
Abstract
Diversification of the physician workforce has been a goal of Association of American Medical Colleges for several years and could improve access to primary care for under-served populations and address health disparities. We found that family physicians' demographics have become more diverse over time, but still do not reflect the national demographic composition. Increased collaboration with undergraduate universities to expand pipeline programs may help increase the diversity of students accepted to medical schools, which in turn should help diversify the family medicine workforce.
Racial and ethnic minority physicians are important for the delivery of primary care to underserved populations.1 Physicians from underrepresented minority populations are more likely than white physicians to practice primary care in impoverished areas and in regions experiencing physician shortages2; however, a significant gap exists between the racial and ethnic composition of the general population and primary care physicians, family medicine faculty, and family medicine residents.2⇓–4 Diversification of the physician workforce has been a goal of Association of American Medical Colleges for several years4 and could improve access to primary care for underserved populations and address health disparities.5 Our objectives were to assess how well the racial and ethnic composition of American Board of Family Medicine (ABFM) diplomates (a proxy for the family medicine workforce) mirrors the national population and to determine trends by year of initial certification.
We aggregated racial and ethnic demographic data provided by family physicians during their application for the ABFM Family Medicine Certification Examination from 2013 to 2017 and calculated the percentage of each category by year of initial certification. Examinees were asked to select one race category from the following options: American Indian or Alaska Native, Asian, black or African American, Native Hawaiian or other Pacific Islander, or white. A response option of Other was added in 2017 but was omitted from this analysis. They were also asked to select one ethnicity between either non-Hispanic or Hispanic or Latino. We then compared the racial/ethnic composition of this sample to estimates of the US population by using July 1, 2017, data from the US Census Bureau.6
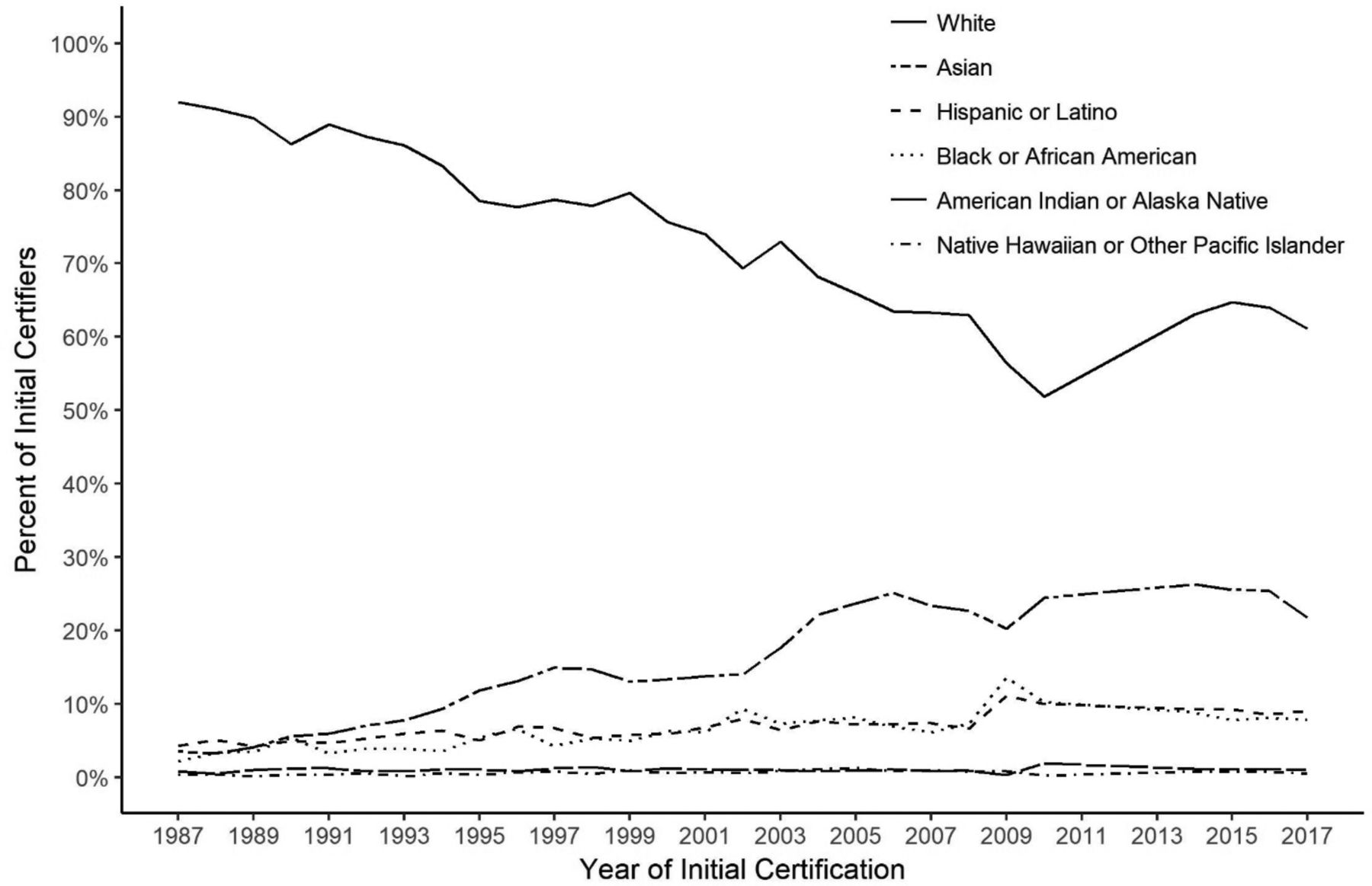
Data aggregation resulted in matching 66,542 board certified family physicians by their year of initial certification, which ranged from 1987 to 2017. Compared with the US population, ABFM diplomates are more likely to be Asian (21.8% vs 5.7%) or Native Hawaiian or other Pacific Islander (0.5% vs 0.2%) and less likely to be Black or African American (7.8% vs 13.3%), American Indian or Alaska Native (1.0% vs 1.3%), or Hispanic or Latino (9.1% vs 17.8%). Non-Hispanic white diplomates are generally representative of the US population (61.2% vs 61.3%). The group trends for the past 30 years (1987 to 2017) in Figure 1 show the percentage of Black or African American physicians increasing from 1.3% to 7.8% and Hispanic or Latino physicians increasing from 2.3% to 9.1%. However, both groups remain substantially underrepresented compared with the general population.
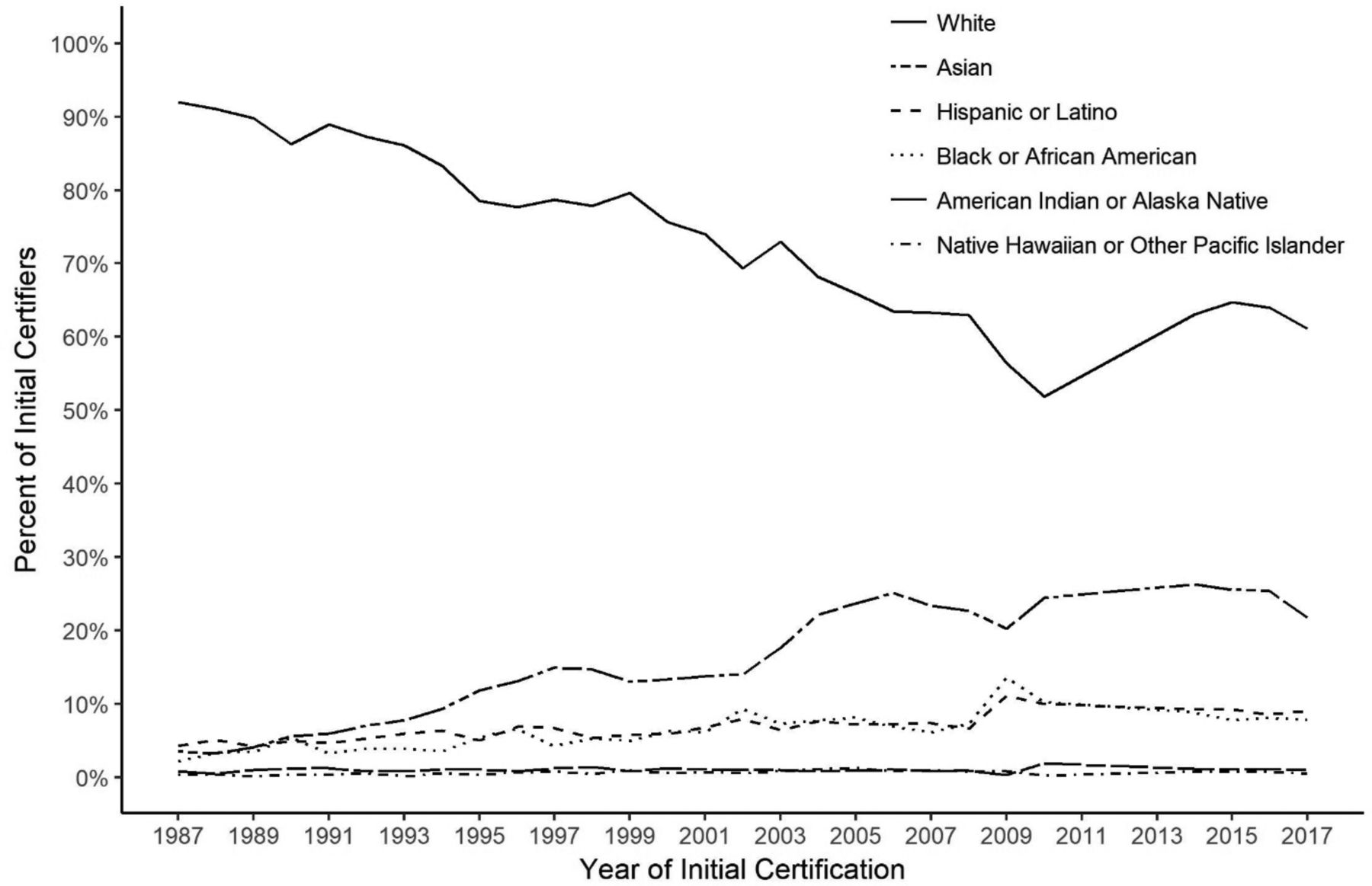
Proportion of board certified family physicians by group and year of initial certification since 1987.
Our results indicate that efforts to increase diversity seem to have been effective for some groups but not all. Black or African Americans and Hispanics, in particular, have struggled to reach a mark representative of the US population. Although family medicine may have the most proportionate distribution of physicians to the general population,2 the specialty still feels the effects of a lack of diversity at the undergraduate medical education level. Medical schools should work more closely with their associated universities to increase the number of underrepresented minorities applying to medical school and ensure that these students are appropriately prepared for the rigors of medical school. Increasing the number of pipeline programs (e.g., Health Careers Opportunities Program) may help to recruit a more diverse medical school applicant pool, which in turn should help diversify the family medicine workforce.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: MP, AE, and RP are employees of the American Board of Family Medicine.
To see this article online, please go to: http://jabfm.org/content/31/6/842.full.
- Received for publication April 26, 2018.
- Revision received June 21, 2018.
- Accepted for publication June 25, 2018.
In this issue




{kind=link}
Related Articles
Cited By...
- Family Physicians' Barriers and Facilitators in Incorporating Medication Abortion
- Racial/Ethnic Representation Among American Board of Family Medicine Certification Candidates from 1970 to 2020
- Informing Equity & Diversity in Primary Care Policy and Practice: Introducing a New Series of Policy Briefs, Commentaries, and Voices in JABFM
- The American Board of Family Medicine's 8 Years of Experience with Differential Item Functioning
- Content Usage and the Most Frequently Read Articles of 2018
- Slow Progress and Persistent Challenges for the Underrepresented Minority Family Physician