
Article Figures & Data
Figures
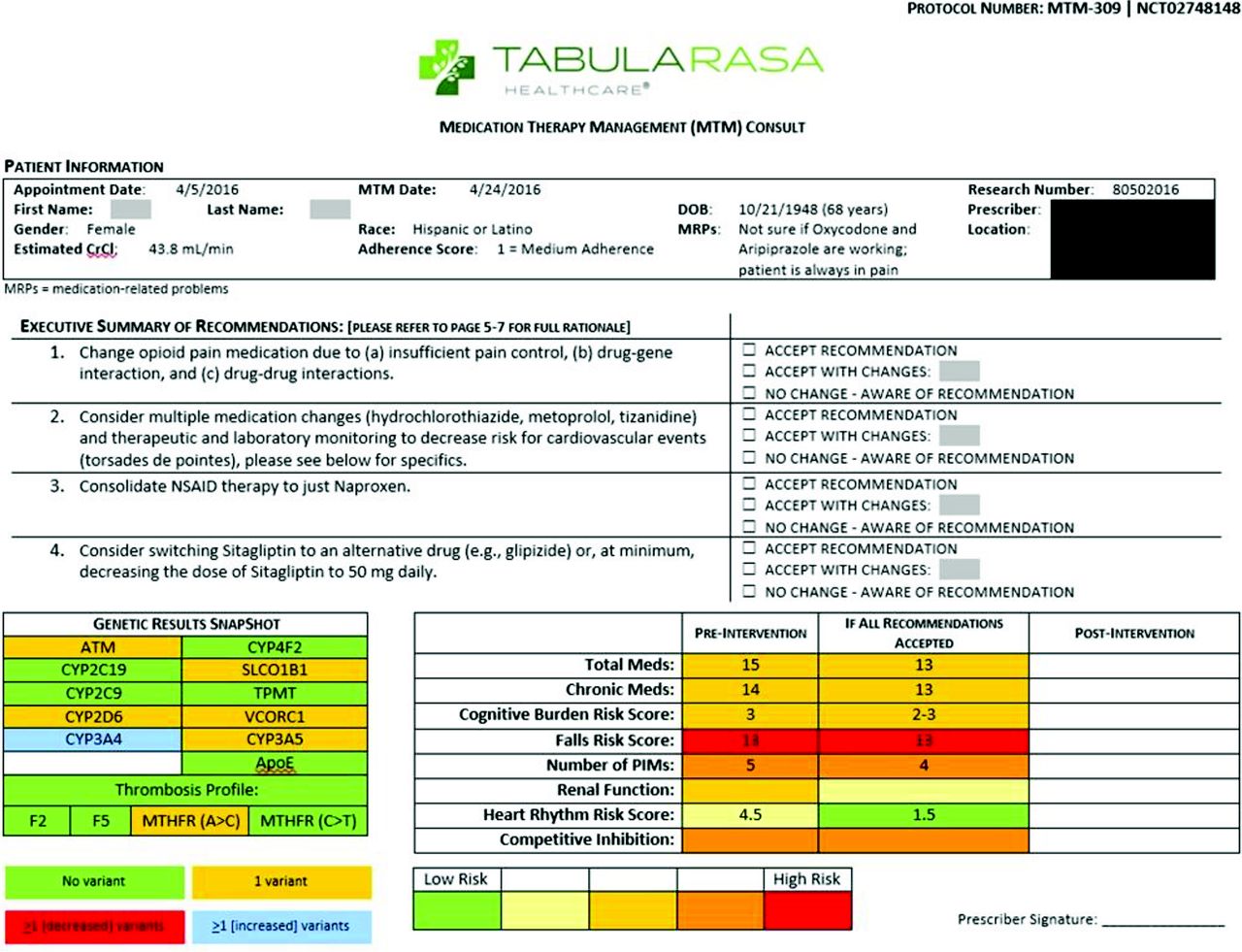
- Figure 1.
Flowchart of patient eligibility and enrollment process. In March 2016, the onsite research pharmacist reviewed 626 patient charts to determine eligibility for enrollment in the study. Among patients screened, 185 met inclusion criteria. However, approximately 50% of the time, either the pharmacist or patient was not available for informed consent. Among the 92 remaining eligible patients, 42 were excluded from enrollment in the study for various reasons. A total of 50 patients were enrolled and received medication therapy management (MTM) Plus services led by the pharmacist.
- Figure 2.
Medication Therapy Management (MTM) Plus process workflow. The MTM Plus process workflow employed the following steps: 1) evaluated medication utilization by performing medication reconciliation and assessing medication adherence; 2) performed PGx test by conducting informed consent specifically for the test, observing patient perform buccal swab for PGx test, and sending PGx test to laboratory with deidentified research number; 3) obtained additional patient-specific information from the EHR to inform the consult and documented this information into a secure, HIPAA-compliant form; 4) obtained PGx test results and matched them up to patient deidentified research number; 5) conducted consult, which was informed by clinical decision support data and PGx test results, and reviewed recommendations with a subgroup of a personalized medicine committee; and 6) shared consult, including PGx test results, with PCP. Abbreviations: EHR, electronic health record; MTM, medication therapy management; PCP, primary care physician; PGx, pharmacogenomics.
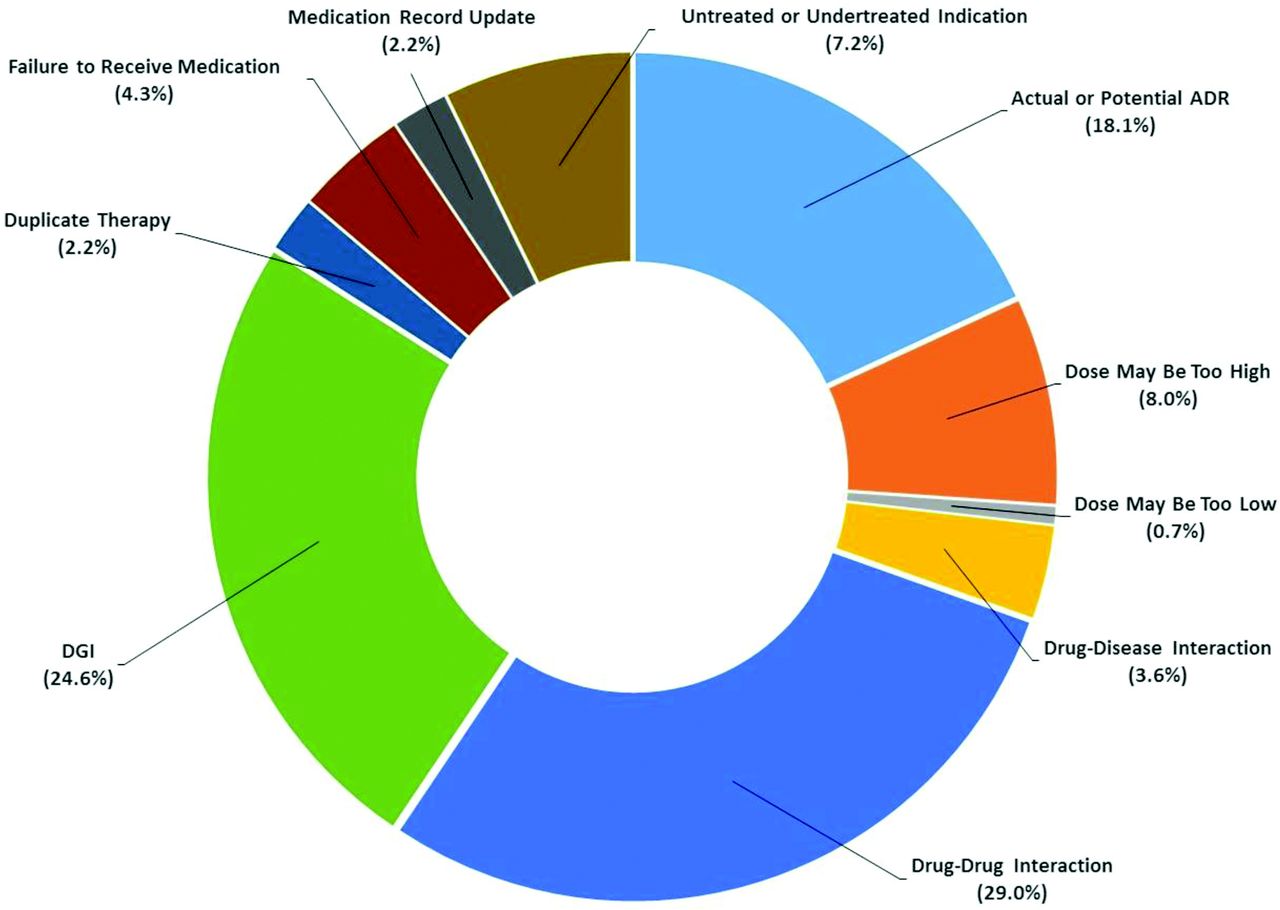
- Figure 3.
Types of medication-related problems identified by the pharmacist (N = 138). While performing consults, the pharmacist identified a total of 138 MRPs for the 50 patients enrolled onto the study. The most common types of MRPs identified were drug-drug interactions (29.0%), such as competitive inhibition involving 2 drugs (eg, metoprolol interfering with oxycodone activation) and multi-drug combination (eg, metoprolol and atorvastatin interfering with mirtazapine clearance), and DGIs (24.6%), such as inability to activate clopidogrel to its active metabolite and poor statin uptake into the liver. Abbreviations: ADR, adverse drug reaction; DGI, drug-gene interaction; MTM, medication therapy management; MRP, medication-related problem.
- Figure 4.
Types of recommendations made by the pharmacist (N = 138) and physician acceptance rates. For each MRP identified (N = 138) as part of the consult, the pharmacist made a recommendation for the PCP to resolve the MRP. The most frequent types of recommendations made were to monitor the patient (n = 38; 27.5%) and start alternative therapy (n = 35; 25.4%). Examples of monitoring recommendations included monitor for ADRs from nebivolol due to decreased CYP2D6 isoenzyme activity and monitor for side effects from mirtazapine due to multi-drug competitive inhibition. Examples of recommendations to start alternative therapy included switch clopidogrel to an alternative antiplatelet with a different metabolic pathway (eg, prasugrel or ticagrelor) due to a DGI and decrease dose of simvastatin or switch to an alternative statin (eg, rosuvastatin or pravastatin) due to a DGI. The majority of the pharmacist’s recommendations (90.9%) were accepted (ie, accepted or accepted with changes) by the PCPs. Abbreviations: ADRs, adverse drug reactions; DGI, drug-gene interaction; MTM, medication therapy management; MRP, medication-related problem; PCPs, primary care physicians.
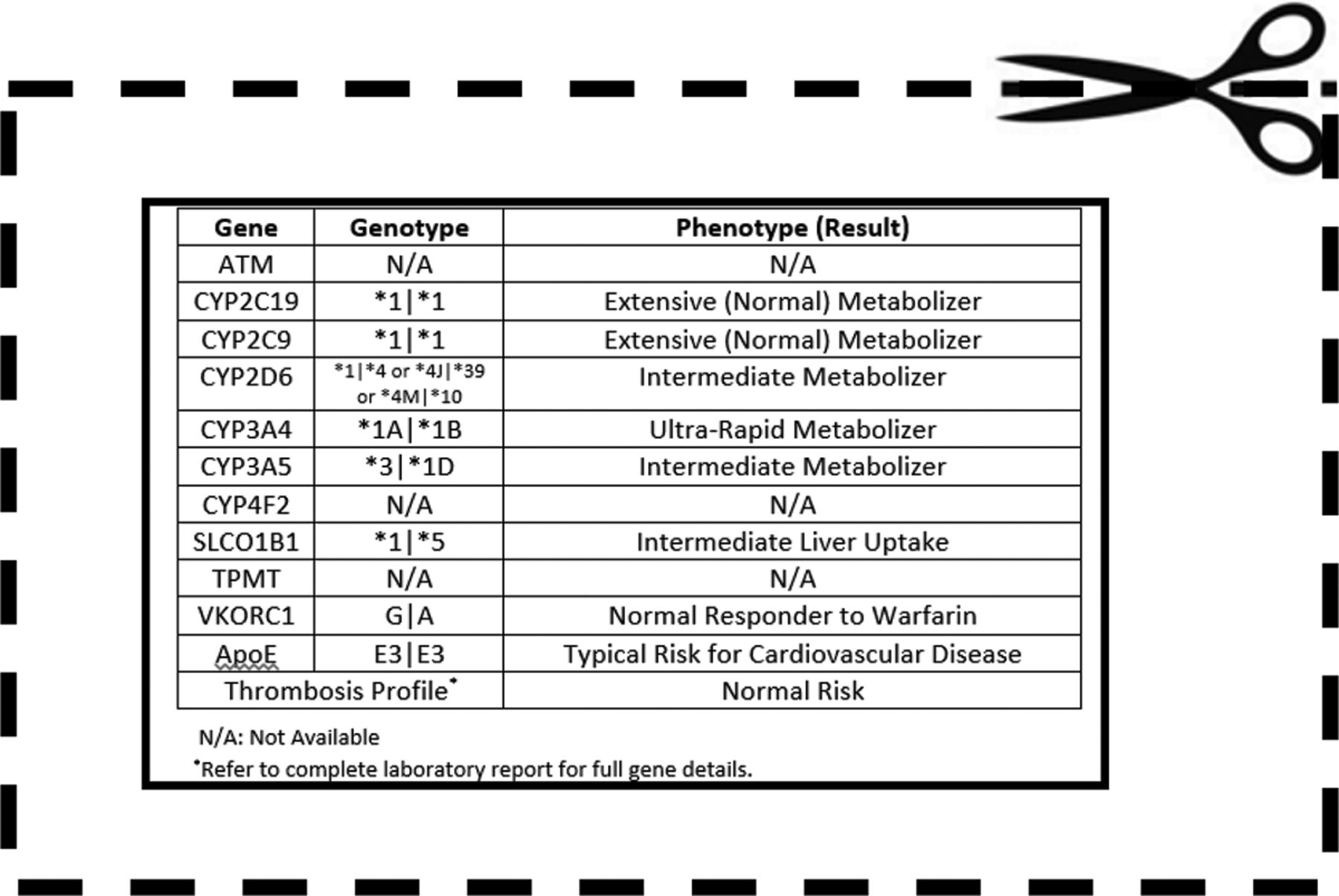
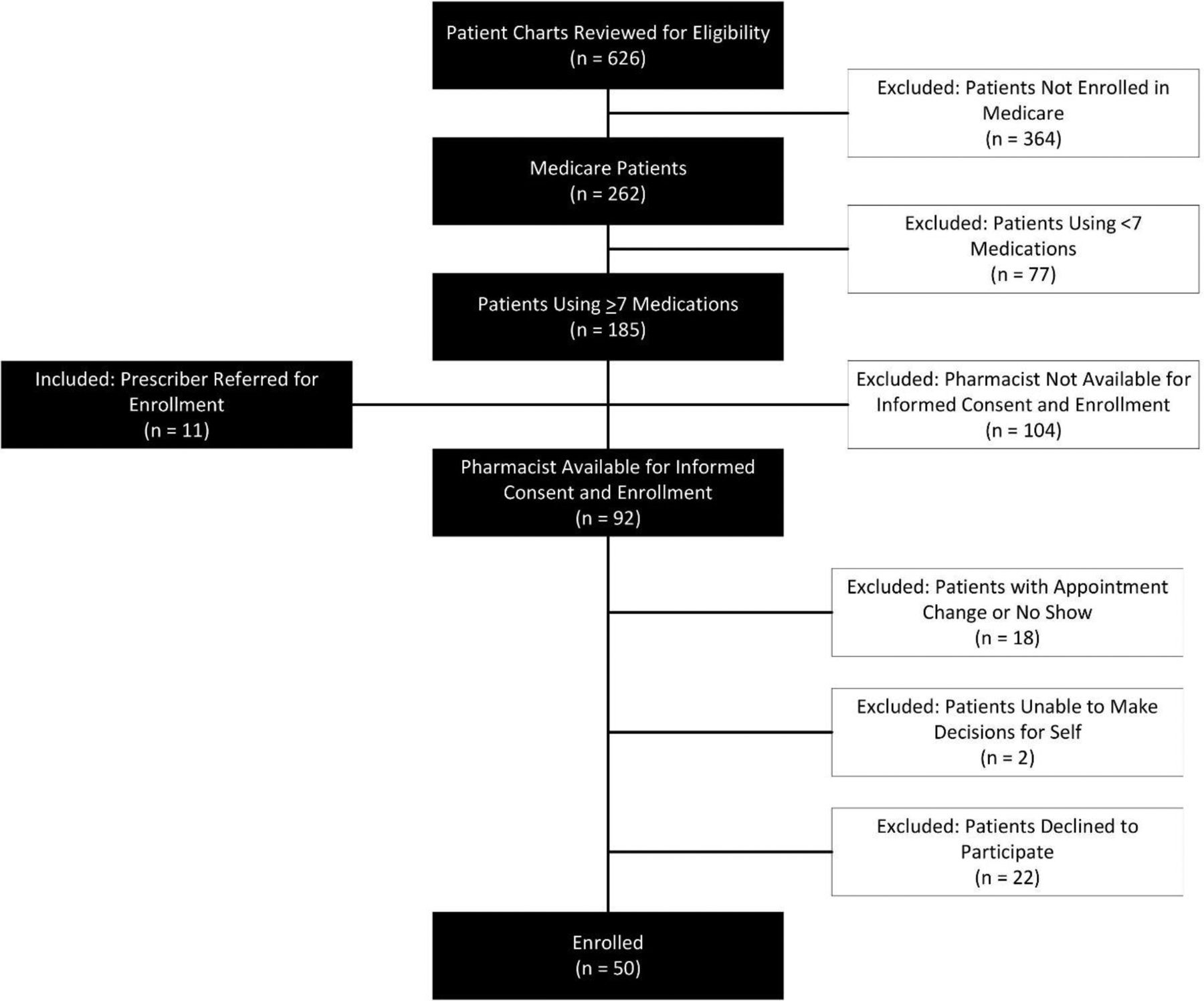
- Figure 5.
Phenotype distribution of the genes tested in 50 patients. All 50 patients who underwent PGx testing had at least 1 genetic variant, and the majority (66.0%) had ≥5. Notably, among the genes tested, 36.0% of patients were identified as rapid metabolizers for the CYP2C19 isoenzyme; 40.0% were considered intermediate or poor metabolizers for the CYP2D6 isoenzyme; 30.0% were determined to have reduced activity for the SLCO1B1 transporter; and 50.0% and 14.0%, respectively, were identified as having reduced and significantly reduced VKORC1 activity. (Reduced and significantly reduced refer to intermediate and poor phenotypes respectively as shown in the figure.) *Thrombosis profile included testing the following genes: F2, F5, MTHFR (A1298C), and MTHFR (C677T). Abbreviations: PGx, pharmacogenomics; CYP, Cytochrome P450.





Tables
Characteristics Value Demographics Age, years, mean (range) 69.0 (42.0 to 94.0) Sex, n (%) Male 27 (54.0) Female 23 (46.0) Ethnicity, n (%) White or Caucasian 42 (84.0) Hispanic or Latino 2 (4.0) Other or unspecified 6 (12.0) Most frequent diagnoses, n (%)* Hyperlipidemia 38 (76.0) Hypertension 38 (76.0) Type 2 diabetes mellitus 23 (46.0) Hypothyroidism 16 (32.0) Vitamin D deficiency 16 (32.0) Allergic rhinitis 11 (22.0) Anxiety 10 (20.0) Gastroesophageal reflux disorder 10 (20.0) Major depressive disorder 8 (16.0) Insomnia 7 (14.0) Medications Number, mean (± SD)† Total medications 12.1 (± 4.6) Chronic medications 10.4 (± 4.3) Medication risk mitigation–associated factors Cognitive burden risk score 2.0 (± 1.7) Falls risk score 5.5 (± 4.0) Number of PIMs 1.4 (± 1.2) Creatinine clearance (mL/min) 66.2 (± 20.8) Heart rhythm risk score 3.6 (± 3.6) Most frequently prescribed, n (%)‡ Aspirin 25 (50.0) Vitamin D 24 (48.0) Atorvastatin 23 (46.0) Levothyroxine 17 (34.0) Omega-3 fatty acids 14 (28.0) Amlodipine 13 (26.0) Esomeprazole 11 (22.0) Clopidogrel 8 (16.0) Metoprolol succinate 8 (16.0) Omeprazole 8 (16.0) ↵* As reported in the patient’s chart. Percentage out of total patients included.
↵† As determined by the pharmacist’s medication reconciliation process.
↵‡ As determined by the pharmacist’s medication reconciliation process. Percentage out of total patients included.
Abbreviations: PIM, potentially inappropriate medication; SD, standard deviation.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}