
Abstract
Background: Bordetella pertussis (BP) is a common cause of prolonged cough. Our objective was to perform an updated systematic review of the clinical diagnosis of BP without restriction by patient age.
Methods: We identified prospective cohort studies of patients with cough or suspected pertussis and assessed study quality using QUADAS-2. We performed bivariate meta-analysis to calculate summary estimates of accuracy and created summary receiver operating characteristic curves to explore heterogeneity by vaccination status and age.
Results: Of 381 studies initially identified, 22 met our inclusion criteria, of which 14 had a low risk of bias. The overall clinical impression was the most accurate predictor of BP (positive likelihood ratio [LR+], 3.3; negative likelihood ratio [LR−], 0.63). The presence of whooping cough (LR+, 2.1) and posttussive vomiting (LR+, 1.7) somewhat increased the likelihood of BP, whereas the absence of paroxysmal cough (LR−, 0.58) and the absence of sputum (LR−, 0.63) decreased it. Whooping cough and posttussive vomiting have lower sensitivity in adults. Clinical criteria defined by the Centers for Disease Control and Prevention were sensitive (0.90) but nonspecific. Typical signs and symptoms of BP may be more sensitive but less specific in vaccinated patients.
Conclusions: The clinician's overall impression was the most accurate way to determine the likelihood of BP infection when a patient initially presented. Clinical decision rules that combine signs, symptoms, and point-of-care tests have not yet been developed or validated.
Pertussis is an acute respiratory illness caused by the Bordetella pertussis (BP) bacterium. Initial symptoms are usually relatively mild, and can include cough, sneezing, coryza, and slight fever. The disease then progresses to produce more severe, paroxysmal coughing fits. During these episodes, the characteristic “whooping” may be heard as the patient tries to inhale through narrowed upper airways and the larynx. Posttussive vomiting, cyanosis, and apnea can occur as a result of the severity of these episodes.1 A recent systematic review of the prevalence of BP infection in patients with prolonged cough found that the overall prevalence of BP infection among primary care patients with prolonged cough (typically >1 week) was 12.4%; it was 18% in studies of children—much higher than suggested by laboratory-based surveillance reports.2 The recent large increase in pertussis cases in the United States has been described by the Centers for Disease Control and Prevention (CDC) as an epidemic.3
For infants and young children, complications from pertussis may be life-threatening, and hospitalization may be warranted. Vaccination against BP is effective at preventing the spread of infection and is recommended for infants, children, and adults.4,5 Though older children and adults are unlikely to experience severe complications from pertussis, they can act as vectors of infection when in contact with those who are more vulnerable, including unvaccinated or incompletely vaccinated infants and children.6,7
CDC guidelines recommend a macrolide antibiotic (azithromycin, clarithromycin, or erythromycin), or, as an alternative, trimethoprim-sulfamethoxazole, for patients diagnosed with pertussis. Ideally, treatment should begin within 1 to 2 weeks of the onset of symptoms.8 However, recognition of patients with pertussis is challenging, as many of their symptoms overlap with those of viral acute respiratory tract infections, and the recommended diagnostic test (polymerase chain reaction [PCR]) typically takes several days. Thus, signs and symptoms may be able to help identify patients at high risk for pertussis, for whom testing should be prioritized. We identified only a single previous systematic review of clinical diagnosis, which excluded studies of young children and studies using culture as a reference standard.1 A number of potentially relevant studies have also been published since its search was completed in 2010. The purpose of this meta-analysis is to perform a comprehensive systematic review and meta-analysis of the accuracy of signs and symptoms for the diagnosis of pertussis in patients of all ages.
Methods
Literature Search
We systematically reviewed studies published in MEDLINE using the following search strategy:
“pertussis”[tiab] OR “whooping cough”[tiab]) AND (“medical history taking”[MeSH Terms] OR “physical examination”[MeSH Terms] OR “signs and symptoms” OR “symptoms and signs” OR “symptom”[Title/Abstract] OR “history and physical” OR “physical examination” OR “physical examination” OR “clinical diagnosis” OR “clinical examination” OR “post-tussive” OR “posttussive” OR “vomiting” OR “c-reactive protein” OR “CRP” OR “sedimentation rate” OR “sed rate” or “WESR” or “procalcitonin” OR “white blood cell count” OR “complete blood count” OR “WBC” OR “CBC”
We did not restrict the search by language or date of publication. In addition, we searched the reference lists of included studies for additional studies not initially identified in our MEDLINE search.
Inclusion and Exclusion Criteria
We included prospective cohort studies of patients presenting with acute cough, prolonged cough, or clinically suspected pertussis if all patients received a reference standard test consisting of PCR, culture, or serology, and if studies provided adequate data to calculate either the sensitivity or specificity of the examined symptoms. We excluded studies if they used a case-control design (which overestimates treatment accuracy)9; if sign and symptom data were collected retrospectively or after the initial patient contact; if the study was performed in a specialized population (eg, immunocompromised patients); if data were gathered only after a positive test had been obtained; or if the study had fewer than 25 patients.10,11 Since outbreak investigations typically gather symptom data retrospectively, and often by telephone, they were not included. Our goal was to identify high-quality studies that gathered clinical data at the time the patient presented, masked to the results of the reference standard test. No age restriction or restriction by immunization status was used.
Data Abstraction
Each abstract was reviewed by 2 investigators (MC and CM) for possible inclusion, and the full text of any study that potentially fit the inclusion criteria was reviewed in detail. Two investigators (MC and CM), working in parallel, abstracted data on study characteristics, study quality, and the accuracy of signs and symptoms. Any discrepancies were resolved by consensus after discussion, involving the third investigator (ME) if necessary.
Quality Assessment
The studies were evaluated for potential bias using the QUADAS-2 framework, which assesses patient selection, index test, reference standard used, and patient flow.12 The reference standard was considered to be at low risk of bias if PCR, culture, paired serology, or some combination of those was used to evaluate all patients in the study, whereas single serology was considered to have a high risk of bias. Assessments were conducted in parallel, such that each study was examined by at least 2 of the investigators, and disagreements were resolved by consensus after discussion.
Statistical Analysis
We performed bivariate meta-analysis using the mada and metafor procedures in R, version 3.2.2. We calculated summary estimates and 95% confidence intervals for sensitivity, specificity, positive likelihood ratios (LR+), negative likelihood ratios (LR−), and diagnostic odds ratios (DORs) using the Reitsma method from the mada procedure. This method can only calculate summary estimates when both sensitivity and specificity are available. Some of the included studies did not report specificity. In these situations, the summary estimates of sensitivity were calculated using a random effects model of raw proportions using the metafor procedure. The raw proportion was the sensitivity for each symptom, calculated by the number of true positives divided by true positive plus false negative (TP/[TP + FN]). Two variables (headache and wheezing) had positive likelihood ratios <1.0, so we report the accuracy of the absence of these signs or symptoms. We used summary receiver operating characteristic (ROC) curves to explore heterogeneity and plot 95% confidence intervals for the summary estimates of accuracy.
Results
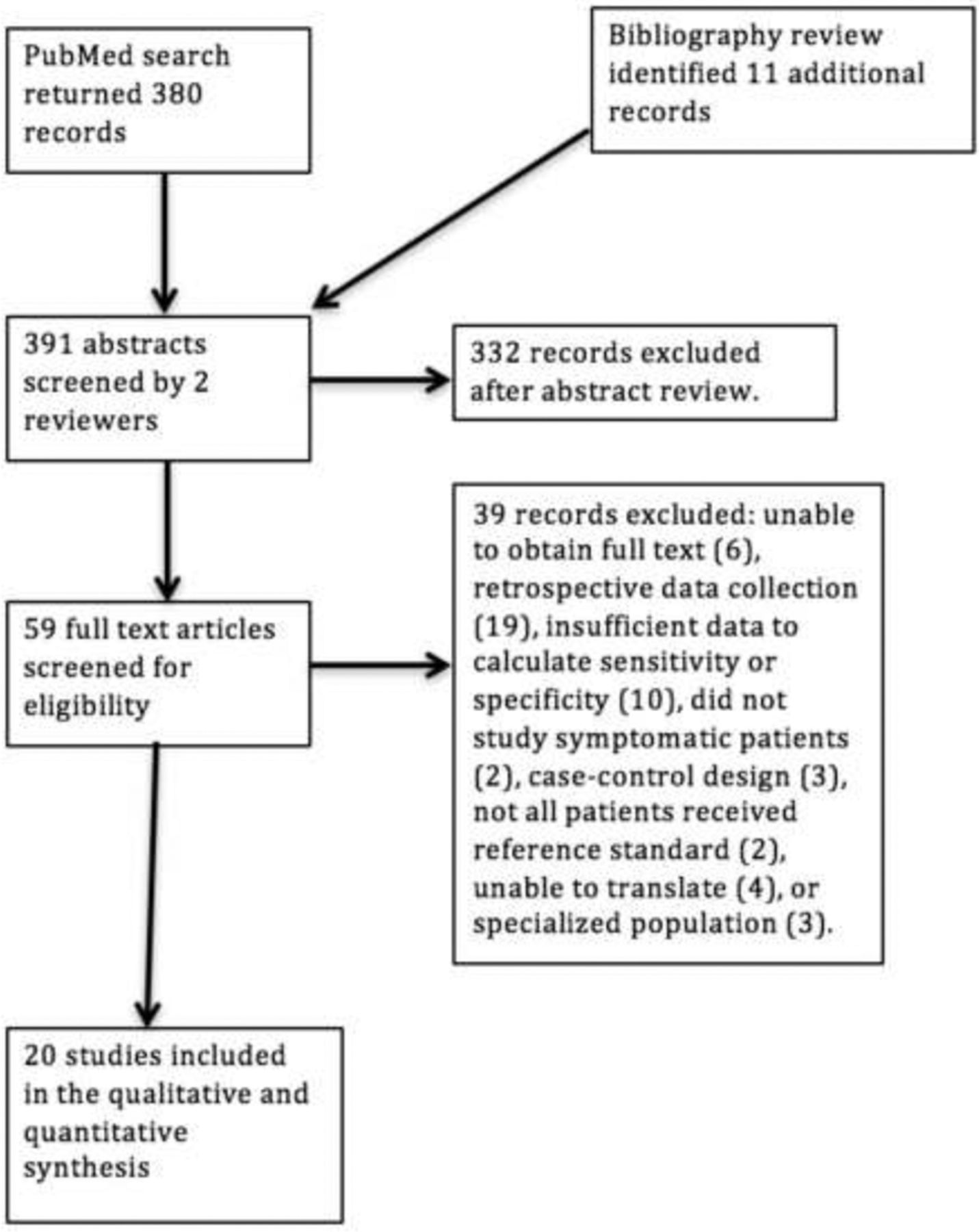
The results of the search process are summarized in the Preferred Reporting Items for Systematic Reviews and Meta-analyses diagram (Figure 1). The initial MEDLINE search identified 381 studies, of which 17 were included; a review of the reference lists of included studies identified 5 more. Overall, 22 studies with a total of 15,909 patients met the inclusion and exclusion criteria. Their characteristics are summarized in Table 1. Twelve were set in Europe, 2 in Korea, and the remainder each in 1 of 8 countries in Australasia, Africa, or the Americas. Study size ranged from 32 to 3,629 patients. Nineteen studies used PCR, culture, or paired serology as the reference standard; only 3 studies used a single serology as the reference standard. Four studied adults only, 8 studied children only, and 10 studied both adults and children.

Preferred Reporting Items for Systematic Reviews and Meta-analyses flow diagram. Only the first identified reason for excluding an article is listed. In some cases >1 reason was identified.
Characteristics of Included Studies
Quality Assessment
The quality assessment is summarized in Table 2, using the QUADAS-2 framework. Overall, we judged 14 studies to be at low risk of bias, 4 at moderate risk of bias, and 4 at high risk of bias.
Assessment of Study Quality Using the QUADAS-2 Framework
Accuracy of Signs and Symptoms
The accuracy of individual signs and symptoms (reported by at least 3 studies) is summarized in Table 3 (full results by individual study are available in the online Appendix). The overall clinical assessment by the physician was the most helpful single piece of information at ruling in pertussis when positive, with an LR+ of 3.3, an LR− of 0.63, and a DOR of 5.3. While the overall impression of a physician was quite specific (0.85), it lacked sensitivity (0.47) and would therefore fail to identify more than half of patients with pertussis.
Summary Estimates of the Diagnostic Accuracy of Signs and Symptoms for Bordetella pertussis Infection*
The following individual signs and symptoms were significantly associated with pertussis (LR+ and LR− both were significantly different from 1.0): whooping cough (overall and in children only), posttussive vomiting, paroxysmal cough, sputum, sleep disturbed by cough, and absence of headache. However, the likelihood ratios were all between 2.1 and 0.58, indicating little diagnostic value.
While paroxysmal cough was the most sensitive single finding, it lacked specificity (0.35) because it occurs in many other respiratory infections. The 3 signs or symptoms that were best at ruling out pertussis when absent or negative were the overall clinical assessment by a physician (LR−, 0.57), the absence of paroxysmal cough (LR−, 0.58), and the absence of sputum production (LR−, 0.63). Still, these LR− values are quite close to 1.0 and are therefore only minimally helpful.
Because prolonged cough was often part of the inclusion criteria, it was not reported by most studies as a clinical variable. When it was reported, studies generally indicated the overall duration of cough for the episode of illness, rather than the duration of cough at the time the patient initially presented to a clinician. Two studies did report the likelihood of pertussis for patients with cough for >2 weeks at presentation, compared with a shorter duration. One was a large, contemporary European multicenter study that enrolled 3074 patients, of whom 93 had pertussis by PCR. Pertussis was more likely among patients with cough for >2 weeks, but the sensitivity was only 27% and specificity 82% (LR+, 1.5; LR−, 0.89).13 An older study also reported data for this variable, but similarly did not find it to be a helpful predictor of pertussis (LR+, 1.1; LR−, 0.98).30
We were able to evaluate separately for adults and children the accuracy for 3 key symptoms: whooping cough, posttussive vomiting, and paroxysmal cough. Both whooping cough (41% vs 20%) and posttussive vomiting (56% vs 34%) were more sensitive in children, although the specificity was similar. The LR+ for whooping cough was 4.1 in children and only 1.4 in adults.
No studies of a clinical decision rule (CDR) combining data for several signs and symptoms met our inclusion criteria. One study used the combination of symptoms and the local prevalence of pertussis for the week in which a sample was drawn to predict the likelihood of infection. However, it gathered data retrospectively and has not been prospectively or externally validated.35 The CDC has defined the clinical case for pertussis as cough for ≥14 days plus at least 1 other typical symptom (paroxysms of cough, inspiratory whoop, or posttussive vomiting). Three studies reported the accuracy of the CDC criteria, with summary estimates of accuracy at 90% sensitivity, only 16% specificity, LR+ of 1.1, and LR− of 0.66.19,25,27
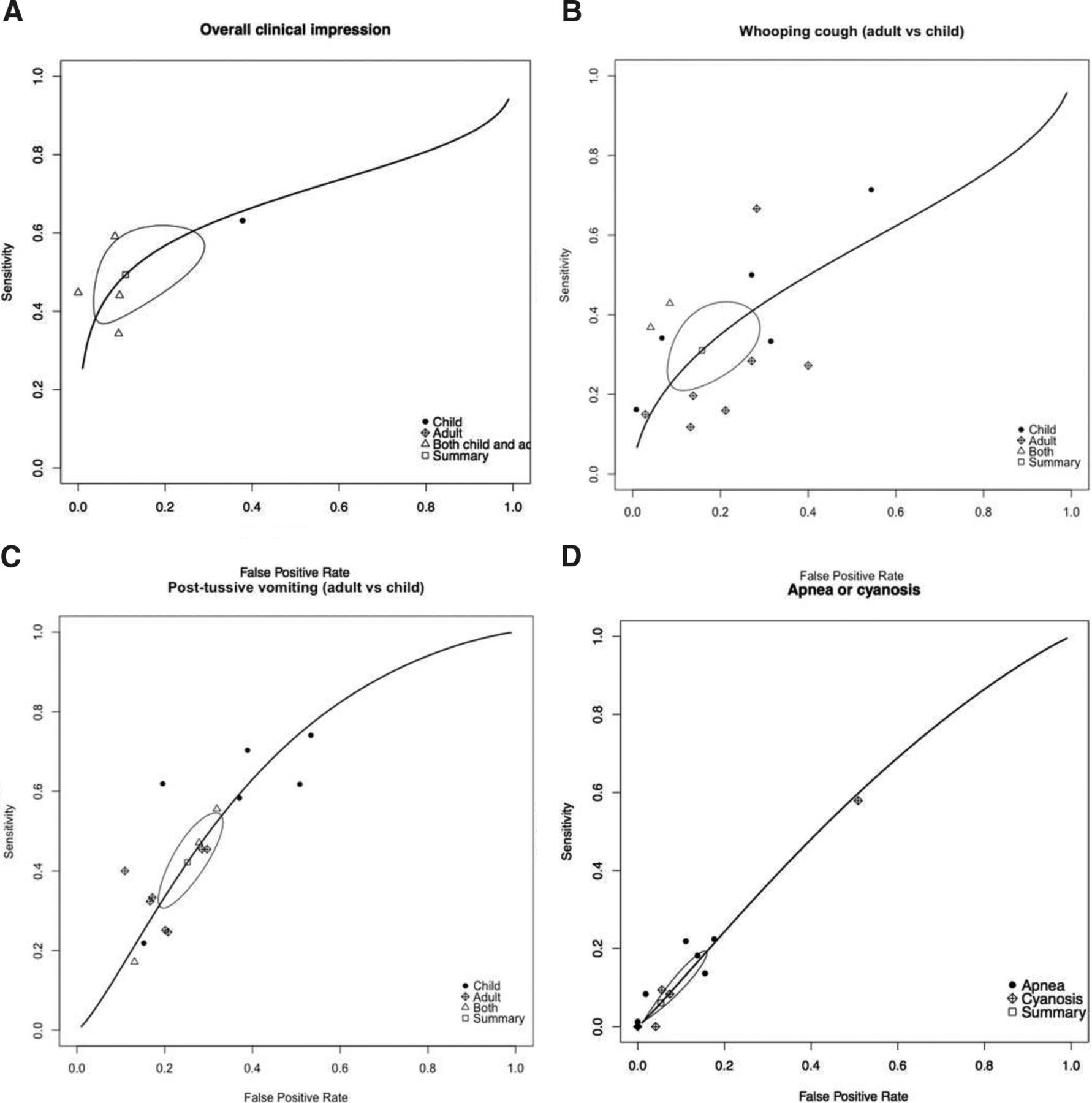
Summary ROC Curves
Summary ROC curves for key signs and symptoms are shown in Figure 2A through D, stratified by age, where possible. The ROC curve for the overall clinical impression (Figure 2A) shows good consistency and a fairly narrow confidence interval around the summary estimate of accuracy. As noted earlier, whooping cough (Figure 2B) and posttussive vomiting (Figure 2C) were both more sensitive in children than in adults. Apnea and cyanosis (Figure 2D) are plotted together because they had very similar sensitivity and specificity values. Of 4 studies reporting data for cyanosis, 3 found that it was highly specific (>0.95) but lacked sensitivity.
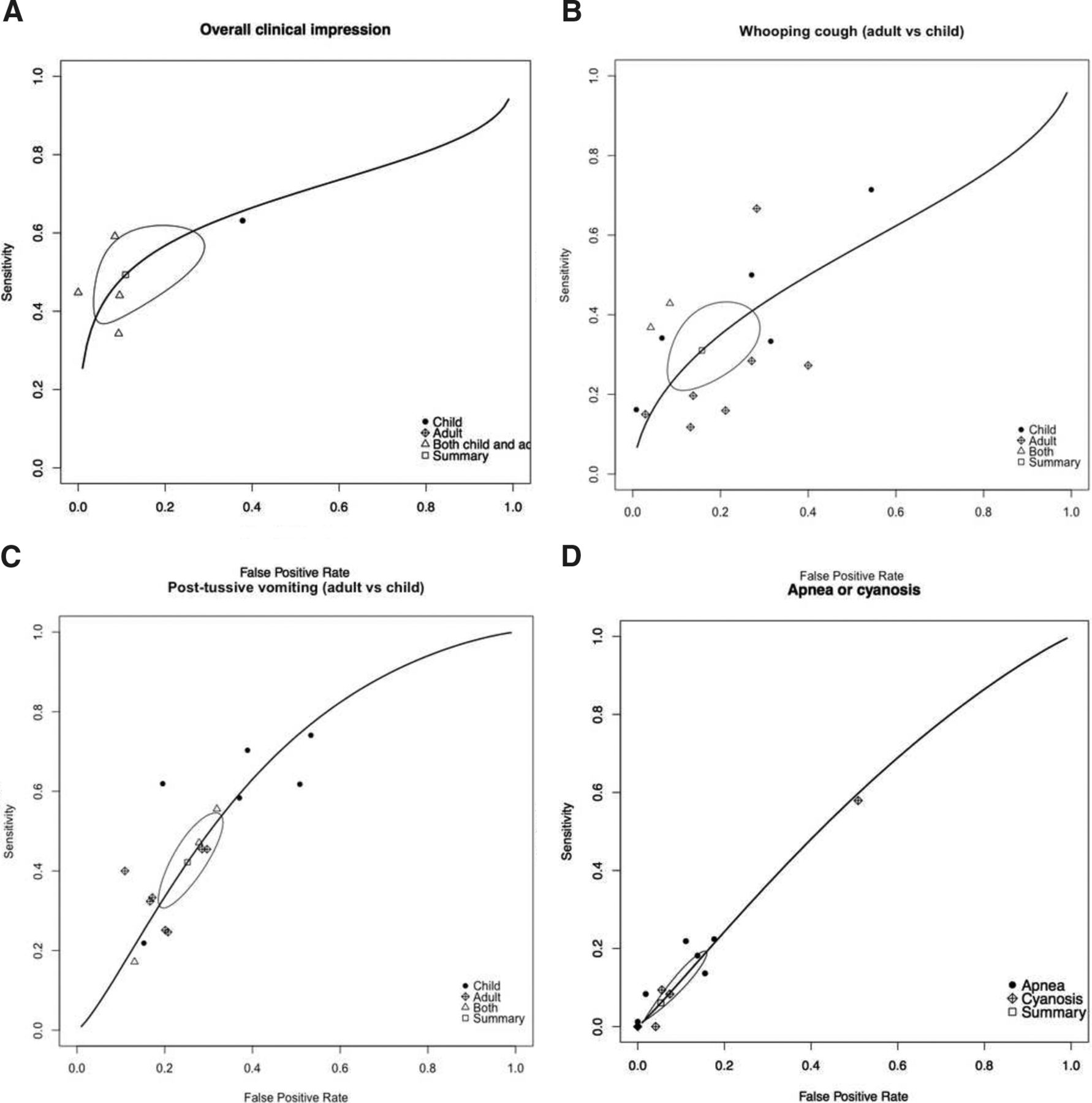
Summary receiver operating characteristic curves for overall impression (A), whooping cough (B), posttussive vomiting (C), and apnea or cyanosis (D), stratified by age.
Vaccination Status
Summary ROC curves comparing populations that have high rates of vaccination with those that have low rates are shown in Figure 3A through D. Given the small number of studies in these comparisons, the ability to draw inferences is limited, and the data should be interpreted cautiously. The observed pattern based on these limited data is that in a vaccinated population, typical signs and symptoms of pertussis are more sensitive but less specific than those in an unvaccinated population.
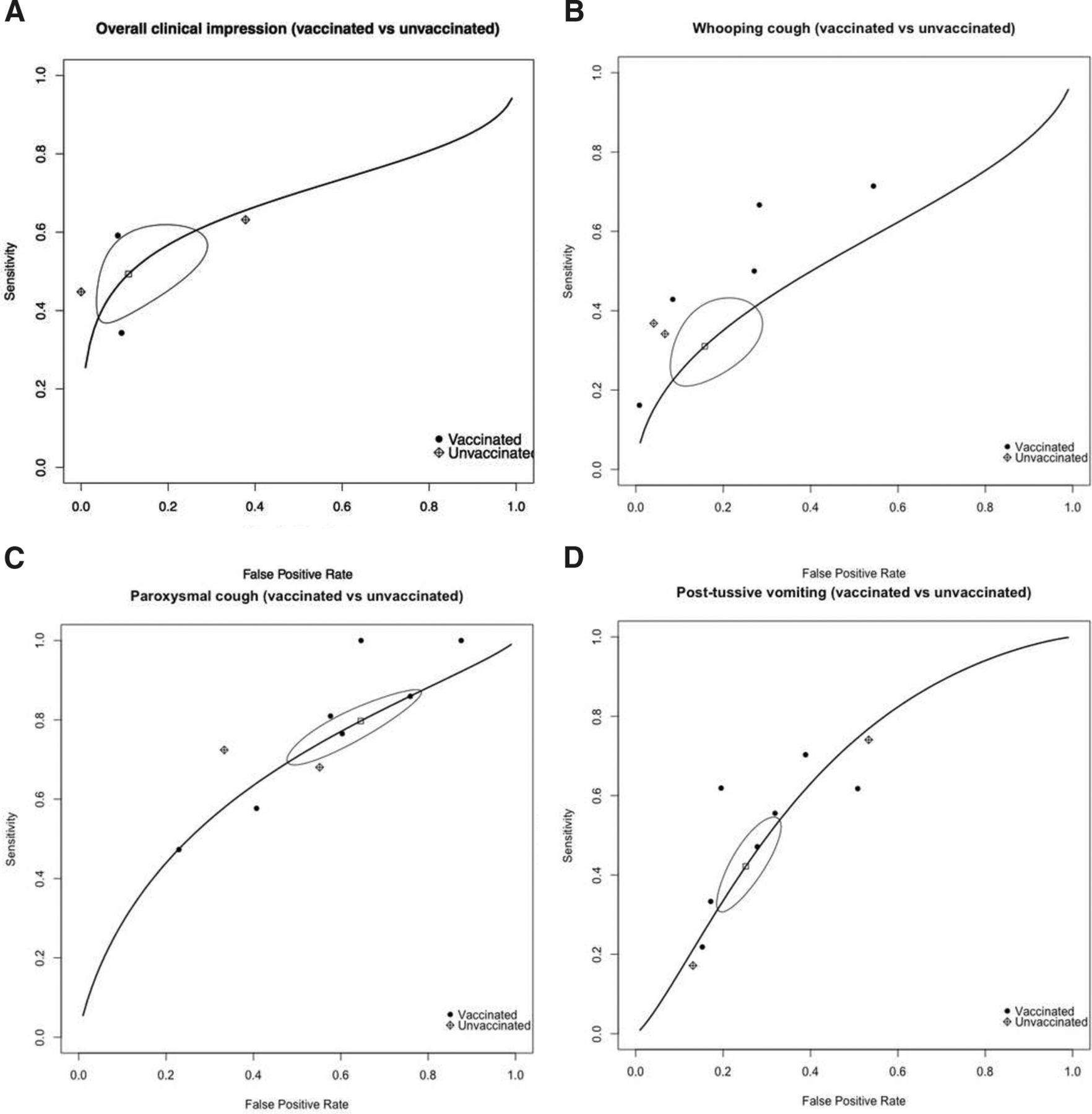
Summary receiver operating characteristic curves for overall impression (A), whooping cough (B), paroxysmal cough (C), and posttussive vomiting (D), stratified by vaccination status.
Discussion
We have reviewed the best available evidence regarding the clinical diagnosis of BP infection in adults and children. The overall quality of the included studies, aided by the strict inclusion criteria of our systematic review, was good, with over half at low risk of bias. Unfortunately, we must conclude that individual signs and symptoms are of limited value, with none having an LR+ >2.1 or an LR− <0.5. The exception is the overall clinical impression, which had an LR+ of 3.3 and an LR− of 0.63. While the overall clinical impression has excellent specificity, it lacks sensitivity and would fail to identify half of the patients with pertussis. However, it clearly suggests that when a clinician has a strong clinical suspicion for pertussis, he or she should trust that suspicion and order confirmatory testing. Of course, the positive predictive value depends on the prevalence of pertussis. For example, it is 15% when the prevalence is 5%, 27% when the prevalence is 10%, and 45% when the prevalence is 20%.
Our overall summary estimates of accuracy were similar to those of a previous systematic review.1 However, we identified a number of additional studies, including 7 published since that review, and were able to stratify our results by adult versus child and vaccinated versus unvaccinated populations. Two symptoms, whooping cough and posttussive vomiting, were more sensitive in children than in adults. This may be because of physiologic differences in airway size in children versus in adults; aerophagia, which is more common in children than in adults; and possibly a lower threshold for vomiting in children than in adults. Whooping and posttussive vomiting are therefore less diagnostically useful in adults, and the absence of these symptoms does not rule out pertussis in this group.
Based on a review of the ROC curves, it seems that typical signs and symptoms of pertussis are more sensitive but less specific in a vaccinated population than in an unvaccinated population. More sensitive signs and symptoms may have their greatest value in ruling out pertussis when negative. However, the small number of studies makes it difficult to draw conclusions, highlighting the need for studies of clinical diagnoses among contemporary vaccinated populations. These possible differences in the presentation between vaccinated and unvaccinated populations makes it important that we perform contemporary, well-designed, and adequately powered studies of signs, symptoms, and CDRs, as older data may no longer apply to the many parts of the world where >95% of the population is vaccinated.
Our systematic review had several limitations. Data regarding the duration of a symptom or combination of symptoms and their association with the diagnosis were limited. The area under the summary ROC curves calculated by the mada procedure were somewhat unreliable because of sparse data and clustering of data in 1 part of many of the curves. The small number of studies for comparing vaccinated with unvaccinated populations limited out ability to draw conclusions, and some studies were quite old. Finally, considerable heterogeneity exists for common symptoms of pertussis, such as whooping cough and paroxysmal cough. This could be a result of differences in how the question was asked or differences in the population (adult vs child, vaccinated vs unvaccinated).
An important gap in the literature is the lack of validated CDRs. CDRs have been useful in other acute respiratory infections such as pharyngitis36 and pneumonia.37 They typically classify patients as low, moderate, and high risk; these categories correspond to patients in whom disease is ruled out, further testing is needed, or disease is ruled in.38,39 We identified only 1 CDR for pertussis; it is for infants and incorporates surveillance data but has not been prospectively validated.35 The CDC's definition of a clinical case could be considered a kind of CDR; however, it is sensitive but very nonspecific (16%). This reflects the fact that it is a clinical case definition intended for use in outbreaks, with the knowledge that more specific confirmatory testing with culture or PCR would be available.
CDRs for other conditions have sometimes incorporated point-of-care tests such as C-reactive protein or procalcitonin40,41; this is a promising area for further research in the diagnosis of pertussis. Another, as demonstrated by Fine and colleagues,35,42 is the incorporation of surveillance data or novel approaches like using Google searches to predict the prevalence of pertussis.
Appendix
Individual patient data. Continuity correction applied to avoid division by zero where necessary
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/30/3/308.full.
- Received for publication October 20, 2016.
- Revision received January 13, 2017.
- Accepted for publication January 13, 2017.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Immune boosting and the perils of interpreting pertussis seroprevalence studies
- Multicenter Clinical Evaluation of the Automated Aries Bordetella Assay
- Could this be whooping cough?
- Content Usage and the Most Frequently Read Articles of 2017
- Pertussis manifesting as recurrent cough and wheezing in an incompletely vaccinated 8-month-old infant
- Re: Clinical Diagnosis of Bordetella Pertussis Infection: A Systematic Review
- Response: Re: Clinical Diagnosis of Bordetella Pertussis Infection: A Systematic Review
- Research on Clinical Decisions Made Daily in Family Medicine