
Article Figures & Data
Figures
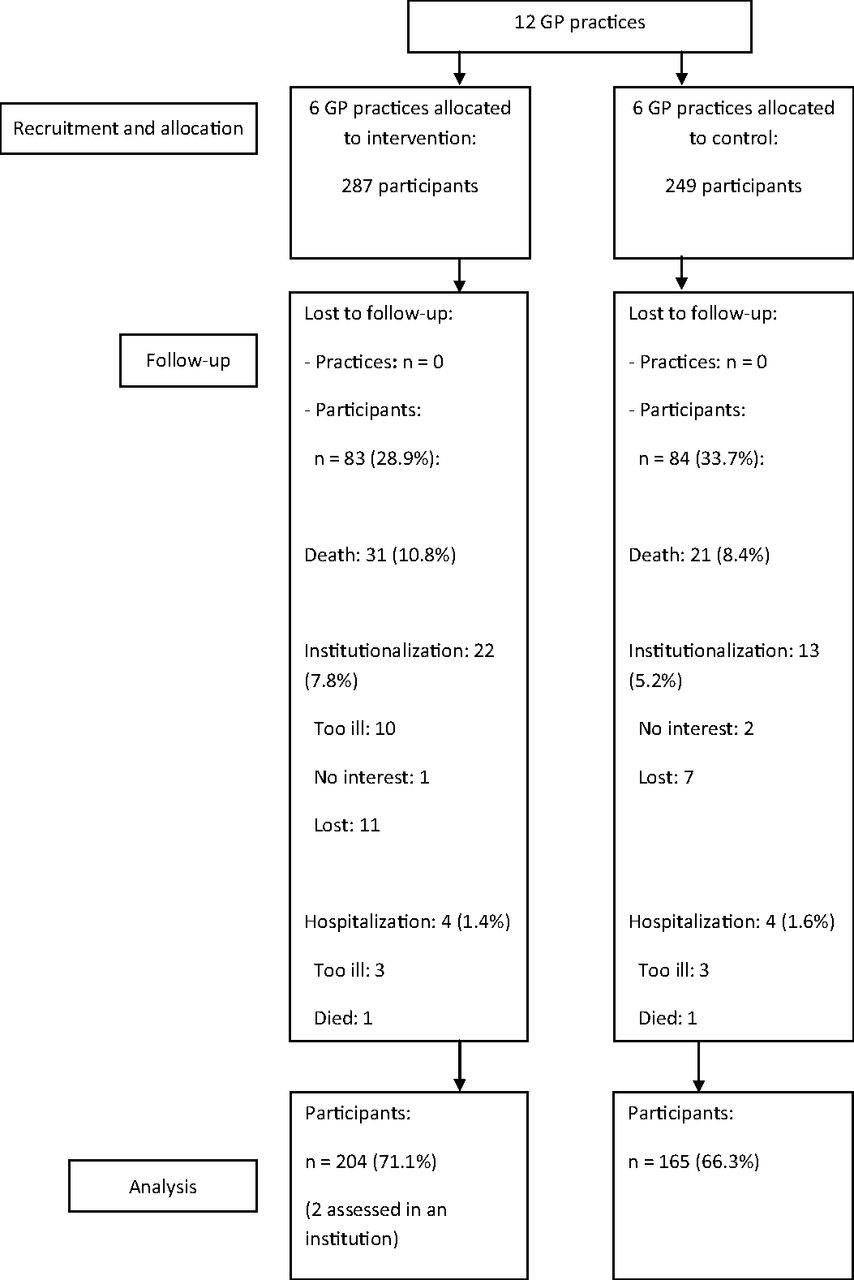
- Figure 1.
Flow diagram of practices and participants. GP, general practitioner.

Tables
- Table 1. Baseline Characteristics of Participants in the Intervention Group and Control Group
Characteristics CareWell Primary Care (n = 287) Usual Care (n = 249) P Value for Difference Age (years), mean (SD) 83.1 (5.6) 80.5 (6.0) .42 Female sex 192 (66.9) 160 (64.3) .52 Living alone 182 (63.4) 136 (54.6) .039 Socioeconomic status score,* mean (SD) 0.5 (1.1) 0.2 (0.5) <.001 Low level of education 69 (24.1) 100 (41.0) <.001 Cognition score,† mean (SD) 7.5 (7.0) 5.3 (4.8) <.001 Katz-15 index,‡ mean (SD) 5.4 (2.9) 4.6 (2.7) .33 EQ-5D+C,§ mean (SD) 0.6 (0.3) 0.6 (0.3) .08 RAND-36 mental health¶ 61.1 (13.1) 62.4 (13.7) .38 Presence of health-related limitations in social functioning‖ 178 (64.3) 88 (37.1) <.001 Frailty index,** mean (SD) 0.4 (0.2) 0.4 (0.2) .90 Presence of care complexity 60 (21.1) 75 (30.1) .017 Data are expressed as numbers (percentage) unless otherwise indicated.
↵* Socioeconomic status score was based on postal code areas (income, employment, and education); a higher score indicates more social disadvantage.
↵† Based on a modified Mini-Mental State Examination (range, 0–28); a higher score indicates more cognitive problems.
↵‡ Katz-15 scores range from 0 to 15; a higher score indicates more dependence in (instrumental) activities of daily living.
↵§ EQ-5D+C scores range from −0.33 to 1.00; a higher score indicates a higher health-related quality of life.
↵¶ The 36-item RAND Mental Health questionnaire (RAND-36) scores range from 0 to 100; a higher score indicates better mental health.
↵‖ Based on the social functioning subscale of the RAND-36. Answers were dichotomized as the “absence of limitations” vs. the other categories indicating the “presence of limitations.”
↵** The frailty index measures accumulated deficits (scale 0 to 1); a higher index suggests a more frail status.
EQ-5+C, EuroQuol instrument; SD, standard deviation.
Outcome CareWell Primary Care* (n = 204) Usual Care* (n = 165) Estimated Intervention Effect* (95% CI) P Value Baseline Change at Follow-up Baseline Change at Follow-up Katz-15 index† 5.4 (2.9) 0.8 (1.9) 4.6 (2.7) 0.5 (2.1) 0.37 (−0.1 to 0.8) .10 EQ-5D+C‡ 0.6 (0.3) 0.0 (0.3) 0.6 (0.3) 0.0 (0.3) −0.031 (−0.1 to 0.0) .37 RAND-36 mental health§ 61.1 (13.1) −0.28 (13.6) 62.4 (13.7) −0.8 (13.7) 0.86 (−2.3 to 4.0) .56 Health-related limitations in social functioning¶ 1.5 (1.4) −0.1 (1.6) 0.9 (1.3) 0.3 (1.7) 0.037 (0.2–0.2) .76 Data are mean (standard deviation) unless otherwise indicated.
↵* Adjusted for clustering; baseline values of relevant covariates (living situation, health-related limitations in social functioning, cognition score, socioeconomic status score, and care complexity); baseline value of the Katz-15 index; and, in the case of secondary outcomes, baseline value of the outcome parameter.
↵† Katz-15 scores range from 0 to 15; a higher score indicates more dependence in (instrumental) activities of daily living.
↵‡ EQ-5D+C scores range from −0.33 to 1.00; a higher score indicates a higher health-related quality of life.
↵§ The 36-item RAND Mental Health questionnaire (RAND-36) mental health scores range from 0 to 100; a higher score indicates better mental health.
↵¶ Based on the social functioning subscale of the RAND-36. Answers are dichotomized as the “absence of limitations” vs. the other categories indicating the “presence of limitations.”
CI, confidence interval; EQ-5D+C, EuroQol instrument.
Outcome CareWell Primary Care (n = 204) Usual Care (n = 165) Odds Ratio (95% CI) P Value Residential and nursing home admissions 24 (8.3) 13 (5.2) 1.32 (0.64–2.71) .46 Hospital admissions 52 (18.1) 57 (22.9) 0.74 (0.48–1.14) .17 Mortality 31 (10.8) 21 (8.4) 1.13 (0.61–2.08) .70 Data are n (%) unless otherwise indicated. CI, confidence interval.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Personalised care planning for older people with frailty: a review of factors influencing implementation
- Understanding the implementation of interventions to improve the management of frailty in primary care: a rapid realist review
- What long-term care interventions have been published between 2010 and 2020? Results of a WHO scoping review identifying long-term care interventions for older people around the world
- Use of standardized brief geriatric evaluation compared with routine care in general practice for preventing functional decline: a pragmatic cluster-randomized trial
- Cross-sectional study evaluating the association between integrated care and health-related quality of life (HRQOL) in Dutch primary care
- Frailty assessment in primary health care and its association with unplanned secondary care use: a rapid review
- Outcomes of Health System Structures, Highly Pertinent Clinical Information, Idea Stimulators, Clinical Reviews, and Prediction Tools: JABFM Exemplified