
Article Figures & Data
Figures
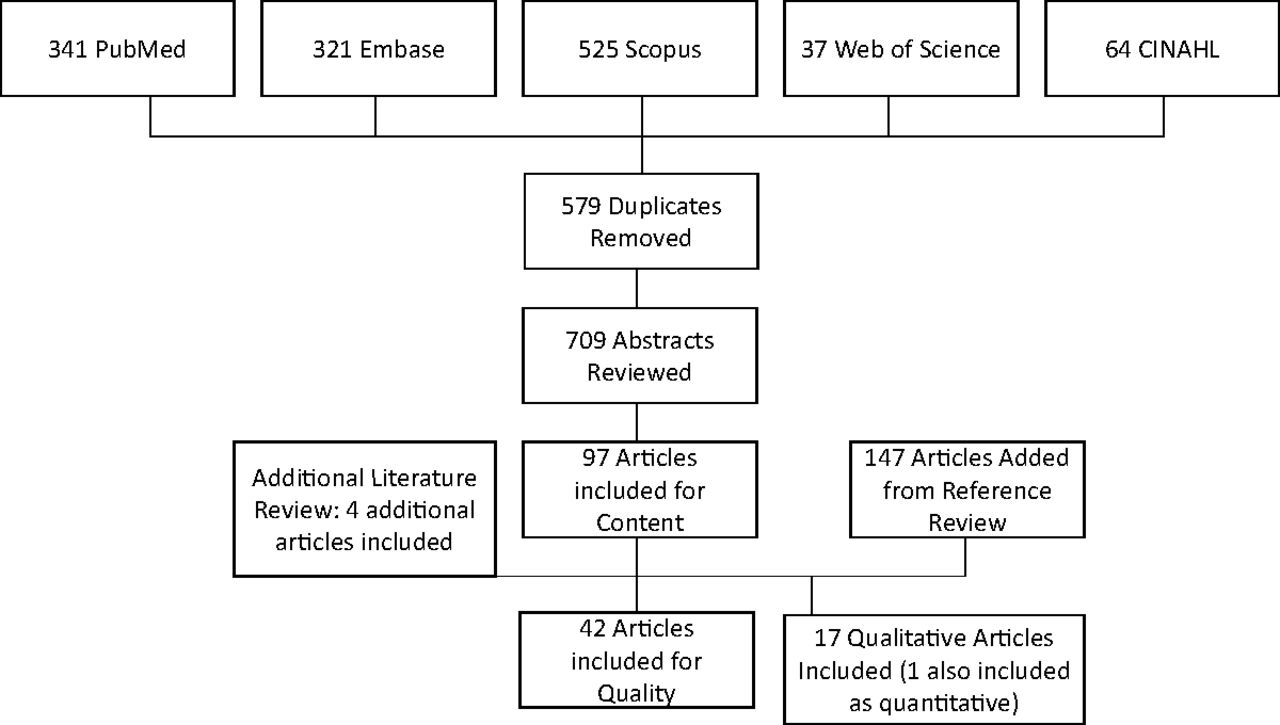
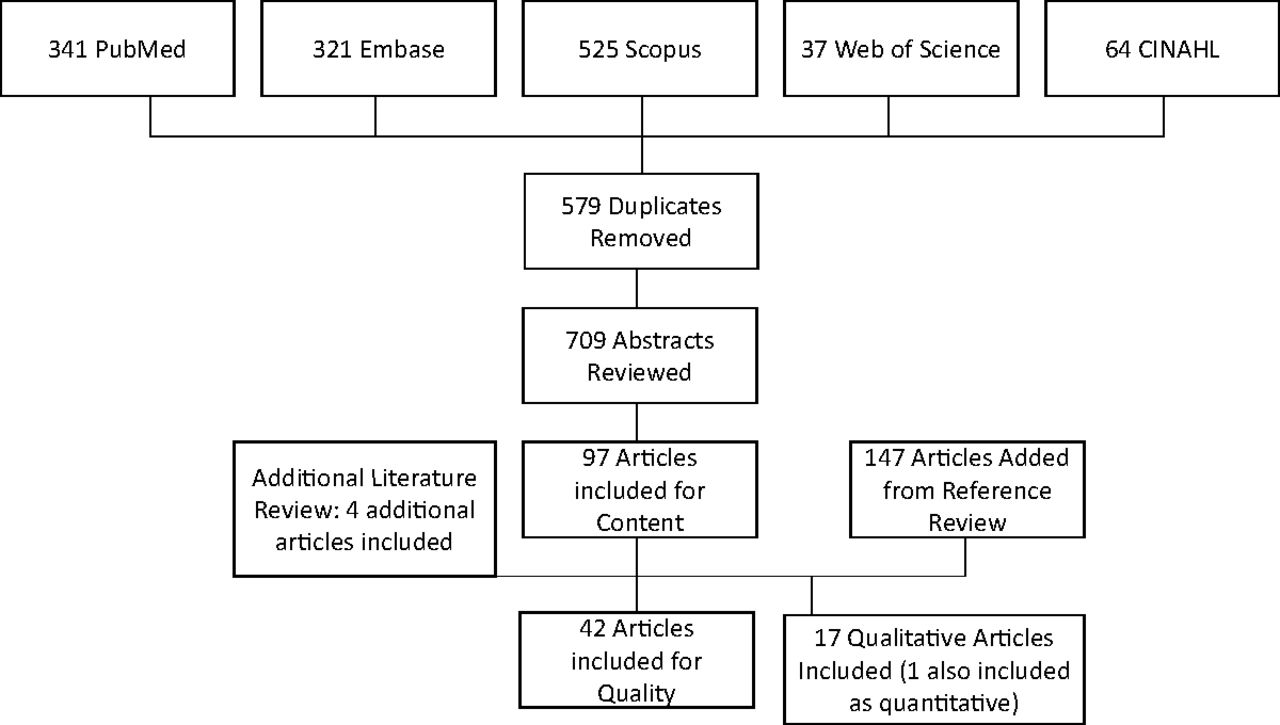
- Figure 1.
Flow chart demonstrating inclusion of articles in the review. Rigorously designed quantitative studies of ambulatory antibiotic stewardship interventions (randomized controlled trials and quasi-experimental studies with stepped wedge and interrupted time series approaches), as well as qualitative studies describing barriers and facilitators to ambulatory antibiotic stewardship were included. Databases were searched through November 7, 2016, with additional titles added based on knowledge of the literature and relevance to the work.
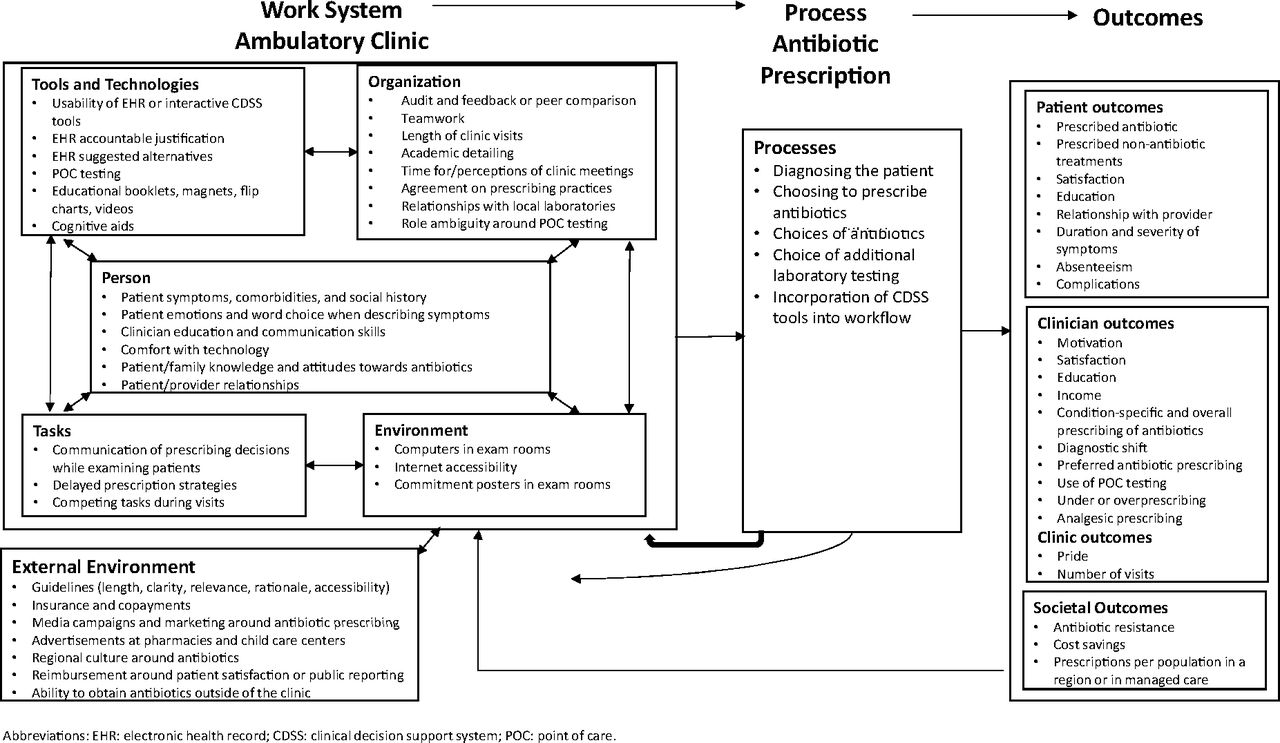
- Figure 2.
Adaptation of the Systems Engineering Initiative for Patient Safety (SEIPS) 2.0 model of the health care work system to approaches taken in the literature to improve antibiotic stewardship in the ambulatory setting.

Tables
- Table 1.
Aspects of Ambulatory Antimicrobial Stewardship Interventions as Applied to Components of the Ambulatory Work System, SEIPS 2.013*
Tools / Technology Components Person(s) Components Organizational Components Task Components Physical Environment Components External Environment Components • EHR-based CDSS20,38,41 to 42,50,54,67,70,72 • Commitment to use and agreement with CDSS20 • CDSS alters practice workflow20 • Improves efficiency20 • Computer location20,33 • External clinician guidelines20,26,30,37,39–41,54–55,65–67,76 • Hyperlink to patient education20,54,66 • Technically savvy staff20 • Role of person initiating task is different in different clinics (ie, triage nurse, medical assistant, and clinician)20,69 • Ordering an antibiotic in EHR21 • Brochures and posters in exam rooms and waiting rooms24,31,38,43,46,59–60,66 • New guidelines written57 • Hyperlink to and accessibility of guidelines39,40,54,66 • Comfort with prior ARI templates20 • Computerized patient flow manager designed by clinics33 • Protocols support decision making73 • Regional clinician newsletter61,72 • EHR-based audit and feedback20 • Providers signed letter/poster soliciting support27,31,56,58,59 • Patients see physicians with different practices66,72,73 • Amoxicillin as placebo if physician did not think they need antibiotics76 • Insurance policies regarding cost-sharing25,66 • EHR-based antibiotic prescribing agreement49 • Prescribing feedback22,23,37,3–41,44,46,51,54,57,60,62–63,67 • Previsit triage and education by nurses may prevent visits72 • Limited time during patient visits, antibiotics to save time66,72,73,77 • Meetings with community leaders38 • Template for ARI clinic visits41 • Intensive intervention for highest prescribers58 • Large health systems enable system-level alerts66 • Competing demands72 • Mass media campaign38,56,61,72,74 • EHR-based accountable justifications and suggested alternatives (pop-up of alternatives and educational material)21,44 • Clinician instruction on evidence-based medicine30,72 • Need for hospital lab35,69 • Restricted susceptibility testing70 • Education at pharmacies, health fairs, child care centers, and offices38,47,48,75 • Limited printing capabilities20 • Clinician instruction on problem solving and communication30,49,52,53,59 • Peer comparison21,23,44,46,51,60,62–63 • Diagnostic uncertainty72,76 • CDC campaigns for judicious antibiotic use43,54 • Tool adaptability20,62,77 • Older prescribers: prescriptions influenced by habit70 • Other clinicians see accountable justification21,44 • Checklist completed by clinician and patient62 • Disclosed prescribing status monthly to patients, health authorities, and health workers45 • Network issues20 • Newer prescribers: nervous about making mistakes73 • Group follow-up meetings with individual feedback24,52–54 • Communicating with patients59,64,65,77 • Health ministry-required tasks70 • Mailed intervention22,38,43,47,48,55,58 to 60,75 • Depend on patient to decide to take antibiotics36 • On-site group educational time24,38–41,43,59,66,67 • Setting expectations36,64,66 • Performance-based incentives66,70,72 • Printed patient education23.36,41–43,47,59–60,65,70,71,73,75 • Engaged patients: focus groups with elderly volunteers60 • Academic detailing47,75,52–54,58,67 • Educating patients59,64,66,70,73 • Patient can get antibiotics elsewhere66,68 • Letters/posters/videos about avoiding inappropriate antibiotic prescribing with clinician photos or signatures27,31,56,58,59 • Patient/family pressure and expectations62,64,72,74 • Large training sessions55,59 • Use physical exam to communicate64,77 • Other countries or healthcare settings thought to be responsible for resistance68 • Refrigerator magnets38,59,60 • Patient physical traits20,64,65,67,70,77 • Local clinicians led initiative at local hospital medical staff meetings38 • Flexible interventions increase feasibility67 • Willing to postpone treatment if told others would do the same71 • Flip chart or reference card for ARI self-management38,60 • Patient symptoms20,62,64,65,73 • Clinicians compensated for each visit38 • Interventions should engage GPs67 • Social capital71 • Stickers, lapel pins, and otoscope insufflators47,75 • Patient background and knowledge74 • Practice-specific antibiotic prescribing rates39,40,43,49,59,70 • CRP testing has associated tasks (eg, quality assurance)69 • Loss of income from POC testing and reimbursement69 • All received printed versions of poster and electronic version of guideline46 • Avoiding confrontation64 • Clinic champions41–43 • Legal protections73 • Discussion guide at well-child visits20,47,75 • Negotiating with patients64 • Kick-off dinners47,75 • School or day care requires antibiotics74 • Prescription pads for treatment of viral infections47,58,71,75 • Hedging64 • Peer review of colleague transcripts with simulated patients52,53 • Adaptability of intervention to regional culture77 • Delayed prescription: prescribe antibiotics to take only if symptoms worsen36,71 • Patient reward for copays and taking off work66 • Clinics set goals59 • Website for feedback required physicians to log in with individual access code37 • Most PCPs did not see antibiotic resistance as a problem in their practice68 • Clinic pride64 • Dashboard51 • Worried about patient illness from not prescribing antibiotics67,70 • Relationships with patients64,71 • Want local resistance data68 • GPs assume practice already follows guidelines67 • Limit antibiotic availability in outpatient settings70 • Antibiotic resistance seen as issue for secondary care rather than primary care68 • CRP POC testing24,35,52,53,62,65,69,77 • No accountability for prescribing72 • Procalcitonin testing26 • Peer support helpful with demanding patients73 • POC streptococcal testing65 • Fewer visits, decreased income77 • Multiplex PCR for respiratory viruses32 • Dermatologic consultation27
• Institutional guidelines29
• Prior approval of ID physician70SEIPS, Systems Engineering In Patient Safety; PCP, primary care provider; CDSS, clinical decision support system; POC, point of care; ARI, acute respiratory infection; EHR, electronic health record; CDC, Centers for Disease Control and Prevention; GP, general practitioner; CRP, C-reactive protein; ID, infectious diseases; PCR, polymerase chain reaction.
↵* Studies described include rigorously designed quantitative and qualitative studies describing antibiotic stewardship interventions and the context around antibiotic prescribing decisions, included through November 7, 2016.
- Appendix B:
Aspects of Ambulatory Antimicrobial Stewardship Interventions as Applied to Components of the Ambulatory Work System (SEIPS 2.0).13*
Reference SEIPS 2.0 Element Study Type Tools / Technology Components Person(s) Components Organizational Components Task Components Physical Environment Components External Environment Components Litvin et al20 Qualitative analysis of quasi-experimental study • CDSS through EHR note template
• Hyperlink to patient education
• EHR audit and feedback
• Limited printing capabilities
• Not tailored to multiple complaints
• Facilitates discussion
• Tool adaptability
• Network issues• Patient symptoms
• Patient age
• Commitment to use CDSS
• Agreement with CDSS
• Technically savvy staff
• Comfort with prior ARI templates• CDSS alters practice workflow
• Role of person initiating CDSS is different in different clinics (ie, triage nurse, medical assistant, and clinician)• Improves efficiency • Computer location • External clinician guidelines Persell et al21 2 × 2 × 2 RCT of patients with ARIs comparing (1) accountable justification, (2) suggested alternatives, and (3) peer comparison with educational module • EHR used for accountable justifications and suggested alternatives (pop-up of alternatives and educational material) • Monthly peer comparison emails
• Other clinicians see accountable justification• Ordering an antibiotic in EHR Hux et al22 RCT of PCPs in Ontario randomized to mailed intervention combining prescribing feedback with educational bulletins • Mailed intervention • Prescribing feedback Hallsworth et al23 Randomized 2 × 2 factorial trial of GPs who prescribed antibiotics in the upper 20th percentile randomized to (1) patient educational leaflet and feedback and (2) patient-focused intervention • Patient education leaflet
• Patient-focused information• Feedback intervention given letter saying they prescribed >80% of local practices Strykowski et al24 Spanish RCT of GPs: acute exacerbation of COPD or chronic bronchitis, comparing (1) multifaceted intervention and CRP POC, (2) multifaceted intervention alone, and (3) usual care • CRP POC testing • Both groups had follow-up meetings with individual feedback
• Both groups had training on ARIs• Brochures and posters in waiting rooms Foxman et al25 RCT of nonelderly patients in 6 areas in United States assigned to insurance plans varying by level of cost sharing • Insurance policies regarding cost sharing Long et al26 Shanghai RCT of patients with suspected CAP, randomized to procalcitonin or guidelines alone • Procalcitonin testing • Guidelines for CAP treatment Arakaki et al27 Nonblinded RCT of adults diagnosed with cellulitis by PCP, randomized to outpatient dermatologic consultation • Dermatologic consultation Taylor et al28 RCT of educational intervention aimed at parents of children <2 years of age • Pamphlet, videotape with local pediatrician promoting judicious antibiotic use Torres et al29 Observer-blinded RCT parallel-group study of clinical prediction rule of which children have bacterial pneumonia • More chest X-rays in the control group • Alternative: management based on institutional guidelines Le Corvoisier et al30 RCT of GPs: interactive seminar presenting evidence-based guidelines for ARIs • Subgroups: 2-day evidence-based medicine course only or with 1-day problem-solving course • Specific French guidelines Meeker et al31 RCT in 5 adult primary care clinics to posted commitment letter or usual care in ARIs • Letters/posters about avoiding inappropriate antibiotic prescribing included clinician photos and signatures • Poster-sized commitment letters in exam rooms Brittain-Long et al32 Swedish randomized open label study to receive a rapid (next day) or delayed (8 to 12 days) result of PCR throat swab • Multiplex PCR for respiratory viruses Christakis et al33 RCT of primary care pediatricians for POC evidence delivery on otitis media • Computerized patient flow manager and online prescription manager • NPs, physicians, and housestaff • Computerized patient flow manager designed by clinics • Computer workstations Dahler-Eriksen et al35 Danish randomized crossover trial of CRP measured within 3 minutes or with results in 1 to 2 days • Intervention group: measure CRP within 3 minutes and got results 1 to 2 days later • Needed hospital lab De la Poza Abad et al36 Pragmatic open label RCT among 23 Spanish primary care centers and ARIs to (1) delayed patient-led prescription, (2) delayed prescription collection strategy requiring patients to collect prescription from PCP, (3) immediate prescription, or (4) no antibiotics • All patients given information about antibiotics
• Delayed prescription: prescribe antibiotics to take only if symptoms worsen• Patients told it was normal to feel worse at first, depend on patient to decide to take antibiotics • Patients told it was normal to feel worse at first Hemkens et al37 Swiss pragmatic randomized trial of PCPs with highest antibiotic prescribing randomized to quarterly prescription feedback over 2 years or usual care • Website required physicians to log in with individual access code • Personalized feedback by mail and online • 1 time provision of evidence-based guidelines for ARIs and UTIs Samore et al38 Cluster RCT in rural communities in Utah and Idaho comparing community intervention with CDSS on paper and CDSS with handheld computer • Mailings to parents
• Refrigerator magnets
• Spiral bound flip chart for ARI self-management
• 3 CDSS tools made for ARIs
• Patient-initiated documentation tool
• CDSS generated diagnostic and therapeutic recommendations• Local clinicians led initiative at local hospital medical staff meetings
• Continuing medical education
• Clinicians compensated for each visit and could keep handheld computers• Exam room posters and brochures • Meetings with community leaders
• News releases on self-management of ARIs
• Self-care materials distributed at health fairs
• Education at pharmacies and officesGerber et al39 and Gerber et al40 Cluster randomized trial of pediatric practices focusing on ARIs,39 and follow-up for 18 months after intervention terminated40 • ARI guidelines available as links in EHR • Quarterly personalized feedback and audit • 1 hour on-site clinician education
• Practice-specific antibiotic prescribing rates• Used prescribing guidelines Gonzales et al41 3-arm cluster randomized trial, with 11 practices in each group: (1) printed CDSS, (2) computerized CDSS, and (3) control. • Arm 1: printed CDSS for acute cough
• Arm 2: EHR CDSS
• Arm 3: no decision support
• Arm 1 and 2: printed patient education material
• Arm 1 and 2: template for ARI clinic visits• Provider education and feedback in both intervention groups • Half-day training session • Provider education
• Practice guidelines
• Clinical champions
• Audit and feedbackJenkins et al42 Cluster randomized study of 8 primary care clinics randomized to CDSS pathways and patient education or usual care • 1 page CDSS pathway incorporated into EHR encounter template
• Patient education• Peer champion provider at each clinic Finkelstein et al43 Cluster randomized trial: 12 pediatric practices in 2 MCOs in eastern Massachusetts and Washington State • Parents mailed CDC brochure on antibiotic use • Physician peer leaders reviewed prescribing guidelines in practice meetings
• Given feedback on practice prescribing• Education displayed in waiting rooms • CDC campaigns for judicious antibiotic use Meeker44 Cluster randomized study of 47 primary care practices randomized to receive 0, 1, 2, or 3 behavioral interventions: (1) suggested alternatives, (2) accountable justification, and (3) peer comparison • Suggested alternatives: electronic order sets suggesting nonantibiotic treatments
• Accountable justification: prompts to enter justifications for prescribing antibiotics for nonindicated diagnoses• Peer comparison: emails comparing antibiotic prescribing rates with those of top performers • Accountable justification: written justification would be seen in EHR as a note • All groups received online ARI diagnosis and treatment education Yang et al45 Matched-pair cluster randomized trial in China • Disclosed prescribing status monthly to patients, health authorities, and health workers Schnoor et al46 Cluster randomized trial of 8 German clinical centers and 4 computer-based interventions • All received printed versions of poster and electronic version of guideline • Every other month, GPs given peer comparison • All received poster Finkelstein et al47 and Ackerman et al75 Controlled, community-level cluster randomized trials in 16 Massachusetts communities: physician behavior change strategy47 with follow-up75 • Discussion guide at well-child visits
• Prescription pads for treatment of viral infections
• Stickers, lapel pins, and otoscope insufflators
• Bimonthly educational briefs
• Patient brochure• Introductory letter to pediatricians and family practitioners • Educational coordinator visited practices
• Kick-off dinners• Advertisements at child care centers and pharmacies Huang et al48 Cluster randomized trial of 3-year community-wide intervention for parents of children in 16 communities11 • Educational newsletters • Educational materials in pediatrician offices, pharmacies, and child care settings Vervloet et al49 Matched randomized study of meeting with PCPs and pharmacists, 4 groups with intervention, and 4 matched controls • PCP communication skills training
• Antibiotic prescribing agreements in EHR• Feedback session about group's prescribing
• More variation between physicians than within practicesLinder et al50 Cluster randomized trial of 27 primary care practices to receive an EHR-integrated ARI CDSS • CDSS tool integrated into EHR Linder et al51 Cluster RCT of 27 primary care practices, by using an ARI quality dashboard • ARI quality dashboard • Audit and feedback Cals et al52 and Cals et al53 Pragmatic cluster randomized trial of Dutch PCPs of the impact of POC CRP testing and communication skills on antibiotic use in LRTIs,52 with follow-up of 3.5 years53 • POC CRP testing • Communication training for physicians • Peer review of colleague transcripts with simulated patients Mainous et al54 Quasi-experimental design with 3-month baseline data collection period and 15-month follow-up in 9 intervention and 61 control practices • EHR CDSS tool is populated when ARI diagnosis entered
• CDSS installed on each practice's EHR progress note template
• Hyperlinks to patient and provider education• Performance review
• Audit and feedback• Quarterly meetings with audit and feedback
• Academic detailing
• Monthly phone calls with staff• NIH and CDC guidelines to improve antibiotic prescribing for ARIs
• CDC Get Smart programSlekovec et al55 Quasi-experimental study of French GPs on quinolone prescription for UTIs • Guidelines mailed to GPs and available on website • 200 GPs attended training sessions • Regional guidelines Gonzales et al56 Quasi-experimental community-level study of mass media campaign in Colorado with comparison communities • Providers signed postcard soliciting support • Mass media campaign including outdoor and radio advertisements, billboards, bus tails, bus stop posters, interior bus signs, health fairs, and opinion pieces Hurlimann et al57 Swiss quasi-experimental study of sustained feedback of antibiotic prescription for ARIs and UTIs • Sustained individual feedback • New guidelines written Vinnard et al58 Quasi-experimental study with concurrent control groups of academic detailing and educational mailings • Educational mailings to providers and patients
• Prescription pads for symptomatic treatments
• Providers signed letters to patients• Intensive intervention for highest prescribers • Academic detailing of providers (visits from pharmacist and antimicrobial stewardship expert) Gonzales et al59 Nonrandomized controlled trial, with (1) full intervention, (2) limited intervention, or (3) usual care • Full intervention: household and office-based patient education materials
• Limited intervention: office-based educational materials
• Full intervention: educational refrigerator magnets
• Full intervention: patients mailed pamphlet and letter from medical director• Full intervention: clinician education
• Full intervention: clinic-specific antibiotic prescription rate for acute bronchitis
• Full intervention: 30 minutes of staff meeting
• Full intervention: setting clinic goals• Full intervention: education on acute bronchitis management
• Full intervention: clinicians taught how to refuse antibiotic prescriptions• Both intervention groups: educational posters in exam rooms Gonzales et. al60 Nonrandomized controlled trial of elderly patients with ARIs: 4 intervention practices and 51 control practices in Denver • Mailed campaign to patients
• Office-based materials
• Introductory letter from Department of Public Health
• Patient reference card on ARIs
• Patient refrigerator magnet
• Patient brochures on antibiotic resistance• Focus groups with elderly volunteers for feedback • Individual prescribing profiles • Colorado-wide initiative to provide PCPs with performance feedback • Office-based materials: CDC posters, patient reference cards, and exam room posters Formoso et al61 Community-level, controlled, nonrandomized trial in northern Italy of educational campaign • Region-wide posters, brochures, and local media advertisements
• Region-wide physician and pharmacist newsletterYardley et al62 Process analysis of RCT of GPs in study of LRTI antibiotic prescribing, including web-based training in use of CRP • Training software modifiable
• Patient booklet with checklist
• CRP intervention helpful• Symptoms important to patients • Completing patient booklet checklist Szymczak et al63 Semistructured interviews with pediatricians, following an intervention39 • Parental pressure as a barrier to stewardship • Skepticism of audit and feedback reports
• One respondent admitted to gaming behaviorMustafa et al64 Semistructured interviews of family doctors on ARIs • Avoiding confrontation
• Negotiating with patients
• Hedging
• Physical traits
• Exaggerated symptoms
• Patient expectations• Clinicians ask patients about antibiotic expectations
• Pride
• Rapport• Use physical exam findings to minimize signs
• Careful word choice
• Thorough exam
• Education
• Setting expectationsGrondal et al65 Semistructured interviews of GPs regarding pharyngitis • GPs believed rapid Streptococcus test to be unreliable, as it only detects one bacterium
• CRP used to diagnose bacterial pharyngitis as way to screen for all bacterial infections• Clinical presentation outweighs test results
• Streptococal pharyngitis should be diagnosed based on appearance• All bacteria must be treated • Clinical presentation outweighs guidelines for management of Streptococcal pharyngitis Munoz-Plaza et al66 In-depth interviews of 6 PCPs and 3 urgent care providers about acute sinusitis • Need to find guideline when needed
• Visual cards and graphs to show patients when they will improve
• EHR with web-based patient education• Help patients understand symptoms
• Patients want reward for copays and taking off work• Patients see physicians with different practices
• No protected group education time
• Large health systems enable system-level alerts
• Limited time during patient visits• Large educational posters in exam rooms • External pressures for patient satisfaction
• Patient can get antibiotics elsewhere
• Information overload with updated guidelines
• Copays for visitsTonkin-Crine et al67 Semistructured interviews of experts involved in GP ARI guideline development across 5 countries • Complementary patient education
• Computer reminders to reinforce guidelines• Address GP concerns and explain the need for guidelines
• GPs worry about patients becoming ill without prescription
• Prescribing feedback helpful• Academic detailing
• GPs assume practice already follows guidelines
• GPs may not engage with mandatory meetings• Flexible interventions increase feasibility
• Interventions should engage GPs• Develop guidelines based on research, not to save money
• Guidelines should be consistent
• Guidelines difficult to locate and lengthy
• Local versions of national guidelines
• Governmental funding and national campaignsWood et al68 Qualitative interviews with PCPs in 9 European countries • Request access to local resistance data • Most PCPs did not see antibiotic resistance as a problem in their practice • Antibiotic resistance seen as issue for secondary care rather than primary care • Other countries thought to be responsible for resistance
• Self-prescribing of antibiotics
• Prescribing by dentists and hospital physicians leads to resistanceMauffrey et al70 Qualitative study of French PCPs about preferences for interventions • Dedicated prescription for antibiotics considered excessive
• Limit antibiotic availability in outpatient settings
• Computerized prescription aids
• Educational resources for patients in office• Physician training
• Patient characteristics
• Avoiding prescribing antibiotics is dangerous
• Older prescribers: prescriptions influenced by habit• Practice evaluation is difficult due to competing demands
• Prior approval of ID physician would make practice harder• Restricted susceptibility testing
• Explain and repeat key messages
• Role of PCPs in educating patients
• Too many other health ministry-required tasks• Performance-based incentives
• Public campaigns reinforce what they tell patients
• Physician awareness campaignsRonnerstrand et al71 Qualitative semistructured interviews: patients asked to imagine seeing a physician for ARI, and how long they would delay filling prescription • Given prescription to fill later • More trust means patients would delay prescription • Willing to postpone treatment if told others would do the same
• Social capitalDempsey et al72 Semistructured interviews of 13 PCPs • Prefer of CDSS
• Prefer over-the-counter prescription pad
• Prefer patient educational materials• Meet patient expectations • No accountability for prescribing
• Other clinicians' misconceptions about acute bronchitis
• Previsit triage and education by nurses may prevent visits• Prescribe antibiotics to save time and money
• Diagnostic uncertainty• Reporting of quality measures may help Huddy et al69 Qualitative focus group study of barriers and facilitators to use of CRP for diagnosing CAP among European GPs • Want not just POC CRP but other lab testing in the same system
• Need to test equipment and stay aware of shelf life of cartridges• CRP as aid to communication • Centralized labs
• Different people perform test in different clinics (GP, nurse, and in-house lab)• Quality control tasks
• Responsibility of GP• Although CRP is cost-effective, individual practices may be liable for the cost of the test
• Loss of income to central labsRowbotham et al73 Semistructured interviews and focus groups of UK NPs about experience with ARIs • Used drawings or information leaflets to teach patients • New NPs worried about making mistakes
• Patients exaggerated symptoms• Peer support helpful with demanding patients
• Previous experiences with getting antibiotics from other providers• Protocols support decision making
• Visits are time consuming and complex
• Provide self-management education
• Educate patients to prevent return visits• Legal protection of NPs versus GPs Kuzujanakis et al74 Parenteral surveys • Parents demand antibiotics
• Privately insured and with more or older children had more knowledge• Alternatives to antibiotics • Media information about antibiotics
• School or day care requires antibioticsMurphy et al76 Qualitative interview of GPs reviewing own charts of ARI encounters • Children less likely to receive antibiotics • Amoxicillin as placebo if physician did not think they need antibiotics
• Uncertainty in prescribing antibiotic• External guidelines Anthierens et al77 Qualitative study using think-aloud approach with European GPs about using online tool for CRP ordering • Online intervention
• CRP used as evidence for patients on condition's seriousness
• Tailoring for individual countries and languages• Considering needs of patients
• Level of attention and time taken needs to be brief• Managing patient demands, fewer visits, decreased income
•• GPs use communication skills
• Clarity of intervention
• Physical exam used to communicate to patients• Countries differ in how involved patients expect to be in the decision
• Study in one country may not help in other countriesPCP, primary care provider; CDSS, clinical decision support system; RCT, randomized controlled trial; POC, point of care; ARI, acute respiratory infection; EHR, electronic health record; NIH, National Institutes of Health; CDC, Centers for Disease Control and Prevention; GP, general practitioner; LRTI, lower respiratory tract infection; CRP, C-reactive protein; ID, infectious diseases; MCO, managed care organization; CAP, community-acquired pneumonia; COPD, chronic obstructive pulmonary disease; NP, nurse practitioner; UTI, urinary tract infection; PCR, polymerase chain reaction; GAS, Group A Streptococcus; CAP, community-acquired pneumonia; UTI, urinary tract infection.
↵* Studies described include rigorously designed quantitative and qualitative studies describing antibiotic stewardship interventions and the context around antibiotic prescribing decisions, included through November 7, 2016.
Reference Process Outcome Patient Outcome Provider Outcome Clinic Outcome System Outcome Litvin et al20 • Choice of prescribing antibiotics Persell et al21 • Prescribing antibiotics • Prescribed antibiotics in 24.7% of inappropriate ARI diagnoses prior to and only 5.2% after the study
• Suggested alternative intervention decreased antibiotic prescribing
• Suggested alternatives and peer comparisons decreased antibiotic prescribing for all ARI diagnoses combinedHux et al22 • Most providers were satisfied with intervention
• More first line antibiotics used• Median prescription cost rose in control group Hallsworth et al23 • Antibiotic prescription/1,000 people decreased Strykowski et al24 • GPs in full intervention reduced antibiotic overprescribing (OR, 0.35; 95% CI, 0.18 to 0.68)
• Underprescribing was not significantly increased (OR, 0.25; 95%CI, 0.06 to 1.0; P = .075)Foxman et al25 • 85% more antibiotics prescribed among those without copays than among those with copays Long et al26 • Median duration of antibiotic: 5 days in intervention versus 7 days in control group
• Prescription of antibiotics 84.4% in intervention versus 97.5% in control groupArakaki et al27 • Diagnosis of cellulitis made in 2/20 in intervention group and 3/9 in control group • Antibiotic use in 2/20 patients in intervention versus all in control group
• All improved 1 week laterTaylor et al28 • Number of ARI visits did not change
• Number of diagnoses and antibiotic prescriptions for otitis media and sinusitis did not change
• Antibiotic prescriptions per patient did not changeTorres et al29 • Five patients in each group had unfavorable outcomes • Antibiotic use decreased in clinical prediction group (48.6% versus 86.6%, P < .001) Le Corvoisier et al30 • Proportion of prescriptions containing an antibiotic decreased in intervention (15.2% to 12.3%; P < .001) but not control (15.3% to 16.4%; between group difference 3.93%)
• Maintained improvement for 30 months after intervention terminated
• More symptomatic treatment prescribed in treatment than control (7.8% versus 3.9%)Meeker et al31 • Antibiotic prescribing for nonindicated ARIs decreased in intervention (42.8% to 33.7%) but not control (43.5% to 52.7%)
• Posted commitment letter decreased antibiotic prescribing for nonindicated diagnoses by 19.7%
• No change in appropriate antibiotic prescriptions• No diagnostic coding shift Brittain-Long et al32 • Rapid test result group prescribed fewer antibiotics within 48 hours of visit (4.5% versus 12.3%)
• No difference in symptoms at follow-up
• No significant adverse eventsChristakis et al33 • Proportion of prescriptions for otitis media <10 days decreased 34% in intervention group
• Less likely to prescribe antibiotics in interventionDahler-Eriksen et al35 • Antibiotics started earlier in patients with lower CRP concentrations
• No reduction in antibiotics• Use of ESRs decreased by 8% in intervention
• Blood samples sent to hospital lab decreased by 6%
• Proportion of study patients needing a follow-up telephone call reduced from 63% to 53%De la Poza Abad et al36 • Symptom duration increased only for the no-prescription group
• No difference in symptom severity
• Antibiotic use less in no-prescription and delayed strategies
• Patient satisfaction similar across all groups
• Patient belief in antibiotic effectiveness decreased in no-prescription and delayed strategiesHemkens et al37 • Only 11% of physicians in the intervention group logged onto the online audit and feedback tool • Overall antibiotic prescription in defined daily doses/100 clinic visits did not decrease in the first or second year (0.81%, P = .64; −1.73%, P = .32; respectively)
• Antibiotic prescribing decreased 8.61% among 6 to 18-year-old children in first year only (P = .01)
• Antibiotic prescribing declined 4.59% among adults aged 19 to 65 in second year only (P < .01)Samore et al38 • Macrolides decreased in CDSS but not in community intervention alone
• Greater decrease in antibiotic prescribing in CDSS than in community intervention aloneGerber et al39 • Combination of 2 practices decreased overall and broad-spectrum antibiotic prescribing Gerber et al40 • Antibiotic prescribing increased after intervention ended (intervention, 16.7% to 27.9%; controls, 25.4% to 30.2%; P = .02) Gonzales et al41 • Educational intervention did not further decrease ARI antibiotic prescription Jenkins et al42 • Antibiotic prescriptions decreased 42.7% to 37.9% versus 39.8% to 38.7%
• Decreased broad-spectrum antibiotic useFinkelstein et al43 • Ages 3 months to 3 years: intervention decreased 18.6% versus 11.5% in controls (16% adjusted effect) • Age 3 to 5 years: intervention decreased 15% versus 9.8% in controls (12% adjusted effect) Meeker44 • Control practices: antibiotic prescription decreased from 24.1% to 13.1%
• Suggested alternatives: prescriptions decreased from 22.1% to 6.1% (insignificant)
• Accountable justification: prescriptions decreased from 23.2% to 5.2%
• Peer comparison: prescriptions decreased from 19.9% to 3.7%
• No interactions seenYang et al45 • Reporting at individual and institutional level • Public reporting resulted in 9% decline in antibiotics Schnoor et al46 • Decrease in CAP-related mortality higher in intervention (2.9% versus 0.5%)
• No change in patient adherence to duration of treatment• Increased proportion of visits adhering to antibiotic guidelines (5.6%) Finkelstein et al47 • Downward trend in prescribing even without intervention
• Change in antibiotics dispensed per person-year: no decrease in those <2 years, but 4.6% decrease in 2 to 3 years and 6.7% decrease in 4 to 5 yearsHuang et al48 • More parents in intervention communities correctly answered survey questions Vervloet et al49 • Number of ARI antibiotic prescriptions decreased overall, but intervention group improved more Linder et al50 • 6% of ARI visits in the CDS group used the CDS • Antibiotic prescribing rate for ARIs 39% in intervention versus 43% in control clinics (OR, 0.8; 95% CI, 0.6 to 1.2)
• For antibiotic-appropriate ARIs, no difference antibiotic prescribing in intervention and control clinics (54% versus 59%)
• For nonantibiotic appropriate diagnoses, no difference intervention and control clinics (32% versus 34%)
• When CDSS used, associated with a lower antibiotic prescribing rate for acute bronchitis (OR, 0.5; 95% CI, 0.3 to 0.8)Linder et al51 • Only 28% of intervention clinicians logged into the quality dashboard • No difference in antibiotic prescribing for ARI visits overall (47% versus 47%, P = .87), antibiotic-appropriate ARI visits (65% versus 64%, P = .68), or nonantibiotic-appropriate ARI visits (38% versus 40%, P = .70)
• Those who used the dashboard had a lower ARI prescribing rate (42% versus 50%, P = .02)Cals et al52 • Antibiotic prescribing at index visit: 31% in CRP and 53% without CRP; 27% in education and 54% in no training
• Antibiotic prescribing during 28-day follow-up: no difference
• Total antibiotic prescribing: 45% versus 58% with and without CRP and 38% versus 63% in communication skills trainingCals et al53 • Long-term follow-up over next 2 to 3 years: no difference number of LRTI visits • CRP not used over time: only in 3.7% of visits 2 to 3 years later • Communication training led to a long-term decrease of 10.4% in visits resulting in antibiotic prescription Mainous et al54 • Use of CDSS tool
• Help with diagnosis
• Decide about antibiotics
• How often CDSS template used• Decreased overall prescribing of broad-spectrum antibiotics in adults and children (16.6% to 1.1% and 19.7% to 0.9%, respectively) and antibiotics overall among adults • How often CDSS template used
• Inappropriate prescribing
• Diagnostic shiftSlekovec et al55 • Quinolone prescriptions decreased by 9%, but nitrofurantoin and fosfomycin increased by 36.8% and 28.5% respectively Gonzales et al56 • No adverse impact on emergency department visits or ARI complications • Fewer pediatric clinic visits • Cost savings
• 3.8% decrease in antibiotic prescriptions/1000 persons
• 8.8% decrease in antibiotic dispenses/1000 managed care membersHurlimann et al57 • Increased percentage of prescriptions of penicillins for ARIs treated with antibiotics (49% to 57%)
• Did not decrease the percentage of COPD exacerbations treated with fluoroquinolones
• Did not decrease the proportion of sinusitis and other upper ARIs treated with antibioticsVinnard et al58 • Nonindicated antibiotic prescriptions decreased from 43% to 33% in academic detailing group Gonzales et al59 • Full intervention decreased antibiotic prescription for acute bronchitis (74% to 48%) but not control (78% to 76%) or limited intervention (82% to 77%) • Diagnoses of acute bronchitis did not change Gonzales et al60 • Antibiotic prescribed to 64% of respondents at intervention and control clinics
• Patient satisfaction did not differ: 69% very good or excellent satisfaction in intervention clinic, 63% in control clinicFormoso et al61 • Defined daily doses of antibiotics/1,000 person-days decreased 4.3% in intervention area
• Broad-spectrum antibiotics decreased more
• Intervention did not affect knowledge and attitudes about antibiotic resistanceYardley et al62 • Communication patient and clinician
• Decision to provide antibiotic• Belief in harm or need for antibiotics
• Attitudes towards antibiotics
• CRP: patient feels less enabled and less satisfied• Importance of reducing antibiotic use
• Perceptions of damage to patient/clinician relationship
• Those who did CRP testing showed trend of lost confidence in ability to reduce antibiotic prescribing• CRP testing means less antibiotics Szymczak et al63 • Gaming of audit and feedback • Belief in audit and feedback reports Mustafa et al64 • Learn patient expectations• Decide on antibiotic • Patient/provider relationship
• Education
• Set expectations with next ARI• Avoid confrontation
• Patient/provider relationship
• Dissatisfaction
• Be a good physician• Pride in practice • Antibiotic resistance Grondal et al65 • Choice to do rapid Streptococcus test
• Choice to do CRP• Antibiotics prescribed Munoz-Plaza et al66 • Poor satisfaction • Unwarranted prescribing practices for sinusitis
• Poor patient satisfaction scoreTonkin-Crine et al67 • Use of guidelines among GPs • Engage GPs in interventions Wood et al68 • GPs perceive antibiotic resistance as due to secondary care, pharmacists, dentists, and even other countries Mauffrey et al70 • Interventions should not impact clinic flow Ronnerstrand et al71 • Patient trust in others Dempsey et al72 • Perception of patient requests Huddy et al69 • Quality checks of POC CRP testing • Patients like the test • Increase job satisfaction • Too many visits Rowbotham et al73 • Clinician confidence Kuzujanakis et al74 • Prescribed antibiotic
• Education on antibioticsAckerman et al75 • Preferred an exam room poster with diagnostic algorithm • Patient expectations seen as impacting prescribing • Compared with prior surveys, clinicians demonstrated greater awareness of antibiotic resistance and impact of their prescribing decisions Murphy et al76 • Reminder of danger of antibiotic resistance Anthierens et al77 • Communication with patients • Patient satisfaction • Education about antibiotic resistance • Fewer visits, decreased income ARI, acute respiratory infection; CDSS, clinical decision support system; OR, odds ratio; CI, confidence interval; CAP, community-acquired pneumonia; CRP, C-reactive protein; LRTI, lower respiratory tract infection; COPD, chronic obstructive pulmonary disease; ESR, erythrocyte sedimentation rate; POC, point of care; GP, general practitioner.
↵* As studied in rigorously designed quantitative and qualitative studies describing the context around antibiotic prescribing decisions and antibiotic stewardship interventions, through November 7, 2016 on outcomes, including process outcomes and outcomes to the patient, provider, clinic, and health system.




{kind=link}
{kind=link}