
Abstract
Background: The role of primary care providers (PCPs) in decision making around cancer care remains largely unknown. We evaluated how frequently men with localized prostate cancer report receiving help from their PCP about their treatment, and whether those men who do are less likely to receive definitive treatment.
Methods: We mailed surveys to men newly diagnosed with localized prostate cancer between 2012 and 2014 in the greater Philadelphia region. Participants were asked whether their PCP helped decide how to treat their cancer. The outcome was receipt of definitive treatment (either radical prostatectomy or radiotherapy).
Results: A total of 2386 men responded (adjusted response rate, 51.1%). Among these men, 38.2% reported receiving help from their PCP regarding choosing a treatment, and 79.6% received definitive treatment. In adjusted analyses, non-Hispanic black men (odds ratio, 1.76; 95% confidence interval, 1.37–2.27) were more likely than non-Hispanic white men to report receiving help from their PCP. However, men who did receive help were not more likely to forgo definitive treatment overall (P = .58) or in the subgroups of men who may be least likely to benefit from definitive treatment.
Conclusions: Though a substantial proportion of men reported receiving help from their PCP about prostate cancer treatment, these discussions were not associated with different treatment patterns. Further effort is needed to determine how to optimize the role of PCPs in supporting patients to make preference-sensitive cancer decisions.
In 2013, the Institute of Medicine called for collaboration between cancer specialists and primary care providers (PCPs) to improve delivery of comprehensive, high-quality cancer care.1 This was motivated, in part, by recognizing the growing number of cancer patients with complex medical needs. The role of PCPs in cancer care has typically been limited to screening, diagnosis, and, more recently, survivorship.2,3
Studies evaluating PCP involvement in cancer treatment decision making remain limited.4,5 Wallner and colleagues5 recently found that 35% of women with breast cancer reported a high level of PCP participation in their treatment decision, but this was not with linked with more meaningful deliberation for their treatment decision. Jang and colleagues4 used cancer registry and Medicare claims data to evaluate how PCP visits relate to treatment choice, finding that 22% of men visited their PCP before their prostate cancer treatment and were more likely to receive conservative management. However, that study used any visit with a PCP before treatment, as identified in insurance claims, as a proxy for treatment discussions and did not evaluate the effect among subgroups of men eligible for active surveillance.
Building on the prior literature and drawing on a large survey of men diagnosed with localized prostate cancer, we sought to better understand how frequently men reported receiving help from their PCP in deciding on prostate cancer treatment and whether reporting help was linked with different patterns of treatment. Men with clinically localized prostate cancer represent an important clinical group in which to evaluate the potential role of PCPs in treatment decisions. Prostate cancer is diagnosed in 180,890 men in the United States annually,6 and men with localized disease face a choice among treatment options—including radical prostatectomy, radiation therapy, and active surveillance—with varying side effects and benefits. Ideally, patients' preferences, in conjunction with clinical features, should guide the treatment that they receive.7,8 In practice, however, treatment often depends on the type of specialist that a patient sees. Hoffman and colleagues9 found that the urologist who diagnosed a patient's prostate cancer accounted for twice as much of the variation in his ultimate treatment when compared with patient-level characteristics. When cancer specialists are surveyed regarding their management of prostate cancer, specialists tend to recommend the treatment that they themselves deliver: the majority of urologists recommend radical prostatectomy for clinically localized cancer, whereas the majority of radiation oncologists recommend radiation therapy.10⇓–12
PCPs may be in an ideal position to help men with prostate cancer make treatment decisions. First, compared with specialists, PCPs are more likely to have longitudinal relationships with their patients and often act as trusted sources of information and provide emotional support for their patients.13⇓–15 In this role, they may be better suited to elicit patient preferences and consider patient comorbidities in clinical decision making.16⇓⇓–19 Second, unlike specialists who are apt to recommend the treatment they themselves deliver, PCPs may be more likely to deliver balanced treatment recommendations and thereby help patients make treatment decisions consistent with individual values.2,20 A PCP's role may be particularly important for patients who qualify for active surveillance programs based on their age, comorbidities, functional status, and stage of their prostate cancer.
In this study, we hypothesized that men with localized prostate cancer who received help from their PCP to choose a treatment would be less likely to receive definitive treatment with either radical prostatectomy or radiation therapy,4 and we anticipated that the effect would be larger among men who may benefit most from active surveillance, particularly men who are of advanced age, who have a shorter life expectancy, and who have lower-risk tumors.21 In addition, with well-documented racial differences in physician-patient communication and patients' engagement in their own health care,22,23 we hypothesized that black men would be less likely to report receiving help from their PCP before treatment, and that these conversations may be less strongly associated with the type of treatment they receive.
Methods
Patient Cohort
The Philadelphia Area Prostate Cancer Access Study (P2 Access) is a study of black and white men diagnosed with localized prostate cancer within the greater Philadelphia area. This study uses multiple data sources, including a state cancer registry, patient surveys, and provider inventories, to understand how access to care influences racial differences in prostate cancer treatment. This article is a secondary analysis of data from the patient survey. Men diagnosed with prostate cancer between January 1, 2012, and December 31, 2014, were identified from the Pennsylvania Cancer Registry (PCR) using the following inclusion criteria: (1) new diagnosis of prostate cancer; (2) adenocarcinoma histology; and (3) resident of 8 specified counties within the greater Philadelphia area (Berks, Bucks, Chester, Delaware, Lancaster, Lehigh, Montgomery, and Philadelphia). Men were excluded if they (1) died before data could be collected, (2) were unable to speak English or Spanish, and (3) had metastatic disease at the time of presentation. We also excluded men if they had military insurance (including Tricare and Veterans Administration) and received chemotherapy for treatment. This article focuses specifically on the subset of men who reported having a PCP at the time of their cancer diagnosis (95% of the total respondents).
Patient Questionnaire
Men who were newly diagnosed with prostate cancer were invited to participate in a survey between February 2014 and September 2015, reflecting the lag time from diagnosis to identifying patients and obtaining data from the PCR. Participants received up to 2 mailings of the survey, followed by phone calls to all nonresponders. An unconditional $2 incentive was included in the initial mailing, and $15 was provided upon completion of the survey. Survey items were based on prior studies4,24⇓⇓–27 and were pilot tested among a similar cohort of men with newly diagnosed localized prostate cancer.
PCP Help with Treatment Decision Making
To assess the role of PCPs in prostate cancer treatment decision making, men were asked in the survey, “After you found out you had prostate cancer, did your primary care provider help you decide how to treat it?” Responses were yes or no.
Treatment
Data from the PCR was used to define receipt of definitive treatment. Definitive treatment was classified as having either radical prostatectomy or radiotherapy (including external beam radiation therapy or seed brachytherapy).
Covariates
Patient sociodemographic characteristics that have previously been found to influence prostate cancer treatment were obtained from the survey and the cancer registry. From the survey, patients reported their education (less than eighth grade, some high school, high school graduate, some college, college graduate, and beyond college education), race/ethnicity (non-Hispanic white, non-Hispanic black, Hispanic, and non-Hispanic other), and marital status (married or single/other).10,28 We obtained insurance at the time of diagnosis from the PCR, classified as private, Medicaid, Medicare (with and without a supplement), and none.
A validated mortality index was used to calculate the life expectancy for each respondent based on survey data.25 The index included age, body mass index, tobacco use, self-reported comorbidities, and functional status. Participants were grouped into those with low (<25%), intermediate (25–50%), high (50–75%), and very high (≥75%) risks of 10-year mortality.29
Tumor-specific data were abstracted from the cancer registry. For our primary analysis, we evaluated a Gleason score from biopsy (<7, 7, >7), and the clinical tumor stage (stage 1, 2, or 3 based on the American Joint Committee on Cancer TNM system).30 We performed a sensitivity analysis calculating risk based on National Comprehensive Cancer Network classification (NCCN) (low, intermediate, and high risk), which further included prostate-specific antigen results obtained from the PCR. Gleason score, clinical tumor stage, and NCCN risk stratification have all been previously shown to be prognostic predictors of prostate cancer outcomes.21,31
Statistical Analysis
Descriptive analysis was used to provide summaries of patient sociodemographic and tumor characteristics. The χ2 test was used to compare characteristics of men who did and did not receive help from their PCP to decide on prostate cancer treatment following diagnosis. We constructed a multivariable logistic regression model to assess whether receiving help from the PCP regarding treatment was associated with patient sociodemographic (age, race/ethnicity, education, insurance, employment, and marital status) and clinical (life expectancy, Gleason score, and clinical tumor stage) characteristics. Next, we examined the association between receiving help from the PCP and receipt of definitive treatment. Propensity score matching was used to achieve balance on observable characteristics among those who did and did not receive help from their PCP. This was implemented using 1-to-1 nearest-neighbor matching and doubly robust methods in our multivariable regression model.32 Our initial model adjusted for the above-mentioned sociodemographic and clinical characteristics. We then assessed whether the relationship between receiving help from the PCP and treatment patterns varied by patient race by including an interaction term (race × PCP involvement). We performed 3 sets of subgroup analyses to examine the association between receiving help from the PCP and receipt of definitive treatment among men who would be considered suitable candidates for active surveillance under clinical guidelines: (1) age >70 years; (2) limited life expectancy (10-year risk of mortality >50%); and (3) NCCN-classified low-risk prostate cancer.21,33 Finally, among the subgroup of men who received definitive treatment, we examined whether receiving help from the PCP was associated with either type of treatment (surgery or radiation) using a multivariable logistic regression model, adjusting for sociodemographic and clinical characteristics. For covariates with missing data, we used multiple imputation via multiple chained equations based on all available patient characteristics. Five imputed data sets were used in this approach. Analyses were conducted using Stata 13.0 software (StataCorp, College Station, TX). This study was approved by the institutional review boards at the University of Pennsylvania and Johns Hopkins University.
Results
A total of 2386 of 4672 eligible men completed the survey (adjusted response rate, 51.1%). Compared with nonresponders, responders were white (77.5% vs 61.5%) and had higher rates of receiving definitive treatment (79.5% vs 70.9%) (Appendix Table 1). Among the 2294 men in our final analytic cohort, the average age was 65.4 years (standard deviation, 8.3 years; Table 1). Men predominantly were white (78.6%), were married (80.0%), had a higher-level education (62.4%), and had either private insurance (55.4%) or Medicare (40.1%). The majority of men had tumors with a Gleason score ≤7 and clinical tumor stage 1 disease.
Demographic and Clinical Characteristics of Patients
Over a third of men (38.2%) reported receiving help from their primary care provider in deciding how to treat their prostate cancer (Table 2). In bivariate analyses, black men were more likely to have reported receiving help compared with white men. PCP involvement was less likely among men who were employed or retired compared with those who were unemployed. In the adjusted analysis, black men (odds ratio, 1.76; 95% confidence interval, 1.37–2.27) had a significantly higher likelihood of receiving help from their PCP compared with white men (Table 2).
Bivariate and Multivariable Analyses of Patient Characteristics Associated with Receiving Help from the Primary Care Physician Regarding Treatment
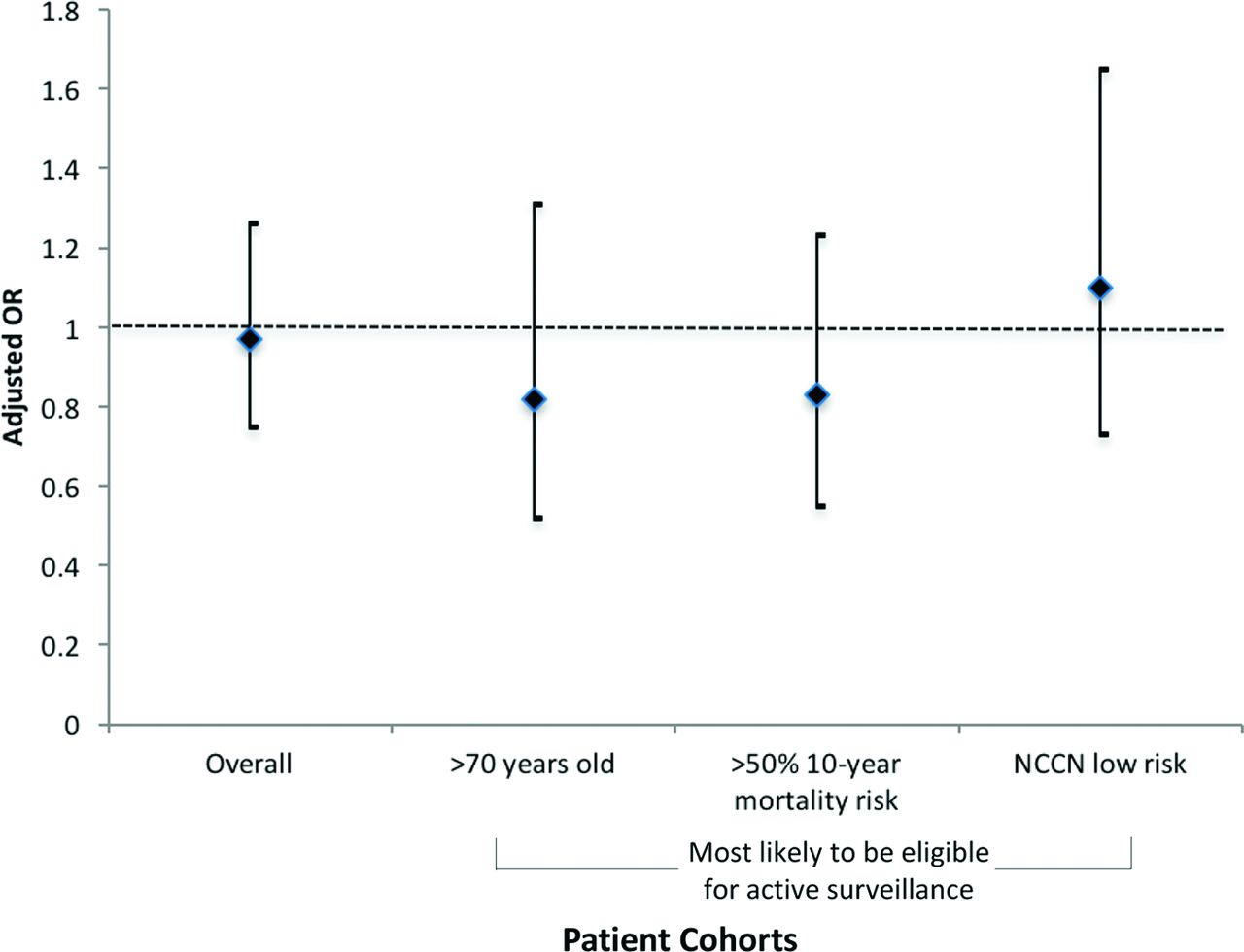
Overall, 1825 men (79.6%) received definitive treatment; 38.8% of men who received definitive treatment reported receiving help from their PCP, compared with 40.3% of men who did not receive treatment (P = .58). Using propensity score matching, we achieved appropriate balance on observable covariates. In our doubly robust models, men who received help from their PCP were as likely to undergo definitive treatment as men who did not report receiving help (odds ratio, 0.97, 95% confidence interval, 0.75–1.26). Race did not modify the effect of PCP involvement on definitive treatment (P = .79). In subgroup analyses of men more likely to be eligible for active surveillance—including men with NCCN-classified low-risk disease, with limited life expectancy (≥50% 10-year risk of mortality), and >70 years old—we did not find evidence that discussions with PCPs were associated with receipt of definitive treatment (Figure 1). Further, we did not find significant associations between PCP help and the specific type of treatment (surgery or radiation) among men who received definitive treatment.
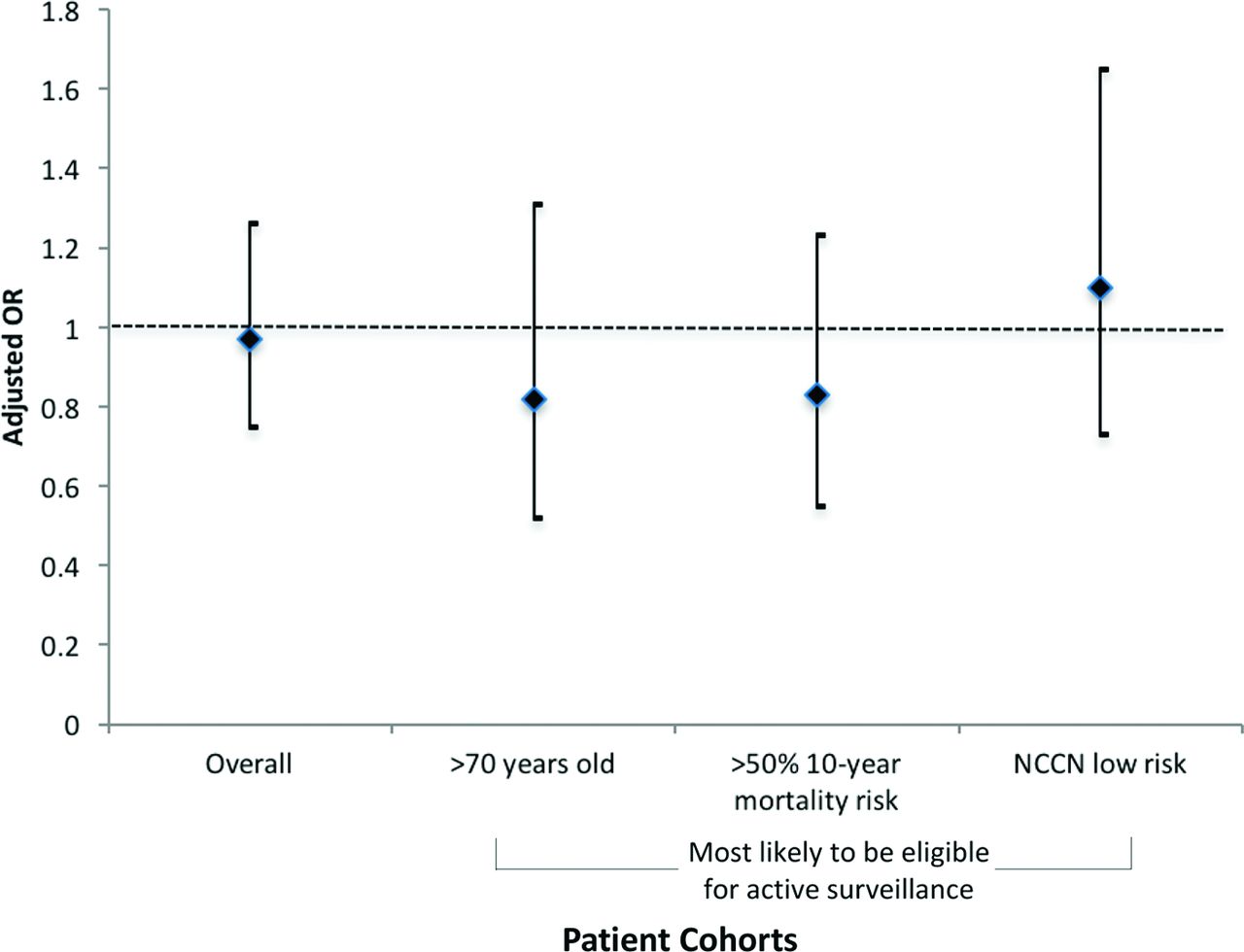
Adjusted odds ratio (OR) and 95% confidence interval of receipt of definitive treatment associated with receiving help from the primary care physician among various patient cohorts. All models adjusted for age, race, education, insurance, employment, marital status, and life expectancy, with models for older men and limited life expectancy additionally adjusted for Gleason score and clinical stage. NCCN = National comprehensive Cancer Network.
Discussion
In a large, population-based sample of men with localized prostate cancer, we found that over one third reported receiving help from their PCP in deciding how to treat their cancer. In particular, black men were more likely to report receiving help from their PCP compared with white men. Contrary to our original hypothesis, we did not find evidence that men who reported receiving help from their PCP were less likely to receive definitive therapy, either overall or in subgroups of men most likely to be considered for active surveillance based on clinical guidelines. Past studies show that PCP involvement is often limited during cancer treatment.15,34,35 Our results may suggest opportunities to increase the role of PCPs in treatment decision making among men with localized prostate cancer.
In our sample, a larger proportion of men (38%) reported receiving help than was found by Jang and colleagues4 (22%). Some of the difference may stem from differences in approaches to measuring PCP involvement. Jang et al used visit patterns from the Surveillance, Epidemiology and End Results/Medicare database and defined PCP involvement as a visit to a PCP between diagnosis and treatment. We rely on patient self-report of receiving help during office visits or through other modes such as telephone or electronic communication. Further, in contrast to the study by Jang et al, we limited our cohort to men who reported having a PCP at the time of their prostate cancer diagnosis. It is notable that, in our study, black men were more likely to report discussing treatment with their PCP, despite evidence suggesting that these men are less likely to be active participants in their health care and to be engaged with their providers.23,36 Our results may suggest that PCP involvement is greater for patients vulnerable to disparities in care. They may also point to potential differences between black and white patients in what they value for high-quality care; similar to findings from prior studies, minority patients may value their PCP's holistic approach to cancer care rather than disease-specific care.37,38 Future efforts to empower PCPs to be able to engage with patients in cancer treatment discussions is critical.
We did not find that receiving help from PCPs was associated with a lower likelihood of receiving definitive treatment. Our results were in contrast to those of Jang and colleagues,4 though in that study it is uncertain whether patients discussed their options for prostate cancer treatment during the PCP visit. It may be that visit patterns with PCPs around the time of diagnosis and treatment are related to other factors that might influence the decision of whether to pursue definitive treatment. Patients perceived their primary care to be of high quality in the study by Wallner et al,5 yet PCP engagement, communication, and participation were not associated with improvement in meaningful deliberation over treatment decisions. Within this context, lack of association with differences in treatment patterns as a result of PCP involvement may reflect the limited influence of PCPs during treatment decision making, a period in which cancer specialists' recommendations carry the most weight with patients. In our study, we also did not find PCP involvement in decision making to be associated with different treatment patterns among men who may be least likely to benefit from definitive treatment, including older men, men with limited life expectancy, and men with low-risk disease. Many of these men receive definitive treatment and are often unaware of the risk-benefit controversies associated with treatments.39⇓–41 PCPs may be particularly well suited to capitalize on their longitudinal relationship with patients within these subgroups of men, using their knowledge of the patient's comorbidities and functional status to help ensure that the patient is making decisions in line with their values and preferences.
With a large portion of patients reporting receiving help but no evidence from our data that, at a population-level, this affected treatment patterns, further work is needed to determine whether and how PCPs' roles might be extended to have a greater influence in the treatment decision-making process. In a survey of PCPs and cancer specialists, Klabunde and colleagues34 found that many PCPs saw themselves as playing a role in providing general medical care, but far fewer reported a role in determining initial cancer treatment. PCPs also report feeling disconnected from their patient's care and endorse having insufficient knowledge about treatment plans.14,42,43 This may limit a PCP's ability to effectively help his or her patients navigate complex cancer treatment decisions. New models of care that integrate interdisciplinary cancer care teams, promote communication between PCPs and cancer specialists, and improve provider competencies around cancer treatment may empower PCPs to engage in more meaningful discussions with their patients about key treatment decisions.
This study has several limitations. First, while men reported obtaining help from their PCP in choosing a treatment, we are unable to determine the ways in which PCPs helped. It is possible that some PCPs engaged in discussing the risks and benefits of different treatment options and assessing patient preferences, others may have provided emotional support, and still others may have had more limited conversations. Delving deeper into the type of help provided—both from a patient and a PCP perspective—and analyzing the content of conversations around these issues is an important next step. Second, we do not have information on the duration of the PCP-patient relationship, which may affect the quality of the discussions and the influence of the PCP on treatment decisions. We might expect that longer relationships are associated with greater provider trust and more influence on decision making. Third, nonresponse bias may have affected our findings, as responders were more likely to be white men and received definitive treatment. With conflicting prior evidence,4,5 the direction in which this would bias our findings on the association between PCP involvement and definitive treatment remains unclear. Fourth, patient self-report of discussions with their PCP could be susceptible to recall and social desirability biases; however, they are similar to those reported in prior studies.5,20 Fifth, data were obtained from a single geographic area, which may limit the generalizability of the study. However, the study area includes 5.3 million residents across urban and suburban locales. It is racially and ethnically diverse, and 29% of the area's population is nonwhite.
Conclusions
Receiving help from a PCP was not associated with differences in treatment patterns in our study population of men with clinically localized prostate cancer, either overall or in cohorts who may be least likely to benefit from definitive treatment. Our study may point to opportunities to leverage the help that PCPs are providing to their patients in order to promote preference-sensitive care, and also the need to explore new models of collaborative decision making between cancer specialists, PCPs, and patients.
Appendix
Demographic and Clinical Characteristics of Responders and Non-Responders
Notes
This article was externally peer reviewed.
Funding: This work was supported by the National Institute on Minority Health and Health Disparities (P60 MD006900). AR's salary is supported by the National Heart, Lung, and Blood Institute (T32H1007180). CEP's salary is supported by the National Cancer Institute (K07CA151910). JB's salary is supported by the National Cancer Institute (K07CA163616).
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/30/3/298.full.
- Received for publication November 11, 2016.
- Revision received January 30, 2017.
- Accepted for publication February 6, 2017.




{kind=link}