Screening Test for Which They Were Due Q1 (lowest) 984 152/504 (30.2) 191/480 (39.8) 1.53 (1.17–2.00) .9871 Q2 625 100/304 (32.9) 128/321 (39.9) 1.36 (0.97–1.89) Q3 593 99/288 (34.4) 127/305 (41.6) 1.33 (0.95–1.86) Q4 555 114/278 (41.0) 115/277 (41.5) 1.02 (0.73–1.43) Q5 (highest) 730 121/390 (31.0) 150/340 (44.1) 1.73 (1.28–2.36) CI, confidence interval.
- Table 7.
Logistic Regression Results Examining the Effect of Income Quintile on the Likelihood of Patients Receiving at Least 1 Screening Test for Which They Were Due within 6-Months Postintervention (Intention-to-Treat Analysis), Adjusted for Age, Male Patients
Income Quintile Subgroup No. of patients No./Total No. (%) Odds Ratio (95% CI) P Value for Interaction Reminder Letter and Received at Least 1 Screening Test for Which They Were Due Reminder Phone Call and Received at Least 1 Screening Test for Which They Were Due Q1 (lowest) 434 52/198 (26.3) 65/236 (27.5) 1.08 (0.71–1.66) .7118 Q2 226 29/110 (26.4) 32/116 (27.6) 1.06 (0.59–1.91) Q3 243 23/124 (18.5) 32/119 (26.9) 1.62 (0.88–2.97) Q4 233 30/116 (25.9) 36/117 (30.8) 1.26 (0.71–2.24) Q5 (highest) 273 37/129 (28.7) 45/144 (31.3) 1.14 (0.68–1.91) CI, confidence interval.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Recommandations pour des soins preventifs pour promouvoir lequite en matiere de sante
- Preventive care recommendations to promote health equity
- Feasibility of a multifaceted implementation intervention to improve attendance at diabetic retinopathy screening in primary care in Ireland: a cluster randomised pilot trial
- Practice-based Research Network (PBRN) Engagement: 20+ Years and Counting