
Article Figures & Data
Figures
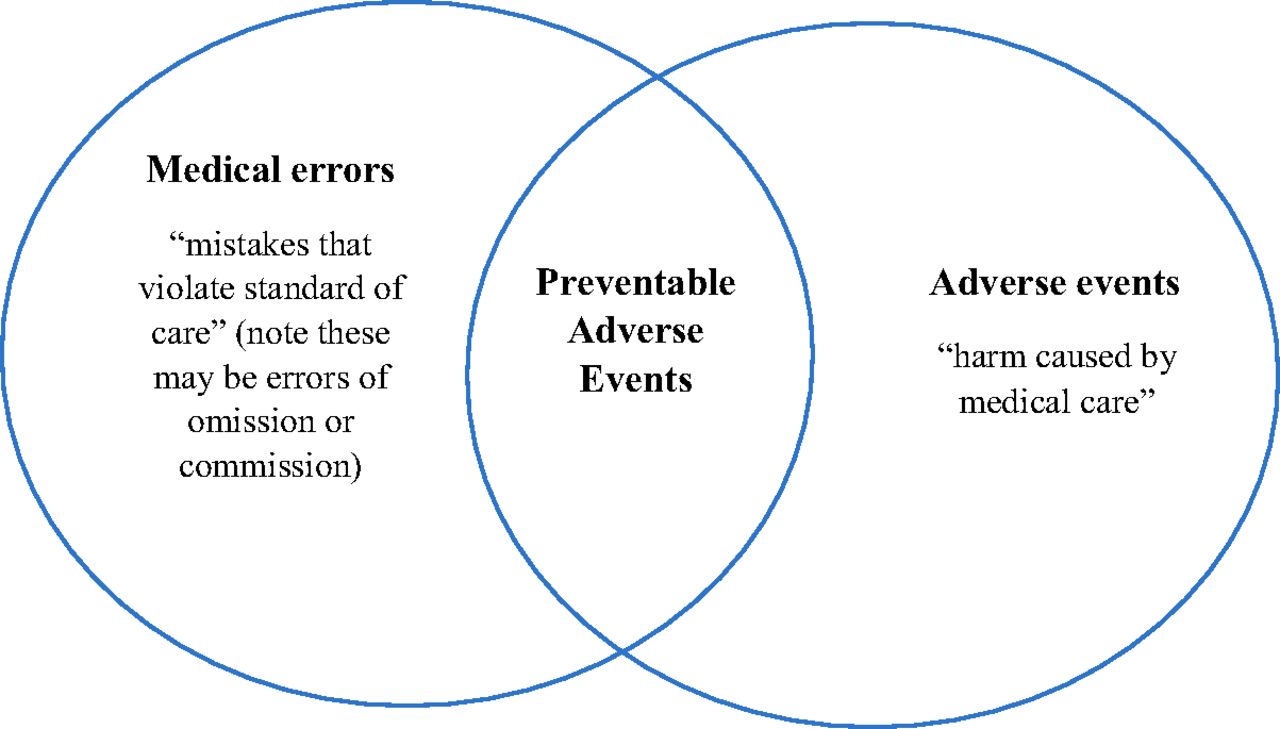
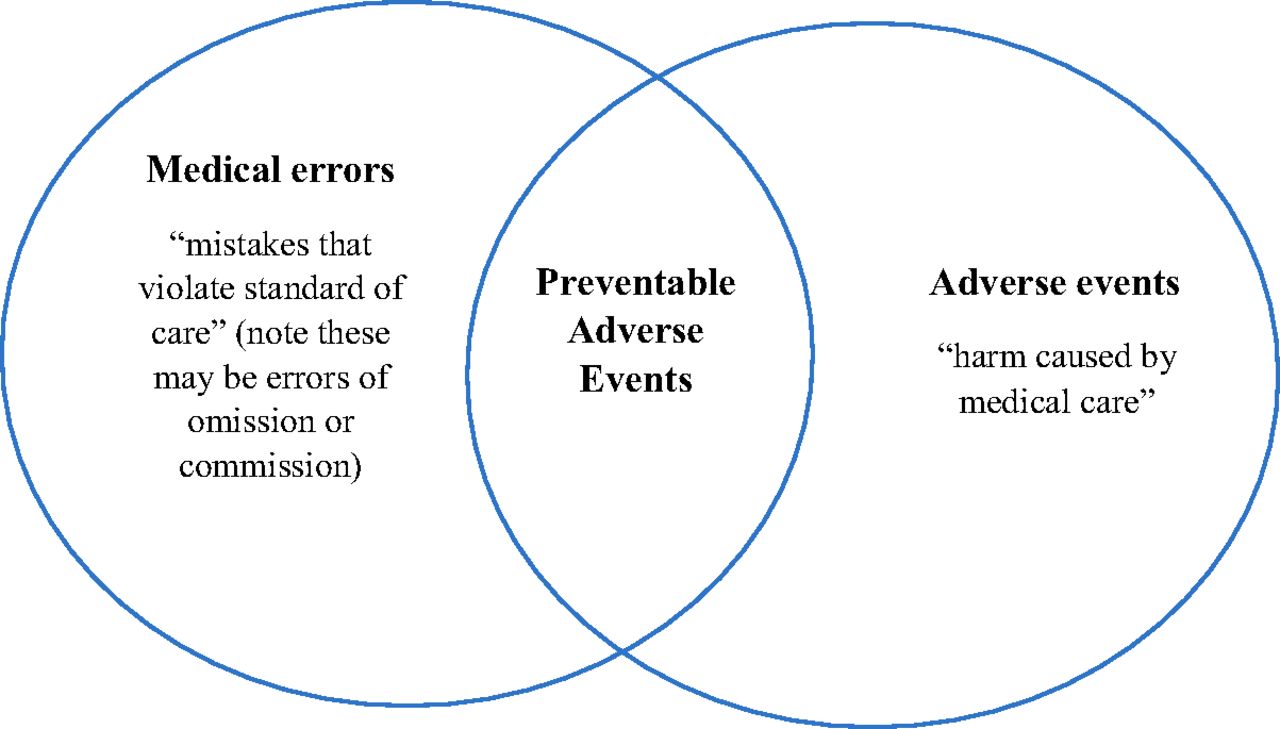
- Figure 1.
Venn diagram of relationship between medical errors, adverse events (AEs), and preventable adverse events (pAEs).
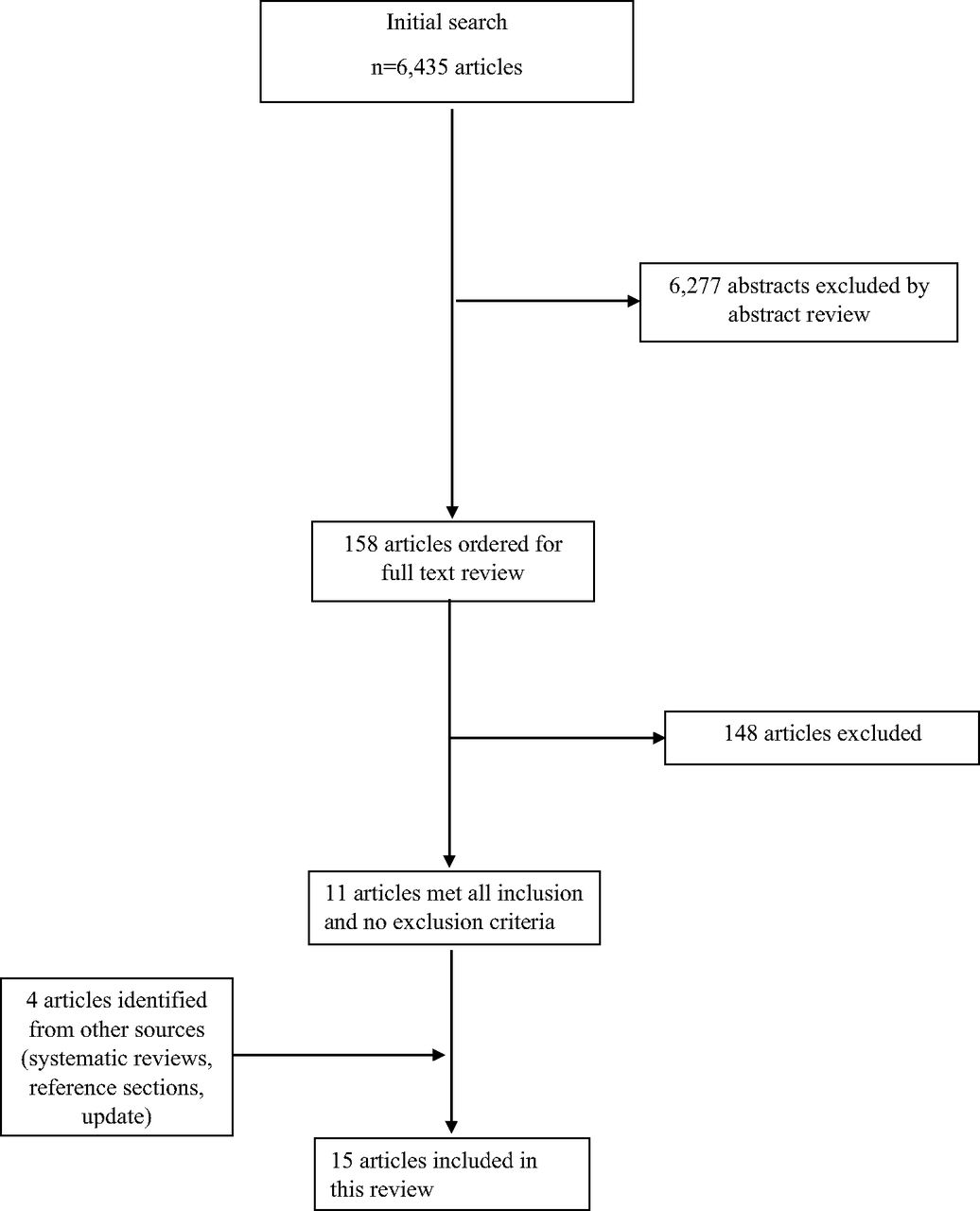
- Figure 2.
Flow diagram for selection of articles in a systematic review of trigger tools for identifying preventable adverse events (pAEs) in the outpatient setting.

Tables
- Table 1.
Summary of Studies included in a Systematic Review of Trigger Tools to Identify Preventable Adverse Events in the Outpatient Setting
First Author Last Name Patients (N) How pAE Was Measured AEs Evaluated pAE Detection Rate Triggers Used (Details within Footnotes) No. of Triggers Manual Review (M), Computerized Data Method (C), or both (B) Bigby et al.36 General, from discharge records (N = 527) Screened by investigator, reviewed by 3 blinded, independent physicians Any pAE, classified as drug or follow-up related 9% preventable admissions* Hospital admission 685 emergency admissions C Brenner et al.37 Adults seeking primary or urgent care, mean age 55 (N = 516) Independent chart review by 2 physicians pADE 0.64% pADEs 13.5% ameliorable Abnormal lab results† 1342 triggers (1322 excluded) C DeWet et al.20 Urban PC (N = 500) Record review, initially independent (5 physicians and 2 nurses) Any pAE 5.4% for pAE,9.4% for AE >3 visits per week, >10 consults per year, laboratory abnormalities, ED visit, hospital admission‡ 730 triggers M Field et al.33 Medicare enrollees over 65 years old who received health care in one of the group practices Chart review, screened by pharmacist, reviewed by 2 independent physicians pADE 1.8% pADE rate 9.2% after pharmacist screening Hospitalization, ED visit, and abnormal lab result§ 23,917 triggers B Gandhi et al.38 General patients with at least one visit to the clinic, mean age 47 to 48 years old (N = 68,013) Charts screened by “trained reviewers”, then reviewed by 2 independent clinicians including at least one physician pADE 0.7% overall 0.1% for laboratory rules 0.05% for drug-laboratory rules Abnormal lab results¶ 48,479 “incidents projected” for all triggers B Hibbert et al.34 Patients aged >75 years old who had attended the practice at least 3 times over 6 months (N = 428) Manual review by trained nurse Any pAE 4.8% pAE, not separated >3 visits per week, hospital admission, ED visit, abnormal laboratory result‖ 273 records with one or more triggers M Honigman et al.39 General patients with at least one visit (N = 23,064) Chart review by 4 independent physicians Any pADE 38% overall Abnormal laboratory results*** 1,802 abnormal labs, 25,056 overall C Lederer et al.40 All patients on warfarin Chart reviewed by Pharmacist, verified by physician Grade C-I (harmful) pADE related to warfarin use Approximately 13% Abnormal lab (INR), also monitored for ED or hospital admission related to warfarin use†† Unclear C Macnee et al.41 General patients with one of five predefined “untoward events” (N = 1,111) Chart review/screening medical charts by trained nurses or medical record room staff “Untoward event”: hospitalization related to missed cancer diagnosis due to inadequate care 84% for breast cancer 92% for rectal cancer Hospital admission for missed cancer diagnosis‡‡ 507 patients with untoward events related to missed cancer C Mathew et al.42 Nursing home residents >60 years old with CKD (N = 5,449) Research database (SPARCS: Statewide planning and research cooperative) Potentially preventable hospitalizations (ambulatory care sensitive hospitalizations) 29.3% (Sensitivity = 57.9%, Specificity = 48.9%) Polypharmacy§§ 2,883 patients with polypharmacy C McKay et al.35 175 “high risk” patients with COPD or ischemic heart disease or homebound and 345 patients >7 years old with ischemic heart disease (N = 520) Chart review by physician trainees Any “patient safety incident” 7.7%, not separated >3 consults, medication change, hospital admission, ED visit, abnormal labs¶¶ 468 triggers M Obreli-neto et al.43 Patients ≥60 years old (N = 433) Manual review, consensus of majority of at least 3 pharmacists Drug-drug interaction related pADEs 0.9% (13% preventable, 87% ameliorable), not separated Abnormal laboratory results‖‖ 433 triggers M Payne et al.44 Adults with long term chronic conditions (N = 180,815) National Health Service data Preventable admissions, defined by standard NHS Scotland list 19.5% for >6 medications 24.8% for >10 medications Polypharmacy*** 18,495 > 6 medications, 8250 > 10 medications M Rev Prescrire31 Discharged from general medicine or surgical wards (N = 2,946) Chart review Any pAE 1.80% Hospitalization††† 2,946 patients hospitalized Unclear Singh et al.17 Elderly patients with cardiovascular disease (N = 1,289) Chart review by unblended physician/pharmacist teams pADE 24% in all charts reviewed 9.3% for medication stop 16.3% for hospitalization 9.0% for ED visit 30.6% for abnormal laboratory Medication stop, hospitalization, ED visit, abnormal lab‡‡‡ 645 charts with at least one trigger, 383 charts reviewed M ↵* 2.2% due only to patient compliance, 6.8% due to iatrogenic or combination.
↵† INR, SCr, BUN, AST, ALT, and TSH undetectable while on levothyroxine.
↵‡ Old version of IHI Tool included new allergy code, new “high priority code.”
↵§ Drug levels, electrolytes, liver and kidney function, INR, blood counts, TSH, C. difficile, and HbA1C; also included provider incident reports and electronic note review.
↵¶ Also included ICD-diagnoses, free text note search, “miscellaneous rules”; potassium, INR, and SCr.
↵‖ INR, GFR, and Hgb.
↵** Multiple abnormal labs, also included text searches, allergy codes, and ICD-9 codes.
↵†† INR > 3 (also included if patient received Vitamin K).
↵‡‡ Hospitalization for breast or colon cancer; also assessed appendicitis ectopic pregnancy, and birth complications.
↵§§ >12 medications.
↵¶¶ Hgb and GFR; also included new allergy code, new “high priority code.”
↵‖‖ Also included subjective symptom review at follow-up visit.
↵*** Looked at polypharmacy for 4 to 6, 7 to 9, and >10 medications.
↵††† All patients admitted in a specific region of France.
↵‡‡‡ INR, TSH, SCr, BUN, ALT, AST, other labs with PPV < 5: drug levels, blood counts, K, Bili, ALP, C. difficile, HgbA1c, and antidote administration.
ADE, adverse drug event; AE, adverse event; ALP, alkaline phosphate; ALT, alanine transaminase; AST, aspartate transaminase; BUN, blood urea nitrogen; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; ED, emergency department; Hgb, hemoglobin; GFR, glomerular filtration rate; ICD, International Classification of Diseases; IHI, Institute for Healthcare Improvement; INR, international normalized ratio; pADE, preventable adverse drug event; pAE, preventable adverse event; PC, primary care; PPV, positive predictive value; SCr, serum creatinine; TSH, thyroid stimulating hormone.
- Table 2.
Institute for Healthcare Improvement18 Outpatient Adverse Event Trigger Explanations
Trigger 1: new diagnosis of cancer Treatment for cancer commonly requires surgery, chemotherapy, etc. This type of care has risks for adverse events related to the care, such as leukopenia from chemotherapy or surgical infection. Avoid wandering into the issue of omission, which can occur easily. For example, failure to do appropriate preventive measures and cancer diagnosis missed for a year is not an adverse event as defined in this tool because it is not an unintended consequence from care delivered. The tool is not meant to evaluate the appropriateness of care, but rather to determine if an adverse event did occur from the care which was delivered. Trigger 2: nursing home placement Determine if the placement was the result of an event, such as over sedation causing a fall and hip fracture or a surgical misadventure requiring long-term care. Trigger 3: admission & discharge from hospital Determine if the reason for admission was related to an event related to any health care interaction, either inpatient or outpatient. Trigger 4: 2 or more consultants in a year of review Multiple consultants can be the result of a medical misadventure. Look for unintended events from other care that required consultation with others afterwards. Trigger 5: surgical procedure Look for evidence of pulmonary embolism, deep vein thrombosis, wound dehiscence, infection, hemorrhage, hematoma, etc.—any of the unintended events that can occur from surgery either while the patient was in the hospital or after discharge. Trigger 6: ED visit Look for the reason for the visit, specifically for an adverse event related to other care that required ED care or events related to the ED visit. Trigger 7: Greater than 5 medications Evidence exists that patients taking greater than 5 medications have a high incidence of adverse medication events. Look for drug-drug interactions, particularly over sedation or overmedication, and development of toxicity. Trigger 8: physician change Look for an abrupt change from a mid-level provider to a physician or out of network referral. Was there an abrupt change in the physician in charge? What might that reason be? Look for adverse events. Trigger 9: complaint letter Look to see if the complaint related to an event (i.e., request for the waiver of co-payment, payment or concern about quality of care). Trigger 10: >3 nursing calls in 1 week Calls might all be related to one event. Trigger 11: Abnormal Lab Value Patients with results outside of range have greater risk of experiencing an adverse event. The lab value itself is only a trigger, so look for evidence of harm. Pay particular attention to lab values related to high-risk medications, such as INR >6 or Glucose <50. ED, emergency department; INR, International normalized ratio.
Section/topic No. Checklist Item Title Title 1 Identify the report as a systematic review, meta-analysis, or both. Abstract Structured summary 2 Provide a structured summary including, as applicable: background; objectives; data sources; study eligibility criteria, participants, and interventions; study appraisal and synthesis methods; results; limitations; conclusions and implications of key findings; systematic review registration number. Introduction Rationale 3 Describe the rationale for the review in the context of what is already known. Objectives 4 Provide an explicit statement of questions being addressed with reference to participants, interventions, comparisons, outcomes, and study design (PICOS). Methods Protocol and registration 5 Indicate if a review protocol exists, if and where it can be accessed (e.g., Web address), and, if available, provide registration information including registration number. Eligibility criteria 6 Specify study characteristics (e.g., PICOS, length of follow-up) and report characteristics (e.g., years considered, language, publication status) used as criteria for eligibility, giving rationale. Information sources 7 Describe all information sources (e.g., databases with dates of coverage, contact with study authors to identify additional studies) in the search and date last searched. Search 8 Present full electronic search strategy for at least one database, including any limits used, such that it could be repeated. Study selection 9 State the process for selecting studies (i.e., screening, eligibility, included in systematic review, and, if applicable, included in the meta-analysis). Data collection process 10 Describe method of data extraction from reports (e.g., piloted forms, independently, in duplicate) and any processes for obtaining and confirming data from investigators. Data items 11 List and define all variables for which data were sought (e.g., PICOS, funding sources) and any assumptions and simplifications made. Risk of bias in individual studies 12 Describe methods used for assessing risk of bias of individual studies (including specification of whether this was done at the study or outcome level), and how this information is to be used in any data synthesis. Summary measures 13 State the principal summary measures (e.g., risk ratio, difference in means). Synthesis of results 14 Describe the methods of handling data and combining results of studies, if done, including measures of consistency (e.g., I2) for each meta-analysis. Risk of bias across studies 15 Specify any assessment of risk of bias that may affect the cumulative evidence (e.g., publication bias, selective reporting within studies). Additional analyses 16 Describe methods of additional analyses (e.g., sensitivity or subgroup analyses, meta-regression), if done, indicating which were pre-specified. Results Study selection 17 Give numbers of studies screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally with a flow diagram. Study characteristics 18 For each study, present characteristics for which data were extracted (e.g., study size, PICOS, follow-up period) and provide the citations. Risk of bias within studies 19 Present data on risk of bias of each study and, if available, any outcome level assessment (see item 12). Results of individual studies 20 For all outcomes considered (benefits or harms), present, for each study: (a) simple summary data for each intervention group (b) effect estimates and confidence intervals, ideally with a forest plot. Synthesis of results 21 Present results of each meta-analysis done, including confidence intervals and measures of consistency. Risk of bias across studies 22 Present results of any assessment of risk of bias across studies (see Item 15). Additional analysis 23 Give results of additional analyses, if done (e.g., sensitivity or subgroup analyses, meta-regression [see Item 16]). Discussion Summary of evidence 24 Summarize the main findings including the strength of evidence for each main outcome; consider their relevance to key groups (e.g., healthcare providers, users, and policy makers). Limitations 25 Discuss limitations at study and outcome level (e.g., risk of bias), and at review-level (e.g., incomplete retrieval of identified research, reporting bias). Conclusions 26 Provide a general interpretation of the results in the context of other evidence, and implications for future research. funding Funding 27 Describe sources of funding for the systematic review and other support (e.g., supply of data); role of funders for the systematic review. ↵* From http://prisma-statement.org/PRISMAStatement/Checklist.aspx.
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med 2009;6(7):e1000097.
For more information, visit www.prisma-statement.org.
PICOS, participants, interventions, comparisons, outcomes, and study design.
- Appendix 2.
Search Strategy for a Systematic Review of Trigger Tools to Detect Preventable Adverse Events in the Outpatient Setting
Database: Ovid MEDLINE(R) 1946 to Present with Daily Update Search Strategy: 1 *ambulatory Care Facilities/ (9251) 2 ambulatory Care/ (37549) 3 outpatients/ (11353) 4 1 or 2 or 3 (56620) 5 “ambulatory care.”ti. (3118) 6 outpatient:.ti. (23080) 7 4 or 5 or 6 (66293) 8 primary health care/ (58821) 9 general practice/ or family practice/ or internal medicine/ (82748) 10 “primary care.”ti. (28235) 11 8 or 9 or 10 (139752) 12 medical errors/ or diagnostic errors/ or medication errors/ or inappropriate prescribing/ or medication reconciliation/ or near miss, health care/ (58395) 13 safety/ or patient harm/ or patient safety/ or safety management/ (60268) 14 Iatrogenic Disease/ (14236) 15 12 or 13 or 14 (125639) 16 (“patient harm” or “patient safety” or “near miss”).tw. (16137) 17 (avoidable or preventable or unintended).tw. (29878) 18 (harm or iatrogneic).tw. (25282) 19 “adverse reaction”:.tw. (23135) 20 “adverse event”:.tw. (83092) 21 “adverse drug event”:.tw. (2065) 22 “adverse drug reaction”:.tw. (8865) 23 (medication adj2 adverse).tw. (522) 24 unplanned.tw. (5392) 25 “critical incident”:.tw. (1508) 26 (error or errors or “Medical error”: or “medication error”: or “diagnostic error”:).tw. (180953) 27 harmful.tw. (33361) 28 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 (390278) 29 7 and 15 (1078) 30 7 and 28 (2601) 31 11 and 15 (1782) 32 11 and 28 (3592) 33 29 or 30 or 31 or 32 (7680) 34 limit 33 to English language (6808) 35 limit 34 to (comment or editorial or letter or news) (373) 36 34 not 35 (6435)




{kind=link}
{kind=link}