
Article Figures & Data
Figures
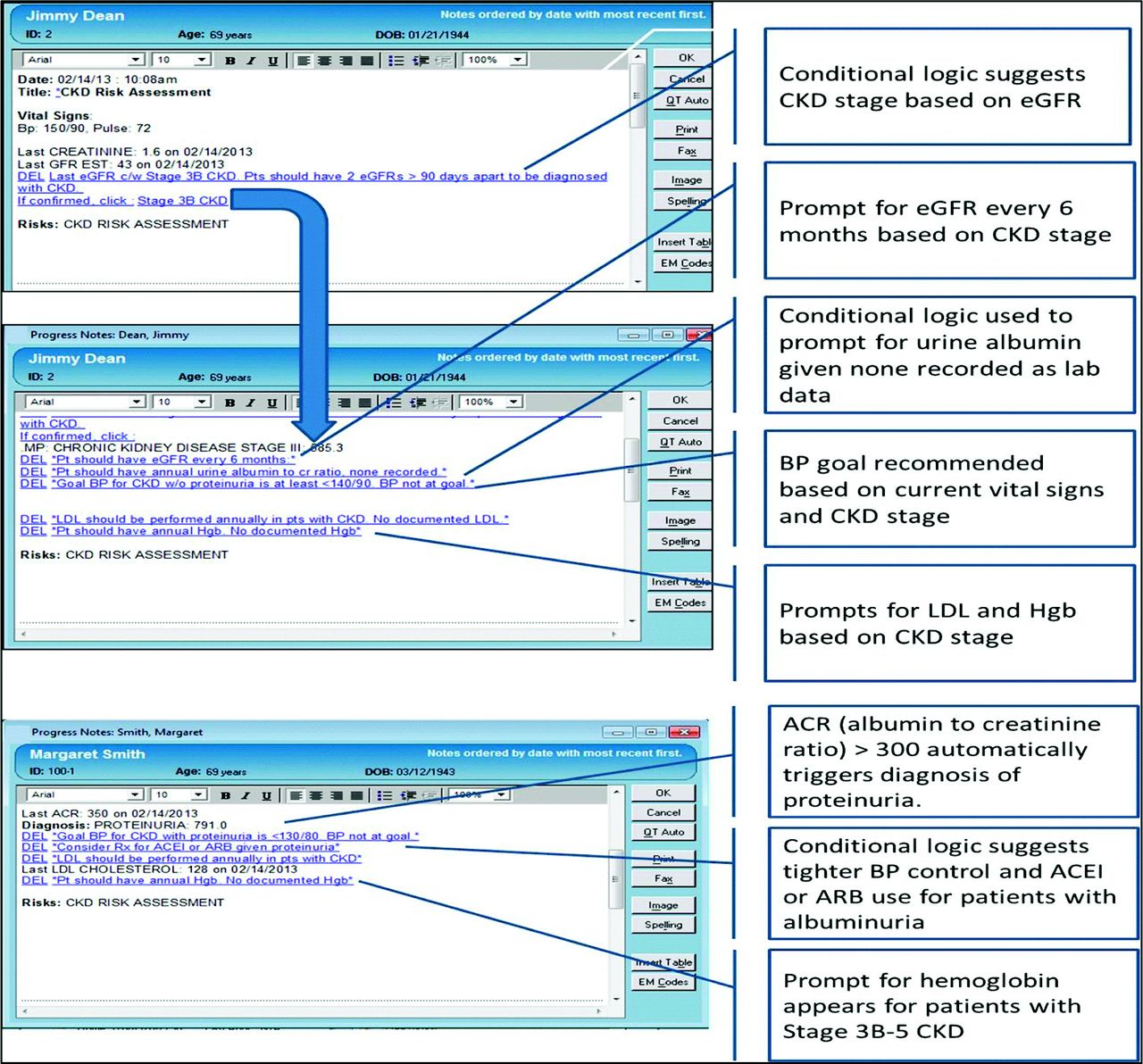
- Figure 1.
Chronic kidney disease (CKD) risk assessment tool. ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; BP, blood pressure; eGFR, estimated glomerular filtration rate; Hgb, hemoglobin; LDL, low-density lipoprotein.
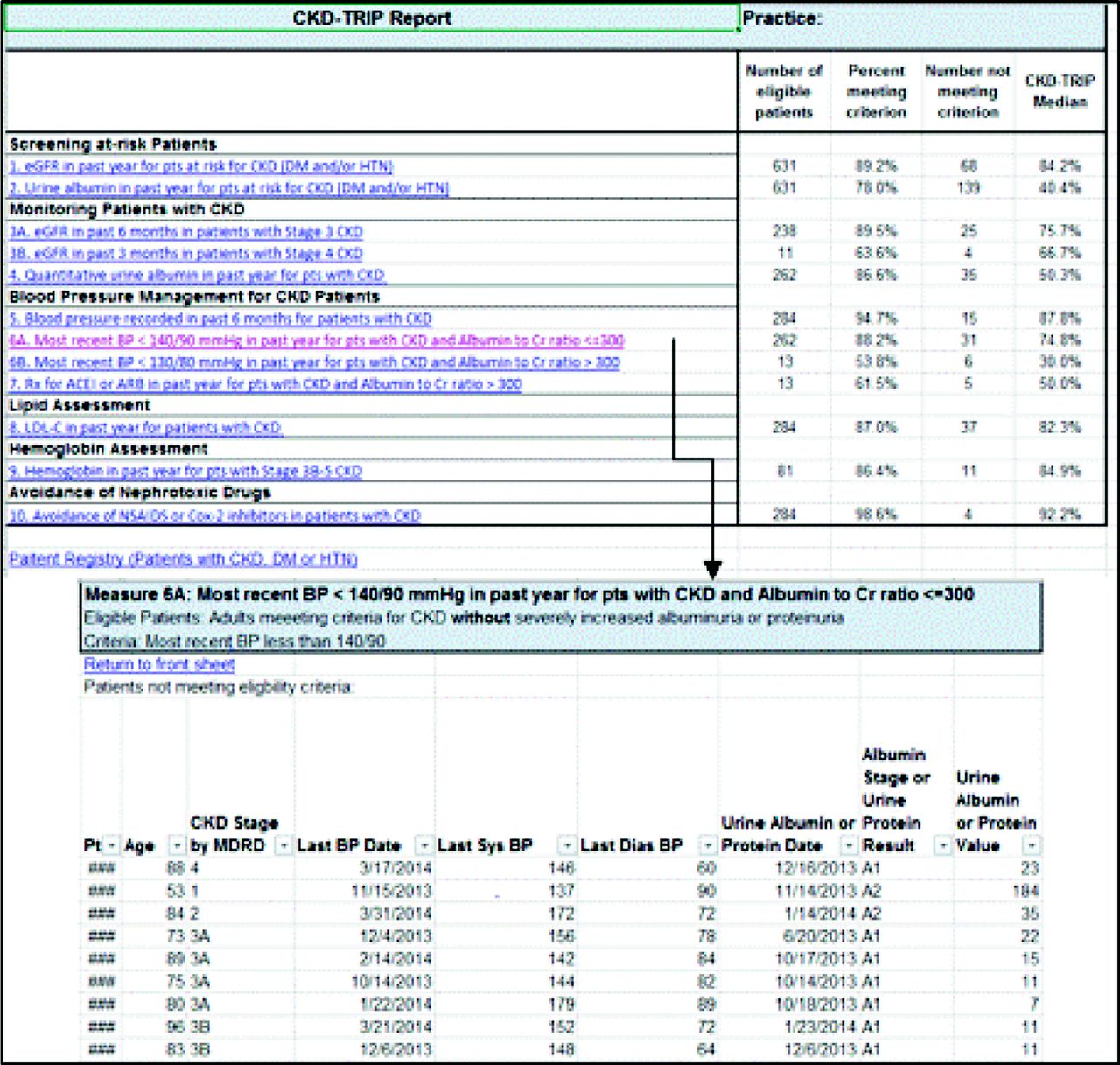
- Figure 2.
Chronic kidney disease flowchart.
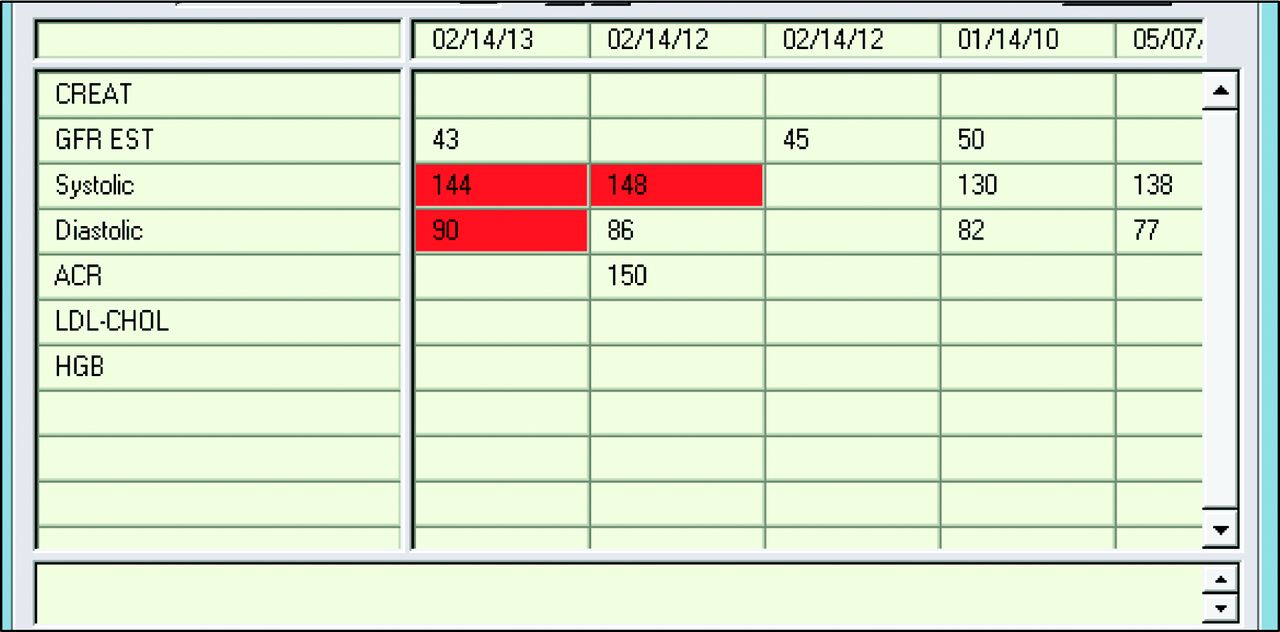
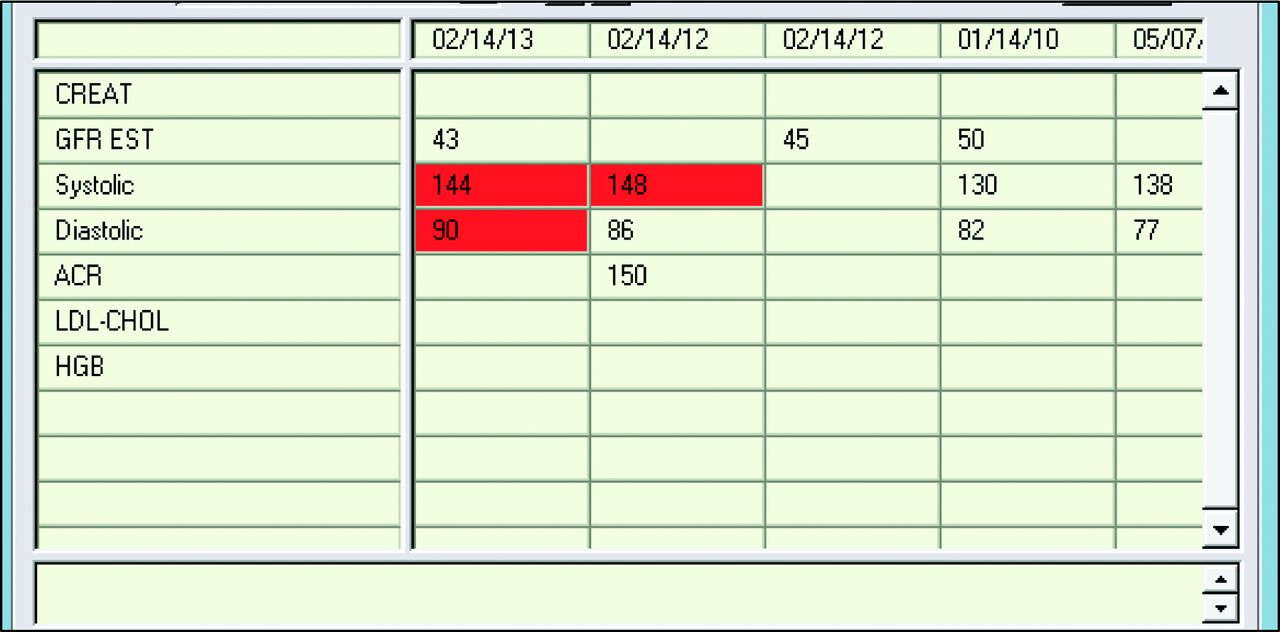
- Figure 3.
Chronic kidney disease patient registry.


Tables
State Specialty Providers Clinical Staff Members Patients per Clinician (Mean) 1 WI Family medicine 2 MDs 1 RN, 3 MAs 933 2 TN Family medicine 2 MDs 2 LPNs, 2 MAs 1299 3 CO Internal medicine 1 MD, 1 NP, 1 PA 1 RN, 2 MAs 2271 (assigned to MD only) 4 WA Family medicine 1 MD 1 RN 521 5 NJ Family medicine 1 MD 0 636 6 OH Internal medicine 3 MDs 1 RN, 3 LPNs, 2 MAs 886 7 PA Family medicine 4 MDs, 1 NP, 3 PAs 5 RN, 11 LPN, 4 MAs 723 per MD; 884 per midlevel provider 8 CT Family medicine 4 MDs 4 MAs 1041 9 AZ Family medicine 2 MDs, 1 PA 3 MAs 2032 per MD; 959 per PA 10 CA Family medicine 3 MDs 3 PAs 7 MAs 1831 per MD; 147 per PA 11 MI Family medicine 1 MD 4 MAs 1629 12 MD Family medicine 1 MD, 4 NPs, 1 PA 4 MAs 3061 per MD; 254 per midlevel provider LPN, licensed practical nurse; MA, medical assistant; MD, medical or osteopathic doctor; NP, nurse practitioner; PA, physician assistant; RN, registered nurse.
- Table 2.
Performance on Chronic Kidney Disease Clinical Quality Measures over the 24-Month Intervention
CKD Clinical Quality Measure Baseline 24 Months Change from Baseline to Month 24 (%M24−BL) %BL NBL %M24 NM24 Identification of patients with CKD eGFR in the past year for patients with DM and/or hypertension 87 (80, 93) 929 (590, 1303) 87.5 (82, 92) 795 (608, 1256) 0.5 (−2.0, 5.0) Screening for albuminuria in the past year for patients with DM and/or hypertension 21.5 (16, 26) 929.5 (590, 1303) 59 (37, 73) 795 (608, 1256) 30.0 (23.0, 46.0)* Monitoring patients with CKD eGFR in the past 6 months for patients with stage 3 CKD 76 (72, 86) 169.5 (122, 279) 80.5 (76, 83) 205.5 (149, 263) 0.5 (−3.0, 3.0) eGFR in the past 3 months for patients with stage 4 CKD 75 (63, 80) 10.5 (5, 16) 74 (63, 80) 11.5 (7, 15) −3.0 (−7.0, 0.0) Monitoring albuminuria in past year for patients with CKD (without prior macroalbuminuria or proteinuria) 34.5 (27, 55) 190.5 (131, 356) 63 (53, 83) 325 (201, 420) 25.0 (22.0, 31.0)* BP management in patients with CKD Most recent BP <140/90 mmHg for patients with CKD without macroalbuminuria or proteinuria 76 (68, 83) 191.5 (131, 357) 76.5 (73, 82) 325.5 (201, 422) 2.5 (0.0, 7.0) Most recent BP <130/80 mmHg for patients with CKD with macroalbuminuria or proteinuria 33 (30, 57) 2.5 (1, 7) 29 (13, 33) 8.5 (3, 15) −1.5 (−50.5, 9.0) ACEI or ARB in the past year for patients with CKD and hypertension with macroalbuminuria or proteinuria 53.5 (43, 67) 2.5 (1, 7) 65.5 (52, 100) 8.5 (3, 15) 23.5 (−5.5, 43.5) Dyslipidemia in patients with CKD Lipid panel in the past year for patients with CKD 84.5 (82, 87) 202.5 (131, 367) 84 (82, 88) 340.5 (209, 441) −0.5 (−4.0, 1.0) Anemia in patients with CKD Hemoglobin in the past year for patients with eGFR <45 77 (74, 82) 60 (34, 110) 86 (70, 91) 69.5 (39, 91) 7.0 (0.0, 8.0) Avoidance of potential nephrotoxic drugs Avoidance of NSAIDs or COX-2 inhibitors in patients with CKD 94 (91, 96) 202.5 (131, 367) 92 (92, 94) 340.5 (209, 441) −1.0 (−2.0, 1.0) Data are median (25th percentile, 75th percentile).
↵* P < .0005.
%BL, Proportion of testing at baseline; %M24, proportion of testing at month 24; %M24−BL, absolute change in proportion; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; CKD, chronic kidney disease; COX-2, cyclooxygenase 2; eGFR, estimated glomerular filtration rate; DM, diabetes mellitus; BP, blood pressure; NBL, number of patients eligible for testing at baseline; NM24, number of patients eligible for testing at month 24; NSAID, nonsteroidal anti-inflammatory drug.
- Table 3.
Reported Facilitators and Barriers to Use of Clinical Decision Support Tools to Improve Chronic Kidney Disease Management
Facilitators Barriers Provider factors ∙ CDS helps focus provider attention on CKD
∙ Perception by users that CDS improves care
∙ Disagreement about CKD guidelines
∙ Confusion about CKD guidelines
∙ Concerns about data validity
∙ Patients comanaged by nephrologists
∙ Lack of awareness of CDS tools
Organizational factors ∙ Practice-wide prioritization of identifying patients with CKD
∙ In-office urine collection and/or albumin testing
∙ Standing orders for laboratory tests
∙ Patient registry used by staff for patient outreach
∙ Staff turnover
∙ Competing obligations (other incentive programs)
∙ Failure to fully implement standing orders
Technical factors ∙ CDS tools customized to workflow of practices by research team during site visits
∙ Research team able to troubleshoot CDS at site visits
∙ Research team demonstrated use of patient registry during site visits
∙ CDS tools required “extra clicks”
∙ Risk assessment tool did not always work
∙ Reports and tools did not capture labs ordered by specialists
∙ Use of registry required re-identifying patients
Patient factors ∙ Patient education about CKD (including educational handouts)
∙ Changing patients' expectations to adhere to urine testing
∙ Concern about patients seeing diagnosis of CKD
∙ Concern about overdiagnosis of CKD
CKD, chronic kidney disease; CDS, clinical decision support.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Barriers and Facilitators to the Use of Clinical Decision Support Systems in Primary Care: A Mixed-Methods Systematic Review
- Chronic Kidney Disease Testing Among Primary Care Patients With Type 2 Diabetes Across 24 U.S. Health Care Organizations
- Quality improvement at scale: evaluation of the drivers and barriers to adoption and sustainability of an intervention to reduce late referral in chronic kidney disease
- Use of a Medical-Alert Accessory in CKD: A Pilot Study
- Content Usage and the Most Frequently Read Articles of 2016
- Evidence, Engagement, and Technology: Themes of and the State of Primary Care Practice-based Network Research