
Abstract
Introduction: Emerging policy consensus advocates that patient-centered care should include an active, practice-level patient role, but it is unknown how commonly these roles are implemented. We sought to understand current prevalence and predictors of practice-level patient engagement in US primary care settings.
Methods: We assessed practice-level patient engagement by using 2016 American Board of Family Medicine Certification Examination registration data, restricted to ambulatory primary care site respondents randomly selected for a patient-centered medical home (PCMH) question module. Multivariate logistic regression models identified predictors of high-intensity patient engagement, defined as a patient advisory council or patient volunteers in quality improvement activities.
Results: A total of 6900 examinees reported practicing in primary care sites; 1368 randomly received PCMH questions. Practice-level patient engagement included patient surveys (76.5%; 95% CI, 74.3–78.8%), patient suggestion boxes (52.9%; 95% CI, 50.2–55.5%), patient board of director memberships (18.8%; 95% CI, 16.7–20.9%), patient advisory councils (23.8%; 95% CI, 21.5–26.0%), and patient participation in quality improvement (20.5%; 95% CI, 18.3–22.6%). High-intensity patient engagement was reported by 31.1% (95% CI, 28.7–33.6%); predictors included large practice size (OR, 3.30; 95% CI, 1.96–5.57), serving more vulnerable patient populations, (OR, 1.83; 95% CI, 1.18–2.84) and PCMH certification (OR, 2.19; 95% CI, 1.62–2.97).
Conclusions: Nearly one-third of physicians reported working in settings with high-intensity practice-level patient engagement. An implementation science approach should examine why high-intensity activities are more common in some practice settings and whether these activities add value through improved patient experience and health outcomes.
- Family Physicians
- Logistic Regression
- Patient-Centered Care
- Patient Engagement
- Quality Improvement
- Surveys and Questionnaires
Patient engagement is the active partnership of patients, families, and caregivers with health care clinicians and staff to improve health care delivery on the individual, organizational, and policy level.1 Although engaging patients in their own personal health care has gained traction in primary care, less focus has been given to patient engagement at the organizational level. Patient engagement at the organizational level of a primary care clinic or practice has been a requirement for Federally Qualified Health Centers (FQHCs) since the 1970s, when FQHCs were mandated to have at least 51% patient membership on their boards of directors.
The advent of the patient-centered medical home (PCMH) movement and accountable care organizations (ACOs) is stimulating broader interest in patient engagement on the organizational level, including outside FQHC settings. As part of its PCMH application process, the National Committee for Quality Assurance offers elective credits for establishing patient advisory councils and for involving patients, family, or caregivers in quality improvement (QI) activities.2
Patient participation on an advisory board is also a requirement for Medicare ACOs and some state Medicaid ACOs.3,4 The Comprehensive Primary Care Initiative (CPC) from the Center for Medicare & Medicaid Innovation as well as its successor CPC Plus, are 2 national experiments of primary care practice transformation among over 500 clinics and include a component of patient and family engagement, evaluations of which are currently underway.5 Consumer advocates assert that involving patients as partners in practice improvement is essential for the delivery of high-quality patient-centered care.6
Despite a groundswell of policies and incentives for patient engagement, very little is known about the degree to which primary care physicians in the United States have implemented patient engagement strategies at the practice level. Prior research has been limited to practices that are FQHCs or formally certified as PCMHs.7,8 Factors such as FQHC requirements for patient participation in governing boards and PCMH scoring systems that award credit for patient engagement are likely to make patient engagement strategies more prevalent at these settings than in other contexts. Concerns have been voiced about the feasibility of implementing patient engagement strategies in small independent practices, especially by using strategies such as patient advisory councils that require considerable resources to implement and sustain. The historic emphasis on patient engagement at the practice level by FQHCs also raises questions about whether this type of patient engagement is more common among practices serving vulnerable populations.
No study to date has investigated patient engagement at the practice level in a nationally representative sample of family physicians. We seek to answer questions about the prevalence of patient engagement: What proportion of family physicians work in practices that have adopted practice-level patient engagement strategies? What types of engagement strategies are the most prevalent? To what extent are practices using more intensive patient engagement strategies, such as patient advisory councils? We also seek to answer questions about predictors of high-intensity patient engagement: How are PCMH recognition and implementation of other PCMH subcomponents associated with the use of intensive practice-level patient engagement strategies? Are practices serving a high proportion of vulnerable patients more likely to invest in patient engagement, independent of whether the practice is designated as an FQHC? Answers to these questions are important both for understanding the current degree of diffusion of practice-level patient engagement strategies in primary care and for targeting interventions to promote greater patient engagement. The scope of this work exclusively focuses on organizational-level patient engagement, not individual-level patient care.
Methods
Study Population and Data Source
The study population included all practicing family physicians who registered for either the spring or fall 2016 American Board of Family Medicine (ABFM) Family Medicine Certification examination. If the same individual registered for both dates, only data from the Fall registration were retained for analysis. The ABFM requires all physicians when registering for the examination, 3 to 4 months before the examination day, to complete a questionnaire, which includes items on physician demographics and practice settings. For this study, we excluded respondents who did not report working in an ambulatory practice.
To explore our primary outcome, we used a survey question that asked all registrants to report activities related to patient engagement in practice improvement at their primary clinical site. In addition, registrants completed 1 of 5 randomly assigned question modules on specific topic areas, one of which focused on PCMH activities. Questions in the PCMH module sought to obtain information regarding the practice's QI processes, enhanced access strategies, and mental health provider integration. Our analysis focused on board examinees who were randomly assigned to the PCMH module, although we also examined prevalence estimates for the entire ambulatory sample. All questions analyzed are included as an appendix.
Analytic Model
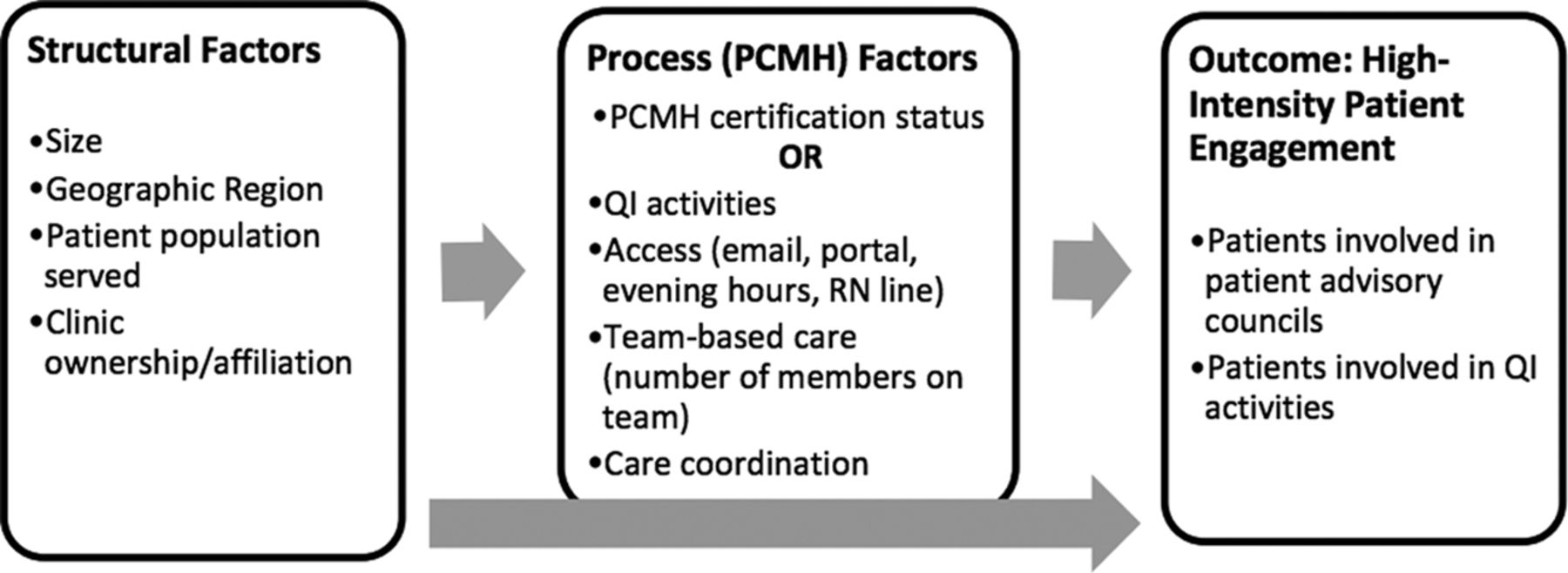
Similar to prior research on predictors of practice-level patient engagement8 and Donabedian's quality framework,9 we constructed an analytic model of structural factors (organizational traits) and process factors (PCMH implementation) hypothesized to be associated with the practice-level patient engagement outcomes (see Figure 1). We constructed this model a priori and included variables that were available from the dataset that corresponded to these factors. We hypothesized that structural attributes, such as a larger practice group or FQHC setting, would provide greater support for a practice to invest in high patient engagement. We hypothesized that geographic region may correspond to regional differences in funding for primary care that would support patient engagement. We also hypothesized that, independent of these structural characteristics, physicians working in PCMH-certified clinics would report higher levels of practice-level patient engagement.

Conceptual Model of structure, process, and outcome factors. PCMH, patient-centered medical home; QI, quality improvement.
Organizational Traits (Structure)
Structural/organizational traits assessed included practice size (small, medium, or large size practices), practice ownership type (Health care Maintenance Organization, FQHC, academic practice, other), geographical region (Western, Midwest, Northeast, and Southern), and self-reported percentage of vulnerable patients served (categorized as <10%, 10% to 50%, and >50%).
Patient-Centered Medical Home Features (Processes)
We used 2 different approaches to capture the presence of PCMH-related processes. The first was self-reported PCMH accreditation status (not applying, applying, or accredited). The second examined responses to more detailed items about specific practice features corresponding with the Agency for Health care Quality and Research's model of PCMH attributes: team-based care, care coordination, patient access, and QI.10 We defined team-based care as an ordinal sum of the number of different disciplines reported as part of the care team (nurse practitioner, registered nurse, licensed practical nurse, physician's assistant, behaviorist, social worker, and pharmacist). We defined care coordination as the presence of a care coordinator on-site. We defined patient access as an ordinal variable capturing the number of practice features that improve patient access including capacity for patients to email their provider, expanded or extended office hours, providing telephone medical advice, or having an online patient portal. We defined QI as an ordinal variable, including having personally participated in a QI project in the past year, agreement that providers participate in QI collaboratives at their site, agreement that providers are given regular performance feedback on chronic disease management, and that providers regularly use decision support tools for chronic disease care. We conducted principal component analysis and assessed Cronbach α scores, which confirmed our variable selection and construction of 4 PCMH subcomponents (see Appendix).
Practice-Level Patient Engagement (Outcome)
Physicians were asked whether their practice used distinct types of patient engagement activities. The survey item question asked “How do you, or your office practice, involve patients who are seen in your clinical site, or their families and caregivers, in practice improvement?” Response options included the following: suggestion boxes, patient or family/caregiver surveys, participation on a governing board, participation on an advisory group dedicated to practice improvement (separate from a governing board), and participation as volunteers or workers on specific practice improvement projects. Response categories were “yes,” “no,” or “do not know” for each activity. Answers of “do not know” were recoded to “no” with the assumption that providers would have awareness of the patient engagement activity if it were implemented in a meaningful way. The item was adapted from an instrument used in a prior cross-sectional survey assessing patient engagement.11
We dichotomized patient engagement activities as “low” or “high-intensity” patient engagement adapted from precedent research7 and the Carman conceptual framework1 that depicts patient engagement activities as a continuum spanning from unidirectional, consultative activities to more active, shared partnerships. We defined “high-intensity” patient engagement as the more active, complex, bidirectional partnership with patients, which included patient advisory council or patients involved in QI projects. We defined “low-intensity” patient engagement as more unidirectional, consultative activities, including patient surveys, comment boxes, or none of any of the patient engagement activities.1,7 The categorization of “lower intensity” is not meant to devalue this form of patient engagement, but rather to distinguish the level of complexity of the patient interaction. We included a question assessing patient participation in a governing board to distinguish between governing board participation (required at FQHCs) and participation in a patient advisory council. Board of directors were not included in our definition of “high-intensity” patient engagement based on our prior qualitative research that showed that FQHC board of director tasks are typically limited to financial and human resources governance decisions rather than practice redesign or QI.12
Data Analyses
We reviewed summary statistics for each predictor and tested whether respondents who answered the PCMH module differed from other respondents by individual and practice-level demographics. We tested if the prevalence of high-intensity patient engagement differed by practice characteristics by using χ2 and t tests. We confirmed that all pairwise correlations between predictors were below r = 0.4 to avoid concerns about collinearity. We conducted multivariate logistic regression to identify predictors of high patient engagement by using all structural and process variables we hypothesized a priori to predict high patient engagement. We calculated goodness of fit of our logistic regression model by using the Hosmer-Lemeshow test.13
Sensitivity Analyses
We compared prevalence estimates and associations with predictor variables between analyses by using the entire sample of respondents in ambulatory practice and the subgroup of respondents who participated in the module assessing PCMH factors.
Geocoding of respondent addresses indicated that some respondents may have been practicing at the same location as one or more of the other respondents in the data set. Because our research question focused on patient engagement at the practice level, we conducted a sensitivity analysis by rerunning our analyses after retaining only one response randomly selected from each potential duplicate pairing or clustering by practice site.
Analyses were conducted using Stata (version 13.1).14 This study was reviewed by the University of California, San Francisco, Institutional Review Board (protocol no. 15–18468) and designated “Not Human Subjects Research,” as it was a secondary analysis of deidentified data.
Results
There were 6900 respondents practicing in ambulatory sites, of which 1368 were randomly assigned the module of PCMH-related questions. Because the survey is a required component of the ABFM examination registration process, there was a 100% response rate. The mean age of respondents in the PCMH module subsample was 51.4 years and 41.6% identified as female (Table 1). For self-reported race, 74.9% reported White, 15.2% Asian, 5.8% African-American, and 5.6% Hispanic/Latino. Most respondents reported practicing at either small (2 to 5 providers, 38.0% of respondents) or medium-sized practices (6 to 20 providers, 32.4% of respondents). The majority (55.0%) reported working in practices owned as private/solo/group practices (vs hospital, Health care Maintenance Organization, FQHC, academic, or other ownership). There was a relatively even spread across geographic region, and a majority (56.7%) reported working in sites serving 10% to 50% vulnerable populations.
Demographic Differences between Low and High Patient Engagement (Unadjusted, Raw Percentages), Restricted to Respondents in Ambulatory Care Who Responded to Patient-Centered Medical Home Survey Module
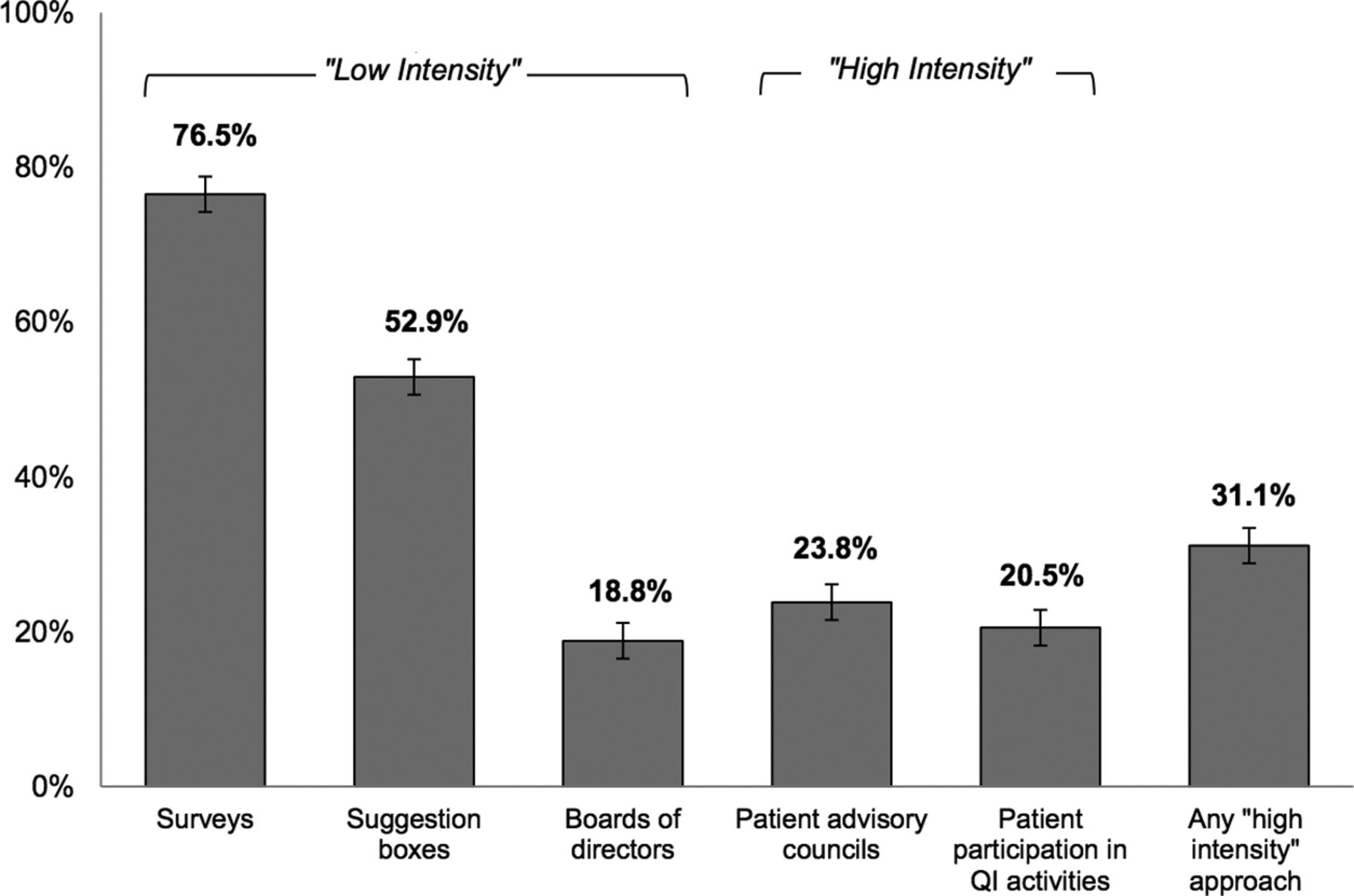
Among the 1368 participants of the PCMH module, respondents reported practice-level patient engagement through patient surveys (76.5%; 95% CI, 74.3–78.8%), patient suggestion boxes (52.9%; 95% CI, 50.2–55.5%), patient membership on clinic board of directors (18.8%; 95% CI, 16.7–20.9%), patient advisory councils (23.8%; 95% CI, 21.5–26.0%), and patient participation in QI activities (20.5%; 95% CI, 18.3–22.6%) (Figure 2). Approximately one-third of subgroup respondents (31.1%; 95% CI, 28.7–33.6%) reported that their practice used high-intensity patient engagement, defined as having patients serve on advisory councils and/or as volunteers in QI activities.

Percent of ambulatory primary care respondents reporting practice-level patient engagement activities. QI, quality improvement.
Among respondents working in PCMH-certified practices, 58.5% reported high-intensity patient engagement activities at their site, compared with 22.1% among practices that are not PCMH certified or applying (P < .001). The prevalence of patient engagement activities differed by less than 1% in the overall ambulatory sample (N = 6900) compared with responses from the subset of respondents assigned to answer questions in the PCMH module (see Appendix), confirming that the subgroup was representative of the entire ambulatory sample.
Our multivariate regression models examined structural and process predictors of practice-level patient engagement; one model incorporated PCMH certification status as the process predictor and the other model incorporated PCMH subcomponents (Table 2). Key practice-level predictors of high-level patient engagement included larger practice sizes of 20 or more clinicians (OR, 3.30; 95% CI, 1.96–5.57 compared with solo practitioners) and practices serving vulnerable populations (OR, 1.77; 95% CI, 1.29–2.43 for practices serving 10% to 50% vulnerable populations and OR, 1.83; 95% CI, 1.18–2.84 for practices serving >50% vulnerable populations). Practice size and proportion of vulnerable patients served were significant predictors when holding all other variables constant, including practice ownership, geographic region, and PCMH characteristics. Associations were consistent whether controlling for PCMH accreditation status (Model 1) or PCMH subcomponents (Model 2).
Predictors of High-Intensity Patient Engagement
Physicians in PCMH practices or those applying for PCMH certification had a higher odds of reporting high-intensity patient engagement at the practice level (OR, 2.19; 95% CI, 1.62–2.97 and OR, 1.66; 95% CI, 1.16–2.36, respectively) than those in practices not applying, even when adjusted for potential confounders such as practice ownership, proportion of clinic population belonging to vulnerable populations, and geographic region.
When investigating specific PCMH subcomponents for their relationship with high intensity patient engagement, the presence of care coordination (OR, 1.75; 95% CI, 1.28–2.39) and QI activities (OR, 1.56; 95% CI, 1.34–1.81) were significant predictors of high-intensity patient engagement. Neither the size of the multidisciplinary care team nor the number of patient access strategies (such as advanced access hours or an email portal) were statistically significant predictors. We did not observe a consistent relationship between high-intensity patient engagement and specific geographic regions, nor a consistent relationship between high-intensity patient engagement and practice ownership.
Results from our sensitivity analysis comparing regression results for the entire sample versus a single respondent from practices from which there were multiple respondents showed similar results, thus we did not exclude clustered responses from the same practice. Our analysis of Hosmer-Lemeshow goodness of fit of our regression models showed that all models performed with a P value greater than .05, suggesting a reasonable fit.
Discussion/Interpretation
This analysis provides the first cross-sectional view of how patient engagement activities are being implemented in family medicine practices across the United States. Prior assessments have focused solely on FQHCs8 or PCMH-certified sites.7 We found that almost one-third of practices have implemented high-intensity patient engagement, suggesting a shift from the “early adopter” to the “early majority” phase of Roger's Theory of Diffusion of Innovations.15 We can hypothesize that innovative patient engagement strategies provide some relative advantage to other practices, perhaps in association with PCMH accreditation and subsequent reimbursement or as a public relations strategy to advertise to consumers.16,17 There may be perceived operational advantages to patient engagement; our prior qualitative and empirical work suggest that patient engagement enhances QI activities, informs clinic priorities for new projects, and provides feedback so that current projects are more patient-accessible.18⇓–20
Our sample provides a snapshot of the phenotype of practices that are more likely to use high-intensity patient engagement. Practices that are further along in practice transformation and PCMH implementation are more likely to have patient advisory councils or patients involved in QI activities; however, it is unknown if organizational goals such as PCMH certification beget patient engagement or vice versa. It is conceivable that patient advisory councils are implemented in service of the long-term goal of developing more patient-centered clinics, which may also gain recognition as a PCMH. PCMH accreditation can result in additional funding for a clinic, which may provide financial incentives to support patient engagement or the actual resources to implement engagement strategies. However, our prior work has found that dedicated funding is not predictive of patient engagement,8and it is unknown what resources are being accessed to implement and sustain patient advisory councils and engage patients in practice improvement.
Physicians in larger practices were more likely to report high-intensity patient engagement. These findings are resonant with prior research demonstrating that small and medium-sized practices are less likely to engage in PCMH processes.21 Larger practices may benefit from more resources and opportunities to initiate and sustain patient engagement activities at the practice level. However, 28.2% of respondents reporting high-intensity patient engagement at their practice worked in practices of only 2 to 5 providers, indicating that some small practices are able to overcome barriers to implementation of high-intensity patient engagement strategies; perhaps these small sites are more nimble with less bureaucratic oversight and can more easily experiment with innovative patient engagement strategies.
We observed a relatively high prevalence of “lower-intensity,” unidirectional patient engagement strategies, such as patient surveys or installation of a suggestion box. A high percentage (76.5%) of respondents reported using patient surveys, which likely captures the widespread use of consumer experience surveys such as Consumer Assessment of Healthcare Providers and Systems Clinician & Group Survey or Press-Ganey surveys that are often required by health care organizations and can be a factor in pay-for-performance incentives.22 Half of the respondents reported the use of suggestion boxes, which is a relatively simple means to gain patient feedback on practice-level experiences. These lower intensity strategies may have more straightforward workflows to implement and are therefore easier to spread as a practice innovation. Almost 1 in 4 practices reported working with patient advisory councils (23.8%) and 1 in 5 involved patient volunteers in QI activities (20.5%).
Practice-level patient engagement activities seem to be more common in settings that serve a predominantly vulnerable patient population. Practices such as FQHCs and safety net clinics may have access to network-wide initiatives that prioritize and provide resources to support patient engagement for the underserved. In addition, medical staff and clinicians who commit to serve diverse and traditionally vulnerable patient populations may share a value system or ethical imperative to promote patient inclusion within practice-level improvement activities. Patient engagement may be especially important in clinics serving patients with lower health literacy, English proficiency, or socioeconomic status, as patient advisors can help illuminate specific barriers to care to improve access. Conversely, clinics serving more affluent populations with higher health-literacy may believe that their patients encounter fewer barriers to engaging in their care and may not see the need for higher-intensity patient engagement activities at the practice level.
Limitations
Because the data are cross-sectional, our analyses cannot confirm the direction of causality or the extent to which the activities reported are becoming more widespread over time. Our data were limited to family physicians who work in ambulatory care settings. Although the results may not be generalizable to other primary care specialties such as internal medicine and pediatrics, family physicians provide the majority of ambulatory care in the United States.23 The term “vulnerable populations” was not formally defined and may have been interpreted differently by respondents. Our data rely on self-report and we did not directly confirm the patient engagement strategies reported or assess their robustness or impact on the practice; further prospective or qualitative work could investigate this in more detail.
There is no evidence-based typology of patient engagement modalities; our definition of “high-intensity engagement” differs slightly from that used by others. We defined high-intensity patient engagement as having patient advisory councils and/or patient participation in QI, 2 examples of voluntary, bidirectional partnerships with practice leaders to develop and implement clinic policies and programs. Patient surveys, suggestion boxes, or board of directors can be important means of hearing patient voices. However, patient surveys and suggestion boxes are typically unidirectional and episodic forms of patient feedback, and patient membership on a governing board of directors usually takes place at a distance from activities organized by clinical teams.
Despite these limitations, our study has notable strengths. The ABFM dataset is one of the largest available samples of primary care physicians providing a representative cross-sectional survey of family physicians. Due to the requirements of the ABFM recertification process, this survey had a 100% response rate. The survey item captured a range of patient engagement activities, including both unidirectional and bidirectional activities. It also distinguished board of directors as a separate patient engagement activity, which are sometimes confused with patient advisory councils.
Conclusion
In this first nationally representative study of clinic-level patient engagement activities in the United States, we found not only a high prevalence of low-intensity, unidirectional modalities such as patient surveys but also that nearly one-third of family physicians report bidirectional, high-intensity patient engagement. Physicians practicing in larger clinics, clinics serving vulnerable populations, and clinics further along in PCMH transformation were more likely to implement high-intensity patient engagement activities, suggesting that the population served as well as resources available to a site may shape priorities for incorporating patient perspectives. Although primary care organizations are heeding the call for high-intensity patient engagement, such as patient advisory councils and patient participation in QI teams, there has not yet been a strong evidence base demonstrating its benefit. Additional research is needed to assess associations between clinic-level patient engagement activities and clinical performance measures. Future research should investigate adoption and implementation trends for practice-level patient engagement and assess if patient engagement at the practice-level leads to improvements in primary care quality and patient experience.
Acknowledgments
Thanks to the ABFM and Bo Fang, PhD, for data pull and data cleaning for this analysis.
Appendix
ABFM Recertification Survey: Survey Questions Analyzed
ABFM Patient Engagement Principal Components Analysis
Prevalence of Patient Engagement Activities in Entire ABFM Ambulatory Practice Sample (N = 6,900) Versus Those Who Completed Patient-Centered Medical Home Module (N = 1,368)
Notes
This article was externally peer reviewed.
Funding: AES's work was supported by the NRSA Award T32HP19025. MK's work was funded by the Kaiser Permanente National Community Benefit Fund of the East Bay Community Foundation 20152632.
KG and MBP are supported by the UCSF Clinical and Translational Science Institute (CTSI), part of the Clinical and Translational Science Award program funded by the National Center for Advancing Translational Sciences (Grant UL1 TR001872) at the National Institutes of Health (NIH).
Conflict of interest: Dr. Sharma has received honoraria for providing training webinars on the topic of patient engagement. Dr. Peterson is an employee of the American Board of Family Medicine. Dr. Grumbach is a core member of the AAFP Family Medicine for America's Health Patient Engagement Tactic Team. The other authors have no disclosures.
To see this article online, please go to: http://jabfm.org/content/31/5/733.full.
- Received for publication October 25, 2017.
- Revision received April 6, 2018.
- Accepted for publication April 23, 2018.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Comparative Analysis of Three Surveys on Primary Care Providers Experiences with Interoperability and Electronic Health Records
- The American Board of Family Medicine's Data Collection Method for Tracking Their Specialty
- Health Care Integration and Coordination with Emphasis on Mental Health, but Not for Medical Marijuana