Abstract
Introduction: In the United States, most antibiotics are prescribed in ambulatory settings. Human factors engineering, which explores interactions between people and the place where they work, has successfully improved quality of care. However, human factors engineering models have not been explored to frame what is known about ambulatory antibiotic stewardship (AS) interventions and barriers and facilitators to their implementation.
Methods: We conducted a systematic review and searched OVID MEDLINE, Embase, Scopus, Web of Science, and CINAHL to identify controlled interventions and qualitative studies of ambulatory AS and determine whether and how they incorporated principles from a human factors engineering model, the Systems Engineering Initiative for Patient Safety 2.0 model. This model describes how a work system (ambulatory clinic) contributes to a process (antibiotic prescribing) that leads to outcomes. The work system consists of 5 components, tools and technology, organization, person, tasks, and environment, within an external environment.
Results: Of 1,288 abstracts initially identified, 42 quantitative studies and 17 qualitative studies met inclusion criteria. Effective interventions focused on tools and technology (eg, clinical decision support and point-of-care testing), the person (eg, clinician education), organization (eg, audit and feedback and academic detailing), tasks (eg, delayed antibiotic prescribing), the environment (eg, commitment posters), and the external environment (media campaigns). Studies have not focused on clinic-wide approaches to AS.
Conclusions: A human factors engineering approach suggests that investigating the role of the clinic's processes or physical layout or external pressures' role in antibiotic prescribing may be a promising way to improve ambulatory AS.
- Antibiotics
- Antimicrobial Stewardship
- Clinical Decision Support Systems
- Patient Safety
- Point-of-Care Testing
- Quality Improvement
Antibiotic resistance is increasing worldwide, largely driven by excessive antibiotic use.1⇓–3 In the United States, antibiotic resistance contributes to 23,000 deaths annually and $20 billion in excess health care costs.4 Antibiotic stewardship (AS) minimizes the development of resistance as well as the risk of harm from antibiotic-associated adverse events by ensuring that only patients who need antibiotics get them and that each patient who needs antibiotics receives the right antibiotic at the right time at the right dose for the right duration.5
Although implementation of hospital-based AS teams have been recommended for a decade6, the majority of human antibiotic expenditures (62%) and use occurs in the ambulatory setting.7 At least 30% of these prescriptions are inappropriate.8 Reducing inappropriate ambulatory antibiotic prescribing is essential to decreasing antibiotic resistance.9,10
Human factors engineering is the “scientific discipline concerned with understanding interactions among humans and other elements of a system.”11,12 According to a health care-specific human factors engineering model, the Systems Engineering Initiative in Patient Safety (SEIPS 2.0) model,13 the characteristics of a workplace (eg, an ambulatory clinic) interact in a work system (comprised of person(s), tools and technologies, the organization, tasks, and the physical environment, within a larger external environment); this work system impacts processes such as antibiotic prescribing, which influence outcomes.13
Although human factors engineering approaches have been occasionally used in ambulatory clinics to improve patient safety and quality of care14⇓⇓⇓–18, human factors engineering approaches and models have not been applied to understanding ambulatory AS. We performed a systematic review because human factors engineering approaches describing the clinic's work system could explain influences on antibiotic prescribing and lead to more effective AS interventions. For example, human factors engineering could explain how clinic characteristics such as the ease with which clinicians adapt the electronic health record (EHR) could enhance the intervention's success. We used the SEIPS 2.0 model13 to frame what is known about effective ambulatory AS interventions and identify barriers and facilitators to successful implementation of ambulatory AS interventions.
Methods
Literature Search and Inclusion Criteria
We included quantitative studies to learn whether ambulatory AS interventions were efficacious and qualitative studies to describe barriers and facilitators to AS. We defined ambulatory settings as outpatient practices or offices in which patients came and left on their own (excluding dentistry and emergency medicine practices). We searched the OVID MEDLINE, Embase, Scopus, Web of Science, and CINAHL databases through November 7, 2016, by using a predetermined set of search terms (Appendix A). We identified additional titles from the Cochrane database as well as from the citations in identified articles. Citation titles and abstracts were screened independently by 2 reviewers (SCK and PDT), and full texts were retrieved for all potentially relevant studies. Duplicate studies were removed.
Studies were limited to English-language human studies of antibiotic-prescribing interventions or qualitative studies seeking to understand antibiotic prescribing practices. Quantitative and qualitative studies were assessed by 2 reviewers (SCK and PDT) to determine if they evaluated AS interventions conducted in ambulatory clinics. We considered AS interventions as any intervention that sought to improve the appropriate use of antibiotics in an ambulatory clinic. We included studies that measured the application of an intervention targeting antibiotic prescriptions, described the factors that influence antibiotic prescribing, or explained the process of implementing approaches to improve antibiotic prescribing. For quantitative studies, we a priori only included studies with rigorous designs: randomized controlled trials (RCTs) or quasi-experimental studies using stepped wedge or interrupted time series approaches. Qualitative studies were included if they described the context in which antibiotic prescribing decisions were made or the context, barriers, or facilitators of AS interventions. Any disagreements about study inclusion were discussed until consensus was achieved.
SEIPS 2.0 Model and Data Extraction
Data for studies meeting inclusion criteria were abstracted using components of the SEIPS 2.0 work system model.13,19 The SEIPS 2.0 work system includes 5 components within a wider external environment: (1) person(s), (2) tools and technologies, (3) organization, (4) tasks, and (5) physical environment. The work system centers around the person(s), including health care professionals, the patient and family, their individual characteristics (eg, age and education), and connections between individuals (eg, a patient-clinician relationship).13 Tools and technologies include objects that people use to do work, such as information technologies, educational materials, medical devices, testing equipment, and physical tools. Organization refers to the structures that organize clinic time, space, resources, and activities, including staff member roles. Tasks are specific actions (eg, placing an electronic order) and have qualities such as difficulty, complexity, ambiguity, variety, and sequence. The physical environment includes the clinic's physical space. The work system lies within a larger external regulatory and cultural environment, including societal, economic, and policy forces that impact a clinic.13
We used these work system components to organize aspects of the interventions and the context of AS and to understand which processes and outcomes were addressed by AS interventions. Our aim in using this approach was to identify how aspects of the clinic work system could affect AS intervention successes. We evaluated identified sources and recorded study design and aspects of the studies that could be interpreted in the context of the SEIPS 2.0 model. We also described how measures and outcomes of the studies could be interpreted in the context of the SEIPS 2.0 work system.
Results
Search Results
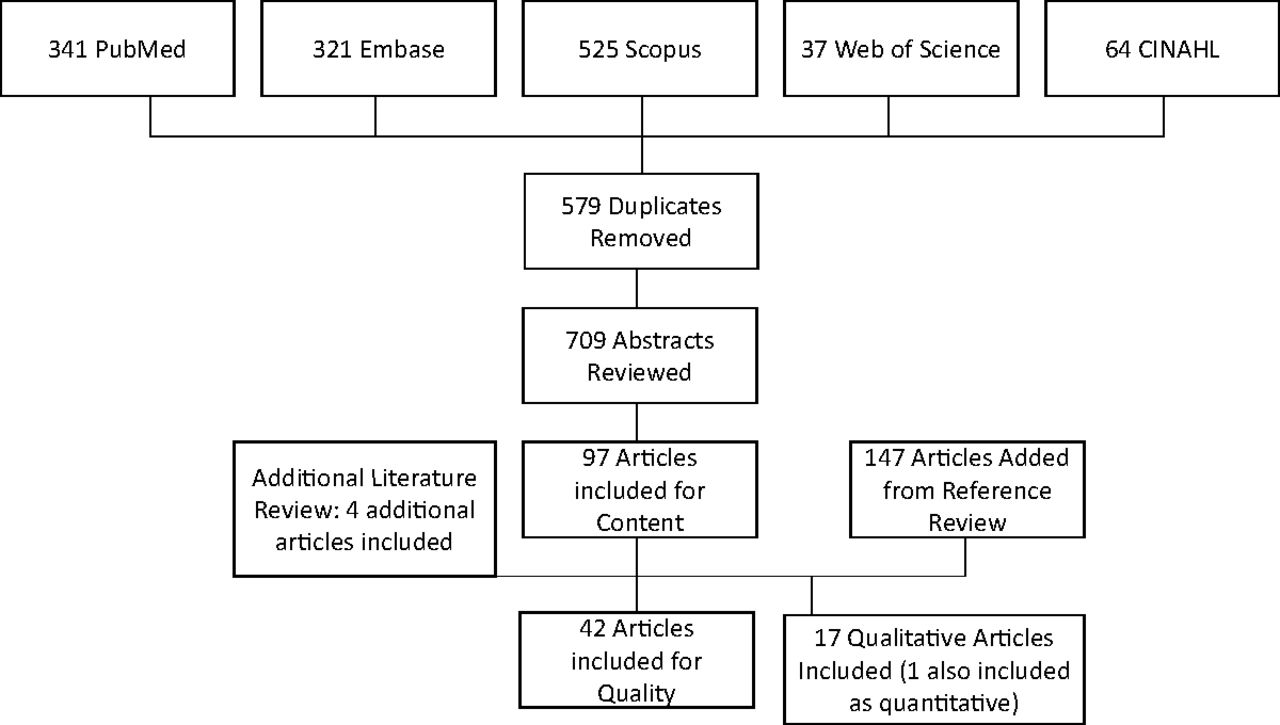
The search identified 1,288 abstracts (Figure 1). Four additional studies meeting inclusion criteria identified through knowledge of the literature were added based on their relevance to the work. Ultimately, 42 quantitative and 17 qualitative articles met the eligibility criteria, with 1 study considered both quantitative and qualitative.19 Fourteen of the quantitative studies were RCTs20⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓–33, 1 was a randomized crossover trial34, 2 were pragmatic RCTs35,36, 14 were cluster randomized trials37⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓–48, 2 were pragmatic cluster randomized trials49,50, and 9 were quasi-experimental, interrupted time series studies.19,51⇓⇓⇓⇓⇓⇓–58
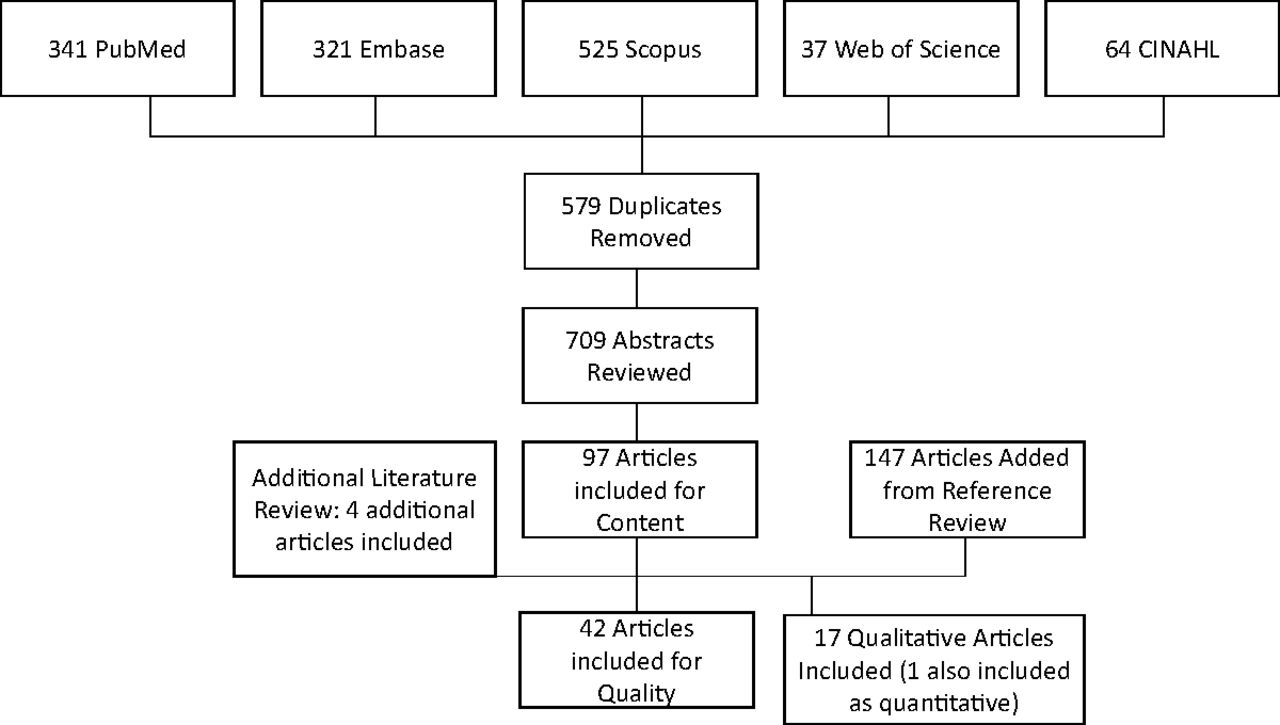
Flow chart demonstrating inclusion of articles in the review. Rigorously designed quantitative studies of ambulatory antibiotic stewardship interventions (randomized controlled trials and quasi-experimental studies with stepped wedge and interrupted time series approaches), as well as qualitative studies describing barriers and facilitators to ambulatory antibiotic stewardship were included. Databases were searched through November 7, 2016, with additional titles added based on knowledge of the literature and relevance to the work.
Of the qualitative studies, 3 were follow-up studies to prior quantitative work19,59,60 (1 of which had been described in the quantitative review).19,38 Eight studies used semistructured interviews61⇓⇓⇓⇓⇓⇓–68 and 1 used focus groups.69 One combined interviews and focus groups70 and 2 involved surveys.71,72 A single study focused on written physician self-reflection, prompting them to review the medical charts of patients.69 Finally, 1 study used a “think-aloud” approach where physicians commented on their inner thought processes.73
AS Interventions and the SEIPS 2.0 Work System
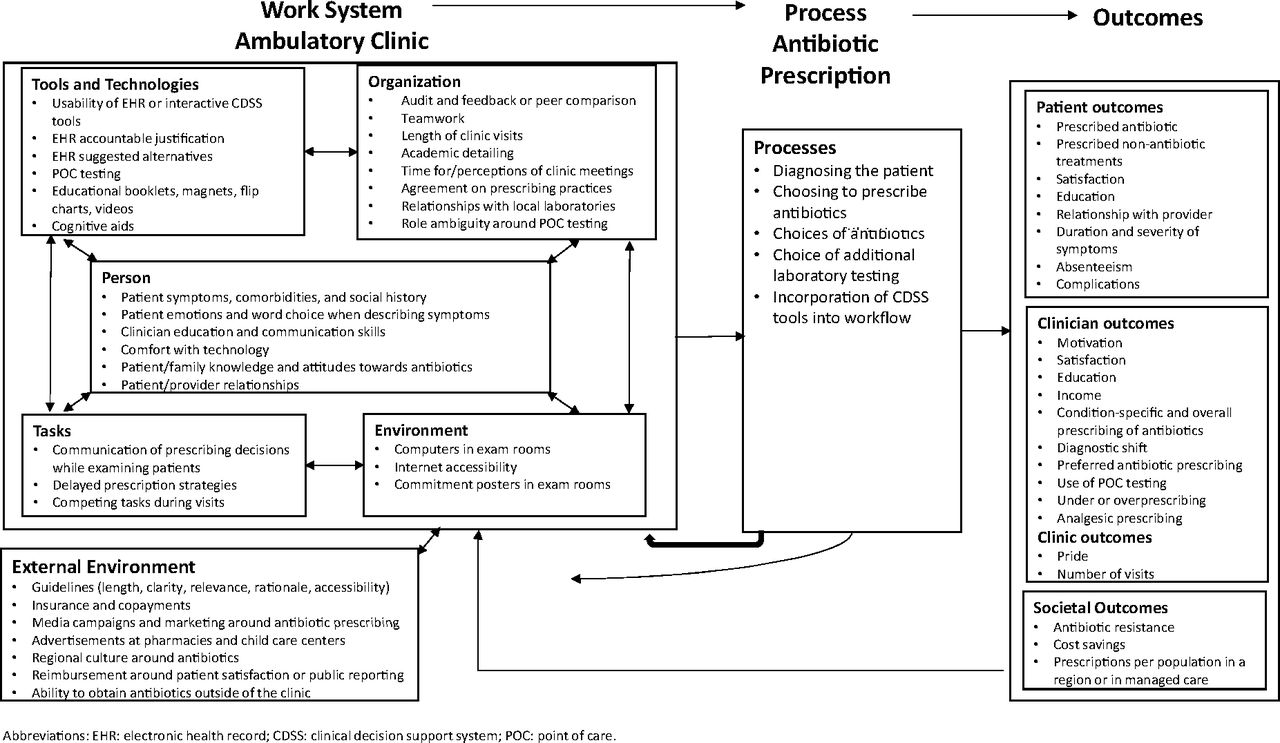
Table 1, Appendix B, and Figure 2 describe how aspects of included studies fit into components of the clinic work system.13. Appendix C describes the processes and outcomes used in each included study.
Aspects of Ambulatory Antimicrobial Stewardship Interventions as Applied to Components of the Ambulatory Work System, SEIPS 2.013*

{kind=link}
{kind=link}
Adaptation of the Systems Engineering Initiative for Patient Safety (SEIPS) 2.0 model of the health care work system to approaches taken in the literature to improve antibiotic stewardship in the ambulatory setting.
Tools and Technology
Tools and technologies include objects and technologies that people use to do work. AS interventions incorporating tools and technologies included clinical decision support systems (CDSS), interventions based in EHRs, educational tools (eg, newsletters, booklets, and videotapes), AS messaging tools (eg, magnets and lapel pins), and point-of-care (POC) testing.
CDSS tools and other EHR-based interventions were frequent and often effective. Highlighting several CDSS tools, a CDSS incorporated into an EHR encounter template decreased acute respiratory infection (ARI) antibiotic prescriptions from 43% to 38% (versus 40% to 39% in control groups).41 An RCT of a computerized patient flow manager with evidence-based prompts decreased antibiotic prescriptions for acute otitis media by 34%.32,74
EHR-based tools have incorporated behavioral interventions. In a 2 × 2 × 2 randomized factorial study comparing accountable justification (providing a written explanation for prescribing nonindicated antibiotics) and suggested alternatives (pop-up messages with education and nonantibiotic alternatives), the suggested alternatives arm was associated with decreased antibiotic prescriptions for ARIs.20 In a larger cluster randomized trial, suggested alternatives did not decrease antibiotic prescription, but accountable justification decreased inappropriate antibiotic prescribing (23% to 5%).43
However, the context in which electronic tools were deployed impacted their implementation. Factors associated with unsuccessful incorporation of CDSS tools and EHR technologies into clinics included nonintuitive tools, need for additional software,51 computers not being available in examination rooms, and slow internet connectivity.19 CDSS tools needed to be used to have an effect; in a cluster randomized trial, EHR-integrated CDSS did not impact antibiotic prescribing, but the CDSS tool was used in only 6% of intervention clinic visits.75
The effect of educational tools was mixed. Educational booklets (eg, on self-care for respiratory infections, potential harms of antibiotics, and other topics) were developed with the goals of assisting patients with understanding harms associated with unnecessary antibiotic use and supporting clinicians with antibiotic prescribing.59,66 As a broader intervention including physician feedback, mailing brochures to parents of children successfully decreased community-wide antibiotic use by 4.6% among those aged 2 to 4 years and by 6.7% among those aged 4 to 5 years.42 However, in another study involving mailed patient and clinician education, antibiotic use did not decrease.55 In addition, in a trial of patient educational materials including a letter from the medical director along with pamphlets compared materials mailed to patients and to office practices, pamphlets mailed to offices only, and usual care on antibiotic prescription for acute bronchitis.56 Only the full intervention sites showed a decline in antibiotic prescriptions for acute bronchitis visits, from 74% to 48%.56
Evidence was similarly mixed regarding the impact of multifaceted educational tool bundles. In a cluster randomized trial in 16 Massachusetts communities, clinicians were given tools with AS messages (ie, stickers, lapel pins, and otoscope insufflators), bimonthly newsletters regarding AS, and prescription pads with written recommendations for symptomatic treatment of viral ARIs.46,53 Parents of young children were also mailed brochures and advertisements were placed in child care centers and pharmacies.46 Although there was no difference in ARI antibiotic prescribing in children <2 years, a 5% decrease in children 2 to 3 years and a 7% decrease in children 4 to 5 years was observed.46 In an additional cluster randomized trial, a multifaceted intervention (educational information at pharmacies and clinics, patient mailings, clinic posters, refrigerator magnets, flip charts, patient-initiated chart documentation tools, and CDSS tools) resulted in a decrease in antibiotic prescriptions among children <6 years.37 Another multifaceted intervention (CDSS, clinician education, audit and feedback, and patient education brochures) also led to decreases in the percentage of adolescents and adults prescribed antibiotics for ARIs at CDSS sites (decreased 12%) versus control sites (increased 1%), with no impact on 30-day return visits.40
Interventions involving tools for patient and family education were not always successful. An intervention including mailed information and guideline distribution did not decrease antibiotic use among elderly patients with ARIs.57 Meanwhile, providing patients with an educational pamphlet and videotape of their pediatricians did not decrease the number of viral ARI visits, antibiotic prescriptions for acute otitis media or sinusitis, or total antibiotic prescriptions.27 Patient characteristics such as older age and the need to open the pamphlet or view the videotapes may have made these interventions less effective.
Other studies focused on POC testing as a tool. C-reactive protein (CRP) POC testing may perform better than clinical symptoms and signs in predicting the diagnosis of pneumonia52, but decreases clinician confidence in reducing antibiotic prescribing and decreases patient satisfaction.59 In a study of POC CRP testing availability, antibiotic prescription improved49, but on follow-up 2 to 3 years later, POC CRP testing was only performed in 4% of eligible patient visits.50 POC tests have also been criticized for their short shelf life, need for quality control testing, and difficulties linking the test result to the EHR.76 These factors may have made the tools more difficult to incorporate into practice and limited their effectiveness.
Person
The person component of the SEIPS 2.0 work system describes individual characteristics and relationships between individuals. However, characteristics and perspectives of other clinic staff members such as medical assistants, nurses, and front desk staff were not described.
Patients and Families
Patient factors such as symptoms and comorbidities influence whether a clinician would prescribe antibiotics.19,61,66 Patient and family factors such as education, knowledge of antibiotics, or trust in their physician decreased requests for antibiotics.35,67,71
Clinicians
Clinician training, particularly focusing on communication training, problem-solving strategies, and peer review, was also studied. In an RCT, French general practitioners were randomized to a day-long seminar focusing on problem-solving strategies after all attended a 2-day seminar on evidence-based ARI management.29 The intervention group sustained a decrease in the proportion of antibiotics prescribed over 30 months.29 General practitioners who attended a training session or received in-office instruction along with clinician-specific feedback increased adherence to community-acquired pneumonia guidelines.45 A workshop including peer reviews of transcripts of interactions with standardized patients reduced antibiotic prescriptions from 54% to 27%,49 sustained for 2 to 3 years.50
Clinician and Patient Relationships
Relationships between individuals are an important part of the ambulatory work system.13 Some physicians think that patients want antibiotics61 and prescribe antibiotics to meet perceived patient expectations.68 Physicians may also believe that patients want something (ie, an antibiotic prescription) in exchange for taking off work and paying copays.63
Organization
The organization refers to the structures and roles that organize a clinic. Characteristics of the clinic, roles of clinic members, and the larger organizations in which clinics operate were explored through investigating roles of clinic team members, comparing clinicians to peers, and learning how clinic structures allow clinician education or improve communication.
Few studies involved changing roles of nonclinician staff members to impact AS. Only 1 study included a nonclinician staff member in an educational intervention and the role of this person was not specified.51 In a qualitative study, clinicians suggested using nurses to perform previsit triage and education.72 In POC testing interventions, participants found that it was unclear which staff members to train in POC testing, as various organizational roles performed the test in different clinics.76,77
Audit and feedback interventions, where clinicians are compared with others, have had success.20,48 In a Canadian RCT where clinicians were mailed educational information or prescribing feedback, the feedback group was more likely to use first-line antibiotic prescriptions.21 In a cluster randomized trial, comparing clinicians with top performers (those who seldom prescribe antibiotics inappropriately) decreased inappropriate prescriptions from 20% to 4%.43 In an RCT, antibiotic use decreased among providers who received a letter from England's chief medical officer saying they were prescribing more antibiotics than 80% of local practices.22 An RCT found that the combination of clinician education and audit and feedback decreased antibiotic prescribing overall and broad-spectrum prescribing in particular.38
However, audit and feedback may not be universally successful. In the above RCT,38 after the termination of audit and feedback, prescribing of broad-spectrum antibiotics returned to a level above baseline.39 In a follow-up qualitative study, some clinicians expressed skepticism and discounted the reports.60 Furthermore, in a recent RCT of high-prescribing physicians across Switzerland, receiving letters and an online log-in code with information about antibiotic prescribing did not impact antibiotic prescribing over 2 years.36 Only 11% of physicians in the intervention group viewed their prescribing data.36 Similarly, a cluster randomized trial of an audit and feedback dashboard led to no difference in antibiotic prescribing for ARI visits78, but only 28% of intervention-group physicians used the dashboard. These clinicians had a lower ARI antibiotic prescribing rate (42% versus 50%).78
Organizational structures could pose barriers to AS. Clinic visits were often too brief to discuss guidelines with patients.63,70 If patients saw multiple clinicians in a practice with different prescribing practices, patients may have expected to receive antibiotics.63,70 Many clinics did not have protected time for group education.63 However, in practices where physicians discussed AS guidelines, outcomes improved.52,46
If clinics had protected time for group education, academic detailing, where an expert visits a practice to discuss AS,51,64 was successful.55 In a study comparing (1) office-based patient education, (2) office- and home-based patient and clinician education (practice profiling, setting clinic goals, and academic detailing), and (3) usual care, full intervention sites had a substantial decline in antibiotic prescriptions for acute bronchitis (74% to 48%), whereas the control and limited intervention sites did not.56
Tasks
Tasks describe specific actions and their characteristics. Clinicians pick particular words when describing physical examination findings to patients or perform a thorough physical examination to explain to patients why they were not prescribing antibiotics.61,66,73
In delayed prescription strategies, the clinician gives the patient a prescription and leaves it up to the patient whether to fill it after a specified time or with worsened symptoms. Patients with acute uncomplicated ARIs were randomized: (1) deciding to fill the prescription after 2 days, (2) returning to the clinic after 2 days for a prescription, (3) no prescription, or (4) immediate prescription.35 Patient satisfaction was similar in all groups, and antibiotic use and belief in antibiotic effectiveness was lower in all groups compared with the immediate prescription group.35
Physical Environment
The physical environment refers to the clinic's layout. Most physical environment-based interventions used posters.24,38,46,59,60 By themselves, posters about avoiding antibiotics for “chest colds” did not decrease antibiotic prescription for acute bronchitis.56 However, visible signed commitments about avoiding unnecessary antibiotics decreased unnecessary antibiotic prescribing by up to 20%.31 Studies did not discuss optimizing the placement of these posters.37,45,46,53,56,57
External Environment
The larger external environment includes guidelines and societal, economic, and policy forces that impact a clinic. External guidelines were not always used because they were sometimes difficult to locate63,64,69, too long64, or not seen as relevant.64 Some physicians did not trust guidelines, wondering whether they were intended to save money instead of improving care.64
Media campaigns reinforced what clinicians conveyed.66 A Colorado-wide campaign of billboards, bus signs, radio advertisements, and newspaper op-eds decreased population-wide antibiotic dispenses.53,57 Advertisements in child care centers and pharmacies also reduced antibiotic use.46 In another community-level study, interventions including news releases, community meetings, and presentations at health fairs decreased antibiotic prescriptions.37 In an Italian study, region-wide campaign materials (posters, brochures, and local media advertisements) and a doctor and pharmacist newsletter decreased antibiotic prescribing by 4%.58
Discussion
Human factors engineering approaches have only recently been used in ambulatory clinics to describe defects in testing,14 apply new EHR technologies15,18, and improve clinic workflows.16,17 Our review is the first to incorporate a human factors engineering approach to understanding ambulatory AS.
In the SEIPS 2.0 work system, tools and technologies refer to objects and technologies. Tools and technologies used in ambulatory AS interventions have included CDSS and EHR-based interventions, educational materials, and POC testing. CDSS and EHR-based and educational materials improved AS but only if they were used. POC tools such as CRP testing impacted AS, but many clinicians stopped using the POC tests over time. Human factors engineering would suggest that to make these tools more effective, researchers should make them easier to use.
The person component of the work system includes individual characteristics and relationships between individuals. In particular, clinician communication training had a sustained positive impact on AS, and interventions aimed at educating patients and families also showed a positive impact on AS. However, although clinicians have mentioned the potential impact of other members of the health care team, characteristics of other health care team members have not been studied. Human factors engineering would suggest that the role of other members of the health care team in AS interventions should be studied and these team members should be engaged.
Few studies focused on the organization component of the work system model or the structures and roles that organize a clinic. Audit and feedback and academic detailing had a positive impact on AS. However, we know little about the role of nonclinicians in AS. Engagement of the entire ambulatory team has the potential to send a consistent message about appropriate antibiotic prescribing.68 Human factors engineering would suggest research exploring the roles of clinic staff and clinic flow in an intervention's effectiveness.
Similarly, few interventions focused on the work system component of tasks or specific actions and their characteristics, although delayed prescription strategies were promising. Few interventions focused on the impact of the physical environment of the clinic on antibiotic prescription. However, clinic posters with signed commitments advocating AS positively impacted AS. Human factors engineering would suggest an investigation into the role of the location of clinic posters and other elements of the physical environment, as well as qualities of tasks related to antibiotic prescription, on AS interventions.
Finally, the work system occurs within the external regulatory and cultural environment. Several interventions incorporated the external environment, showing that media-based interventions could improve AS at a community level and showing that external guidelines needed to be accessible to clinicians and trusted by clinicians. The role of the external environment in the form of external pressures on AS interventions such as patient satisfaction-based reimbursement has not been fully examined and should be a focus of future research.
Our review has several limitations. We only included well-controlled quantitative studies and may have missed other domains if they were targeted only in uncontrolled studies. We did not assess for publication bias. Finally, our findings are more applicable to ARIs, the focus of most studies, as we were unable to identify many high-quality studies that implemented AS for other conditions (eg, urinary tract infections and cellulitis).
Evidence-based AS interventions impact different portions of the ambulatory work system, and using a human factors engineering approach may facilitate the intervention's success. However, interventions did not typically engage all clinic staff in the implementation, a model that has led to successes in patient safety and quality improvement.79⇓⇓⇓⇓–84 Few interventions have accounted for physical environment or task characteristics in implementing interventions. Future work in ambulatory AS should address the entire work system in which the intervention is implemented. Such work system interventions, if rigorously evaluated, may have greater potential than isolated interventions to improve the effectiveness of ambulatory AS.
Acknowledgments
We gratefully acknowledge the support of Maria Trusky, MLS, for her assistance in extracting the articles. We also appreciate the assistance of Kathleen Speck, MPH, for assistance in formatting the tables.
Appendix A: Search Terms
PubMed 341 Results, 11/7/2016
(“Anti-Infective Agents”[Mesh] OR “Anti Infective Agents” OR “Anti Infective Agent” OR “Antiinfective Agents” OR “Antiinfective Agent” OR “Anti-infective agents” OR “anti-infective agent” OR “Microbicides” OR “antimicrobial agents” OR “antimicrobial agent” OR “antimicrobials” OR “Anti-Microbial Agents” OR “antimicrobial agent” OR “Anti Microbial Agents” OR “anti microbial agent” OR “antibiotics” OR “antibiotic” OR “antibiotics” OR “antibiotic” OR “Anti Bacterial Agents” OR “Anti Bacterial Agent” OR “Antibacterial Agents” OR “Antibacterial Agent” OR “Bacteriocidal Agents” OR “Bacteriocides” OR “Anti-Mycobacterial Agents” OR “Anti Mycobacterial Agents” OR “Antimycobacterial Agents”) AND (“stewardship” OR “stewards” OR “antimicrobial management” OR “antimicrobial prescribing behavior” OR “antibiotic stewardship” OR “antimicrobial stewardship” OR “appropriate use” OR “Drug Utilization”[Mesh] OR “ASP”) AND (“Ambulatory Care”[Mesh] OR “ambulatory care” OR “ambulatory health services” OR “outpatient care” OR “outpatient health services” OR “outpatient health service” OR “urgent care” OR “urgent cares”).
Embase 321 Results, 11/7/2016
(“antiinfective agent”/exp OR “anti infective agent*” OR “antiinfective agent*” OR “anti-infective agent*” OR “microbicide*” OR “antimicrobial*” OR “antimicrobial agent*” OR “anti microbial agent*” OR “antibiotic*” OR “antibiotic*” OR “anti bacterial agent*” OR “antibacterial agent*” OR “bacteriocidal agent*” OR “bacteriocide*” OR “antimycobacterial agent*” OR “anti mycobacterial agent*”) AND (“drug utilization”/exp OR “drug utilization” OR “drug utilization” OR “stewardship” OR “stewards” OR “antimicrobial management” OR “antimicrobial prescribing behavior” OR “antibiotic stewardship” OR “antimicrobial stewardship” OR “appropriate use” OR “asp”) AND (“ambulatory care”/exp OR “ambulatory care” OR “ambulatory health service*” OR “outpatient care*” OR “outpatient health service*” OR “urgent care*” OR “dispensary care” OR “extramural care”).
Scopus 525 Results, 11/7/2016
(TITLE-ABS-KEY (“antiinfective agent*” OR “anti infective agent*” OR “anti-infective agent*” OR “microbicide*” OR “antimicrobial*” OR “antimicrobial agent*” OR “anti microbial agent*” OR “antibiotic*” OR “antibiotic*” OR “anti bacterial agent*” OR “antibacterial agent*” OR “bacteriocidal agent*” OR “bacteriocide*” OR “antimycobacterial agent*” OR “anti mycobacterial agent*”)) AND (TITLE-ABS-KEY (“stewardship” OR “stewards” OR “antimicrobial management” OR “antimicrobial prescribing behavior” OR “antibiotic stewardship” OR “antimicrobial stewardship” OR “appropriate use” OR “Drug Utilization” OR “drug utilization” OR “ASP”)) AND (TITLE-ABS-KEY (“ambulatory care*” OR “ambulatory health service*” OR “outpatient care*” OR “outpatient health service*” OR “urgent care*” OR “dispensary care” OR “extramural care”)).
Web of Science 37 Results, 11/7/2016
TS = (“antiinfective agent*” OR “anti infective agent*” OR “anti-infective agent*” OR “microbicide*” OR “antimicrobial*” OR “antimicrobial agent*” OR “anti microbial agent*” OR “antibiotic*” OR “antibiotic*” OR “anti bacterial agent*” OR “antibacterial agent*” OR “bacteriocidal agent*” OR “bacteriocide*” OR “antimycobacterial agent*” OR “anti mycobacterial agent*”) AND TS = (“stewardship” OR “stewards” OR “antimicrobial management” OR “antimicrobial prescribing behavior” OR “antibiotic stewardship” OR “antimicrobial stewardship” OR “appropriate use” OR “Drug Utilization” OR “drug utilization” OR “ASP”) AND TS = (“ambulatory care*” OR “ambulatory health service*” OR “outpatient care*” OR “outpatient health service*” OR “urgent care*” OR “dispensary care” OR “extramural care”).
CINAHL 64 Results, 11/7/2016
((MH “Antiinfective Agents+”) OR “antiinfective agent*” OR “anti infective agent*” OR “anti-infective agent*” OR “microbicide*” OR “antimicrobial*” OR “antimicrobial agent*” OR “anti microbial agent*” OR “antibiotic*” OR “antibiotic*” OR “anti bacterial agent*” OR “antibacterial agent*” OR “bacteriocidal agent*” OR “bacteriocide*” OR “antimycobacterial agent*” OR “anti mycobacterial agent*”) AND ((MH “Drug Utilization”) OR “stewardship” OR “stewards” OR “antimicrobial management” OR “antimicrobial prescribing behavior” OR “antibiotic stewardship” OR “antimicrobial stewardship” OR “appropriate use” OR “drug utilization” OR “ASP”) AND ((MH “Ambulatory Care”) OR “ambulatory health service*” OR “outpatient care*” OR “outpatient health service*” OR “urgent care*” OR “dispensary care” OR “extramural care”).
Appendix
Aspects of Ambulatory Antimicrobial Stewardship Interventions as Applied to Components of the Ambulatory Work System (SEIPS 2.0).13*
Appendix
Summary of the Impact of Ambulatory Antimicrobial Stewardship Interventions*
Notes
This article was externally peer reviewed.
Funding: This work was supported by the Agency for Healthcare Research and Quality (AHRQ) (HHSP233201500020I/HHSP23337003T). The findings and conclusions in this document are those of the authors, who are responsible for its content, and do not necessarily represent the views of AHRQ. No statement in this report should be construed as an official position of AHRQ or of the U.S. Department of Health and Human Services. SCK received funding from the National Center for Advancing Translational Sciences/Johns Hopkins Institute for Clinical and Translational research, KL2 award KL2TR001077.
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/31/3/417.full.
* An asterisk indicates that a word stem was used as a search term (for example, antibiotic* signified that either “antibiotic” or “antibiotics” was searched for).
- Received for publication June 7, 2017.
- Revision received December 28, 2017.
- Accepted for publication January 4, 2018.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.
- 51.
- 52.
- 53.
- 54.
- 55.
- 56.
- 57.
- 58.
- 59.
- 60.
- 61.
- 62.
- 63.
- 64.
- 65.
- 66.
- 67.
- 68.
- 69.
- 70.
- 71.
- 72.
- 73.
- 74.
- 75.
- 76.
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.