
Abstract
Purpose: Colorectal cancer (CRC) is the third leading cause of cancer death in the United States, yet 1 in 3 Americans have never been screened for CRC. Annual screening using fecal immunochemical tests (FITs) is often a preferred modality in populations experiencing CRC screening disparities. Although multiple studies evaluate the clinical effectiveness of FITs, few studies assess patient preferences toward kit characteristics. We conducted this community-led study to assess patient preferences for FIT characteristics and to use study findings in concert with clinical effectiveness data to inform regional FIT selection.
Methods: We collaborated with local health system leaders to identify FITs and recruit age eligible (50 to 75 years), English or Spanish speaking community members. Participants completed up to 6 FITs and associated questionnaires and were invited to participate in a follow-up focus group. We used a sequential explanatory mixed-methods design to assess participant preferences and rank FIT kits. First, we used quantitative data from user testing to measure acceptability, ease of completion, and specimen adequacy through a descriptive analysis of 1) fixed response questionnaire items on participant attitudes toward and experiences with FIT kits, and 2) a clinical assessment of adherence to directions regarding collection, packaging, and return of specimens. Second, we analyzed qualitative data from focus groups to refine FIT rankings and gain deeper insight into the pros and cons associated with each tested kit.
Findings: Seventy-six FITs were completed by 18 participants (Range, 3 to 6 kits per participant). Over half (56%, n = 10) of the participants were Hispanic and 50% were female (n = 9). Thirteen participants attended 1 of 3 focus groups. Participants preferred FITs that were single sample, used a probe and vial for sample collection, and had simple, large-font instructions with colorful pictures. Participants reported challenges using paper to catch samples, had difficulty labeling tests, and emphasized the importance of having care team members provide verbal instructions on test completion and follow-up support for patients with abnormal results. FIT rankings from most to least preferred were OC-Light, Hemosure iFOB Test, InSure FIT, QuickVue, OneStep+, and Hemoccult ICT.
Conclusions: FIT characteristics influenced patient's perceptions of test acceptability and feasibility. Health system leaders, payers, and clinicians should select FITs that are both clinically effective and incorporate patient preferred test characteristics. Consideration of patient preferences may facilitate FIT return, especially in populations at higher risk for experiencing CRC screening disparities.
Colorectal cancer (CRC) is a leading cause of cancer deaths in the United States.1 Screening for CRC aids in early detection and treatment of the disease.2,3 However, in 2015 only 63% of age-eligible adults were up to date with CRC screening, and 1 in 3 adults had never been screened.4,5 This is far behind the National Colorectal Cancer Roundtable goal to have 80% of age-eligible adults up to date by 2018.6 It also falls behind national screening rates for breast and cervical cancer (72% and 81%, respectively).7 Further, disparities in CRC screening persist among rural, minority, and low-income groups.5,8,9
To improve CRC screening rates and to facilitate early detection and treatment, national experts encourage shared decision making and promoting the message, “the best test is the one that gets done.”10,11 The United States Preventive Services Task Force (USPSTF) recommends multiple screening modalities for average-risk adults, including endoscopic (colonoscopy every 10 years; flexible sigmoidoscopy every 5 years) and annual home-based fecal testing options.12 Although colonoscopy is commonly used for CRC testing, many resource-challenged communities find that it is not practical for population-level screening.13,14 Colonoscopy is an expensive test that includes risk of intestinal perforation, requires specially trained medical staff, and has finite capacity, especially in rural areas.15⇓⇓–18 Patients may experience barriers to completing colonoscopies related to emotional (eg, fear) and logistic challenges (eg, costs, bowel preparation, transportation, time off work).19⇓⇓–22 Some patients, particularly those in populations experiencing low CRC screening rates, prefer home-based fecal testing.23⇓⇓–26
Fecal testing is an important component of population-level CRC screening programs,27 the success of which depends highly on participation rates.13,28 Fecal testing detects hidden (occult) or overt blood in the stool, identifies people who are more likely to have early stage CRC, and directs them to colonoscopy.5 More than 130 tests are approved by the US Food and Drug Administration (FDA) for the detection of fecal blood on the Clinical Laboratory Improvement Amendments (CLIA)-waived database as of June 13, 2017 (https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfCLIA/results.cfm). Although guaiac fecal occult blood tests (gFOBT) are cheap and efficacious, they are being replaced by fecal immunochemical tests (FITs) due to superior performance data and higher participation rates.27,29,30 Studies suggest that FITs may have greater adherence because they only require 1 or 2 stool samples and they do not require dietary or medication restrictions.31,32 However, limited research explores how patients perceive other test characteristics (eg, collection tool, instruction clarity) or allows patients to complete and to compare multiple FITs concurrently.
FITs vary in test effectiveness (eg, sensitivity and specificity)32,33 and other test characteristics (eg, cost, number of samples, collection tool). Although test effectiveness and cost may be primary motivators in FIT selection by clinics and health systems, specific test characteristics may be associated with patient willingness and ability to complete screening as recommended. In 2016, data to inform FIT selection was identified as a priority at Oregon CRC Roundtable. Beyond the number of samples required in a fecal test, we found a paucity of research identifying FIT characteristics associated with completion28 and little practical guidance for stakeholders regarding FIT selection. Therefore, we conducted this community-led research study to assess and describe patient preferences for FIT characteristics and to use our novel findings from user testing in concert with evidence on test effectiveness to inform selection of a single FIT that could be utilized by primary care and health system leaders in the study region to improve CRC screening rates.
Methods
This article utilizes data from Finding the Right FIT, a small-scale community-led study conducted from June 1, 2015 to November 30, 2016 with 3 aims: 1) understand patient preferences for FIT characteristics, 2) assess clinician preferences for CRC screening, and 3) evaluate clinical workflows for fecal testing for CRC. This article reports on findings related to patient preferences, which were assessed using a sequential explanatory mixed-methods design.34,35 First, we used quantitative data from FIT user testing to measure acceptability, ease of completion, and specimen packaging and adequacy. Second, we gathered qualitative data from focus groups to refine FIT rankings and gain deeper insight into the pros and cons associated with each tested FIT kit.
Study design, data collection, and analysis were driven by community-based team members (SC, BF, KC, CY, KD) with the support from academic partners (MD, RP). Our multidisciplinary team had expertise in primary care and community health, health system leadership, popular education and community engagement, and quantitative and qualitative research methodology. This study received approval from the Oregon Health & Science University Institutional Review Board (IRB No. 11893); we received a full waiver of the HIPAA Authorization of written consent. All team members involved in data collection and analysis completed Human Subjects training.
Regional Context and Study Setting
This study was led by community and academic partners associated with the Community Health Advocacy and Research Alliance (CHARA; see www.communityresearchalliance.org) and the Columbia Gorge Health Council (CGHC). The CGHC is governed by a board consisting of health care providers, community members, and other stakeholders.36 The CGHC oversees a clinical advisory panel, which consists of primary and behavioral clinicians who provide guidance on clinical standards and implement clinical priorities, and a consumer advisory council. The consumer advisory council includes representatives of the community and each county government served by the Coordinated Care Organization (CCO); Medicaid members must constitute a majority of the council's membership.37 The CGHC works in partnership with the Columbia Gorge CCO, 1 of 16 accountable care organizations in Oregon that provide coordinated systems of physical and behavioral health care for Medicaid recipients in their region.38,39 CCOs were established in 2012 and are accountable to the state through multiple financially-incentivized quality measures, including CRC screening.40,41 CRC screening rates across Medicaid members in Oregon's CCOs averaged 46.6% in 2015.41 The Columbia Gorge CCO's CRC screening rate was 47.3% in 2015.42
The Columbia Gorge CCO includes 2 counties in North-Central Oregon, part of the larger 6-county Columbia Gorge region that spans both Oregon and Washington. The region's 70,000 residents are mostly white, have lower incomes, and are older than the US average. In addition, some counties have up to 31.1% Latino residents and a significant number of undocumented and uninsured residents.42
Materials: FITs
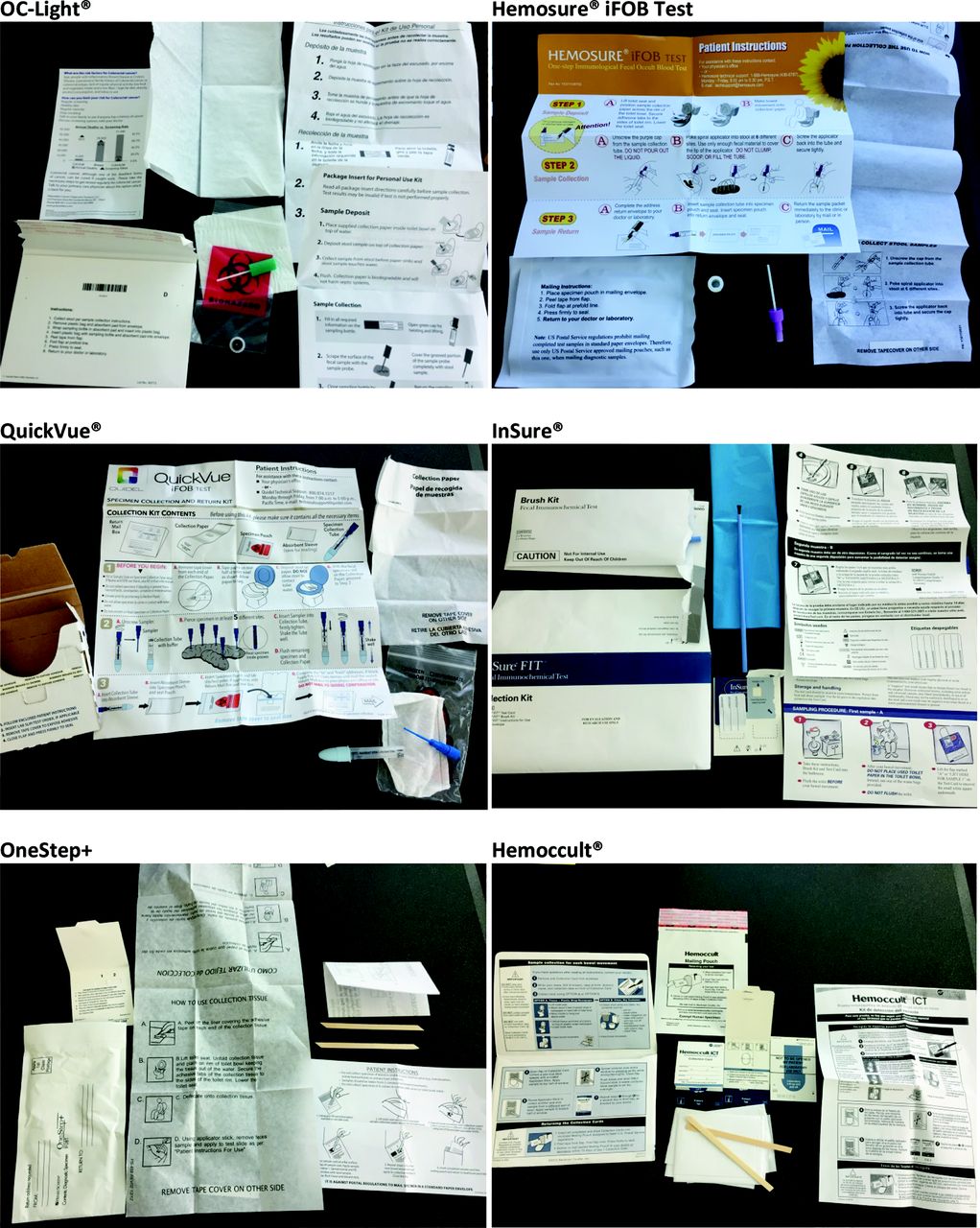
We worked with local primary care clinics and the clinical advisory panel to identify 6 FIT kits for inclusion, see Table 1. Five FITs (OneStep+, InSure FIT, QuickVue, Hemosure iFOB Test, Hemoccult ICT) were used by primary care clinics within the Columbia Gorge CCO. One FIT (OC-Light) was used widely by other CCOs in Oregon and being considered for use by a clinic in the study region. These FITs varied in terms of collection tools and methods, number of required samples, packaging, instructions, and clinical characteristics (see Table 1). Although laboratory processing of completed FITs was outside the scope of our current study, all 6 FITs were CLIA waived and could be manually processed at the point of care. We could not locate published data on clinical performance for 2 of the tests, QuickVue and OneStep+. Photographs of each FIT kit appear in Appendix 1.
Characteristics of FITs Identified for User Testing (Selection Date: Summer/Fall 2015)
Participants and Recruitment
We engaged local health and social service providers and a bilingual community health worker (BF) to assist with participant recruitment. We distributed English and Spanish recruitment fliers to consumer advisory council and clinical advisory panel members of the CCO and posted them in public health departments, primary care clinics, and local businesses. We also produced a study public service announcement that was broadcasted on a local Spanish-language radio station.
We sought to enroll up to 30 participants in user testing, with the intent to recruit at least 50% Spanish-speaking adults. Eligible participants were 1) residents in the Columbia Gorge region, 2) English or Spanish speaking, 3) uninsured or receiving government insurance coverage, and 4) age eligible for CRC screening (ie, 50 to 75 years). We originally targeted Medicaid patients in the CCO region, but we expanded eligibility to include participants in the broader Columbia Gorge region to increase the final sample size. We conducted an intake call to assess interest and eligibility. Eligible participants were invited to participate in user testing and a focus group. Participants received a $25 gift card for completing up to 3 FIT kits, a $50 gift card for completing 6 kits, and an additional $50 gift card for attending a focus group. Participants could elect to have 1 of the completed FITs returned to their primary care clinic for clinical processing and followup. Participants had to return at least 1 completed questionnaire and a FIT kit to be included in the final analysis.
Data Collection and Analysis
A bilingual community health worker (BF) enrolled participants, distributed FIT kits and questionnaires in a participant's preferred language (English or Spanish), and instructed them to complete the kits according to manufacturer instructions. Participants were instructed to place all completed kits and questionnaires in a single preaddressed mailer for return to study staff.
Questionnaires
For each FIT, participants were asked to complete a 20-item questionnaire that assessed ease of completion (eg, unpacking, mailing), instruction clarity, attitudes toward the process, and time to complete (see example in Appendix 2). Items on the questionnaire were gathered from existing instruments43,44 and revised using partner feedback to facilitate readability (Flesch-Kincaid Grade Level: 4.4). The questionnaire was reviewed by local partners for cultural literacy and translated into Spanish by a certified translator at a regional partner organization. Items employed Likert-style and open-ended response options. For the 13 fixed-response items, we calculated the percentage of participants who endorsed positively worded items (ie, “Agree” or “Strongly Agree”) and who did not endorse negatively directed items (ie, “Disagree” or “Strongly Disagree”). For each item, we then identified the highest and lowest performing kit(s) based on these percentages. Due to the small sample sizes, we provide descriptive statistics only. A sensitivity analysis found no significant diffidences in the probability of a favorable survey response for those completing 3 versus 6 kits. Open-ended response-options were categorized as “pro” or “con” and tabulated. Analyses were conducted using IBM SPSS Statistics 22.0.
Focus Groups
Three focus groups (1 English and 2 Spanish language) were facilitated by community health workers using a semistructured interview guide (see Appendix 3). Additional project staff attended focus groups to audio record each session, collect detailed field notes, and record FIT prioritization using flip charts. Focus groups lasted 90 minutes on average. The project manager (SC) and the community health worker (BF) used field notes and flip chart lists to prioritized FITs and identify characteristics that facilitated or impeded sample collection. Three team members (RP, MD, KD) conducted an inductive qualitative descriptive analysis to identify patient preferred FIT characteristics.45,46 This included an independent review of field notes followed by group meetings to review codes, reconcile discrepancies, and to identify and finalize emergent themes.
Specimen Adequacy Analysis
Participants could elect to have 1 completed kit returned to their primary care clinic for laboratory processing. All other returned FITs were included in a specimen adequacy analysis completed by a physician (KD) to assess 3 main attributes: 1) adequacy of the sample provided, 2) labeling of the specimen kit, and 3) packaging of kit for shipping. FITs that were returned to participants' primary care clinic for routine clinical care were excluded from the specimen analysis. Criteria for an adequate specimen collection were not included in the manufacturer instructions. Therefore, a descriptive specimen evaluation rubric was developed through an initial examination of kits returned by 5 participants, expert consultation, and input from the study team (Appendix 4); all kits were then evaluated in a single session. Specimens were rated for adequacy using a visual assessment of coloration in vial tests (clear, tan, or brown) or percentage coverage of a card's test area (more than 50%). In addition, we assessed whether participants attempted to label vials or cards as outlined in the instructions, and if different collection dates were noted for multi-day kits. Finally, we evaluated adherence to manufacturer instructions for repackaging completed kits.
FIT Kit Final Ranking
Two members of the study team (SC, KD) reviewed findings from the questionnaires, specimen evaluation, and focus groups to create a preliminary list of preferred tests and test characteristics. This list was reviewed by the full study team and refined using themes from the focus groups. Differences in FIT rankings were resolved through consensus.
Results
A total of 76 FIT kits and 76 questionnaires were completed by 18 participants (mean, 4 FITs per participant; range, 3 to 6 FITs). As summarized in Table 2, mean participant age was 56 years (range, 50 to 66 years), 50% (n = 9) were female and 56% (n = 10) self-identified as Hispanic. Over half of the participants received government subsidized health insurance including Medicaid or Medicare (61%); 3 participants (17%) were uninsured. Thirteen individuals attended 1 of 3 focus groups: 10 who completed FIT kits and questionnaires, 3 who had not (2 were 49 years old, 1 was 78 years old). Seven (54%) focus group participants were Hispanic.
Demographic Characteristics of Participants Engaged in FIT Testing and Focus Groups
Questionnaires
Participant agreement or disagreement with key statements about each FIT kit are summarized in Table 3. Participants reported the most challenges with the Hemoccult ICT kit, which employs a wooden stick for sample collection and requires multiple samples that are dried between collection days. The OneStep+ kit also employs a wooden stick, but was viewed as easier than completing the Hemoccult ICT. Participants generally responded positively to the other kits. Participants generally agreed with the statement that collecting the sample was quick (range, 60% to 92%) and reported that they felt confident that they completed the kit correctly (range, 64% to 86%). However, the majority of participants viewed kit completion as disgusting (range, 18% to 55% disagreed).
Participant Agreement with Statements about the FIT Kits on the Study Questionnaires
Overall, participants rated FITs that used probes for sample collection the highest. All respondents reported that the Hemosure iFOB Test and OC-Light probes were easy to use and that they had minimal problems with sample collection. Over 90% of participants found the InSure brush easy to use for sample collection. Although QuickVue and Hemosure iFOB has similar characteristics to OC-Light (ie, probe, 1 sampling day), participants rated OC-Light more favorably.
Focus Groups
Four themes emerged from focus groups pertaining to preferences for FIT characteristics and CRC screening. First, in contract to colonoscopy, participants liked that fecal tests could be completed at home, were convenient, generally easy to use, and required no preparation in advance. Second, participants preferred tests that required “1 trip to the bathroom” to complete and provided a grooved probe for collecting the sample. In contrast, they disliked collection sticks, multi-sample tests, and cards that required drying samples overnight. However, focus group participants raised questions about how much stool was needed to satisfy a sample, why some kits required 6 pokes while others only 1, and expressed concerns about the effectiveness of using the provided paper to catch the stool sample. Because participants experienced problems with the paper provided to hold the stool sample, they recommended using a pie tin or collection hats, such as those provided in hospitals. In addition, some participants wondered whether tests with more cards/samples were better able to detect CRC than single-sample tests. Third, participants preferred instructions printed in large font with colorful pictures and were appropriately translated. Specifically, Spanish speakers requested instructions written for Spanish readers instead of relying on automatic translation. In addition, focus-group participants noted that having a care team member or community health worker review the FIT with them was helpful in understanding how to complete the test and recommended creating instructional videos that could accompany the tests or available on YouTube. Finally, focus groups identified barriers to CRC screening irrespective of modality such as cost, fear, and cultural sensitivities. Participants stressed the importance of providing follow-up care and navigation support for colonoscopy scheduling to patients with abnormal FIT results.
Specimen Adequacy Analysis
Table 4 summarizes findings from the specimen evaluation of 66 returned FIT kits (86%) in relation to sample adequacy, labeling, and packaging; the remaining 11 FITs were sent to participants' primary care clinics for processing. Nearly all, 92% (33/36), vial-based kits had an adequate specimen (ie, liquid in the vial was tan or brown in color) whereas 80% (24/30) of card-based kits had an adequate sample (ie, specimen covered ≥ 50% of the test area). Many multi-sample cards, especially kits that required 2 samples on 1 card, appeared to have been completed with a single sample.
Descriptive Findings from the FIT Kit Specimen Adequacy Analysis (N = 66)
When participants attempted to write on vials that had preattached labels, their handwriting was often illegible. However, only 38% (5/13) of Hemosure iFOB Test kits were labeled compared with 86% (6/7) of InSure FIT kits. Kit packaging also varied widely. Overall, 64% (23/36) of vial-based tests were packaged correctly. Specifically, 83% (30/36) of the vial-based tests were properly returned in the biohazard bag, but only 55% (24/36) were wrapped in the absorbent pad. Packaging errors on vial tests included placing the vial directly in the mailer without enclosing in the biohazard bag and returning the vial without the absorbent pad included. Comparatively, 97% (29/30) of card based tests were packed according to manufacturer instructions with secured card flaps over the sample site with stickers. However, 2 of the mailing envelopes included waste materials from the kit, making them too heavy for mailing with the recommended postage.
Final FIT Ranking
As summarized in Table 5, the top 2 tests (OC-Light and Hemosure iFOB Test) utilized a probe and required a single sample. The third FIT (InSure FIT) required a brush and 2 days of sampling, yet ranked highly on all assessments in part due to a colorful and clear instruction sheet.
FIT Kit Rankings from Most to Least Preferred by Questionnaire and Focus Group Data
A. Combined Rankings for FIT Kit User Testing Data Sets
B. Test Characteristics for Overall FIT Kit Ranking
Discussion
Participants in our study clearly preferred FITs that use a probe and vial for collection, had simple instructions that include large font text and colorful pictures, and require only 1 sample. Participants had difficulty providing accurate and legible labeling on samples, and multi-specimen tests often seemed to have been completed with a single sample. Final FIT rankings from most to least preferred were OC-Light, Hemosure iFOB Test, InSure FIT, QuickVue, OneStep+, and Hemoccult ICT. In addition, participants provided suggestions for kit improvement, described the benefit of having care team members provide verbal instructions for FIT completion, and stressed the importance of providing follow-up care and navigation support for patients with abnormal results. Attending to patient preferred FIT characteristics may facilitate patient return, clinical processing, and thus improve CRC screening rates and ultimately reduce cancer morbidity and mortality.
Current guidelines and national recommendations emphasize helping patients use the CRC screening modality that best suits their preferences.10,11 Our study evaluated FITs, which before fall 2016 were 1 of 3 screening modalities recommended by the USPSTF.12,47 In the United States and internationally, FITs are replacing older gFOBT options as the standard of care for home-based fecal testing for CRC due to superior performance data and higher participation rates.27,29,30 Currently, 132 different tests are cleared for use in the United States by the FDA for the “detection of blood” in the stool. We assessed 6 FITs that were actively being used by primary care clinics within 1 region. However, 2 of the selected FITs did not include published data on clinical effectiveness. A 2013 study by Daly and colleagues32 found that many FOBT/FIT products listed on the FDA website lacked publicly available proficiency testing information to help health-care professionals make informed decisions regarding test selection. An important consideration for future research is how to generate publicly available data on FIT effectiveness, and how best to support the adoption and use of FITs that are clinically effective and preferred by patients in practice.
Test effectiveness is a critical factor to consider when selecting a FIT kit. However, other physical test characteristics may determine whether patients complete these tests and if they do so correctly. Understanding how patients view the characteristics of FITs currently available on the market can inform product refinement and may facilitate completion. Previous research identified preferences for certain FITs, such as those that only require a single sample.31,48 Other studies have assessed patient perceptions of FIT/FOBTs and reason for completion.43,48⇓–50 For example, Gordon and colleagues49 identified nonusers discomfort in completing the kit and user suggestions to add disposable gloves, extra paper, and wider-mouth collection vials. However, no studies that we are aware of allow patients complete multiple FITs such that they can compare and contrast between them. Our study addresses key gaps in the research by identifying multiple characteristics that patients perceive make specific FITs easier to complete. Although initially our study set out to recommend a single FIT kit, we found that patients preferred test characteristics shared by more than 1 kit.
There are a few notable limitations in the present study. First, we tested 6 FITs that were actively used in the region and varied in their clinical effectiveness, 2 of which did not have publicly available data on clinical effectiveness. Health-system leaders should consider both clinical and physical test characteristics when selecting a FIT for local or regional use. In addition, there may be other FIT characteristics that merit evaluation. Second, we had difficulty recruiting users in our original target population. In response, we expanded our geographic range, included individuals beyond those covered by Medicaid, extended the recruitment timeframe, and implemented protocols to allow participants to return 1 test to their primary care practice for laboratory testing. Attending to these factors as well as asking patients to complete fewer FITs may facilitate recruitment in future studies. Third, our study was a small-scale community-based study primarily designed to inform FIT selection in 1 rural region. Although 76 FITs were completed, they were returned by 18 participants who all identified as either white or Hispanic/Latino. Future studies with a larger, more diverse participant sample could evaluate how FIT preferences differ by participant characteristics (eg, low vs higher socioeconomic status) and may reveal different preferences across racial/ethnic subgroups and regions. Lastly, although we allowed participants to send 1 kit for laboratory analysis, our assessment of sample adequacy used a qualitative rubric designed through expert consultation. Given that we assessed color and/or card coverage and instructed participants not to label tests with their names, actual laboratory processing may have resulted in different outcomes for sample completion.
Despite these limitations, we observed variation in participants' ability to complete and their perceptions of different FITs. Our findings add to the body of knowledge on patient perceptions of FIT acceptability and feasibility of use. Results—when used in concert with data on clinical effectiveness—can inform primary care clinicians, health-system leaders, and payers who seek to increase CRC screening through home-based fecal testing. In addition, findings provide important feedback for manufacturers who can improve kit characteristics (eg, collection method) and to refine the associated instructions to address patient concerns with completing the test (ie, what if sample gets wet). Although some systems and research teams have created pictographs or wordless instructions for low-literacy adults,51 changes by the manufacturer could support widespread distribution and uptake in low as well as high resourced settings. Finally, our results can advise the design of future studies that assess additional FIT kits in larger samples that extend beyond rural English and Spanish speakers and single geographic regions. These studies can offer more sophisticated analyses measuring adequacy of returned FITs and tease apart the association between FIT kit characteristics (eg, number of samples, collection method, instructions) on patient adherence in clinical practice.
Conclusion
Test characteristics influenced patient's perceptions of FIT acceptability and feasibility of use. Study participants preferred FITs that required only 1 sample, used a probe and vial to collect the sample, and had descriptive instructions with large font and colored pictures. Participants reported difficulty using paper to catch samples, had difficulty labeling tests, and emphasized the importance of having care team members provide instruction on test completion and offer follow-up support for patients with an abnormal result. Findings can be used by manufacturers to improve test characteristics and by researchers to inform larger-scale studies and intervention trials. When considered in concert with information on FIT effectiveness, clinics and health systems can use our results to inform test selection.
Acknowledgments
We thank our study participants and the various community partners who supported study recruitment. The Columbia Gorge Health Council served as the fiscal agent, provided time for staff participation, and supported engagement of the Columbia Gorge Coordinated Care Organization's Community Advisory Council and Clinical Advisory Panel. The Community Health Advocacy and Research Alliance (CHARA) provided training and infrastructure that enabled the current study. Gloria Coronado, PhD helped team members identify and procure FITs. Staff from Nuestra Comunidad Sana at The Next Door, Inc. created community flyers and translated Spanish surveys. FITs used in this study were donated by the manufactures: Beckman Coulter, Polymedco, Henry Schein, Hemosure, Enterix (also known as Clinical Genomics USA), and Quidel. We appreciate the assistance of Eliana Sullivan with manuscript revisions and Katrina Ramsey with quantitative analysis.
Appendix

Images and Materials Associated with Each FIT Kit Tested (N = 6 FITs)
Notes
This article was externally peer reviewed.
Funding: This study was funded in part through a research grant from the Oregon Health and Science University Knight Cancer Institute Community Partnership Program (ID No. CPP.2014.07). Dr. Davis is partially supported by an Agency for Healthcare Research & Quality patient centered outcomes research (PCOR) K12 award (Award K12 HS022981 01). The Community Health Advocacy and Research Alliance (CHARA) was developed through a series of Pipeline to Proposal Awards from the Patient Centered Outcomes Research Institute (ID 7735932, 7735932-A, 7735932B). The findings and conclusions in this study are those of the authors and do not necessarily represent the official position of the funders.
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/30/5/632.full.
- Received for publication April 7, 2017.
- Revision received June 14, 2017.
- Accepted for publication June 17, 2017.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Patients Difficulties with Five Different Fecal Immunochemical Tests
- Patients experience of using colonoscopy as a diagnostic test after a positive FOBT/FIT: a systematic review of the quantitative literature
- Clinic Factors Associated With Mailed Fecal Immunochemical Test (FIT) Completion: The Difference-Making Role of Support Staff
- Faecal immunochemical testing implementation to increase colorectal cancer screening in primary care
- Improving the Health of Patients and Communities: Evolving Practice-based Research (PBR) and Collaborations