
Article Figures & Data
Figures
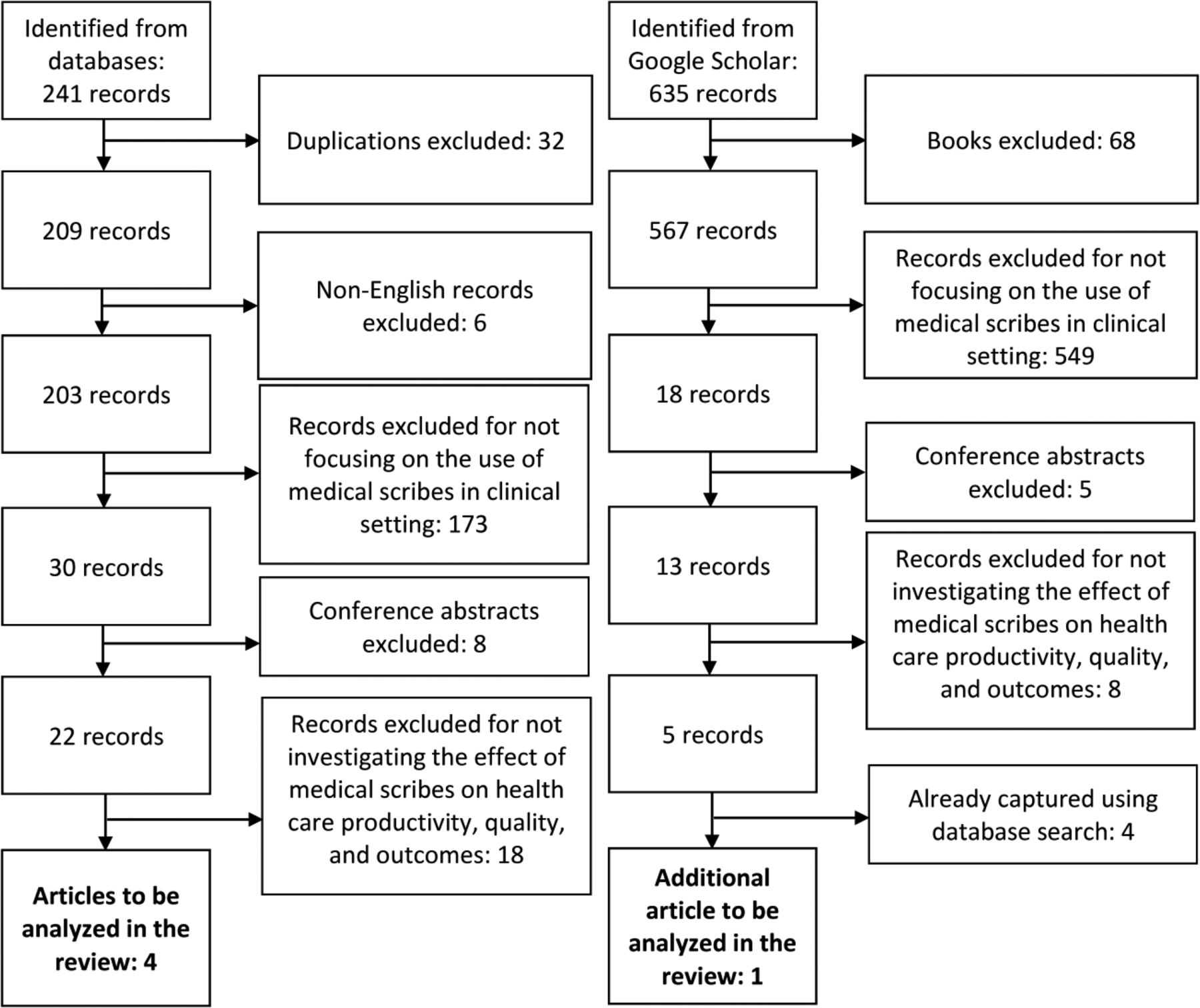
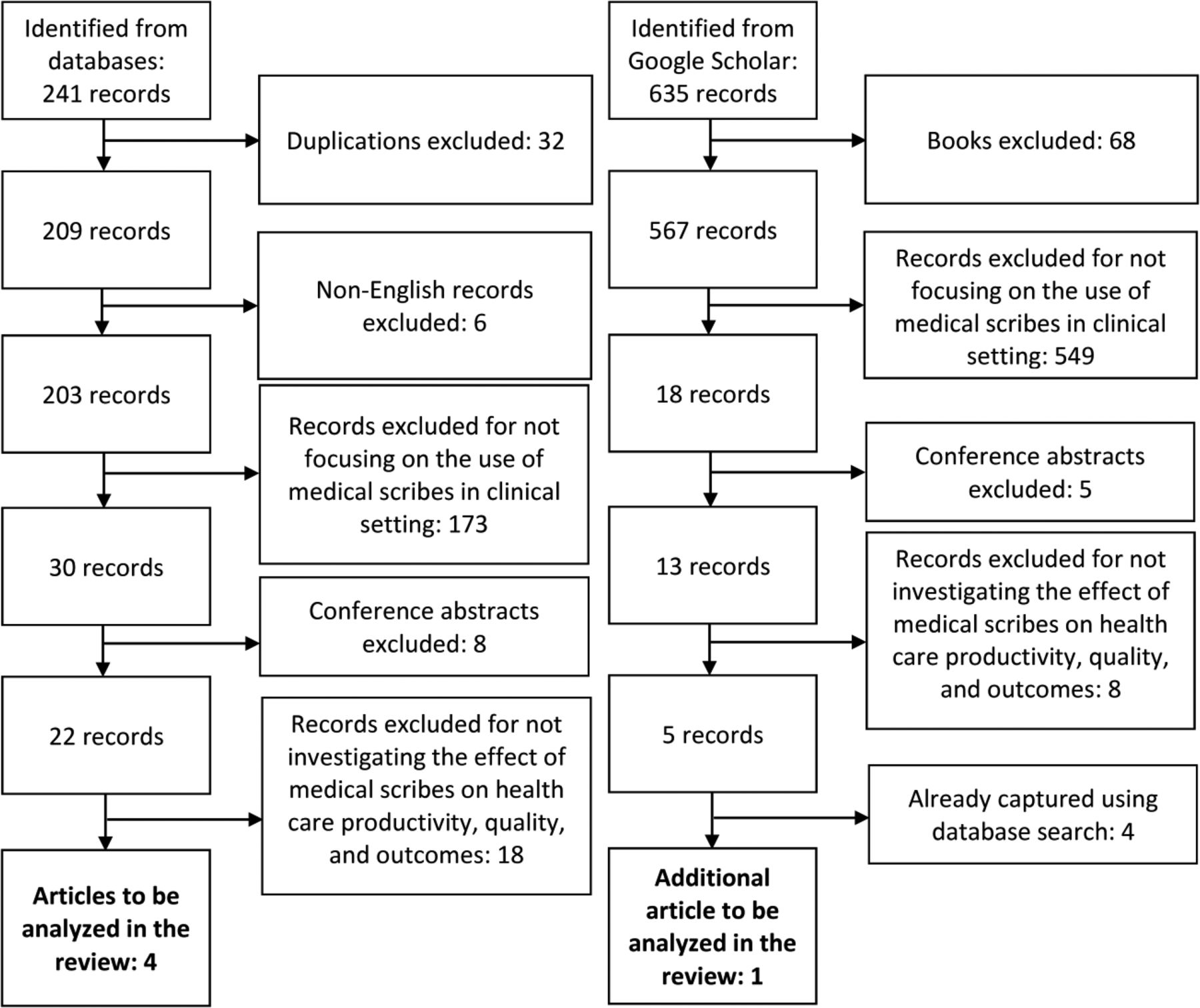
- Figure 1.
Flow diagram of the search strategy used to identify literature investigating the effect of medical scribes on health care productivity, quality, and outcomes. The database search queried the Cochrane Library, the OvidSP Medline database, and the Embase database from January 2000 through September 2014 for articles using scribe or scribes in the title or abstract. The Google Scholar search queried English-language sources (excluding patents and citations) posted from January 2000 through September 2014 and using scribe or scribes in the title.
Tables
- Table 1. Characteristics of English-Language, Peer-Reviewed Studies Assessing the Effect of Medical Scribes on Health Care Productivity, Quality, and Outcomes
Article Setting and Sample Study Design and Scribe Type Measured Outcomes Arya et al25 ∙ Emergency department within a single academic medical center
∙ 243 shifts
∙ 13 emergency physicians
∙ Data collected on all adult (≥21 years old) patient visits∙ Nonrandomized, static-group comparison study
∙ Matched design (shifts with and without scribes)
∙ Scribes: from preexisting program operated through the academic medical center∙ RVU/hour
∙ Patients/hour
∙ Turnaround time to discharge (minutes)Koshy et al26 ∙ Urology clinic within a single academic medical center
∙ 5 urologists; residents
∙ 487 patient surveys
∙ 55 physician surveys∙ Nonrandomized, static-group comparison study
∙ Matched design (shifts with and without scribes)
∙ Scribes: premedical students or first-year medical students∙ Patient acceptance and satisfaction
∙ Physician acceptance and satisfactionBank et al27 ∙ Cardiology clinic within a large, not-for-profit health care organization
∙ 65 hours of clinic care on both control and scribe days
∙ 4 cardiologists
∙ 130 clinic hours
∙ 339 patient visits∙ Nonrandomized, static-group comparison study
∙ Matched design (days with and without scribes); patient visits on scribe days were scheduled to be 25% shorter
∙ Scribe: professional scribe from a medical scribe service∙ Patients seen
∙ wRVU/hour
∙ Patient satisfaction
∙ Physician-patient interaction
∙ RevenueBastani et al28 ∙ Emergency department in a suburban community hospital
∙ Patient encounters over the 11-month study, with “washout” time between groups
∙ Before CPOE, n = 10,578
∙ After CPOE and before scribe, n = 11,729
∙ After scribe, n = 12,609∙ Nonrandomized, 2-stage pretest/posttest design (baseline/before CPOE, after CPOE, and after scribe) with static-group comparison
∙ Scribes: premedical, prenursing, and pre–physician assistant students from a local 4-year university; employed via a professional scribe service∙ Door-to-room time
∙ Room-to-doctor time
∙ Door-to-doctor time
∙ Doctor-to-disposition time
∙ Duration of stay for discharged/admitted patients
∙ Patient satisfactionAllen et al29 ∙ Adult emergency department within a single academic medical center
∙ Patient encounters over the 23-month study, with “washout” time between groups
∙ 11-month periods before and after scribe
∙ 18 residents
∙ 8 physician assistants
∙ 4 nurse practitioners∙ Nonrandomized, pretest/posttest design (before scribe and after scribe)
∙ Scribes: not specified∙ Patients admitted, discharged, and left without being seen
∙ Door-to-triage time
∙ Door-to-room time
∙ Door-to-clinician time
∙ Door-to-disposition time
∙ Door-to-exit time
∙ Clinician-to-disposition time
∙ Disposition-to-exit time
∙ Room-to-disposition time
∙ Room-to-exit time
∙ Clinician satisfactionCPOE, computerized physician order entry; RVU, relative value unit; wRVU, work relative value unit.
Study Duties Arya et al25 ∙ Dedicated service to only one emergency department physician per shift
∙ Create, transcribe, and complete documentation of the patient's medical record
∙ Communicate laboratory and radiography results to physician in a timely manner
∙ Complete medical documentation as instructed by physician
∙ Document time of procedures, calls from physicians, and timeliness of events
∙ Chart narratives, such as course of events in the emergency departmentKoshy et al26 ∙ Dedicated service to a limited number of select urologists, working with only one physician per shift
∙ Record medical information throughout the patient–physician encounterBank et al27 ∙ Dedicated service to a limited number of select cardiologists, working with only one physician per shift Review records before shift and generate preliminary notes
∙ Summarize pertinent clinical visits, hospitalizations, and medical history
∙ Modify progress note and search for additional information at physician's request
∙ Enter diagnoses, revise problem list, complete follow-up request form, type patient instructions, document level of service, complete after-visit summaryBastani et al28 ∙ Dedicated service to only one physician per shift
∙ Document the initial history, review of systems, and physical examination Record all procedures, consultations, and reevaluations
∙ Document electrocardiogram, pulse oximetry, and rhythm strip interpretation
∙ Detail diagnoses, treatment plans, prescriptions, and discharge/follow-up information
∙ Track laboratory and imaging tests, keep a task list, cross-check consultations, and follow admission requests
∙ Complete all charts before the end of shiftAllen et al29 ∙ Medical documentation services to all clinicians (excluding first-year residents) working in a designated area
∙ Provide medical documentation services, including history of present illness, review of systems, physical exam, lab results, and medical decision making
∙ Complete charting of the emergency medical record- Table 3. The Effect of Medical Scribes on Patient Satisfaction, Clinician Satisfaction, Productivity, Revenue, Time/Efficiency, and Patient–Clinician Interaction, By Study
Study Patient Satisfaction Clinician Satisfaction Productivity Revenue Time/ Efficiency Patient–Clinician Interaction Arya et al25 — — RVUs per hour increased
Patients per hour increased— Statistically significant difference in turnaround time to discharge not detected — Koshy et al26 Statistically significant difference not detected Physician satisfaction increased with scribe — — — — Bank et al27 Statistically significant difference not detected — Patients per hour increased
Total wRVUs per hour increasedAdditional revenue was generated as a function of increased patient volume Direct patient contact time was lower for scribe visits, but amount of patient interaction without the computer was greater Single-rater observation scored scribe visits as better in patient–provider interaction Bastani et al28 Statistically significant difference between time periods before CPOE and after scribe not detected
Time periods before CPOE and after scribe were perceived more favorably than the time period after CPOE/before scribe— — — Door-to-room time remained consistent across all 3 waves
Door-to-doctor time increased after CPOE/before scribe but returned back to pre-CPOE levels in the after-scribe time period
Doctor-to-admit disposition time decreased after scribe when compared with time periods before CPOE and after CPOE/before scribe— Allen et al29 — Physician satisfaction increased with scribe Statistically significant difference in the number of patients per day not detected
Proportion of admitted patients increased— Admitted patients:
Door-to-triage, door-to-room, door-to-disposition, and clinician-to-disposition times decreased
Door-to-exit and disposition-to-exit times increased
Discharged patients:
Door-to-disposition, door-to-exit, clinician-to-disposition, and disposition-to-exit times decreased— CPOE, computerized physician order entry; RVU, relative value unit; wRVU, work relative value unit.
- Table 4. Strength of Recommendation Taxonomy: Key Recommendations on the Use of Medical Scribes
Practice Recommendation Evidence Rating* References 1. There is insufficient high-quality evidence to support the claim that medical scribes affect patient satisfaction. B 26–28 2. There is insufficient high-quality evidence to support the claim that medical scribes affect physician satisfaction. B 26, 29 3. There is insufficient high-quality evidence to support the claim that medical scribes affect physician productivity. B 25, 27, 29 4. There is insufficient high-quality evidence to support the claim that medical scribes affect revenue. B 27 5. There is insufficient high-quality evidence to support the claim that medical scribes affect time-related efficiencies. B 25, 27–29 6. There is insufficient high-quality evidence to support the claim that medical scribes affect the quality of the patient–clinician interaction. B 27 ↵* A, recommendation based on consistent and good-quality, patient-oriented evidence; B, recommendation based on inconsistent or limited-quality, patient-oriented evidence; C, recommendation based on consensus, usual practice, expert opinion, disease-oriented evidence, and case series for studies of diagnosis, treatment, prevention, or screening. See Ebell et al30 for more information about the strength of recommendation taxonomy evidence rating system.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Primary Care Clinician Burnout and Engagement Association With Clinical Quality and Patient Experience
- Scenario-based design for a hospital setting: An exploratory study of opportunities and barriers for personal health records usage
- Physician Well-being
- Impact of scribes on emergency medicine doctors productivity and patient throughput: multicentre randomised trial
- Finance and Time Use Implications of Team Documentation for Primary Care: A Microsimulation
- Transforming Nephrology
- One Year of Family Physicians' Observations on Working with Medical Scribes
- Primary care scribes: writing a new story for safety net clinics
- Impact of Scribes on Physician Satisfaction, Patient Satisfaction, and Charting Efficiency: A Randomized Controlled Trial
- Next big thing: integrating medical scribes into academic medical centres
- Re: The Use of Medical Scribes in Health Care Settings: A Systematic Review and Future Directions
- Response: Re: The Use of Medical Scribes in Health Care Settings: A Systematic Review and Future Directions
- Re: The Use of Medical Scribes in Health Care Settings: A Systematic Review and Future Directions
- Electronic Health Record Innovations for Healthier Patients and Happier Doctors