
Abstract
Introduction: Over 12% of US adults report past-year cannabis use, and among those who use daily, 25% or more have a cannabis use disorder. Use is increasing as legal access expands. Yet, cannabis use is not routinely assessed in primary care, and little is known about use among primary care patients and relevant demographic and behavioral health subgroups. This study describes the prevalence and frequency of past-year cannabis use among primary care patients assessed for use during a primary care visit.
Methods: This observational cohort study included adults who made a visit to primary care clinics with annual behavioral health screening, including a single-item question about frequency past-year cannabis use (March 2015 to February 2016; n = 29,857). Depression, alcohol and other drug use were also assessed by behavioral health screening. Screening results, tobacco use, and diagnoses for past-year behavioral health conditions (e.g., mental health and substance use disorders) were obtained from EHRs.
Results: Among patients who completed the cannabis use question (n = 22,095; 74% of eligible patients), 15.3% (14.8% to 15.8%) reported any past-year use: 12.2% (11.8% to 12.6%) less than daily, and 3.1% (2.9%–3.3%) daily. Among 2228 patients age 18 to 29 years, 36.0% (34.0% to 38.0%) reported any cannabis use and 8.1% (7.0% to 9.3%) daily use. Daily cannabis use was common among men age 18 to 29 years who used tobacco or screened positive for depression or used tobacco: 25.5% (18.8% to 32.1%) and 31.7% (23.3% to 40.0%), respectively.
Conclusions: Cannabis use was common in adult primary care patients, especially among younger patients and those with behavioral health conditions. Results highlight the need for primary care approaches to address cannabis use.
Cannabis is the most commonly used drug in the United States, after alcohol and tobacco.1 As of 2013, 13% of US adults—nearly 20 million people—used cannabis in the past year, and over 8 million used daily.1 Nearly 3 in 10 adults who use cannabis have a cannabis use disorder, defined as meeting 2 or more of 11 substance use disorder criteria (Table 1).2,3 The prevalence of a cannabis use disorder increases with increasing frequency of use.1,3,4
Diagnostic and Statistical Manual of Mental Disorders-5th Edition (DSM-5) Criteria for a Cannabis Use Disorder
With expanding legalization of cannabis use, the number of cannabis users—and daily cannabis users at greatest risk for a cannabis use disorder4—is projected to grow during the next 5 to 10 years.5 Medical cannabis use is now legal in 29 states and nonmedical use in 8 states, including California and the District of Columbia, with more states considering legalization.6,7 Sale of cannabis for nonmedical use, including dried plant materials and increasingly, a wide variety of highly-potent cannabinoid products, began in 2014 in Colorado and Washington State, with restricted startup sales beginning in 2015 for Oregon and in 2016 for Alaska.8,9 Yet, to our knowledge, cannabis use is not routinely assessed in US primary care settings. As cannabis use increases, primary care providers may want to know when patients use cannabis regularly.10
No US study has evaluated the population-based prevalence of patient-reported cannabis use among primary care patients, particularly in a state where nonmedical use is legal. Kaiser Permanente Washington (formerly Group Health), an integrated health system in Washington State, is currently implementing routine behavioral health screening as part of behavioral health integration in primary care clinics. At the request of providers, in the context of state legalization, a question about cannabis use was added to the behavioral health screen before a question about illicit drug use.11 The purpose of this study was to assess the prevalence and frequency of self-reported past-year cannabis use among primary care patients. Specifically, the prevalence and frequency of cannabis use is described in the total primary care sample, as well as within demographic and behavioral health subgroups. The study also addresses implications for primary care for patients who use cannabis.
Methods
Setting
Kaiser Permanente Washington, a nonprofit health care system with 25 primary care sites throughout Washington State, implemented annual behavioral health screening, including a question about cannabis use, for adults in 3 primary care sites starting in March 2015. Implementation of behavioral health screening was staggered across the 3 sites, which were chosen for their receptivity to implementation and community representativeness. The sites, spread across 90 miles in Western Washington, enrolled about 80,000 patients (17,000 to 37,000 per clinic). Site A initiated behavioral health screening in March 2015 (2 of 3 primary care clinics within the site); Site B initiated in early October (2 of 4 clinics); and Site C initiated in late October in (1 of 2 clinics). Staff at each site assisted with work flow development for behavioral health screening and met regularly to review and improve screening prevalence (target, 80%). Electronic health record (EHR) prompts alerted staff when patients were due for screening. After check-in, patients completed a 7-item behavioral health screen (described below) on paper. Medical assistants typically entered results into the EHR and shared the results with the provider before the patient-provider visit.
Data Source and Study Population
This observational cohort study obtained study data, including behavioral health screen results and patient demographic and clinical characteristics, from Kaiser Permanente Washington’s EHR. Patients 18 years and older were included if they attended an in-person visit with a primary care provider in 1 of the 3 participating primary care sites from study start (ie, after initiation of screening at each site) through mid February 2016. Patients with EHR documentation of a response to the cannabis question during the study period, indicating question completion, comprised the study sample. This study received approval and waivers of consent and HIPAA authorization from the Kaiser Permanente Washington Health Research Institute Institutional Review Board.
Measures
The 7-Item Behavioral Health Screen
Past-Year Cannabis Use.
The single-item cannabis use question, modeled after the third question of the World Health Organization’s (WHO) 10-item AUDIT12, asked about the frequency of past-year cannabis use (ie, “How often in the past year did you use marijuana?” —“never,” “less than monthly,” “monthly,” “weekly,” and “daily or almost daily”). The response options are identical to the second question of the WHO ASSIST questionnaire.13 A categorical variable for the frequency of past-year cannabis use was defined as none (“never”), less than daily (“less than monthly,” “monthly,” and “weekly”) and daily (“daily or almost daily”). Any response other than ‘never’ was considered positive for any past-year cannabis use. The term “marijuana” was used in the question as it is the most commonly used US cannabis term.14 Marijuana use was not defined and could include nonmedical and medical use.
Additional Behavioral Health Screen Items.
The 7-item screen also included the 2-item Patient Health Questionnaire (PHQ-2) to assess possible depression in the past 2 weeks (item scores 0 to 3; scores of 2 or 3 were positive for depression)15 and the 3-item Alcohol Use Disorders Identification Test–Consumption (AUDIT-C) questionnaire to assess unhealthy alcohol use in the past year (total scores of ≥3 for women and ≥4 for men were positive for unhealthy alcohol use).16 A single-item screen for frequency of past-year illicit drug use or nonmedical use of prescription medication, which followed the cannabis screen, was adapted from a validated screen11 and had response options identical to the cannabis screen, with any response other than “never” positive for past-year illicit drug use/medication misuse. In the uncommon case that a patient completed the 7-item screen more than once during the study period (2.4% of patients), the highest score for each condition-specific screen, if different, was used.
Demographic and Other Behavioral Health Conditions
Sex (women/men), age (18 to 29 years, 30 to 49 yers, 50 to 64 years, ≥65 years), race/ethnicity (Black, Hispanic, other, white, unknown)17 were extracted from the EHR at the time of each patient’s initial in-person visit to the sites during the study period. Behavioral health characteristics were selected based on their association with cannabis use. Current tobacco use was based on any EHR documentation in the year before initial visit that the patient reported currently using tobacco. Diagnostic codes based on ICD-9-CM (before October 1, 2015) and ICD-10-CM (as of October 1, 2015) documentation in the EHR by providers for conditions addressed or considered during an encounter were used to classify mental health and substance use disorders recognized in the year before the cannabis screen. Mental health disorders in the past year were categorized into major depressive disorders, anxiety disorders, including generalized anxiety, panic, phobias, and post-traumatic stress disorder, and serious mental illness, including schizophrenia, bipolar disorder, and psychosis. Substance use disorders in the past year were categorized into alcohol use disorders, cannabis use disorders, and other drug use disorders (ie, does not include nicotine, alcohol, or cannabis). Consistent with the use of the cannabis use question as routine clinical assessment of the frequency of use (ie, not as a diagnostic tool for a disorder), patients with a cannabis use disorder were included in the study. Composite indicators for any mental health disorder (eg, depression, anxiety, serious mental illness) and any noncannabis substance use disorder (eg, alcohol and other drug use disorders) were also evaluated.
Analyses
Analyses described sample characteristics, including the prevalence and frequency of past-year cannabis use. The prevalence and frequency of past-year cannabis use, along with 95% confidence intervals, were also calculated among patient subgroups based on demographic (eg, patients within each category of sex, age, and race/ethnicity) and behavioral health (eg, patients who screened positive on a behavioral health screen or had documentation of a behavioral health condition/diagnosis) characteristics.1 All analyses were conducted in Stata Version 13.1 MP edition.
Results
A total of 29,857 patients visited the 3 primary care sites during the study period, and of those, 22,095 (74.0%) patients had EHR documentation of the question about past-year cannabis use and were included in the study sample. Among patients who made a visit, those who completed the cannabis use question were similar to those who did not (data available on request).
Most patients in the study sample were female, white, and older; 9.7% reported current tobacco use and 15.0% had a major depression diagnosis in the past year (Table 2). Among patients in the sample, 15.3% (95% confidence interval, 14.8% to 15.8%) reported any cannabis use in the past year: 7.7% (7.3% to 8.0%) less than monthly; 2.2% (2.0% to 2.4%) monthly; 2.3% (2.1% to 2.5%) weekly; and 3.1% (2.9% to 3.3%) daily. Among those who reported any cannabis use, 50.1% (48.4% to 51.8%) reported infrequent use (less than monthly), 14.6% (13.5% to 15.9%) and 15.0% (13.8% to 16.2%) reported monthly and weekly use, respectively, and 20.3% (19.0% to 21.7%) reported daily use.
Primary Care Adult Patients Who Attended Pilot Sites and Were Screened for Past-Year Cannabis Use (n = 22,095)
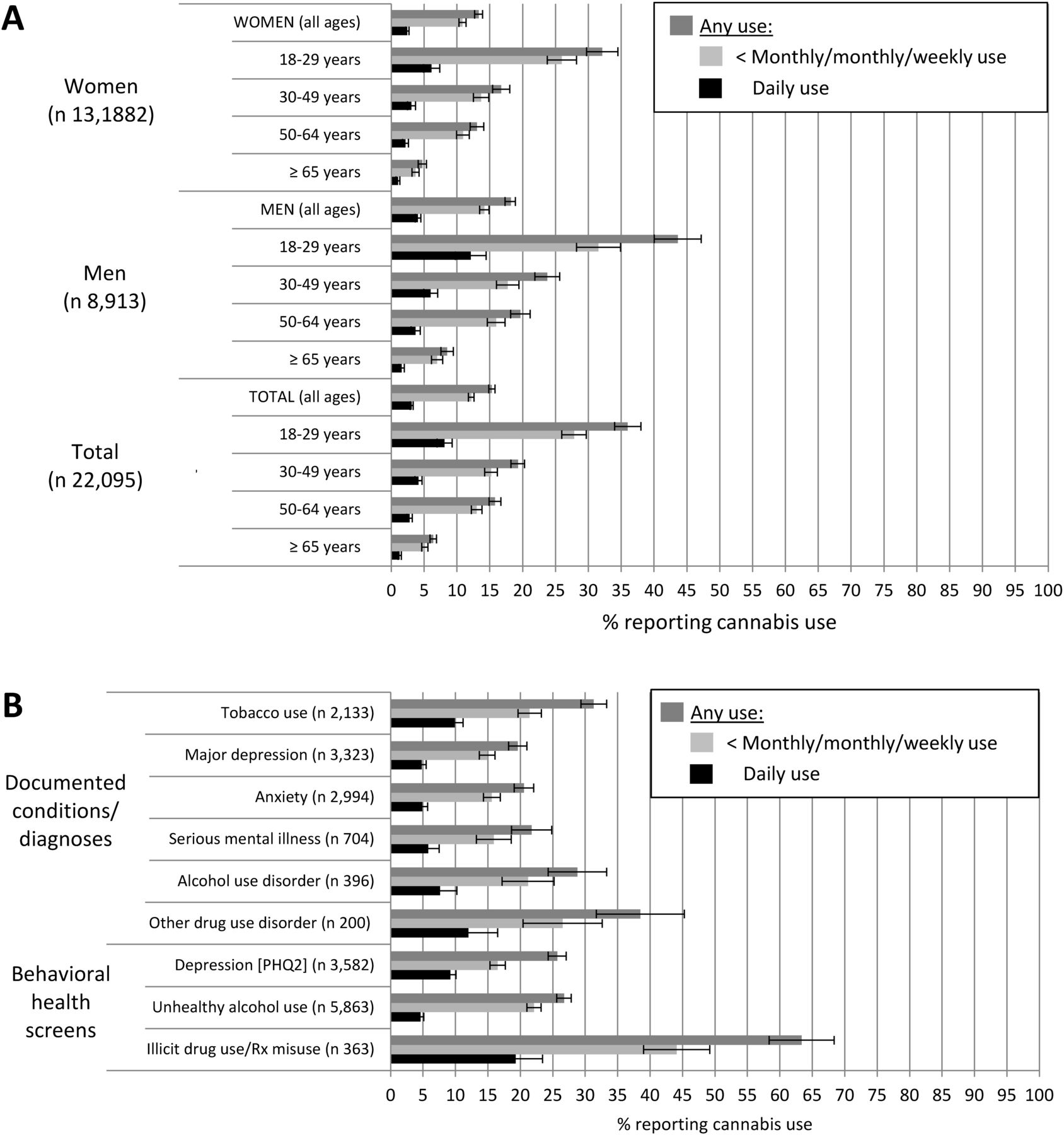
The prevalence and frequency of past-year cannabis use was high among men and patients 18 to 29 years old (Figure 1A). In particular, 32.1% (29.7% to 34.5%) of women age 18 to 29 years reported any cannabis use and 6.1% (4.9% to 7.4%) reported daily use, whereas 43.6% (40.1% to 47.2%) of men age 18 to 29 years reported any cannabis use and 12.1% (9.7% to 14.4%) daily use.
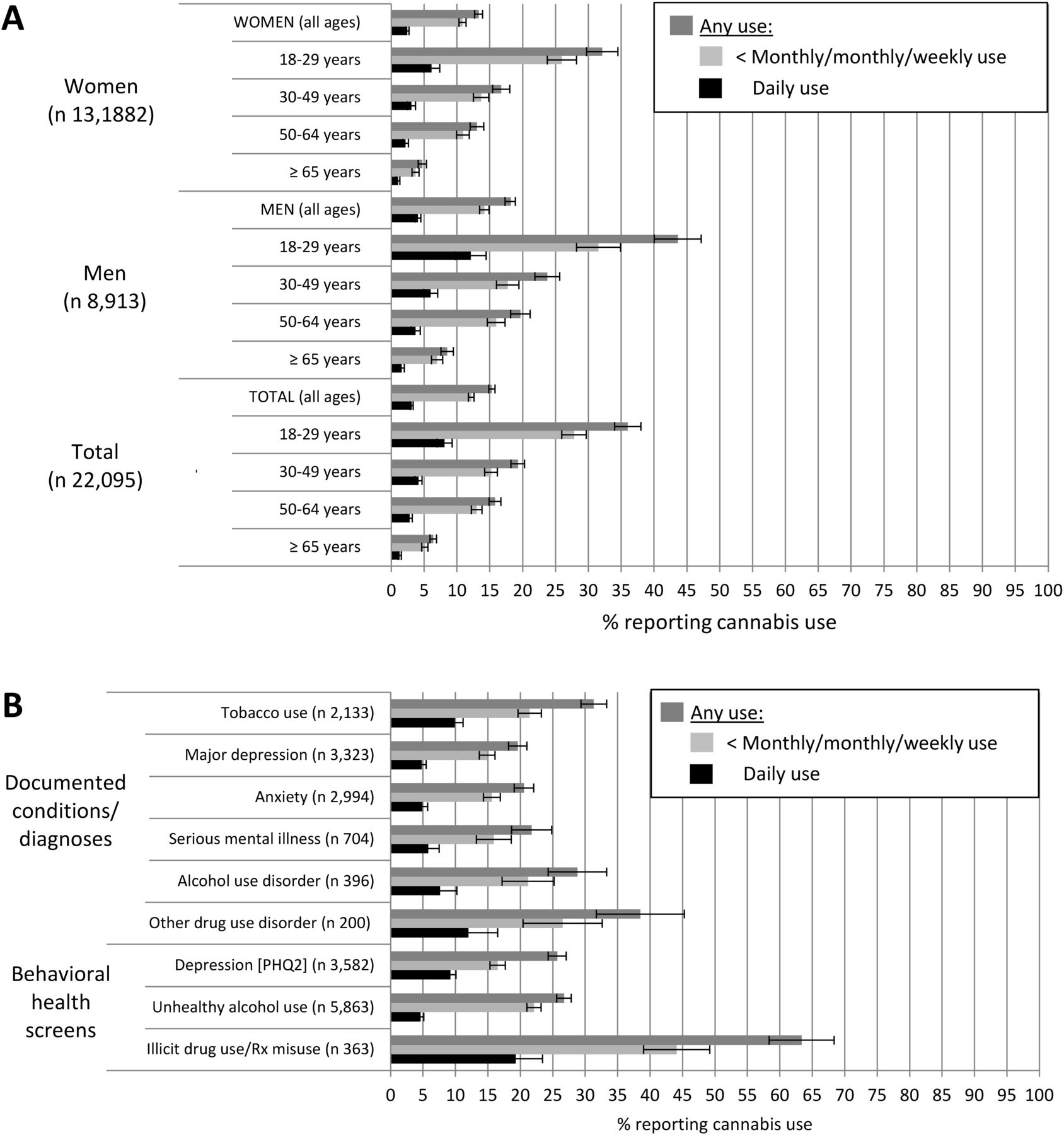
The prevalence of past-year cannabis use among patients in age and gender subgroups (A) and among those with a documented condition, diagnosis, or behavioral health screen (B). Note, any use is the summed total of monthly/monthly/weekly use and daily use. Documented conditions and diagnoses were in the year before the clinic visit. PHQ-2, Patient Health Questionnaire.
Compared with the prevalence among all primary care patients, any and daily past-year cannabis use was higher among patients in each behavioral health subgroup (Figure 1B). Among 5340 patients with a mental health disorder, 18.9% (17.9% to 20.0%) and 4.5% (3.9% to 5.0%) reported any and daily past-year cannabis use, respectively, while among 558 patients with a noncannabis substance use disorder, 31.0% (27.3% to 35.0%) and 8.4% (6.4% to 11.0%) reported any and daily past-year cannabis use, respectively. Among 109 patients with a cannabis use disorder documented in the past year, 84.4% (76.3% to 90.1%) and 49.5% (40.2% to 58.9%) reported any and daily past-year use, respectively.
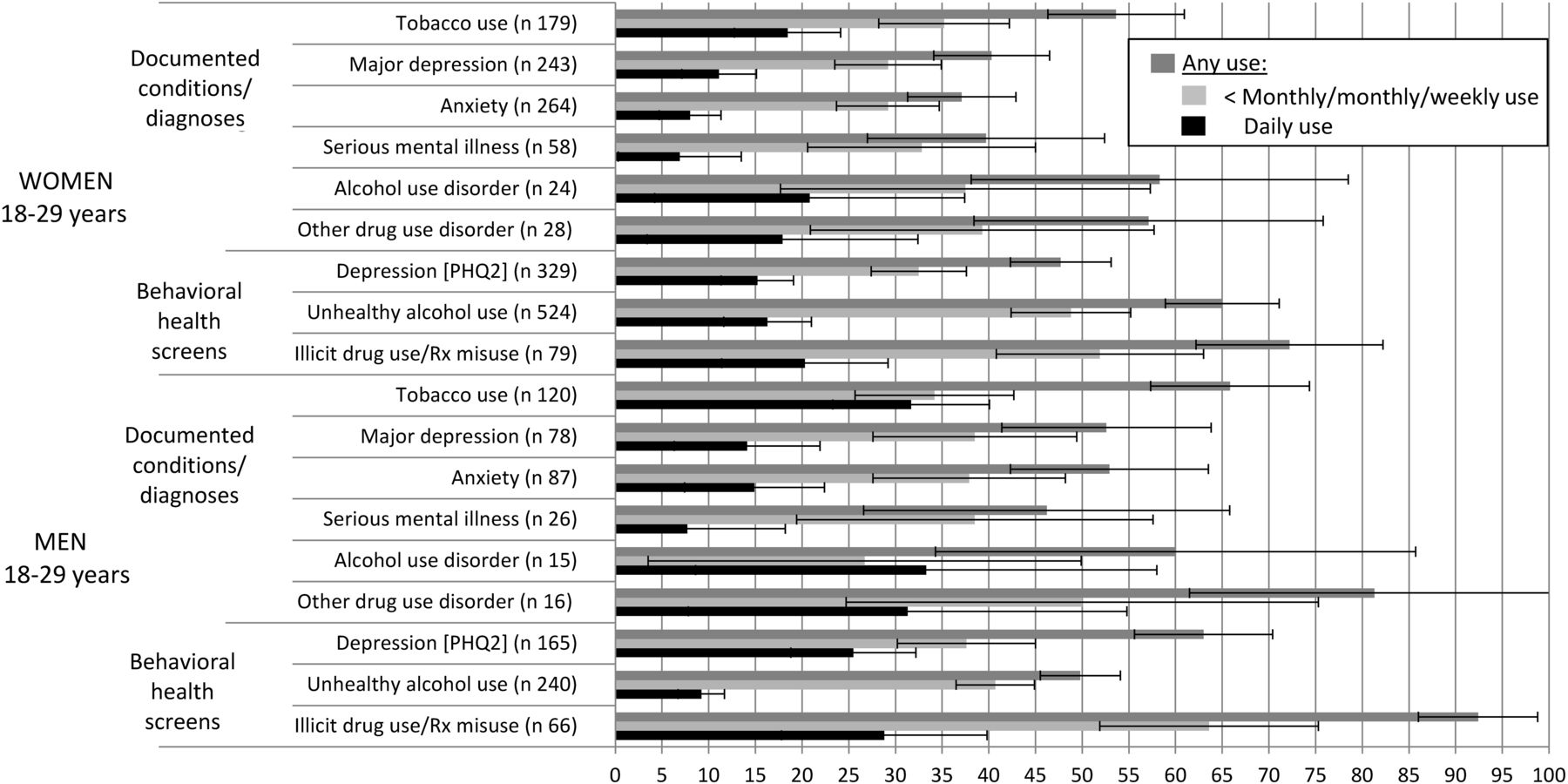
When patient characteristics were combined, the prevalence of cannabis use was higher in some groups (Figure 2; Appendix). For example, among men age 18 to 29 years who screened positive for depression or reported tobacco use, 63.0% (55.6% to 70.4%) and 65.8% (57.3% to 74.4%), respectively, reported any cannabis use, with 25.5% (18.8% to 32.1%) and 31.7% (23.3% to 40.0%), respectively, reporting daily use.

Among young patients 18 to 29 years old with a documented condition, diagnosis, or positive behavioral health screen, the prevalence and frequency of past-year cannabis Use. PHQ-2, Patient Health Questionnaire.
To identify patient characteristics independently associated with increased odds of past-year cannabis use, 2 post-hoc logistic regressions, with binary outcomes for any use and daily use, were performed and adjusted for all measured patient demographic and clinical characteristics.18 The adjusted odds of any use were higher among patients who were male, younger, current tobacco users, or had depression, anxiety, unhealthy alcohol use, or illicit drug use/prescription medication misuse, with similar results for daily use (Table 3). Patients age 18 to 29 years had the highest adjusted odds of any use and daily use, 7.34 (6.42 to 8.40) and 4.82 (3.67 to 6.31), respectively, when compared with patients 65 years and older.
Adjusted* Odds of Any and Daily Past-Year Cannabis Use by Patient Characteristic
Discussion
More than 1 in 6 primary care patients in a state where cannabis use is legal reported using cannabis when screened for depression, unhealthy alcohol use, cannabis and illicit drug use as part of routine behavioral health screening. Cannabis use was particularly common among young adults—nearly 4 in 10 reported past-year use—and among those with tobacco use, unhealthy alcohol use, illicit drug use, or mental health or substance use disorders. Daily cannabis use was reported by 1 in 12 young adults and nearly 1 in 20 patients with a mental health disorder. However, when multiple characteristics associated with use were combined (eg, young men who used tobacco or screened positive for depression), the prevalence of daily use exceeded 25%. These relationships persisted after adjustment, with younger patients and those with other substance use and behavioral health concerns having higher adjusted odds of any and daily cannabis use.
As states legalize use of cannabis, the perception that cannabis use is safe has increased.19,20 However, frequent and/or high-potency cannabis use—irrespective of the purpose—increases the risk of cannabis use disorder. Moreover, the concentration of tetrahydrocannabinol (THC), the main psychoactive and addictive component in cannabis, has increased in cannabis plants from an average of 3% to 12% in recent years, with some in excess of 20%, contributing to a higher prevalence of cannabis use disorders.21 New methods of administration and new products, including concentrated hash oil, synthetic cannabinoids, and edibles, have further increased the per-use potency of cannabis and the risk of addiction.22,23 More than 9% of lifetime cannabis users will develop and 25% to 50% patients who use daily are at risk for a cannabis use disorder.3,24,25 Young adults have the greatest risk, with 35% of current users meeting criteria for a cannabis use disorder.26 Young adults may also be most adversely impacted, as frequent use diminishes educational, occupational, cognitive, and social development.27,28 Patients who use cannabis for medical purposes, the majority of whom also use recreationally, are more likely to use multiples times per day and to use highly potent forms of cannabis to manage symptoms.8 All these factors increase the risk that patients who use cannabis will develop a cannabis use disorder.
Cannabis use poses other significant health risks, which increase with the frequency and intensity of use: 1) central nervous system impairment, acute (eg, judgment, coordination) and chronic (eg, memory, cognition)29, 2) exacerbation and persistence of psychiatric symptoms (eg, depression, psychosis) 30, 3) development of other drug use disorders, including nicotine and alcohol31, 4) prescription medication interactions (eg, antidepressants, opioids)32, 5) prenatal exposure during pregnancy33, 6) pulmonary symptoms29, and 7) accidents, particularly motor vehicle accidents.34 Finally, frequent use of cannabis can cause significant withdrawal, which appears clinically similar to tobacco and opioid withdrawal, with symptoms of anxiety, irritability, depressed mood, disturbed sleep, decreased appetite, and restlessness.35
Although cannabis use has established health risks, the US Preventive Services Task Force does not currently recommend routine preventive screening for cannabis or other illicit drug use in primary care due to the lack of known effective brief primary care interventions to decrease drug use.36 However, the value of asking about cannabis use, separate from brief interventions, has not been investigated. Results of this study suggest primary care patients are willing to report cannabis use, including daily use, as part of behavioral health screening documented in their EHRs.
Knowledge of patients’ cannabis use could help providers initiate conversations with patients, allowing for assessment of the reasons, perceived risks/benefits, and intensity of cannabis use. While cannabis may have therapeutic value for promoting appetite and treating nausea, spasticity, chronic pain, and neuropathic pain, providers may want to advise patients about more effective and/or safer treatment alternatives available for most conditions.27,37 In addition, there is inadequate evidence for the efficacy of cannabis use for some conditions/symptoms, such as depression and anxiety, which can be worsened by cannabis use.38 Because of the potential for harm, women should be advised against cannabis use during pregnancy.39 For patients who use cannabis regularly, assessment of the intensity (eg, frequency per day, method of administration) and potency of use, as well as symptoms of a cannabis use disorder using questionnaires such as the Cannabis Use Disorders Identification Test40 or DSM-5 substance use disorder criteria41 can provide additional information about a patient’s risk for cannabis-related consequences, including addiction.
For patients who have a cannabis use disorder, cognitive behavioral and motivational enhancement therapies are effective, separately and in combination, in reducing cannabis use and the severity of disorder symptoms.42,43 Contingency management can augment treatment outcomes when paired with these therapies.42,43 No medication has proven broadly effective nor been approved for treatment of cannabis use disorders.42 Most pharmacotherapies evaluated, including antidepressants, bupropion, buspirone, and atomoxetine, have shown little value in treating cannabis use disorders.44 Although gabapentin, N-acetylcysteine (NAC), especially NAC for 18-to-21-year-olds45, and medications containing THC have shown promise, further investigation is needed. As most patients with a cannabis use disorder will not seek care in formal treatment settings1,46, behavioral and other effective treatments for cannabis use disorders in primary care are needed.
There are several limitations to this study. Although the question about cannabis use was adapted from well-validated alcohol and substance use measures, it has not been validated against a standard interview for cannabis use. However, the question has high face validity, and underreporting is expected47, making estimates of the prevalence of any cannabis use in this study (15%) conservative. The prevalence of cannabis use in this study is higher than the national prevalence (12.5%)1, consistent with findings that the prevalence of use is higher in states with legalized use.48 Furthermore, the frequency of cannabis use among young adults in this sample of Washington State primary care patients is comparable to that reported by young adults in the same state on a 2014 confidential Internet-based survey.19 Although there was no evidence of selective nonresponse, a quarter of eligible patients did not complete behavioral health screening. Reasons included that medical assistants did not offer the screen (eg, were busy or staffing was low), patients did not speak/read English, or the primary care provider was behind schedule. The prevalence of cannabis and other substance use disorders in this study, based on documentation by clinicians in the EHR in the previous year, was low compared with US population estimates26,49, in contrast with rates for mental health diagnoses50, suggesting under-recognition of substance use disorders. Research is needed to determine whether routine assessment of cannabis and other drug use as part of behavioral health screening increases the prevalence of recognized substance use disorders. Although a question about frequency of past-year cannabis use was practical for routine screening, the question omitted relevant dimensions of use (eg, potency, frequency per-day, medical vs nonmedical use). Future studies of cannabis use among primary care patients need to assess differences in medical and nonmedical use and the intensity, potency, and methods of cannabis used. Finally, this study was restricted to adults and similar research is needed on younger patients.
In summary, this study of the prevalence and frequency of cannabis use among primary care patients, in a state with legalized use, found that most primary care patients who completed recommended routine behavioral health screening (eg, depression and alcohol)51,52, also completed a question about past-year cannabis use. In addition, while 15% of all primary care patients reported any past-year cannabis use, the prevalence was much higher in important patient subgroups. Most notably, more than 1 in 4 younger men who used tobacco or screened positive for depression reported high-risk daily cannabis use. Routinely asking about cannabis use could promote recognition of patients who may benefit from primary care discussions about their cannabis use.
Acknowledgments
Author Contributions: Dr. Lapham had full access to all the study data and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: Lapham, Bradley. Statistical analysis: Lapham. Interpretation of results: All authors. Drafting of manuscript: Lapham, Bradley. Critical revision of the manuscript for important intellectual content: All authors.
Appendix
The Prevalence and Frequency of Past-Year Cannabis Use among Patient Demographic and Behavioral Health Subgroups
Notes
This article was externally peer reviewed.
Funding: Awards from the National Institute on Drug Abuse (UG1DA040314-01S1, UG1 DA01581) and the Agency for Healthcare Research and Quality (R18 HS023173) supported the study implementation, analysis, and manuscript preparation.
Conflict of interest: DM was the principal investigator on research service agreements with Purdue Pharma and Alkermes. GTL, AKL, RMC, KCB, DDW, DRK, and KAB have nothing to declare. The sponsors had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
To see this article online, please go to: http://jabfm.org/content/30/6/795.full.
- Received for publication February 17, 2017.
- Revision received June 9, 2017.
- Accepted for publication June 17, 2017.




{kind=link}
{kind=link}