
Abstract
Purpose: The goal of this study was to assess perspectives of racially/ethnically diverse, low-income pregnant women on how doula services (nonmedical maternal support) may influence the outcomes of pregnancy and childbirth.
Methods: We conducted 4 in-depth focus group discussions with low-income pregnant women. We used a selective coding scheme based on 5 themes (agency, personal security, connectedness, respect, and knowledge) identified in the Good Birth framework, and we analyzed salient themes in the context of the Gelberg-Anderson behavioral model and the social determinants of health.
Results: Participants identified the role doulas played in mitigating the effects of social determinants. The 5 themes of the Good Birth framework characterized the means by which nonmedical support from doulas influenced the pathways between social determinants of health and birth outcomes. By addressing health literacy and social support needs, pregnant women noted that doulas affect access to and the quality of health care services received during pregnancy and birth.
Conclusions: Access to doula services for pregnant women who are at risk of poor birth outcomes may help to disrupt the pervasive influence of social determinants as predisposing factors for health during pregnancy and childbirth.
Social determinants of health (SDOHs), including economic stability, level of education, neighborhood and environment, and social relationships and interactions,1 are predisposing factors that influence health outcomes.2⇓–4 The impact of SDOHs is heightened among vulnerable populations, and they play a crucial role in maternal and infant health outcomes.5
For example, women who have or develop conditions such as diabetes or hypertension during pregnancy are more likely to have a primary cesarean delivery or preterm birth.6 Development of these and related conditions, including obesity, relates to the structural and environmental factors that affect access to exercise and nutrition.6 Women who experience intimate partner violence and exposure to abuse are more likely to have little or no prenatal care, be hospitalized during pregnancy, and give birth to low-birth-weight infants.7,8 Unsafe neighborhoods and adverse environmental exposures increase the likelihood of preterm birth.9⇓–11 Low health literacy among pregnant women is associated with low attendance of prenatal care visits and poor birth outcomes.12,13 Women with low socioeconomic status have greater chances of having a low-birth-weight infant or a preterm birth.14 In addition, pregnant women with limited social support are more likely to have a low-birth-weight infant.15
The pathways between SDOHs and birth outcomes have contributed to pervasive racial/ethnic disparities in maternal health and health care.16⇓–18 Longstanding and complex sociodemographic and historic factors perpetuate the challenges women of color face in achieving positive birth outcomes.19–20 These disparities have persisted despite clinical and nonclinical approaches and interventions in the health care setting, and few solutions with the potential to effectively disrupt the pathway between SDOHs and poor birth outcomes have been identified.16,21
Nonmedical interventions are preferred options in addressing SDOHs.22 Doulas are trained professionals who provide continuous, 1-on-1 emotional and informational support during the perinatal period. Similar to community health workers, they are not medical professionals and do not provide medical services, but work alongside health care providers. Studies show that doula care is associated with lower epidural use and cesarean delivery rates, shorter labors, higher rates of spontaneous vaginal birth, and higher levels of satisfaction.23⇓⇓⇓–27 Low-income women and women of color, who have the highest risk of poor birth outcomes, are also the most likely groups to report wanting, but not having, access to doula services.26 The current evidence base is lacking effective means of mitigating the effects of SDOHs on birth outcomes for these high-risk populations. The goal of this study was to assess perspectives among racially/ethnically diverse, low-income pregnant women of how access to and support from a doula may influence the outcomes of pregnancy and childbirth.
Methods
Conceptual Model
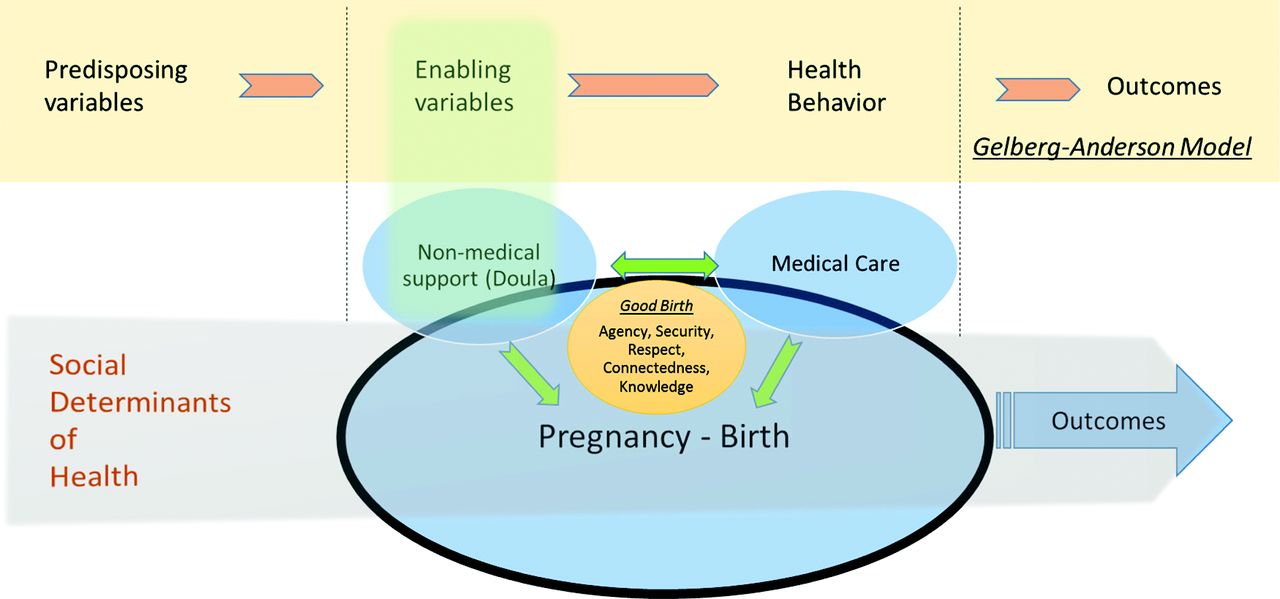
We used the Gelberg-Anderson model of health behavior4, and components of the Good Birth framework28 to create a conceptual model to describe the role of doulas—and of medical care—in the pathway between SDOHs and birth outcomes. SDOHs are present before, during, and after pregnancy, but their effects on birth outcomes may be moderated by the quality of clinical care and the nonmedical support a woman receives (Figure 1).
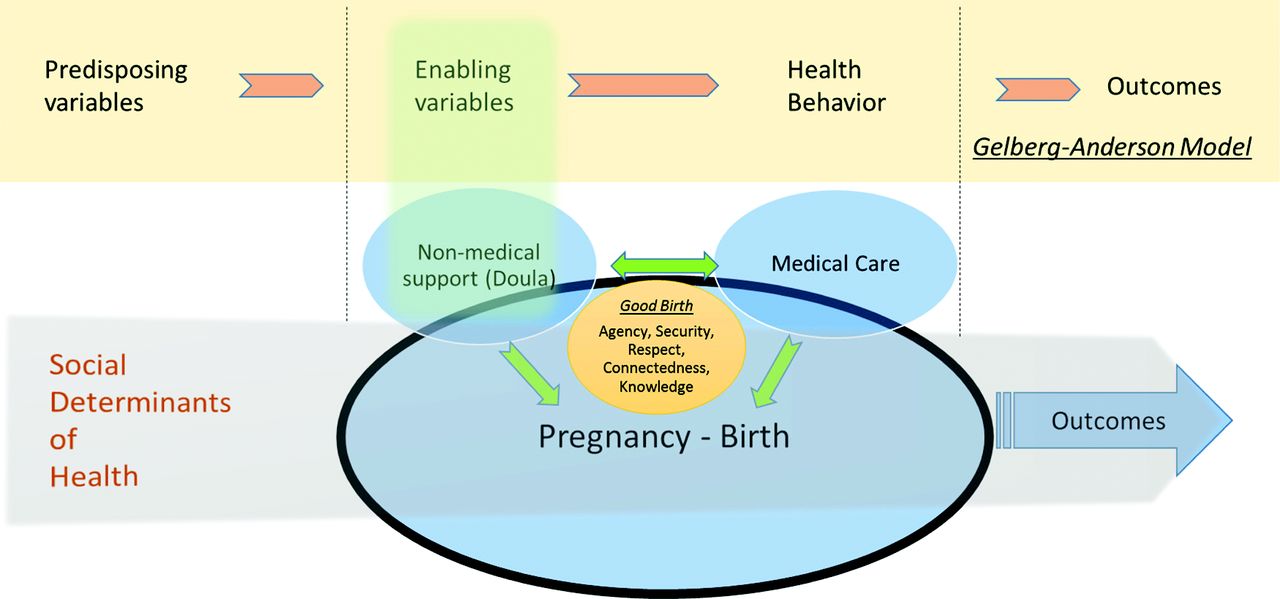
Conceptual model of the pathways between social determinants of health and birth outcomes and the role of non-medical support.
The Gelberg-Anderson model of health behavior focuses on vulnerable populations.4 The Predisposing, Enabling, and Need components of this model predict personal health practices, including the use of health services. The Predisposing domain includes “demographic characteristics” and “social structure patterned social arrangements in society that are both emergent from and determinant of the actions of the individuals.”4 Social structure includes a variety of components that create the context by which SDOHs are manifested and maintained. Thus our study considers the SDOHs1 to be a component of the Predisposing domain. The Predisposing variables affect Enabling variables (eg, social support, health services resources, ability to negotiate the system), which subsequently affect Need. In our framework the Enabling variables include doula services, which are directly associated with a pregnant woman's perceived need for help. Gelberg and colleagues4 suggest that health behaviors and health outcomes will subsequently be impacted by Need. When placing this model within the context of childbirth within vulnerable populations, we also consider the elements of Agency, Personal Security, Connectedness, Respect, and Knowledge that Dr. Anne Lyerly identified as characteristic of a good birth.28 These elements of a good birth can inform strategies to meet the physical and emotional needs of women during pregnancy and childbirth.28 Our model frames the context in which the trajectory of a woman's pregnancy and the SDOHs may be influenced by the support of a doula, the clinical care she receives, and potentially by the interactions between the doula and the patient's clinician.
Study Participants
Thirteen racially/ethnically diverse, low-income pregnant women participated in 4 focus group discussions that were held at 3 locations in Minneapolis, Minnesota, in November and December 2014. Multiple methods (flyers, E-mails, and word of mouth) were used for recruitment. Inclusion criteria included pregnancy and fluency in English. The role of a doula was explained at the outset of the interview, and prior experience with a doula was not required so as not to exclude potential participants who may not have been able to afford or access doula services. All participants consented to participate using a human subjects protection process approved by the University of Minnesota institutional review board (code no. 1403S49085).
Data and Measurement
In collaboration with community-based partners, we developed and pilot-tested a questionnaire to guide semistructured focus group discussions. These discussions were facilitated by 2 investigators (RRH and CAV), both of whom are trained and experienced in qualitative data collection and analysis. Each focus group included between 2 and 6 participants. We had planned for 3 focus groups of 5 to 7 women; however, inclement weather precluded participation for several women in the first scheduled focus group, so we scheduled a fourth focus group meeting to allow their participation. Data saturation was achieved with 4 focus groups. All of the focus group discussions were recorded and transcribed using CaptionSync Professional Transcription, a service provided by Automatic Sync Technologies, LLC (Seattle, WA). Manual notes taken by the facilitators (RRH, CAV) were used to augment the transcripts where comments were inaudible during the recording.
Questions focused on reasons for and barriers to doula support, and the ways doulas influence pregnancy and birth, based on prior research.24⇓⇓–27,29 We used the themes of the good birth framework (agency, personal security, respect, knowledge, connectedness)28 in a deductive approach to code the transcripts. We also created and used separate codes that highlighted (1) the mechanisms associated with doula support and healthy pregnancy, and (2) the relationship of these mechanisms with SDOHs.
Analysis
The initial coding was separately and independently validated using a coanalysis method among the authors (CV, RRH, KBK).30 Coding was conducted in a shared Microsoft Excel document (Microsoft Corp., Redmond, WA). After the first round of coding, we met to discuss differences among coders and to refine codes and definitions for clarity. Then, one of the authors (CAV) led a second round of coding, grouping each of the codes to identify which themes emerged as patterns across the focus groups. We then followed the same 2-step process to code the transcripts for specific mechanisms of doula support that were associated with birth outcomes.
Results
The study participants represented a racial/ethnically diverse group of women, as described in Table 1. Participants were nearly evenly split between nulliparous and parous, and three quarters of participants had a doula supporting them during their current pregnancy. Nearly 40% of women who participated in the focus groups voluntarily disclosed that their pregnancy was complicated by a medical condition (such as hypertension, prior preterm birth, or gestational diabetes).
Descriptive Characteristics of Focus Group Participants
Table 2 contains information on each of the key themes, with illustrative quotes, as described below.
Exemplary Quotations on Key Themes of the Qualitative Analysis
Agency
“[Having a doula] helps prepare you mentally; like it is gotten me more in the mind-set of … the confidence throughout the pregnancy knowing that I can do this….”
Agency is the capacity of an individual to act or to make his/her own choices (as opposed to being someone to whom things happen).28 Low-income and racially/ethnically diverse women suffer a lack of agency in their medical care.31,32 Our findings suggest that doulas play an important role in equipping low-income, diverse pregnant women with agency by either prompting the expression of concerns or by facilitating interactions with the health care provider (Table 2, quote 2). Having a doula plays an important role in a woman's ability to make an informed decision while positively influencing her belief in herself (Table 2 quote 1).
Personal Security
“… I talk to the doctor … and I am calling the doula right after that…. Like, I am scared… and she's like, oh, no do not be…. It is very comforting to know that you have somebody [who] has your back.”
Physical and emotional safety plays an important role in pregnancy and childbirth. Feeling secure, comfortable, and calm is particularly crucial for women contending with complex social circumstances (eg, an unstable living situation, an unsupportive partner). As reflected in the above quote, the respondent's doula contributed to her personal security by addressing her health concerns after an encounter with her provider. This concept of security extends to the incorporation of culturally concordant beliefs about childbirth and personal safety (Table 2, quote 5).
Respect
“… Having someone that is not only knowledgeable, but can put things in layman's terms, in a way that you understand it and respects your culture … your well-being, your upbringing and things about you … to make sure that the baby is okay too.”
Respect is critical to a patient-centered experience, and a physician's respect of a patient's autonomy is often cited as an important goal of the birthing process.28 Further, respect is the basis of informed consent.28 Autonomy in decision making is a marker of respect and was discussed among focus group participants as a key component (Table 2, quote 8). This theme was echoed throughout the groups, and there was consensus that a doula's presence, particularly during the childbirth process, would facilitate greater autonomy and respect in decision making.
Knowledge
“My reasons for wanting a doula. [It is] because I do not have nobody right now, and if I go into labor, … I do not know the techniques or how to calm down.”
Our findings suggest that doulas play a critical role in imparting knowledge to their clients and empowering them to become knowledgeable about the physiologic process of pregnancy. Some women gain this knowledge from their health care providers; however, many of the participants suggested that they often did not fully understand some of the things their provider shared with them. In these instances they relied on their doula to help “translate” their clinical encounters. In addition, having a doula present to share techniques and pass on wisdom and birth strategies is important (Table 2, quote 12). Doulas also play an important role in connecting women with resources to gain new knowledge as they prepare for childbirth (Table 2, quotes 11 and 13).
Connectedness
“… It is good to have a doula because the doctors will say this and your family may say this, but the doula is mindful of who you are.”
Connectedness considers the level at which a woman feels connected to the resources that are available, her clinicians, her infant, and the support people in her life—including her doula. Participants observed that doulas play an important role in ensuring that women who lack social support do not feel isolated (Table 2, quote 14). Women expressed that the connection with their doula would make a difference in their pregnancy and childbirth, sometimes even more so than a health care provider or family member (Table 2, quote 16). Women found the connection with their doula to be important for the general support that the doula provides, beyond specific knowledge or guidance in the birth process (Table 2, quote 15). Many of the participants described stressful life situations and emphasized the desire to connect with a person who shared their culture and background (Table 2, quote 17).
Discussion
Participant responses revealed that nonmedical support from a doula could play a role in helping women overcome barriers to achieving a healthy pregnancy and childbirth. Women's responses aligned with 2 key categories of SDOHs defined in HealthyPeople 20201: health and health care; and social and community context. While the skills they bring and the support they provide are nonmedical, doulas play a role in pregnant women's ability to access health services and in the quality of care they receive by addressing the women's health literacy and social support needs, as well as through interaction with prenatal and intrapartum care providers. While clinicians provide direct patient care in the context of the health and health care SDOH category, study participants also identified doulas as facilitators of improved patient–provider interactions that influence satisfaction with the birth experience and favorable birth outcomes.
Much of the current research on successful interventions to address SDOHs at the time of childbirth come from the international context,33 but programs addressing SDOHs for maternal and child health are increasingly being adopted in the United States, largely owing to the persistence of disparities despite medically focused interventions. For example, a community-based project in California serves as a model for successfully addressing SDOHs to reduce racial disparities and improve birth outcomes for African American women.34 This program shifted prenatal care and case management to include support groups that educate, inform, empower, and connect women socially, culturally, and financially.34 Our findings are consistent with the those that emerged from the California initiative. However, our findings extend the learnings gleaned from individual projects and programs to explore a concept (nonmedical support) that can be integrated within health care financing and delivery systems to affect system change and potentially create long-term, sustainable solutions to persistent disparities in birth outcomes.
Much prior research on doula care has been conducted among white, upper-middle-class women and/or in a randomized controlled trial context.23,29 While emerging research shows that the known benefits of doula care may be even greater among vulnerable populations,24,26 those who could most benefit from doula care frequently have the least access to it.23 Future work should examine the perspectives of doulas and of clinicians to further inform the conceptual model developed here. In addition, policy and clinical efforts to increase access to doula services should address cultural, financial, and geographic barriers to care identified by pregnant women.
Implications for Policy
Access to culturally concordant care and support during childbirth was noted as a potential benefit of doula services by the women in our study, but a lack of diversity among the doula workforce was seen as a potential barrier. Difficulty in ensuring representativeness among doulas is likely exacerbated by the fact that doula services are rarely covered by health insurance, thus creating a barrier to entry into this profession that disproportionately affects low-income communities.29,35 Recent research on doula care and cost savings, especially among low-income women, has ignited discussion regarding reimbursement of doula care by health insurance programs, including Medicaid.24,26,27 Two states (Oregon and Minnesota) currently allow Medicaid reimbursement for doula services. Minnesota passed legislation in May 2013 establishing Medicaid reimbursement for doulas, which became effective starting September 25, 2014, upon federal approval.36 Implementation challenges have been substantial and include alack of awareness about doula services on the part of pregnant women, maternity care clinicians, hospitals, and clinics, and the health insurance plans that provide coverage to Medicaid beneficiaries.37 This research provides a framework for understanding how doula care may influence the pathways between SDOHs and birth outcome, which may inform future efforts to expand health insurance coverage of doula services and integrate nonmedical support within health care delivery systems.
Implications for Clinical Practice
Means of addressing SDOHs are not inherently present in current health care delivery models. In childbirth in particular there is a tendency toward a “technocratic” approach that privileges medical care over nonmedical support.38 Pregnancy and childbirth are critical junctures in the life course, when the impacts of social determinants are heightened. Increasingly, women giving birth in the United States are doing so in isolation, with a lack of personal, social, and emotional support.39,40 Recent studies have highlighted the importance of trust within the patient–provider relationship, the challenges this presents for low-income women, and the resulting effects on overall quality and disparities in maternal and child health outcomes.41,42
Prior research has suggested the need for adequate clinical care, as well as personal support at the individual level, during pregnancy.41 Doulas were seen in our study as providing social support to help improve communication between low-income, racially/ethnically diverse pregnant women and their health care providers via an increase in women's agency and knowledge during pregnancy. Women in our study indicated that doulas helped to create an environment of trust. Our study reflected the sense of engagement and connectedness participants felt in the presence of doulas, and noted that this presence can enhance the clinical encounter via improving the process of informed consent and increasing patient satisfaction.23
Limitations
The sample used for this study included 13 women and was a convenience sample from 1 metropolitan area of the United States; thus broad generalizations cannot be made. This exploratory study helped to generate a conceptual model that sets forth hypotheses for future work but does not establish a causal pathway. The focus groups took place during the early phases of implementation of Medicaid coverage of doula services in Minnesota and do not reflect full implementation of that policy, which may influence access to doula care by vulnerable populations. These results indicate the need for further investigation of the role of nonmedical support in addressing SDOHs.
Conclusions
Improving access to doula services by pregnant women who are at risk of poor birth outcomes may enhance clinical efforts to overcome the pervasive influence of SDOHs on pregnancy and childbirth. This study contributes to the growing body of evidence that doulas are a social support intervention that can influence the pathways between social determinants and birth outcomes by addressing some of the underlying issues that evade clinical approaches to persistent disparities.
Acknowledgments
The authors gratefully acknowledge data entry support from Shruthi Kamisetty and input and feedback provided by Amanda Huber, CMN; Rita O'Reilly, CNM; Debby Prudhomme; and Mary Williams, LPN. This research would not have been possible without the collaboration of our community partners, Everyday Miracles, Cultural Wellness Center, and Missionaries of Charity, all located in Minneapolis, MN.
Notes
This article was externally peer reviewed.
Funding: Research reported in this article was supported a Community Health Collaborative Grant from the National Center for Advancing Translational Sciences of the National Institutes of Health (award no. UL1TR000114).
Conflict of interest: none declared.
Disclaimer: The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
- Received for publication September 12, 2015.
- Revision received November 3, 2015.
- Accepted for publication November 19, 2015.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Community-based doulas for migrant and refugee women: a mixed-method systematic review and narrative synthesis
- Social Distancing in the Era of COVID-19: A Call for Maintaining Social Support for the Maternal Population
- Impact of a Population-based Systems Approach on Evidence-based Care for Medicaid-insured Pregnant and Postpartum Women: A Quasi-Experimental Study
- Sisters in Birth: Improving Birth Outcomes in Mississippi
- Outcomes of Care for 1,892 Doula-Supported Adolescent Births in the United States: The DONA International Data Project, 2000 to 2013
- Social Determinants of Health and Primary Care: Intentionality Is Key to the Data We Collect and the Interventions We Pursue