
Article Figures & Data
Figures
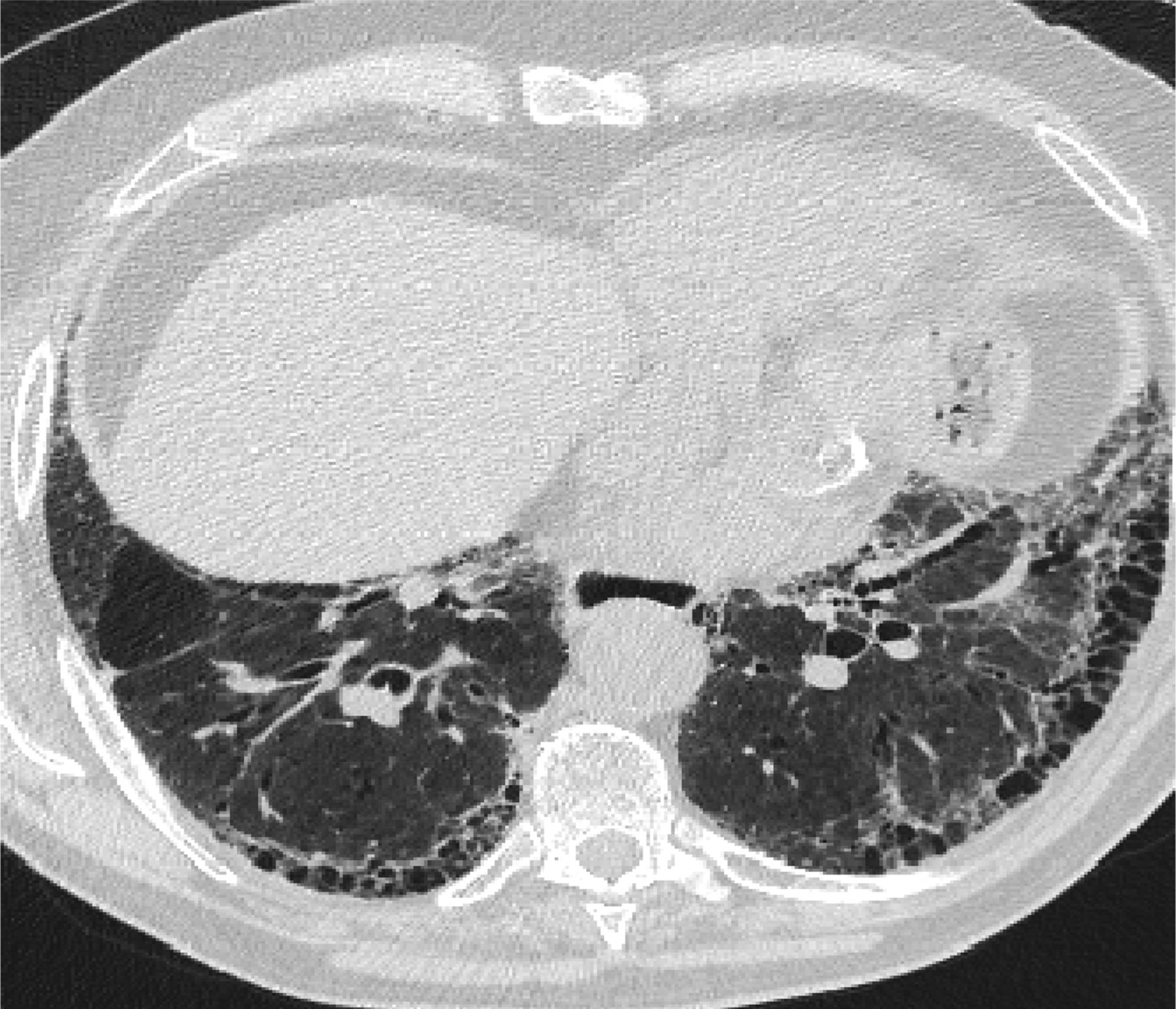
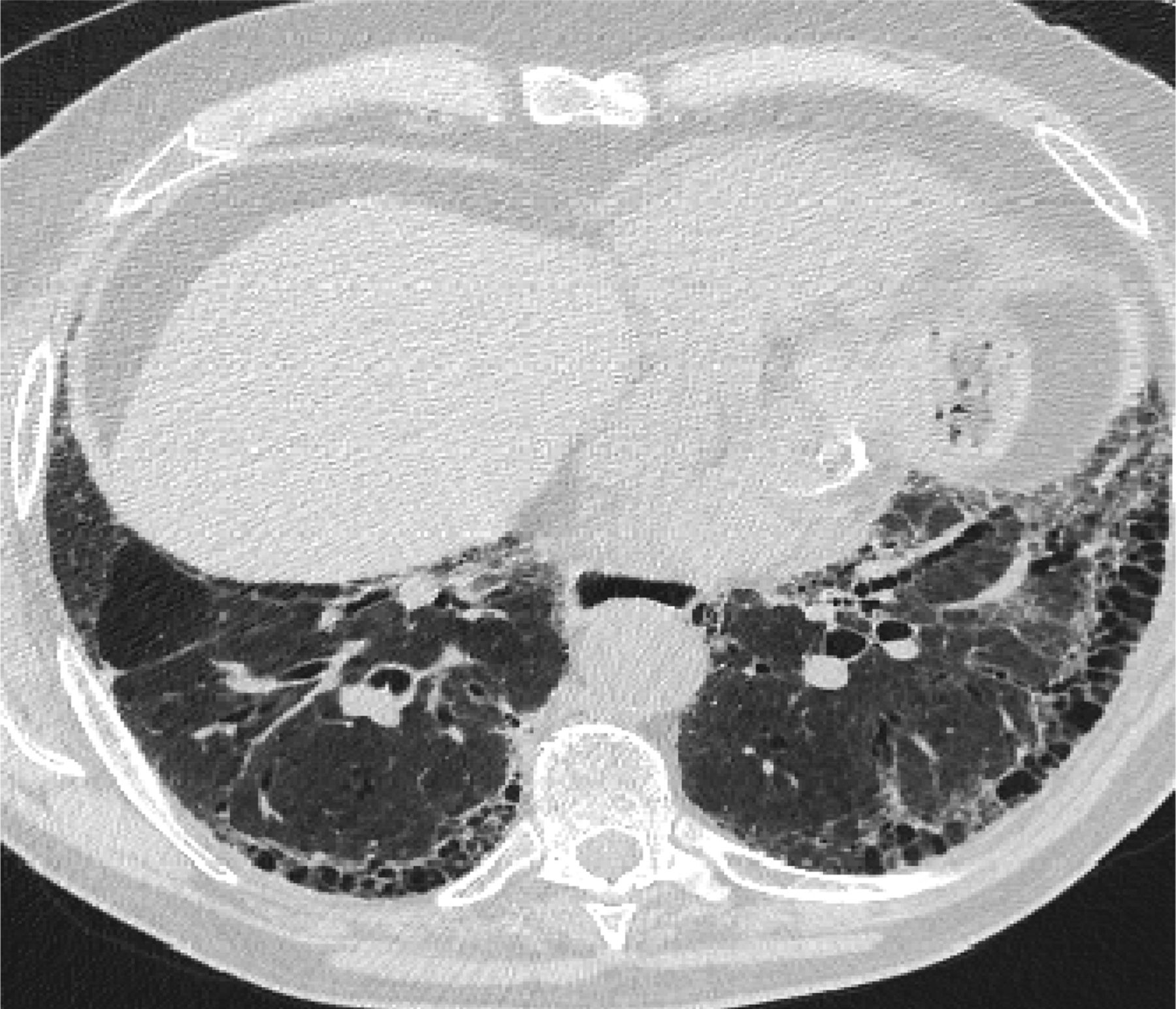
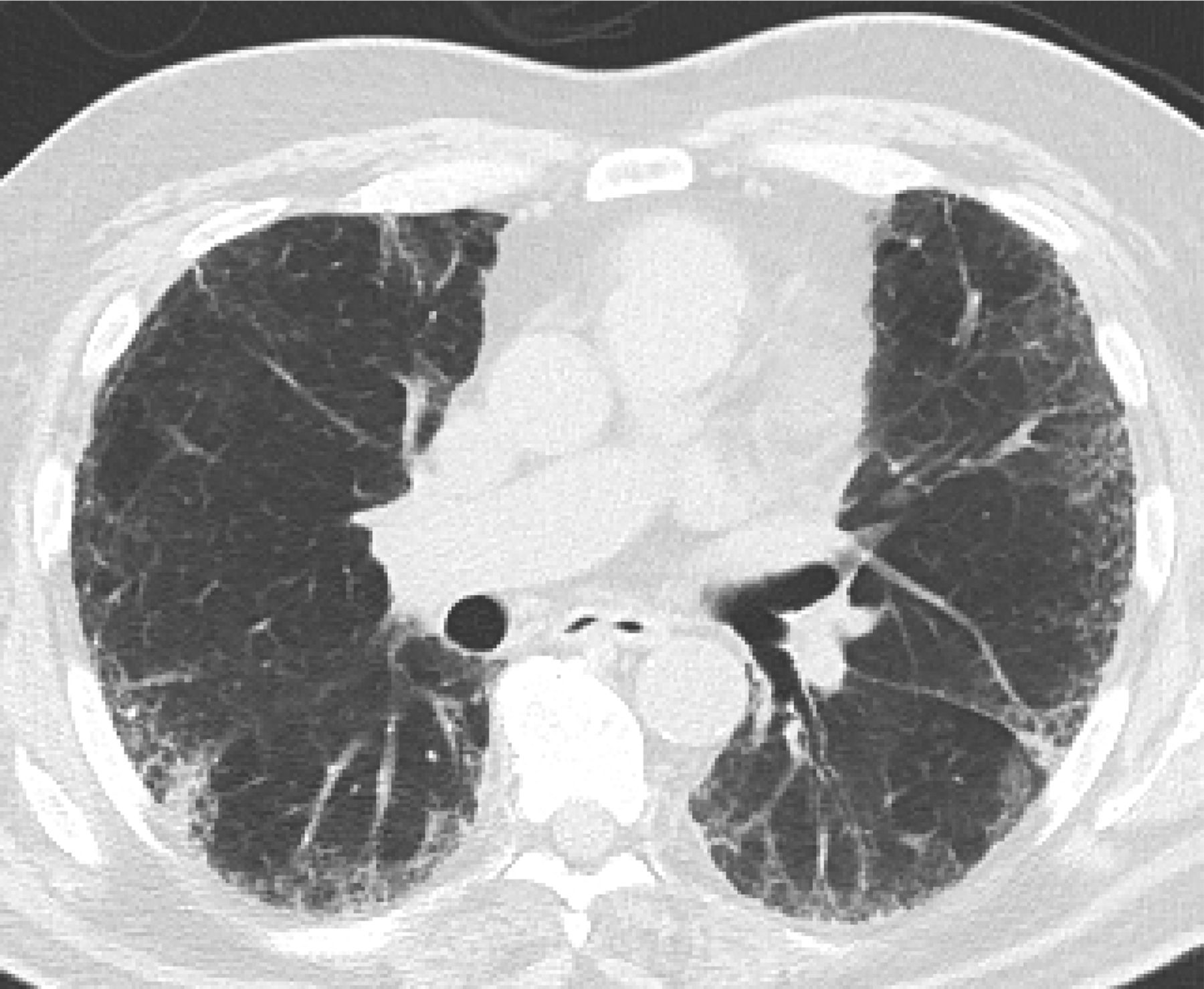
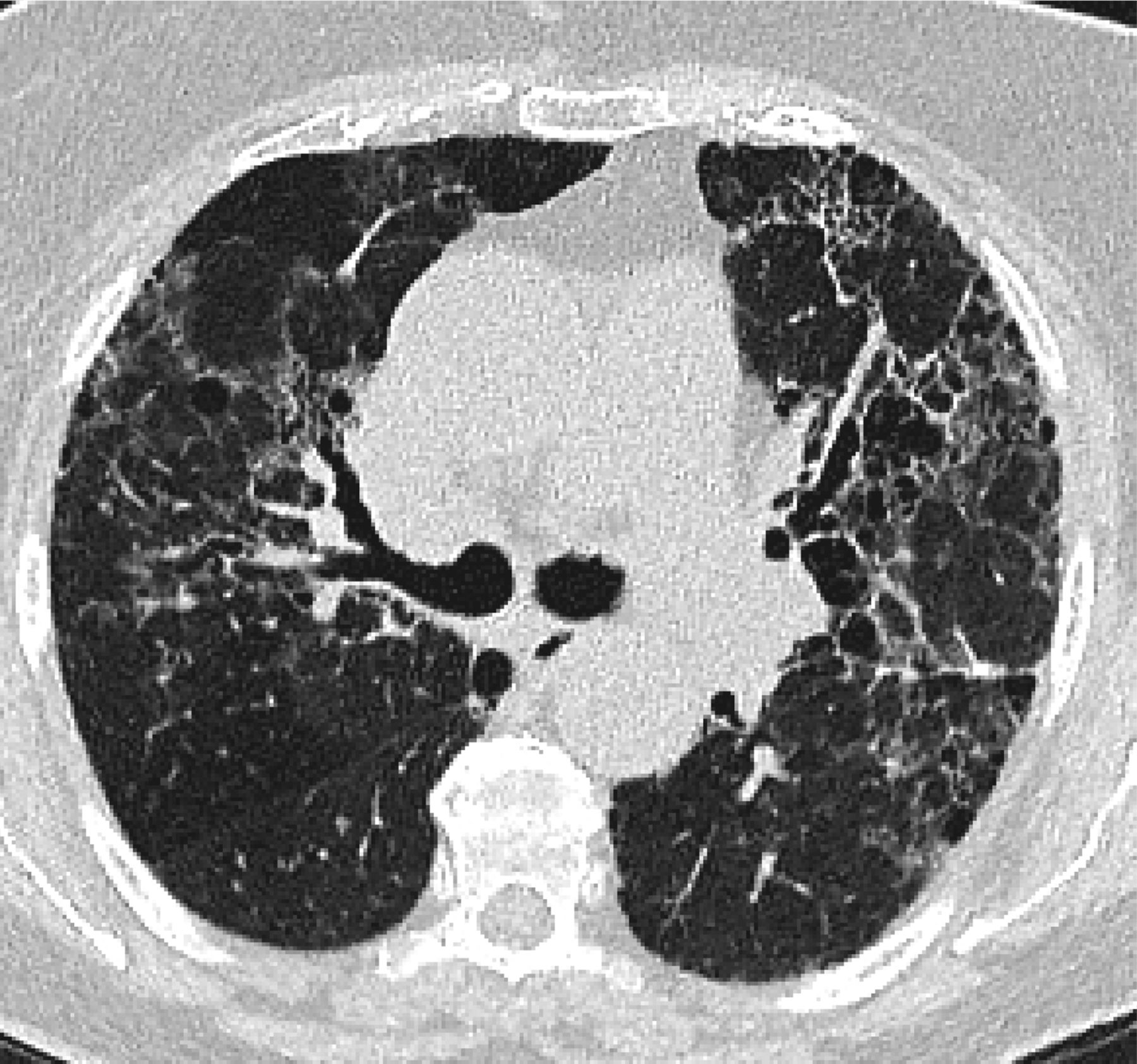
- Figure 1.
A “Usual interstitial pneumonitis (UIP) pattern” radiographically was defined by American Thoracic Society as subpleural basilar predominant fibrosis, reticulations, honeycombing, and absence of features that would support an alternate diagnosis.
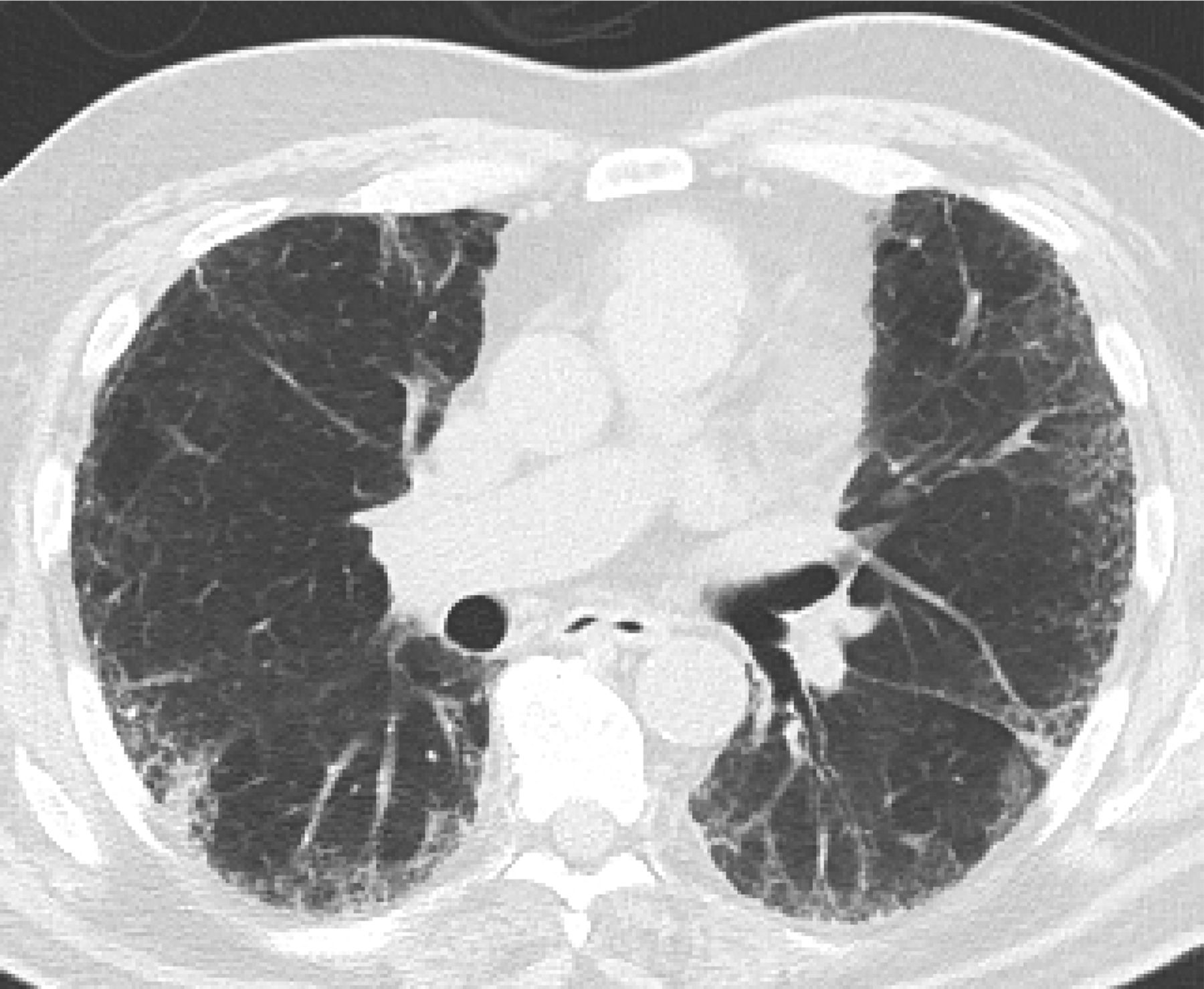
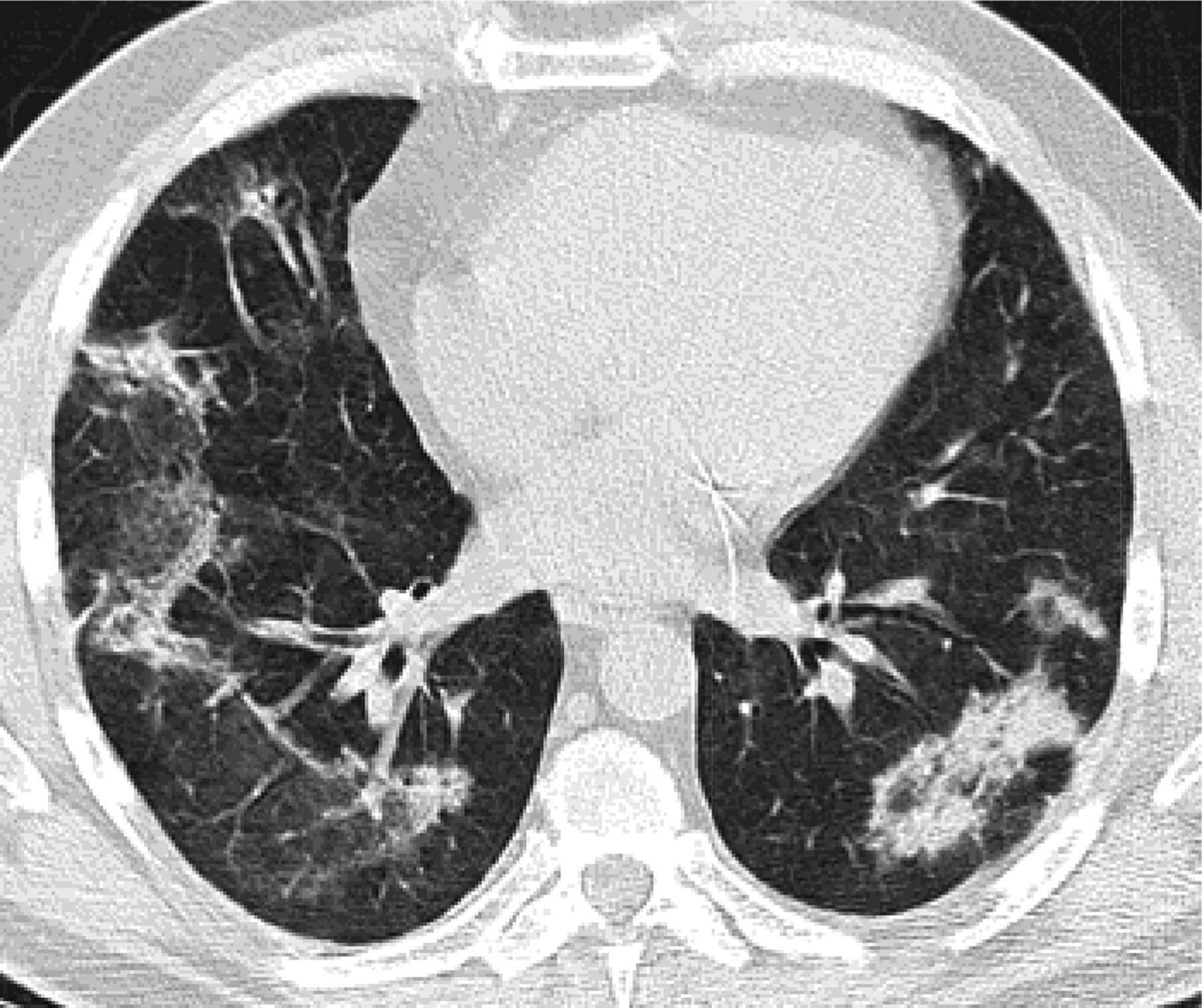
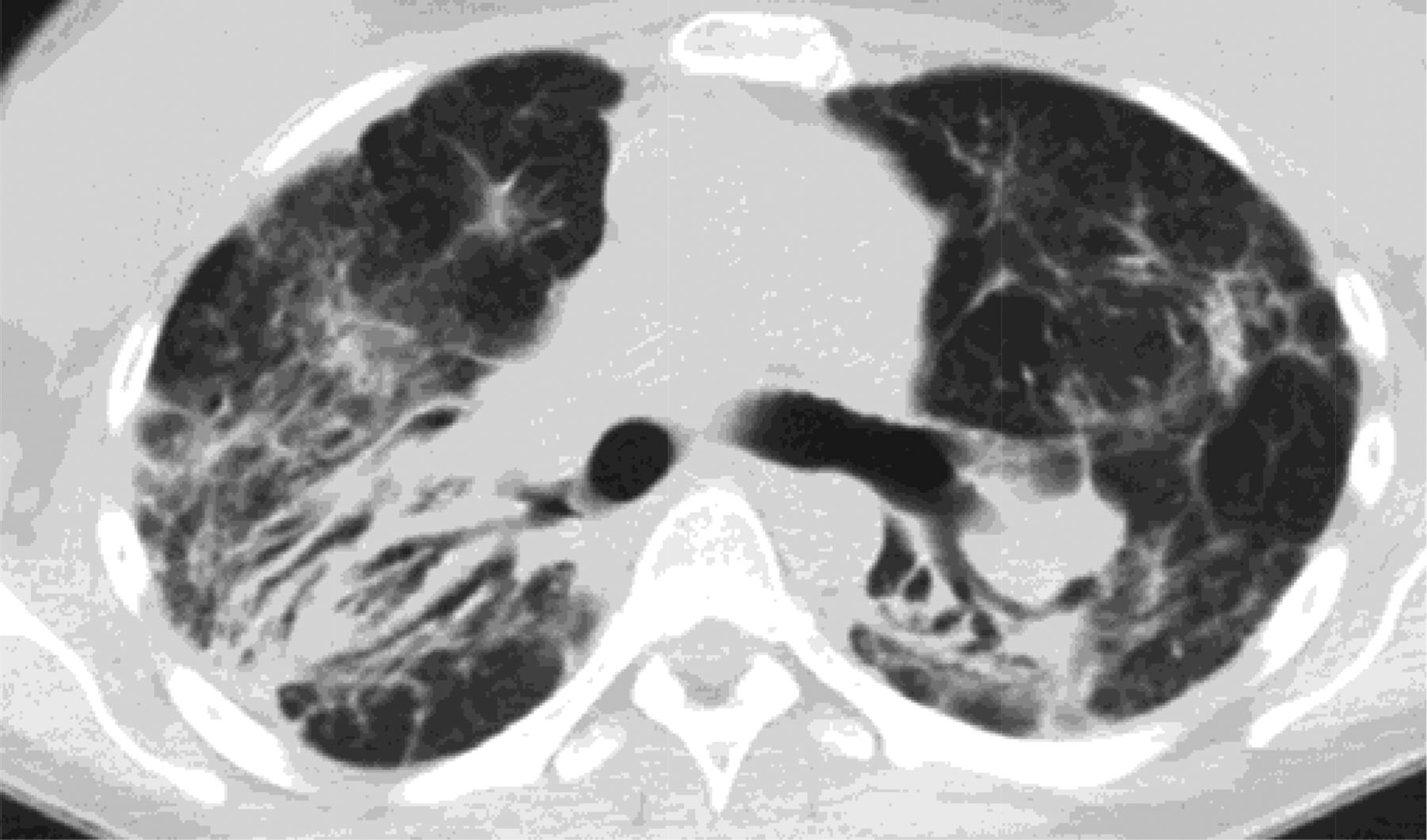
- Figure 2.
If there is no honeycombing but other criteria for a usual interstitial pneumonitis (UIP) pattern are met, the diagnosis is a “possible UIP pattern” radiographically as per the American Thoracic Society (ATS) criteria.
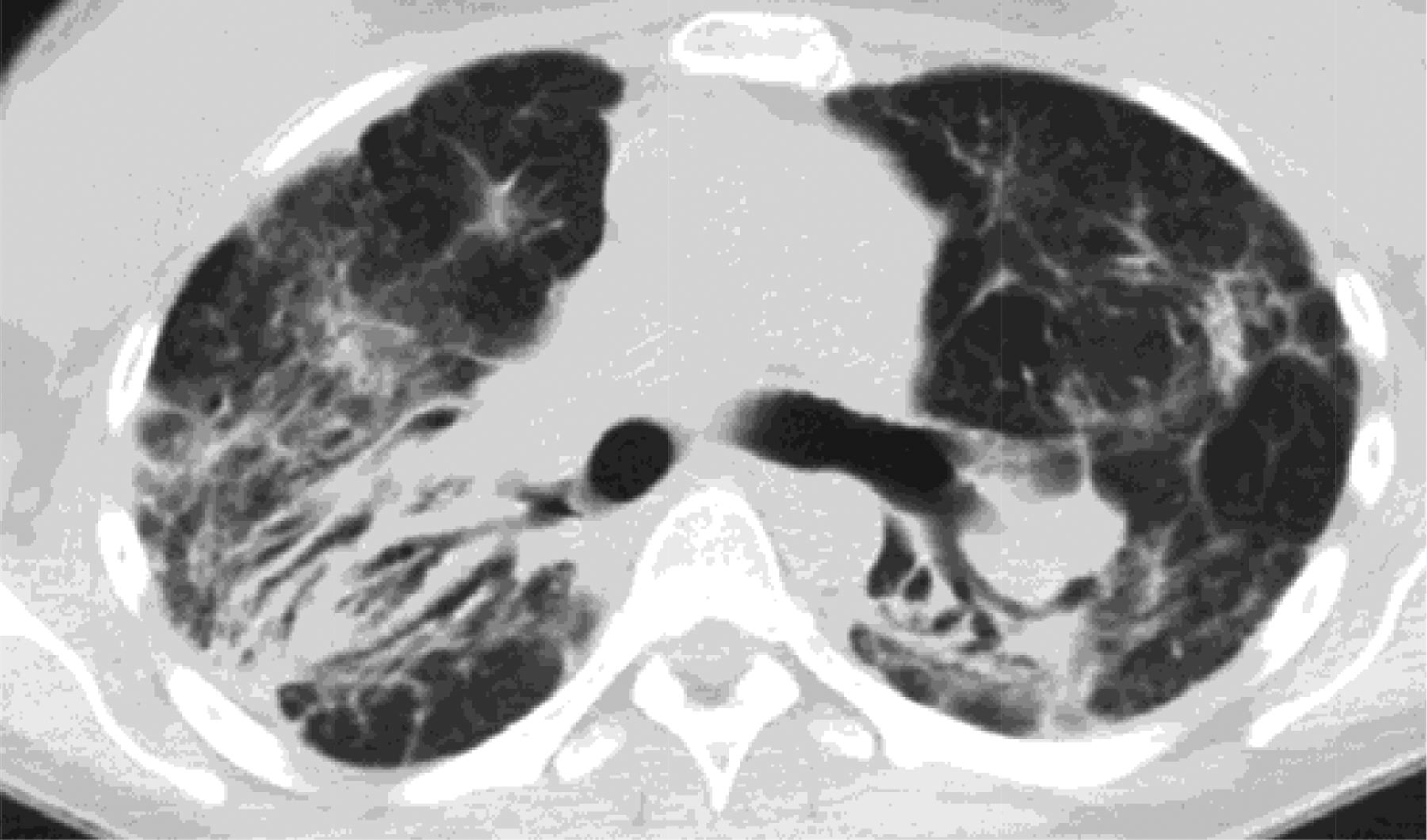
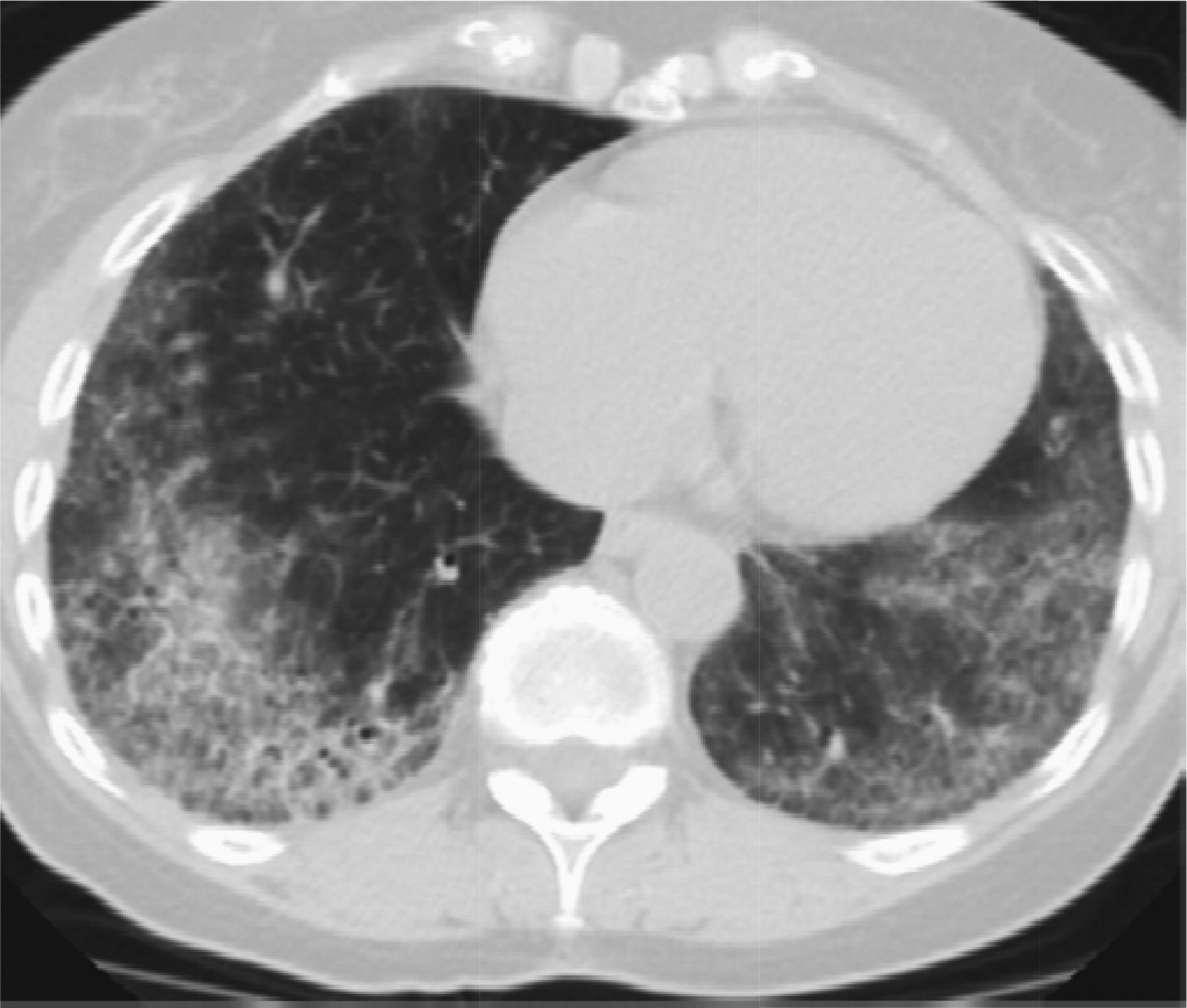
- Figure 3.
Features that would suggest an alternative diagnosis include consolidation as can be seen in organizing pneumonia, which follows the bronchovascular bundles in this example.
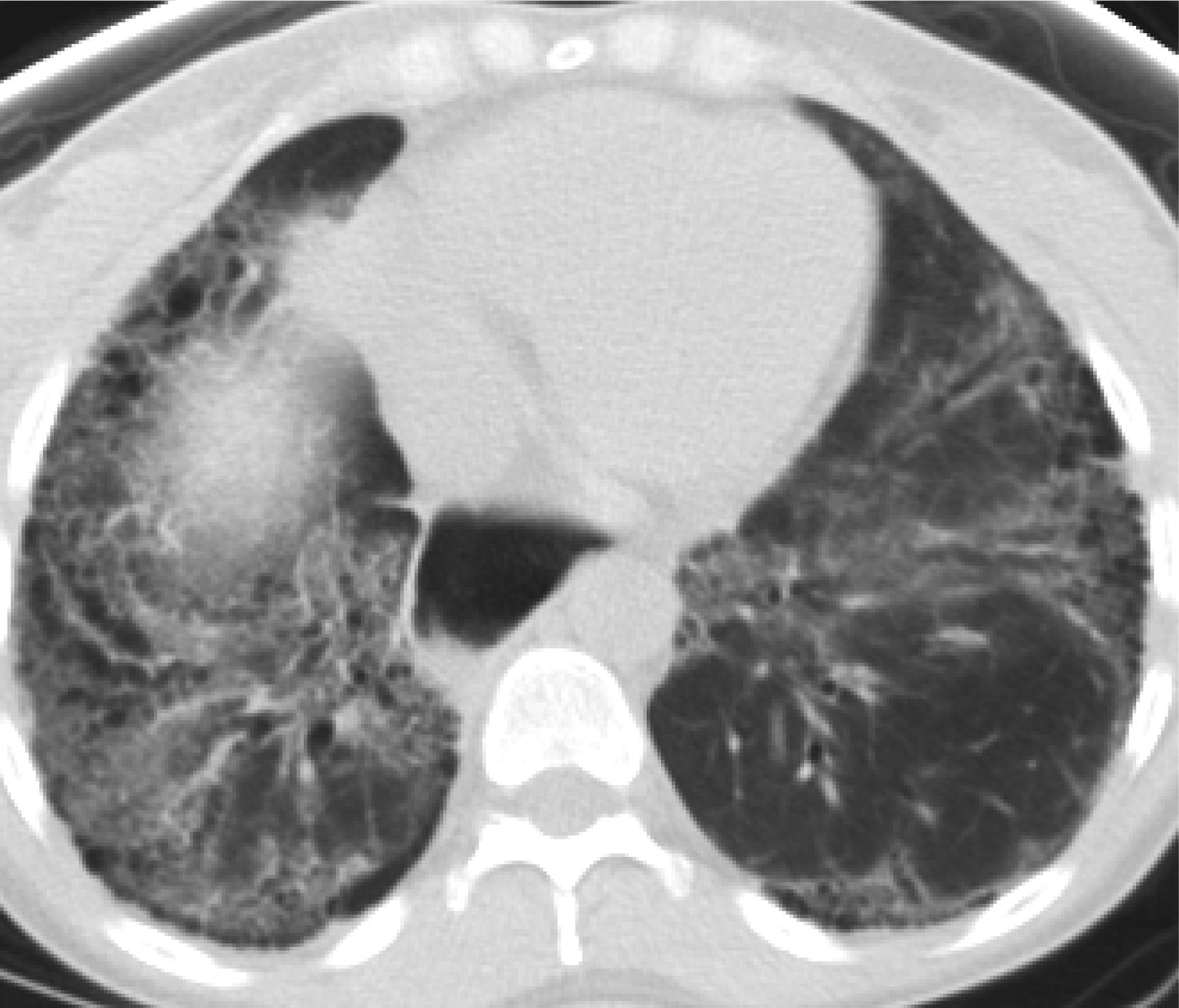
- Figure 4.
Cellular nonspecific interstitial pneumonitis (NSIP) is associated with ground glass opacities and has minimal volume loss. Cellular NSIP is more likely to respond to steroid treatment.
- Figure 5.
Fibrotic nonspecific interstitial pneumonitis (NSIP) has less ground glass opacity and more volume loss then cellular NSIP. The dilated esophagus in this photograph points to the cause of fibrosis, which was scleroderma.
- Figure 6.
Chronic hypersensitivity pneumonitis (CHP) is upper-lobe predominant, airway centered, and frequently has air trapping. The most useful feature radiographically is its airway-centered distribution seen on this image.
- Figure 7.
Stage 4 sarcoidosis is an upper-lobe predominant fibrosis, which helps to differentiate it from usual interstitial pneumonitis (UIP). In addition, it is not peripheral but instead is airway centered.




Tables
Lab Test Implications When Elevated Anti-nuclear antibody Collagen vascular diseases Rheumatoid factor Rheumatoid arthritis Anti-Scl-70 antibody Systemic scleroderma Anti-centromere antibody Limited cutaneous scleroderma Anti-synthetase antibody Dermatomyositis Polymyositis Anti-synthetase syndrome Anti-Ro (SS-A) antibody Sjögren syndrome Lupus erythematosus Anti-La (SS-B) antibody Sjögren syndrome Lupus erythematosus Antiribonucleoprotein Mixed connective-tissue disease LUPUS erythematosus Aldolase Dermatomyositis Polymyositis Creatine kinase Dermatomyositis Polymyositis Erythrocyte sedimentation rate Collagen vascular diseases Anti-cyclic citrullinated peptide Rheumatoid arthritis Pulmonary Radiology Treatment UIP Older age Subpleural Anti fibrotic medications Male sex Basilar predominant Consider referral for lung transplant soon after diagnosis as course is unpredictable and inexorable Smoking history Honeycombing Anti-inflammatory and immunosuppressive Rx NOT indicated (may be harmful) Crackles at lung bases Clubbing NSIP Younger age Homogeneous Anti-inflammatory medications Female sex Bronchovascular Consider referral for lung transplant if advanced disease Connective tissue disease Lower lobe Positive serologies Dilated esophagus Peripheral sparring CHP Older age Peribronchiolar fibrosis Anti-inflammatory medications Female Air trapping Removal of causative antigen Bird owner Upper lobe Consider referral for lung transplant if advanced disease Mold exposure S4 Younger age Upper lobe posterior Anti-inflammatory medications Less symptomatic Calcified lymph nodes Consider transplantation for advanced disease (PHN, hypoxemia, declining PFT's) Peribronchiolar fibrosis CHP, chronic hypersensitivity pneumonitis; NSIP, non-specific interstitial pneumonitis; S4, stage 4 sarcoidosis; PFT, Pulmonary Function Test; PHN, pulmonary hypertension; UIP, usual interstitial pneumonitis.
IPF NSIP CHP S4 Clinical presentation 74-year-old male with history of smoking, cough, and progressive DOE 45-year-old female with history of connective tissue disease and shortness of breath 68-year-old female. male with shortness of breath and parakeet/parrot (hobbies/occupations) 30-year-old male with cough, DOE Absent history of smoking Exams Crackles at lung bases on physical exam Evidence of rash on extensor surfaces. Squeaks and airway sounds as well as rales testing for sensitivity to antigens causing fibrosis Restrictive, obstructive or mixed pulmonary function tests Digital clubbing Capillary testing of fingers Restrictive pulmonary function tests with decreased DLCO Hx of sarcoidosis or evidence of granulomatous inflammation and multisystemic involvement Restrictive pulmonary function tests with decreased DLCO Restrictive pulmonary function tests with decreased DLCO Radiology Subpleural basilar predominant fibrosis with honeycombing compatible with ATS criteria for a UIP pattern Lower lobe fibrosis which follows the bronchovascular bundles and is homogeneous. Sometimes there is peripheral sparring Heterogeneous fibrosis that follows the bronchovascular bundles with slight upper lobe predominance Upper lobe posterior fibrosis sometimes with calcified mediastinal lymph nodes There is usually air trapping Treatment Anti-fibrotic medication Anti-inflammatory medications Anti-inflammatory medications Anti-inflammatory medications Pulmonary rehabilitation Rheumatology consult Removal of antigen causing disease if known Treat esophageal reflux disease Role of transplant Referral for transplant evaluation early after diagnosis or for progressive disease Referral for transplant evaluation for advanced disease Referral for transplant evaluation for advanced disease Referral for transplant evaluation for advanced disease CHP, chronic hypersensitivity pneumonitis; DLCO, Diffusion Capacity of Lungs for Carbon Monoxide; DOE, dyspnea on exertion; IPF, idiopathic pulmonary fibrosis; NSIP, nonspecific interstitial pneumonitis; S4, stage 4 sarcoidosis.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Content Usage and the Most Frequently Read Articles of 2018
- Healthcare utilisation and costs in the diagnosis and treatment of progressive-fibrosing interstitial lung diseases
- Presentation, diagnosis and clinical course of the spectrum of progressive-fibrosing interstitial lung diseases
- Interventions Must Be Realistic to Be Useful and Completed in Family Medicine