
Article Figures & Data
Figures
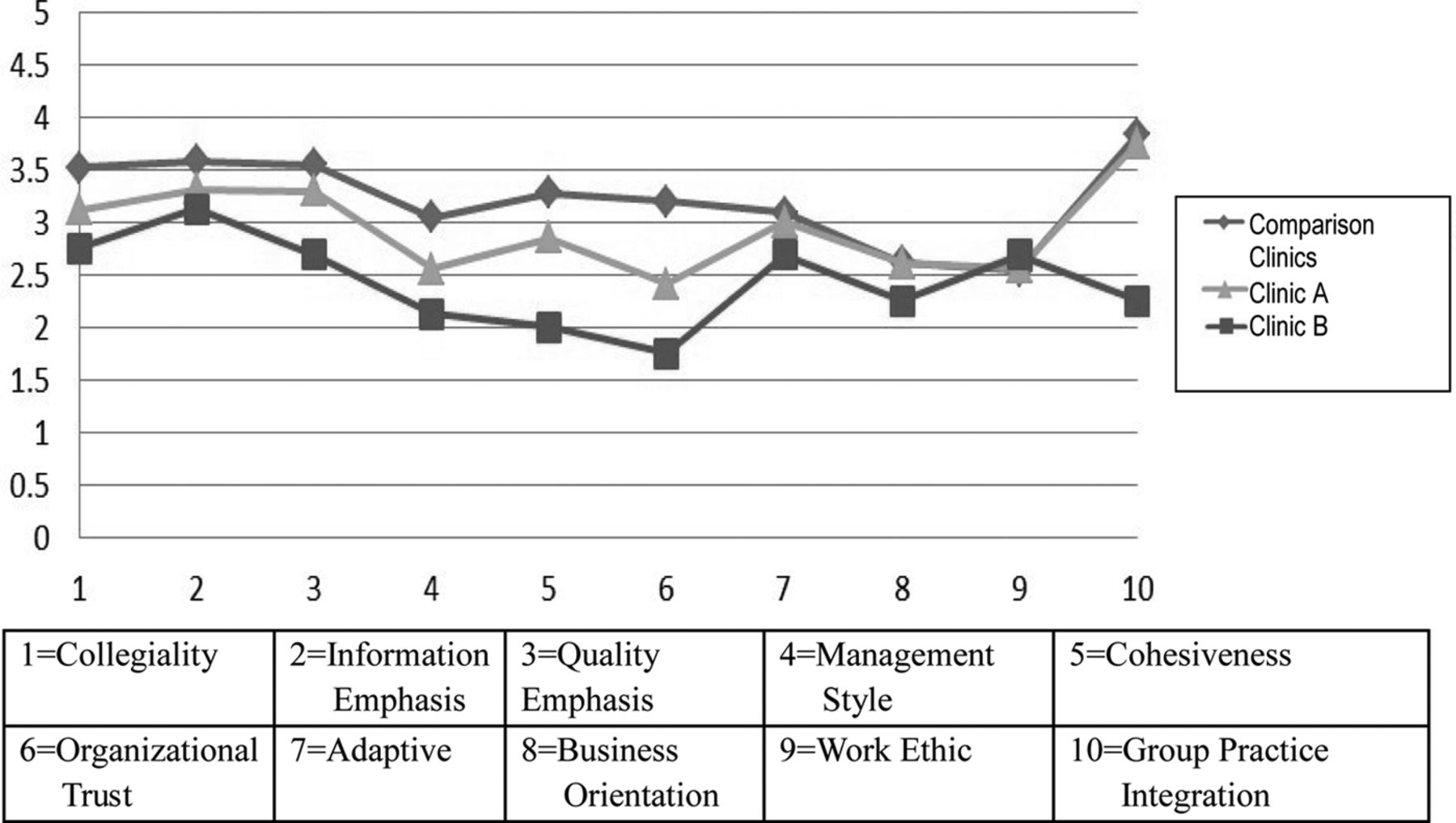
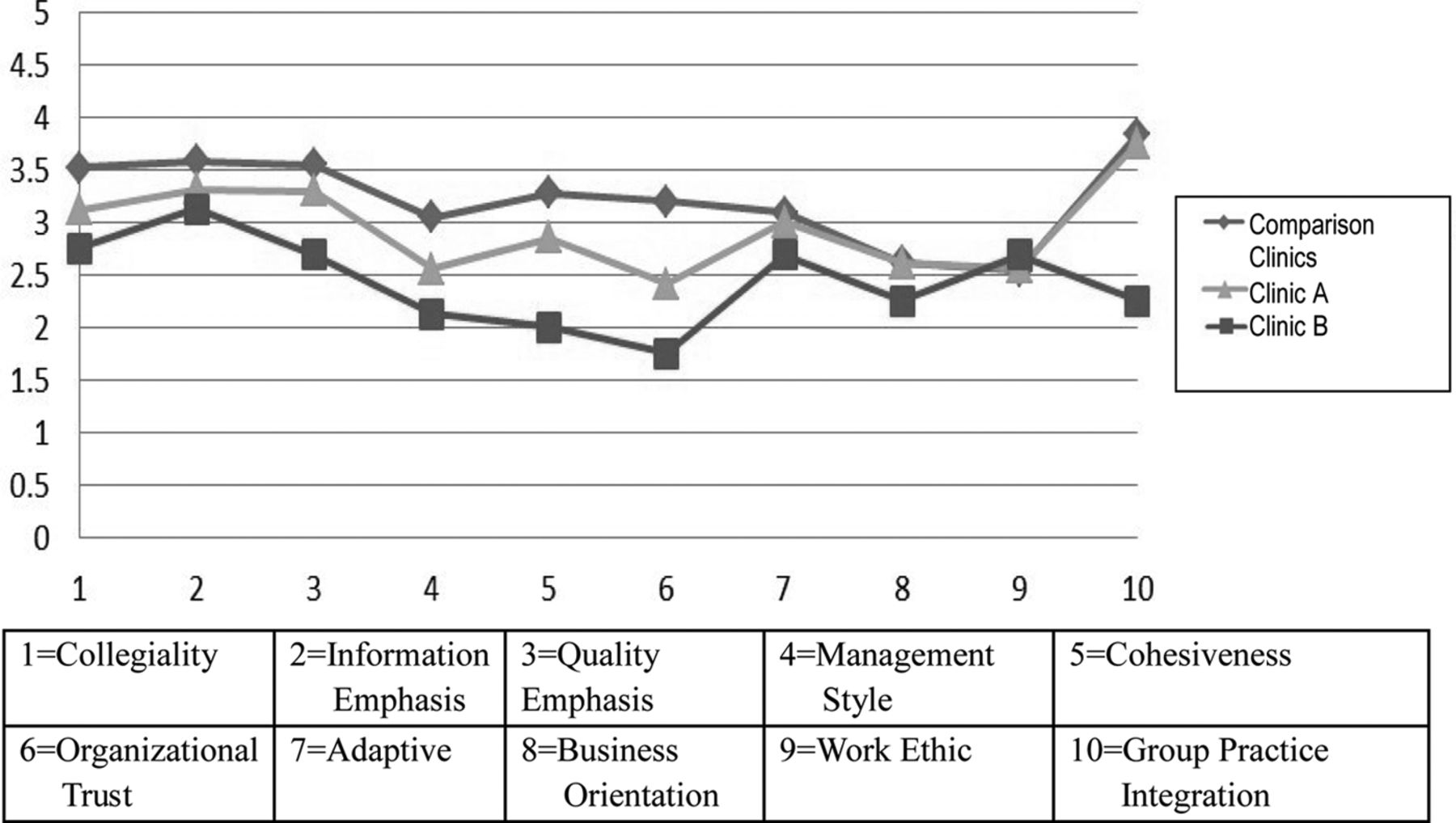
- Figure 1.
Culture assessment scores13 (mean score on a 1 to 5 scale with 5 highest) for Clinics A and B compared with the comparison clinics that had not yet transitioned.
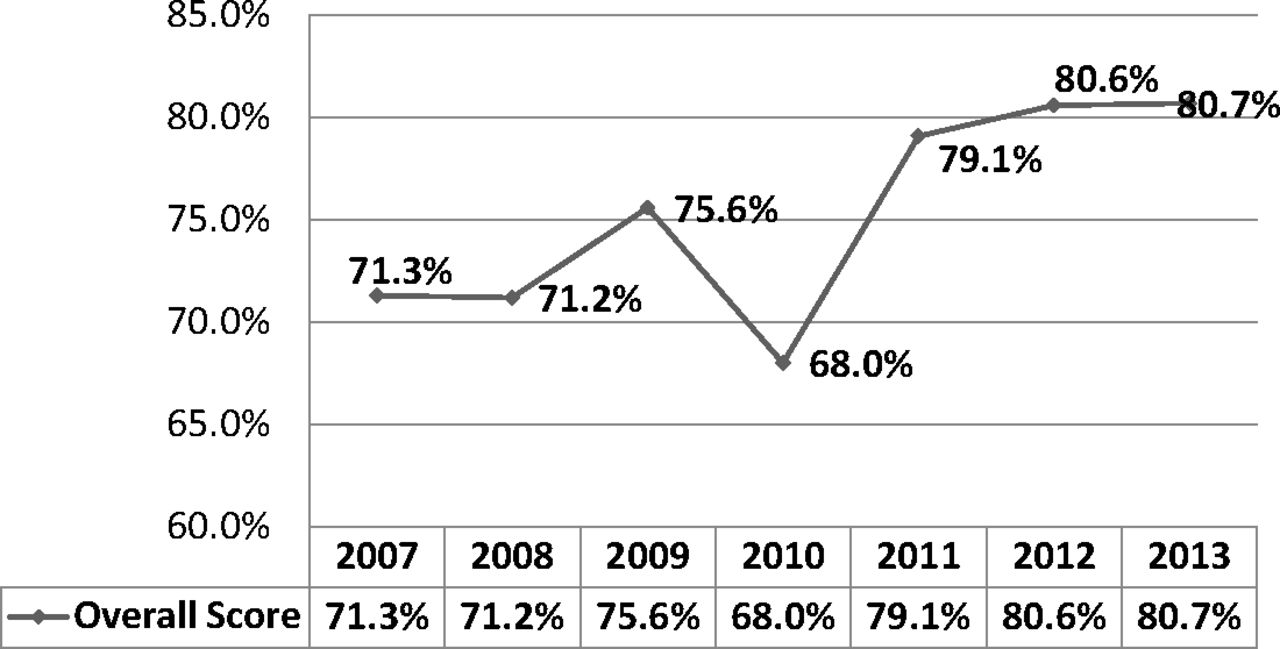
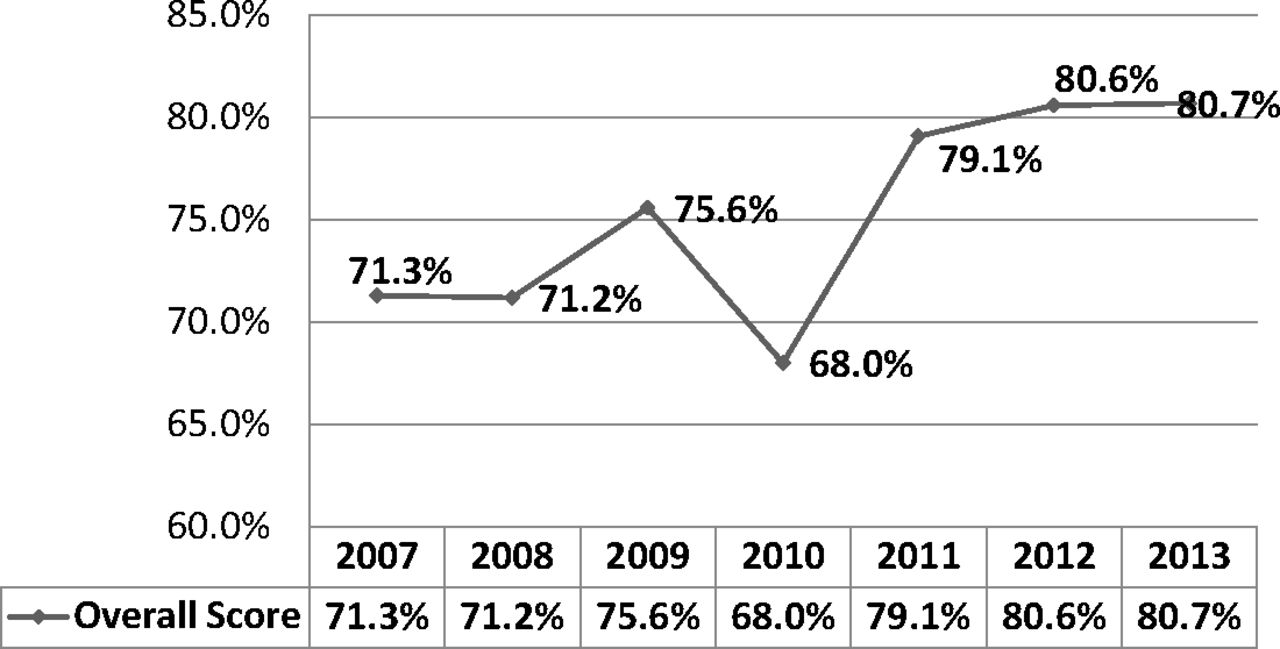
- Figure 2.
Percent of patient respondents rating their health care experience at Clinic A as satisfactory or very satisfactory on Press Ganey patient satisfaction instruments.14 2007 was before transition; 2008 and 2009 during transition; and 2010 to 2013 after transition.
Tables
- Table 1.
Descriptive Information for Clinic A Before (2007), During (2009), and After (2013) the Transition to an Open-Access, Patient-Centered Care Model
Clinic A Clinic B Before Transition (2007) During Transition (2009) After Transition (2013) Before Transition (2007) Full-time equivalent (FTE)* primary care physicians 7.9 8.5 9.3 6.6 FTE nurse practitioners 1.5 0.9 0.8 1.0 FTE support staff 18.2 23.1 29.4 16.5 Registered nurse 4.9 7.4 10.4 3 Registered nurse care coordinator 0.6 Licensed practical nurse /medical assistant 10.0 10.6 13.0 Technician (lab, x-ray) 4.3 5.1 5.4 Total revenue $6,297,991 $6,195,565 $8,958,742 6,084,362 Active patient charts# 14,383 12,340 Average No. patients/normal work day for physician/Nurse Practitioner 15.6/15.6 17/19 Average number of patients/ hour for physician/Nurse Practitioner 4/3 13/13 2.2/2.5 2/2 Net revenue per operating costs 48% 51% Description of Clinic B Before the transition (2007). During and after transition data for Clinic B were incomplete.
Specialty physicians and their support staff, pharmacists and social worker are not included.
↵* 1 FTE equals 34 clinical contact hours per week.
↵# Active charts includes patients seen in the last two years.
- Table 2.
Position Categories for 32 Individuals in Five Stakeholder Groups Interviewed During this Case Study of Clinics A and B
Stakeholder Group Position Category Leaders 3 medical directors, 2 physician leaders at Clinics A and B Managers 2 quality improvement manager, 2 clinic managers at Clinics A and B Clinicians at Clinics A and B 4 physicians, 2 nurse practitioners Nurses at Clinics A and B 5 registered nurses, 3 licensed practical nurses, 6 medical assistants Reception staff at Clinics A and B 3 front desk/reception staff Individual interviews occurred with leaders (5) and managers (4). Two discussion groups were conducted at each clinic (AM and noon hour). Group sizes ranged from five to six individuals, including a total of 23 clinicians, nurses and reception staff.
Financial personnel were interviewed but data are not included in this count or in the report.
- Table 3.
Quotations Illustrating the Human Factors Identified during Interviews or Discussion Groups of the Five Stakeholder Groups in This Case Study
Response to Change Medical Director Health System leader: “I walked out of the last of three planning meetings in the C-suite not believing we could really do this.” Medical Director Health System leader: “In hindsight, we missed the scariness and grief about what we asked them to give up.” Quality Improvement Manager: “Following change theory, some clinics and people embrace change and others do not. Instead they find it difficult and disruptive. Stress levels of staff were high, for some higher than others. Some providers jumped on board and others refused to collaborate with their teams.” Clinic Manager: “We needed to understand the incredible toll on staff, we kept asking folks to do more, to work longer hours, do homework at night. At first it was exciting, but also stressful. They were working harder, but also enjoying it more.” Clinic Manager: “We were cutting costs and the hospital volumes dropped. Hospital administrators got nervous and there was push back.” Clinic Manager: “Nurses started overseeing self-collected samples for vaginitis. Patients celebrated the end of stirrups, but lab personnel were initially reluctant to accept the specimens.” Clinic Manager: “Physicians who could not give up control and embrace teamwork left, but others heard about what we were doing, applied, and were hired.” Nurse: “At one point I felt like we were jumping off a cliff. At night I studied about anti-hypertensive drugs. I needed to understand them if I was responsible for suggesting medication changes to patients. Of course, I could ask for help, but it was very stressful.” Quality Improvement Manager: “One of our biggest learnings was that we need to match trajectory of change to business model and keep in synch. Corporate moved too fast. In our market, our payer and us were the first to do this. We still couldn't bill for our population health or e-visits. We had to scale back. The back paddling was tough as well.” Personal and Professional challenge due to role redefinition: Physician Health System Leader: “The most successful clinics are those that embraced the team-based model—gave up own work to a care team and trusted staff. Practices where doctors own their results and can't share the work with the team still complain about WAC [work after clinic].” Physician leader: “The solo hero western model that embraces ‘I am your doctor’ had to change to ‘I am your doctor and my team includes …” Physician: “I liked leaving the blood pressure med increase and vaginitis for the nurses. I had more time to focus on the challenging cases and my panel pushed 3000.” Physician: “I work every day of the week to take care of our patients and have no ‘days off.’ I function as the quarterback with only 28 hours of scheduled patients and each appointment is 30 minutes. The rest of the time is for e-visits, phone visits and paperwork. A good number of these patients are new to our system. They heard about how we deliver care differently and are intrigued! Each of these patients has a complete intake by our staff to update all of their history as well as current questions and needs. We address every issue and take the time to create and document a care plan for each issue including preventive care. We make sure the patient takes ownership for the care plan as well and has access to it.” Registered Nurse: “I was uncomfortable with the added responsibility at first … I was adjusting blood pressure medications based on a protocol. I could ask for help, but I spent many hours preparing for the next day at home.” Registered Nurse: “But two years later, when we had to scale nurse visits back because we couldn't bill for them, we [nurses] went back to being shackled to our phones and computers.” Nurse Practitioner: “Those who struggled had to let go of what they were used to doing, had to trust that someone else would do it. We had to work as a team.” Reception staff: “Every provider [including nurses] and staff had their own computer, received information and entered patient information into the system. Nursing and reception had access to the physician's inbox. We had to trust each other.” Communication: Clinic Manager: “We spent time building our team. We used personality tests for communication styles. We did exercises to create a safe place to work out our challenges.” Clinic Manager: “We couldn't communicate enough. In the beginning we huddled three times a day. Some weeks we came in early and met for an hour before clinic started. We often worked over lunch, looking at our data and planning the next move.” Physician leader: “Communication wasn't enough, we needed to create a robust environment for dialogue; dialogue, not communication. There needed to be an easy flow down and back up all the time.” Physician: “Team members are co-located in a specific area where they can communicate real time with issues in an efficient manner. Whenever possible, issues are managed immediately.” Quality Improvement NP: “We need to meet frequently to understand the data for our rapid PDSA (Plan-do-study-act) cycles. We had great IT support.”




{kind=link}
{kind=link}