
Abstract
Background: To compare the outcomes of Comprehensive Geriatric Assessments by family physicians and geriatricians.
Methods: An explorative observational study was conducted in six family practices (12 ambulatory family practitioners) and 1 geriatric department (4 hospital-based geriatricians) from a university medical center in Nijmegen (the Netherlands). As participants, we included 587 patients aged 70 years and older and registered in the six family practices. The main outcome measures were the judgment on the following: 1) absence or presence of frailty and 2) the state (good-fair-poor) on 8 underlying domains (physical, medication, cognition, sensory, instrumental activities of daily living scale, mobility, mental, and social) according to family Physicians and geriatricians based on a Comprehensive Geriatric Assessment.
Results: Family physicians and geriatricians agreed on frailty absence/presence in 76% of cases. Geriatricians considered elderly more often frail than family physicians did (n = 294, 50% vs n = 213, 36%). Disagreement on frailty status was notably found in the patients who had less distinct, either poor or good, health states. Discordant frailty judgments, in which the geriatrician rated a person as frail and the family physicians did not, were related to geriatricians more often rating physical health as impaired. Further, geriatricians' judgments of frailty were more strongly related to impaired scores on the domains cognition, sensory, mobility, and mental compared with family physicians judgments: odds ratios 79.3 versus 9.3, 7.6 versus 2.0, 25.0 versus 3.0, and 18.0 versus 2.2, respectively. Impaired physical health and problematic medication use had equally strong associations with frailty in geriatricians and family physicians: odds ratios of 11.5 versus 10.4 and 2.4 versus 2.5, respectively.
Conclusions: Geriatricians more often judge patients as frail compared with family physicians and seem to evaluate the available information differently. With increasing collaboration between primary and secondary care, understanding these differences becomes increasingly relevant.
Family physicians (FPs) are facing an increasing number of frail older persons who are presenting their health problems.1 Hence, FPs try to find ways to improve care for their frail older patients.2 Therefore, they are in need of a valid and reliable method, first, for the identification of frail older patients and, second, to perform problem analysis and management of problems identified. One of the commonly used methods for evaluation and management of geriatric patients in hospital care is the Comprehensive Geriatric Assessment (CGA).3 A CGA determines an older person's medical, psychosocial, functional, and environmental resources and problems and results in an overall care plan. The introduction of CGA in primary care may have beneficial effects because it discloses hidden health problems and treatment needs.4 However, controversy exists over whether the introduction of CGA will be beneficial and cost-effective in primary care.5⇓⇓⇓⇓–10 Furthermore, implementation of CGA is hampered by time and financial constraints.8,11 Therefore, more efficient CGA tools are necessary for family practice, for which we developed a stepwise approach in which a short tool is used as a first step to select the patients who will really benefit from CGA.1,8,12,13
In general, CGA by a hospital geriatrician is used as the standard for validating new primary care frailty instruments. CGA is a valid instrument for the management of frail elderly in hospital care14; however, applying tools for CGA in other than the traditional hospital setting, probably means that their use, meaning, effectiveness, and output differ. Little is known about the differences between CGA by FPs and hospital geriatricians. These differences may arise at several levels. First, primary care and specialist CGAs differ in their content, methods, and intensity, with usually a more efficient approach being applied in primary care. Second, although geriatricians are specifically trained for treating frail elderly, FPs received generalist training for a broader population. Finally, the perspectives of FP and geriatrician differ, with the FP working in the community with larger, unselected groups of patients with usually lower disease prevalence and the geriatrician working with selected populations, often through referral based on the presence of symptoms and thus higher prior probabilities of disease and different risk profiles.15 Having both a generalistic and holistic approach to care, FP and geriatrician also have many similarities. On the balance, it is unclear how these differences and similarities influence CGA performance across FPs and hospital geriatricians.
We evaluated the differences and similarities between CGAs by FPs and hospital geriatricians, by comparing primary care CGA coordinated by an FP (FP-CGA) with specialist care CGA coordinated by a geriatrician (G-CGA).
Methods
Study Population and Design
Six FP practices in and around Nijmegen (the Netherlands) assessed their patients of 70 years and older between February 2010 and August 2011. These practices were situated in urban (n = 2), suburban (n = 1), and rural (n = 3) areas; 1159 older patients were assessed and asked to participate in the study. Patients who were too ill to be assessed were excluded. Patients were also excluded if they were under treatment of a geriatrician or if they had undergone a specialist care comprehensive geriatric assessment in the past 3 months because the information of the geriatrician might influence the frailty judgment of the FP. Informed consent was obtained from 587 older patients, and these were included in the study.
The study participants all underwent a FP-CGA by their own primary care team and a G-CGA by a hospital geriatrician and geriatric nurse. The primary care teams consisted of 12 different FPs and 12 different primary care nurses. All FPs were specifically trained as general practitioners in a 3-year training that follows a basic 6-year general medical training to become an MD in the Netherlands. Experience levels differed from some-to-many years of working in FP. After general nursing training, the nurses were trained as either community/district nurses or practice nurses. The G-CGA was performed by 4 hospital geriatricians (2 consultant physicians specialized in geriatric medicine with several years of working as geriatricians who supervised 2 registrars in geriatric medicine) who were assisted by 2 geriatric specialist nurses working in the outpatient clinic of the Radboud University Medical Center. The time between FP-CGA and G-CGA was a maximum of 4 weeks.
Measurements
Comprehensive Geriatric Assessment by an FP
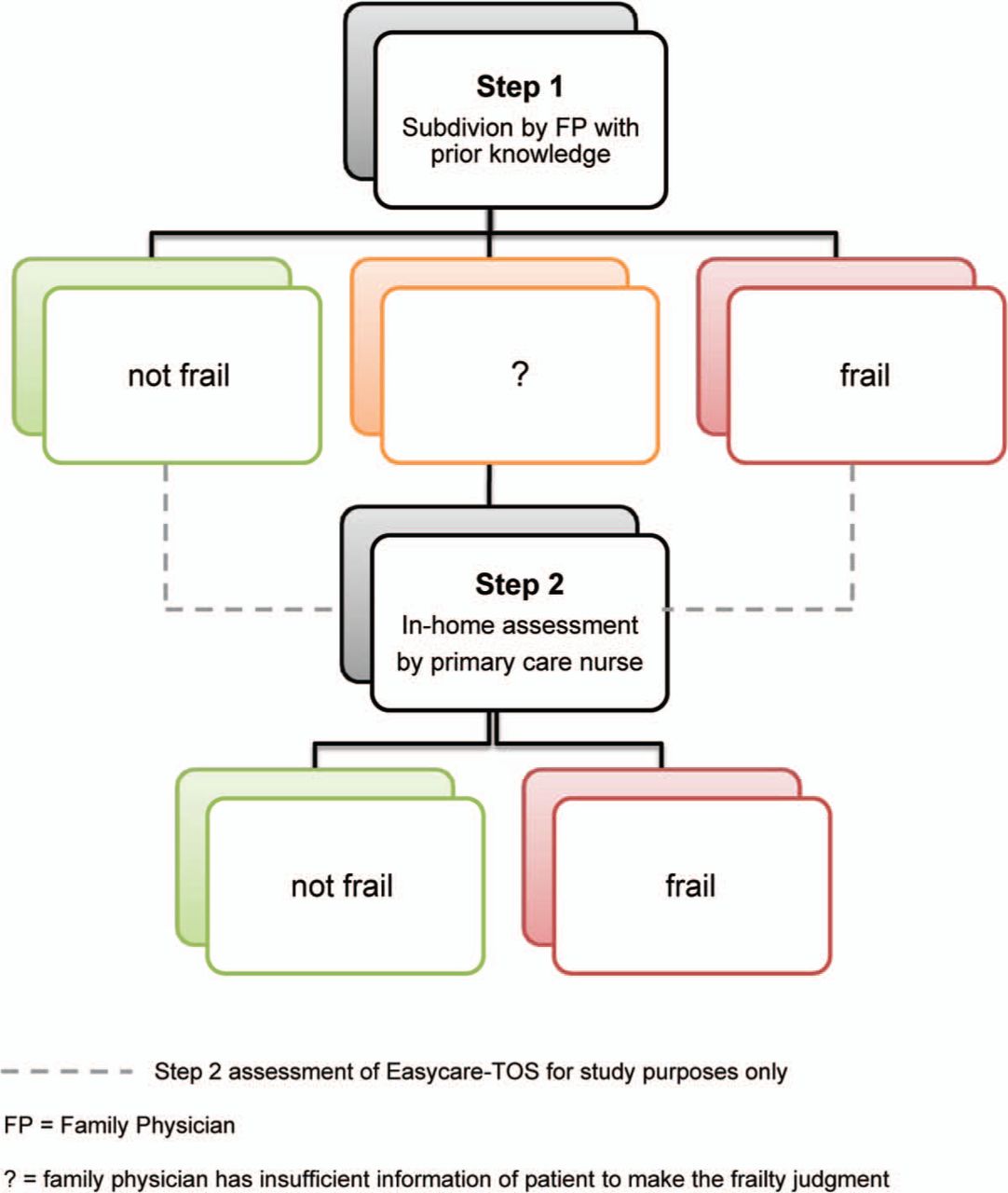
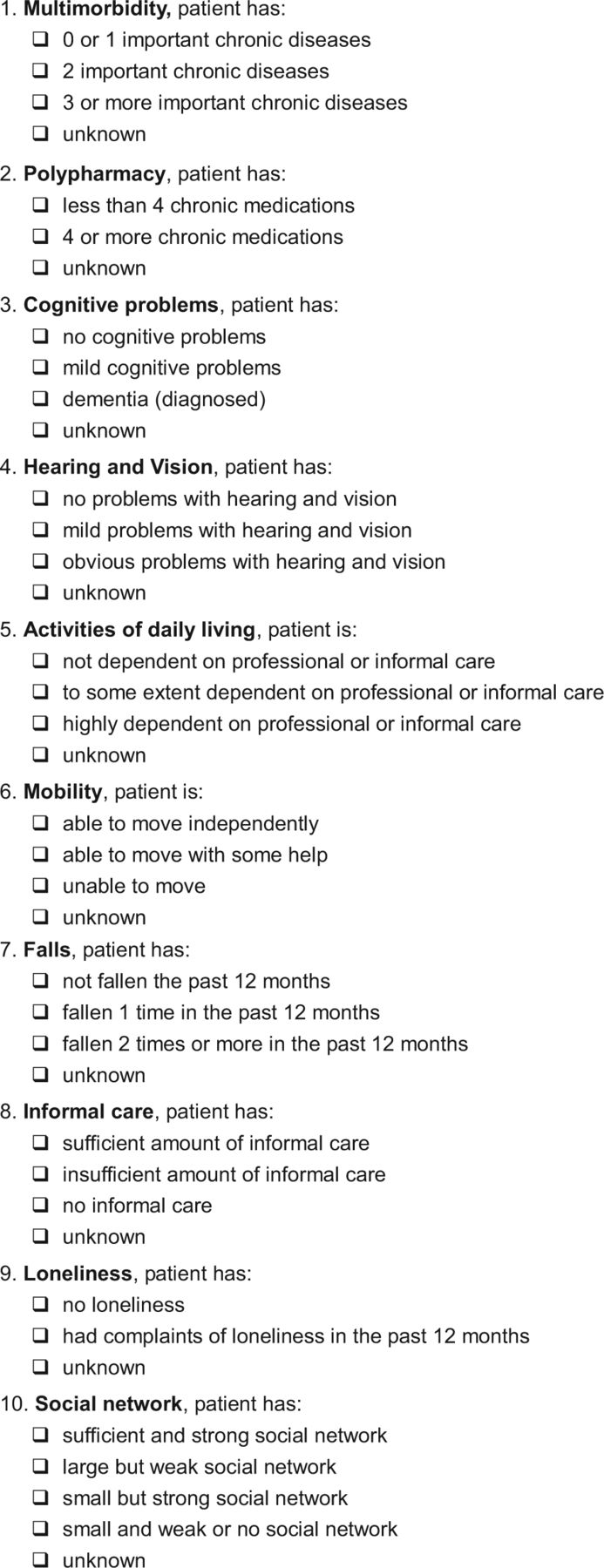
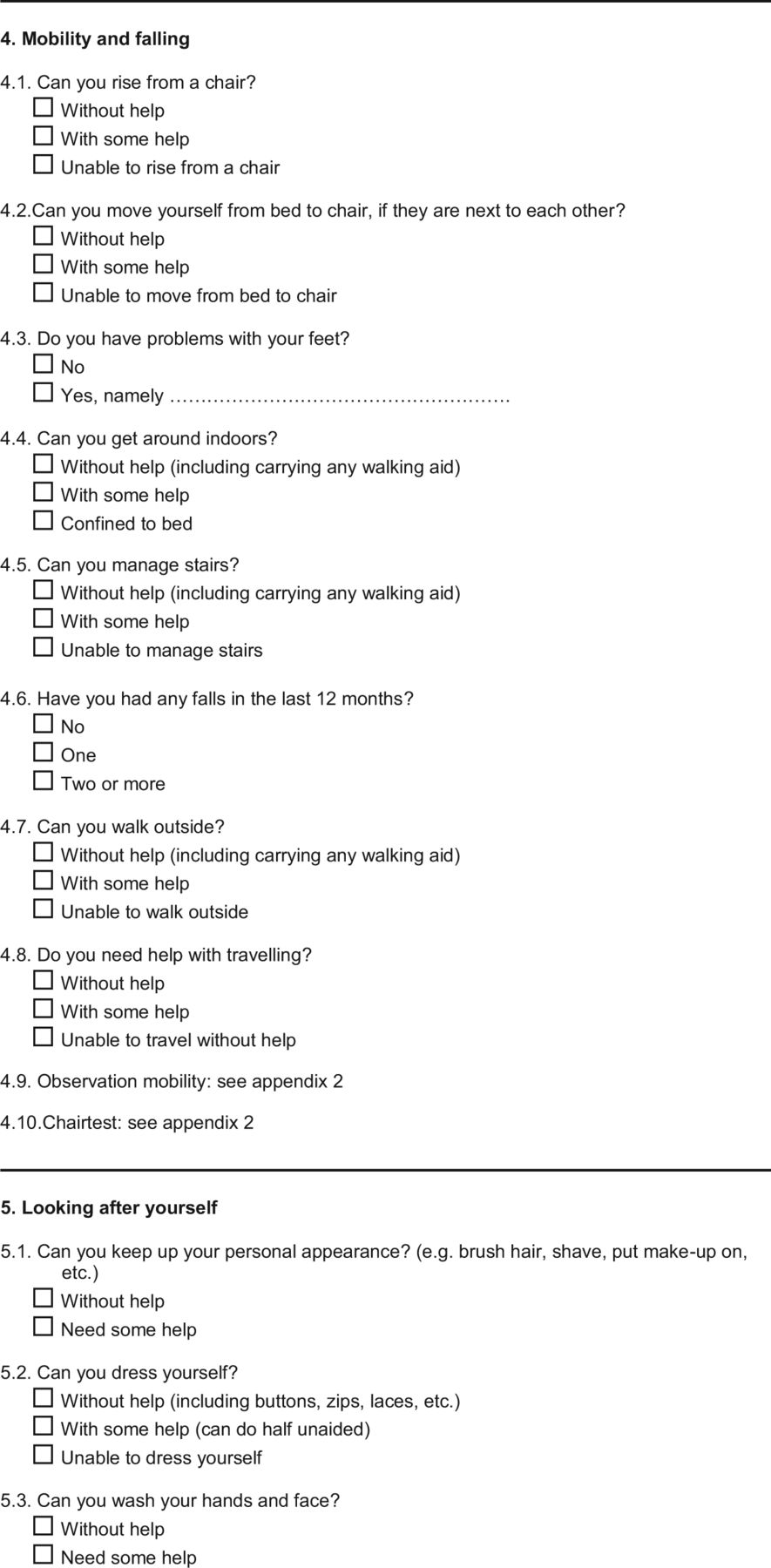
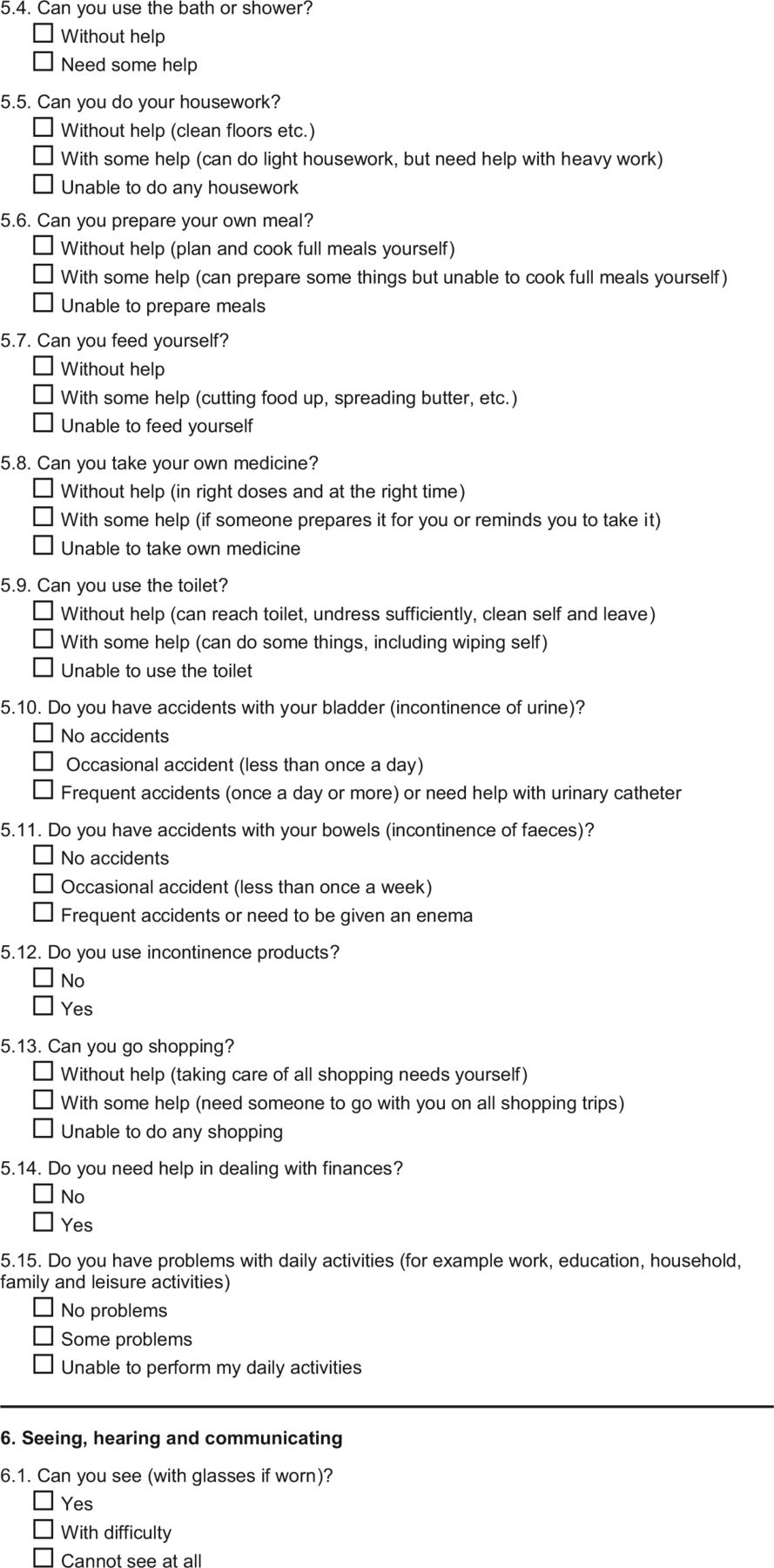
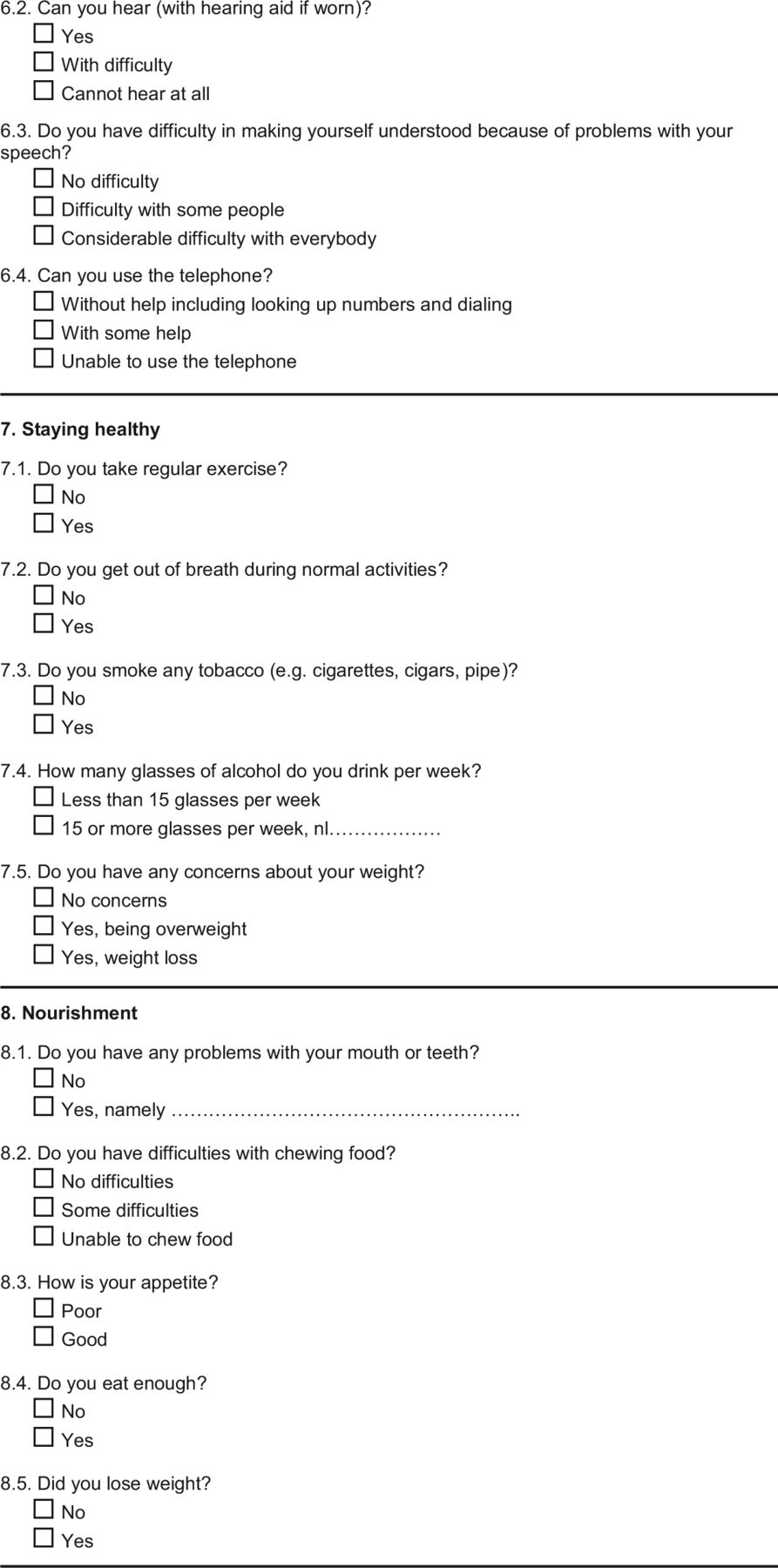
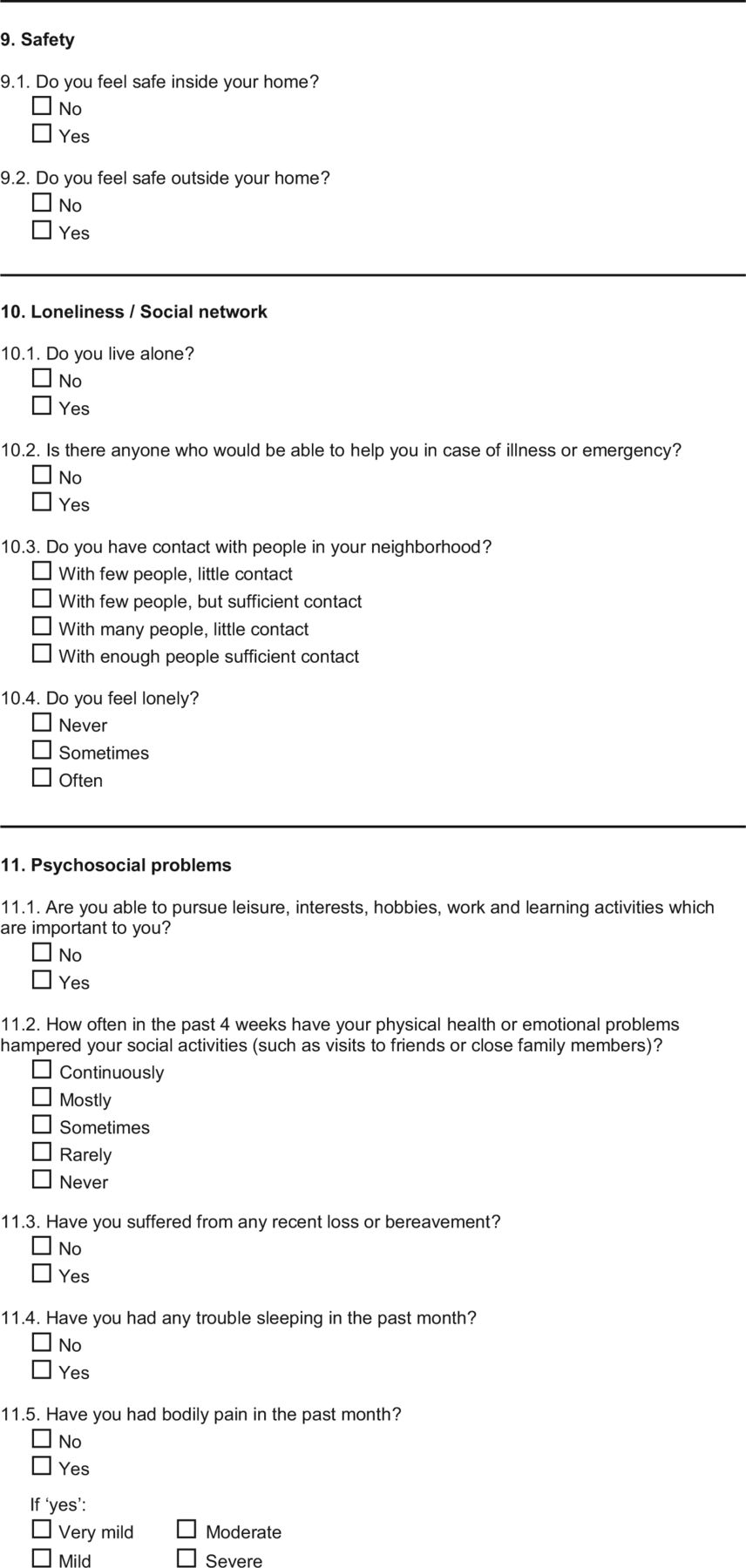
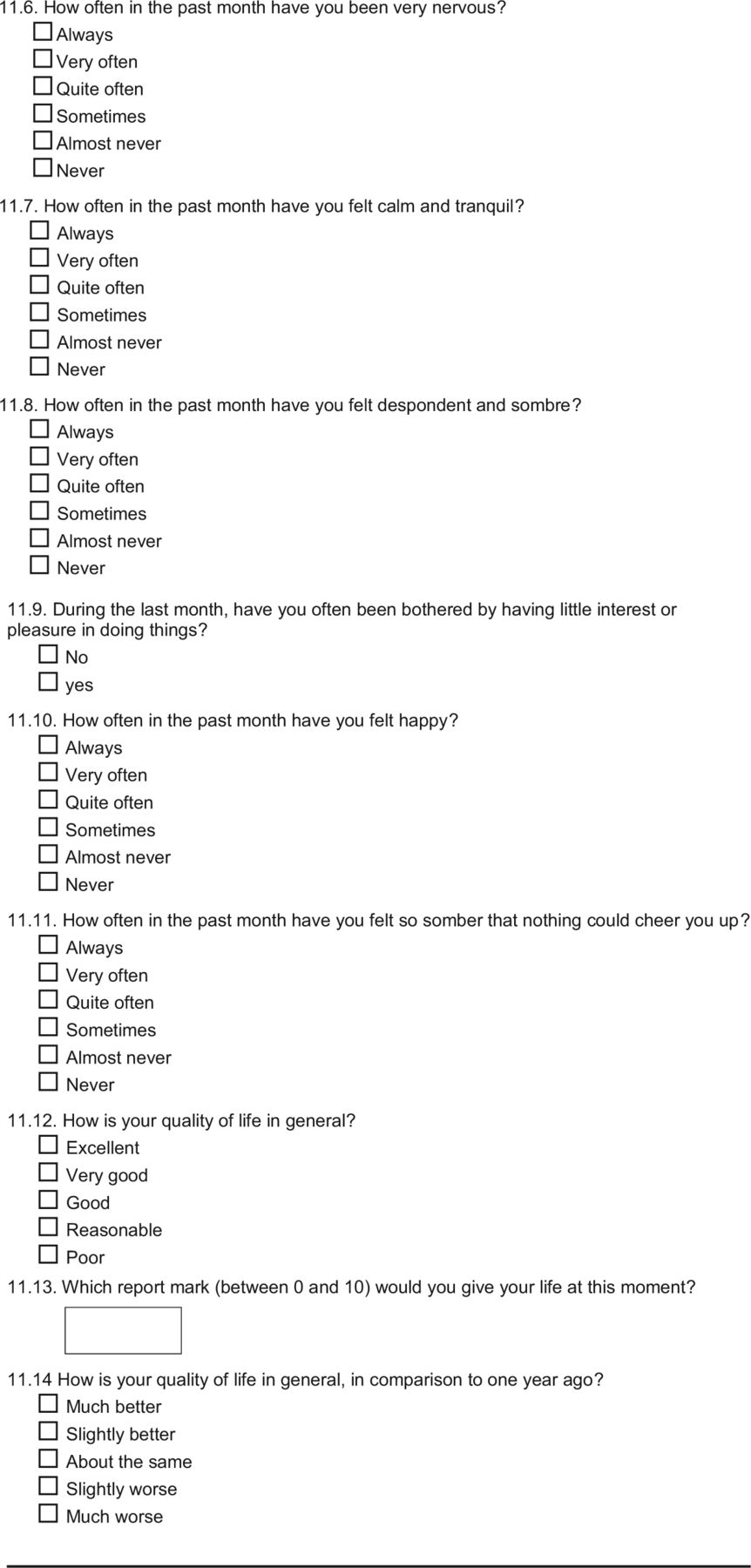
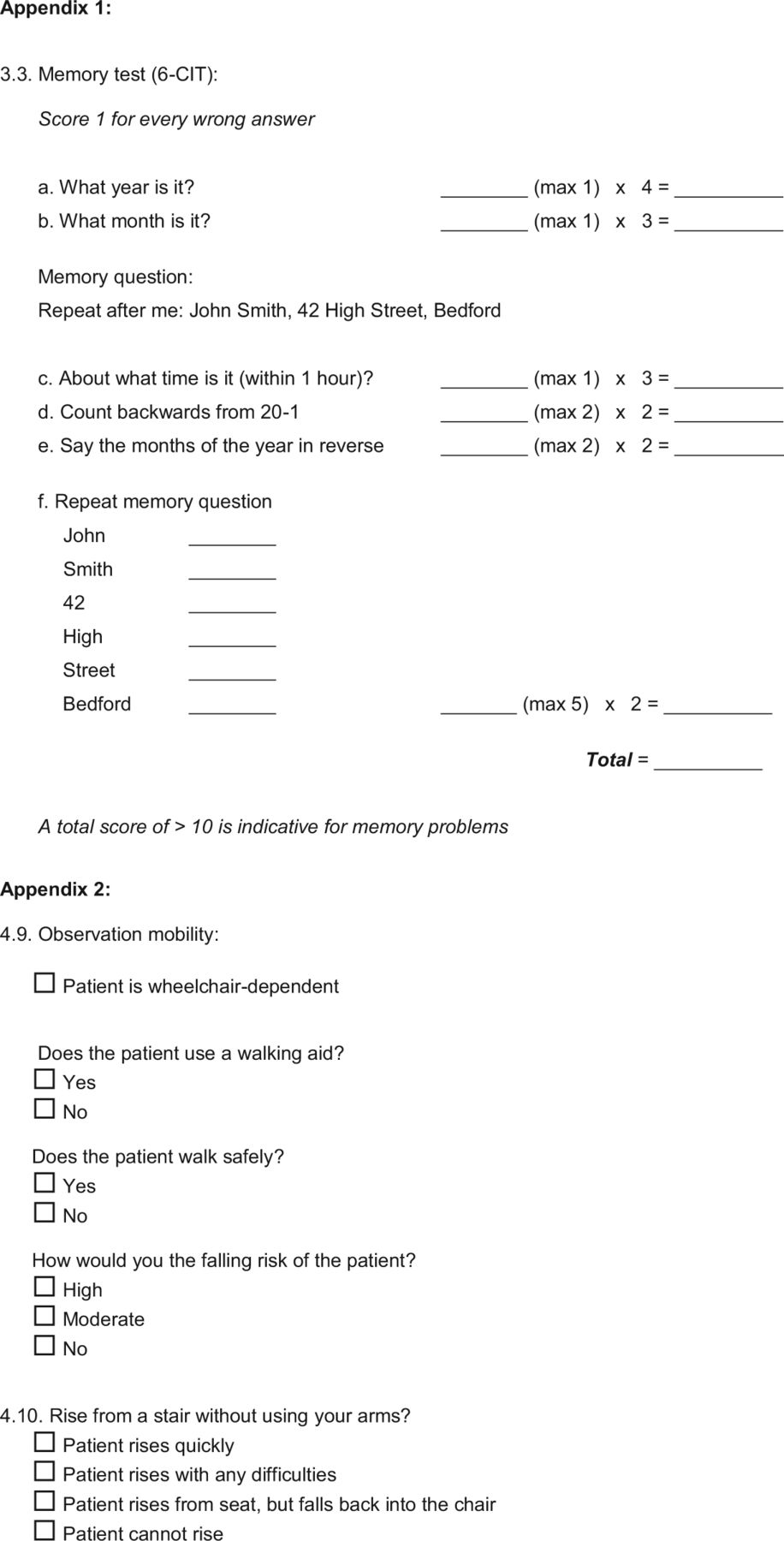
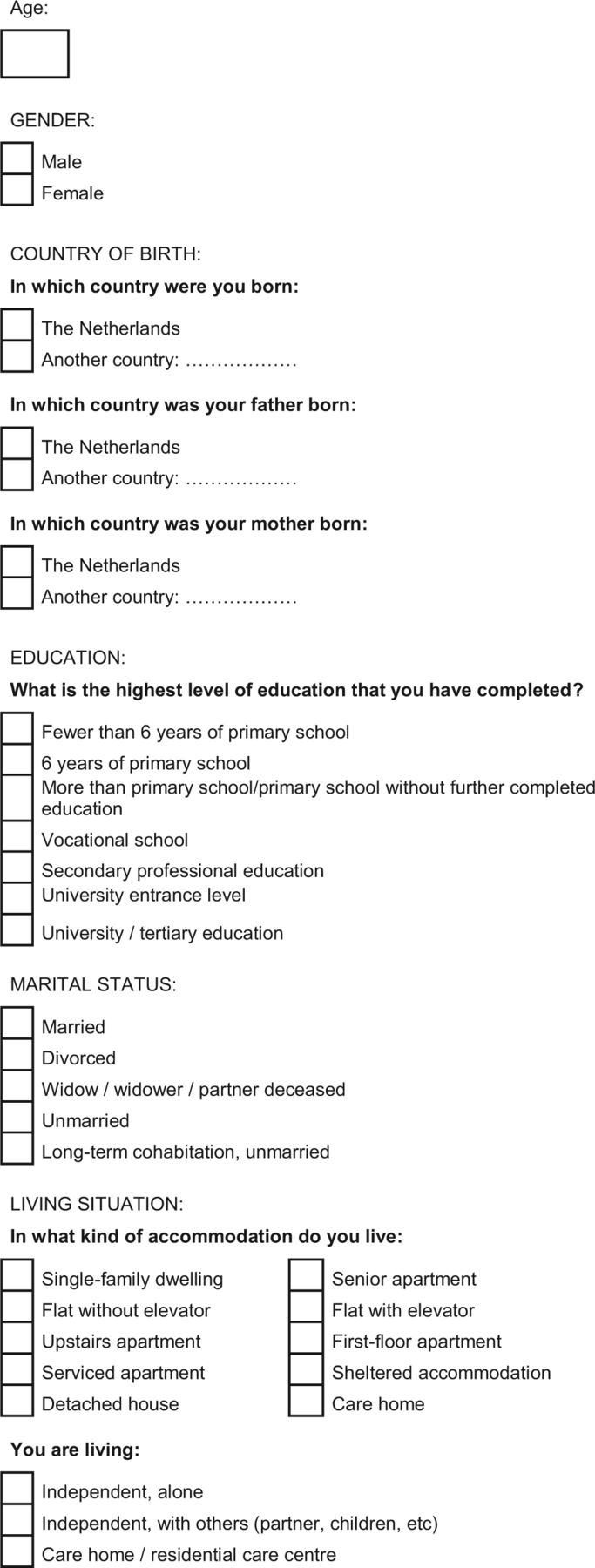
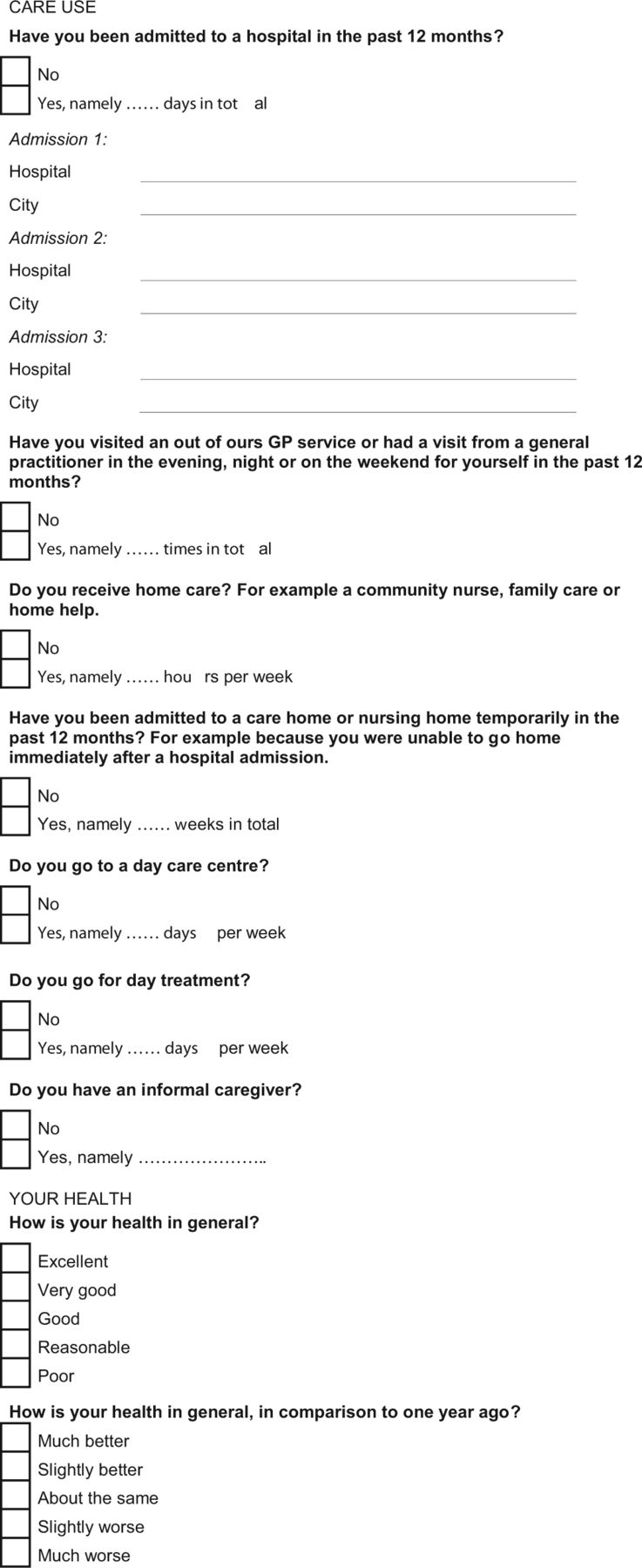
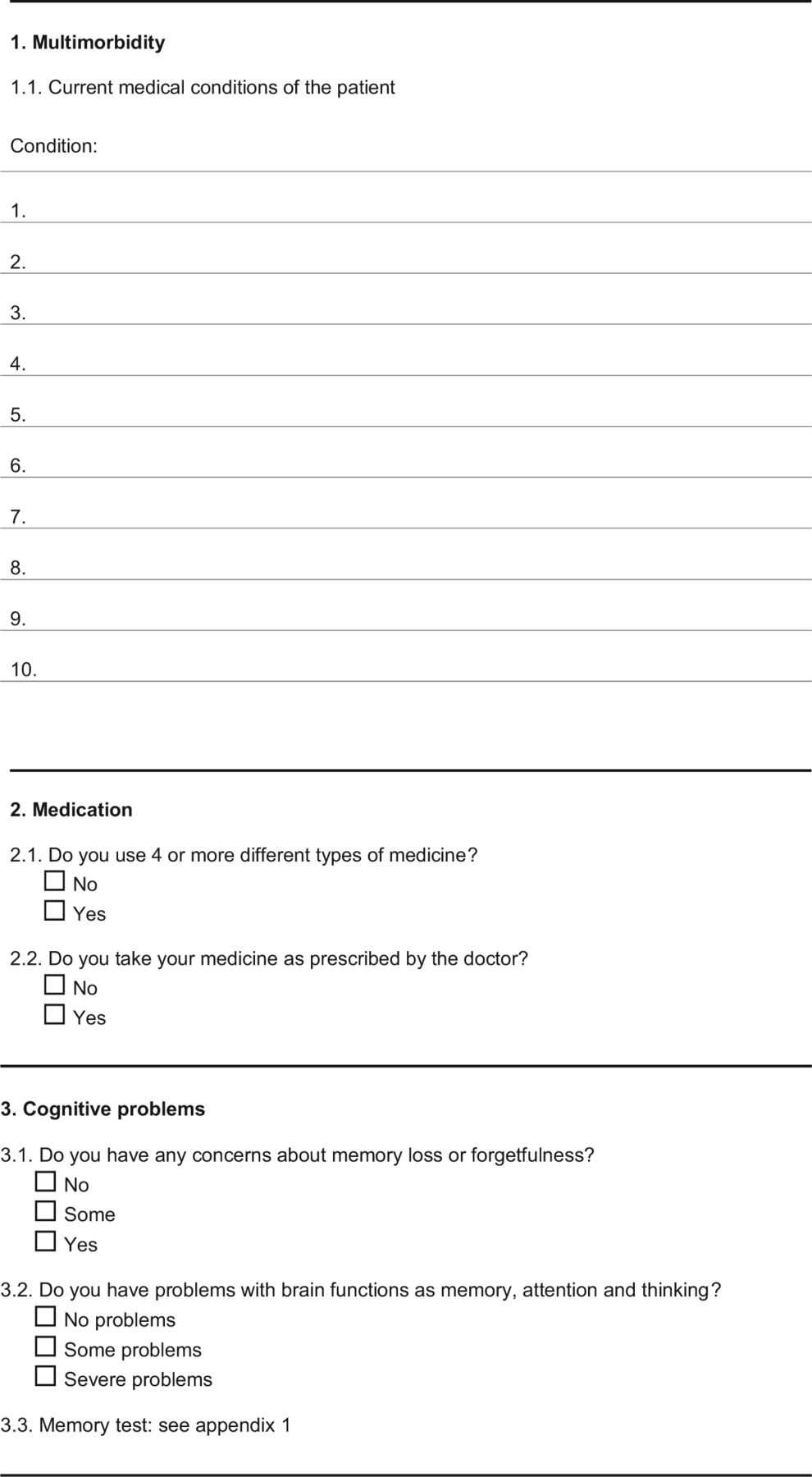
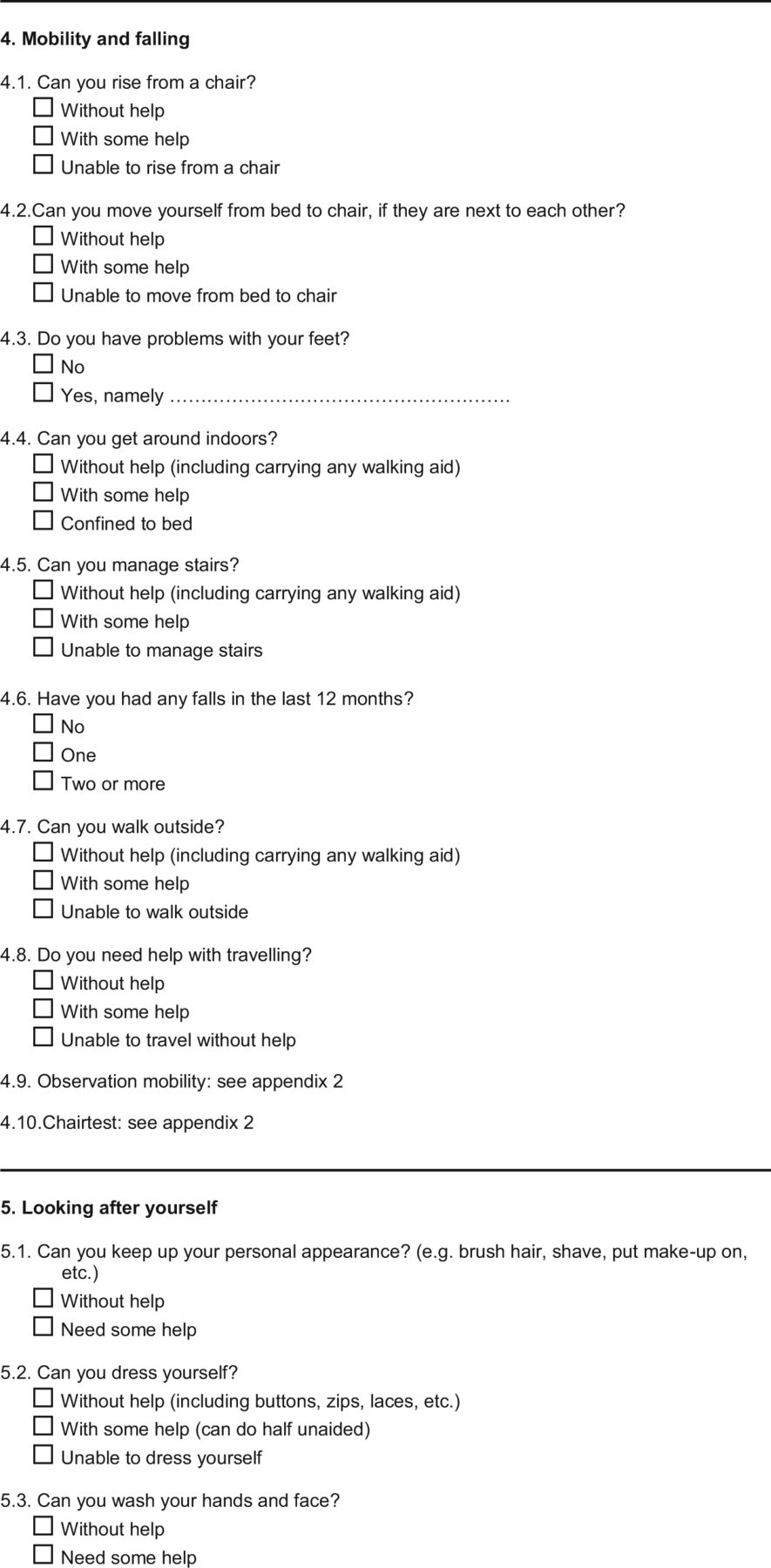
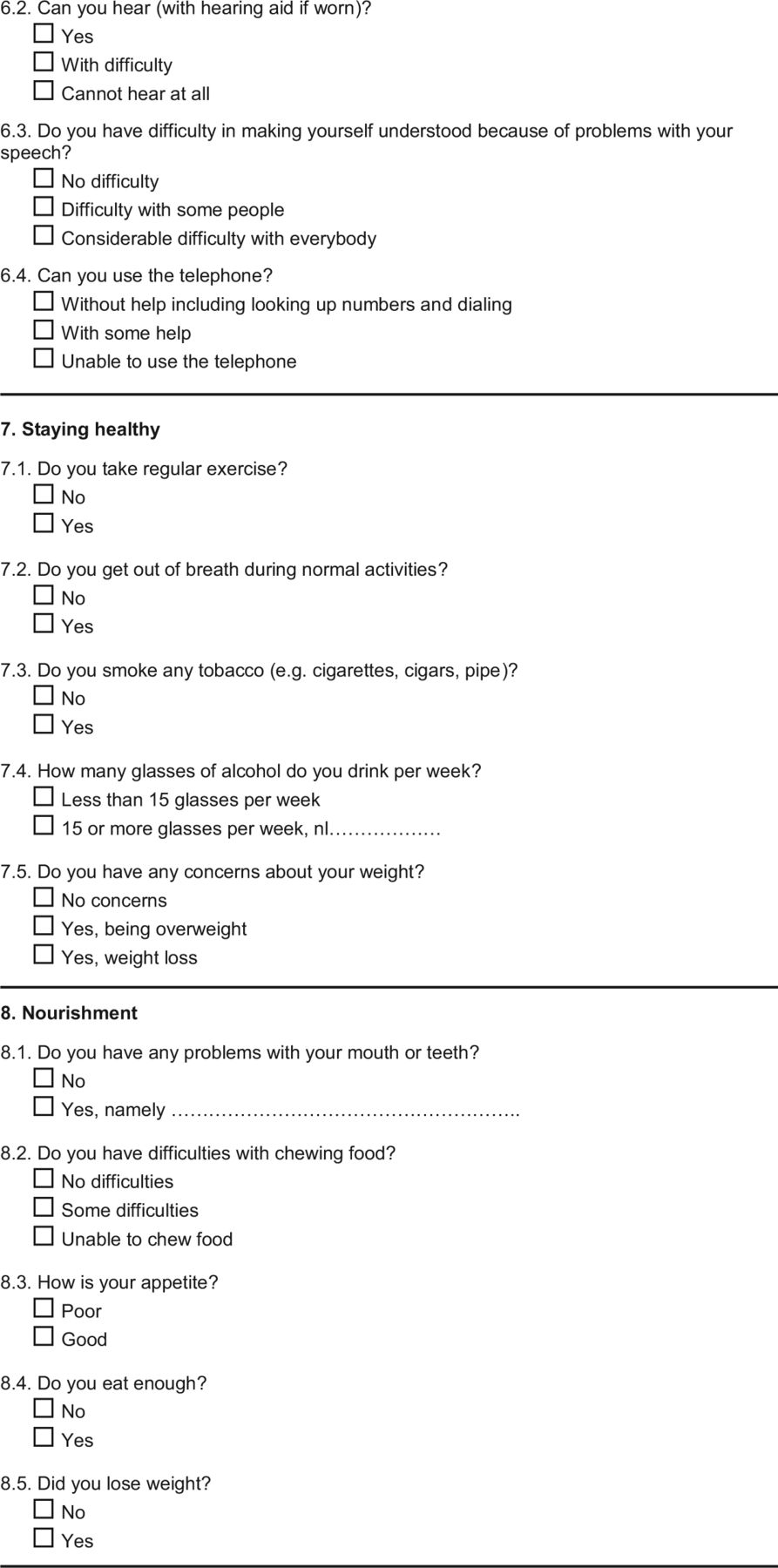
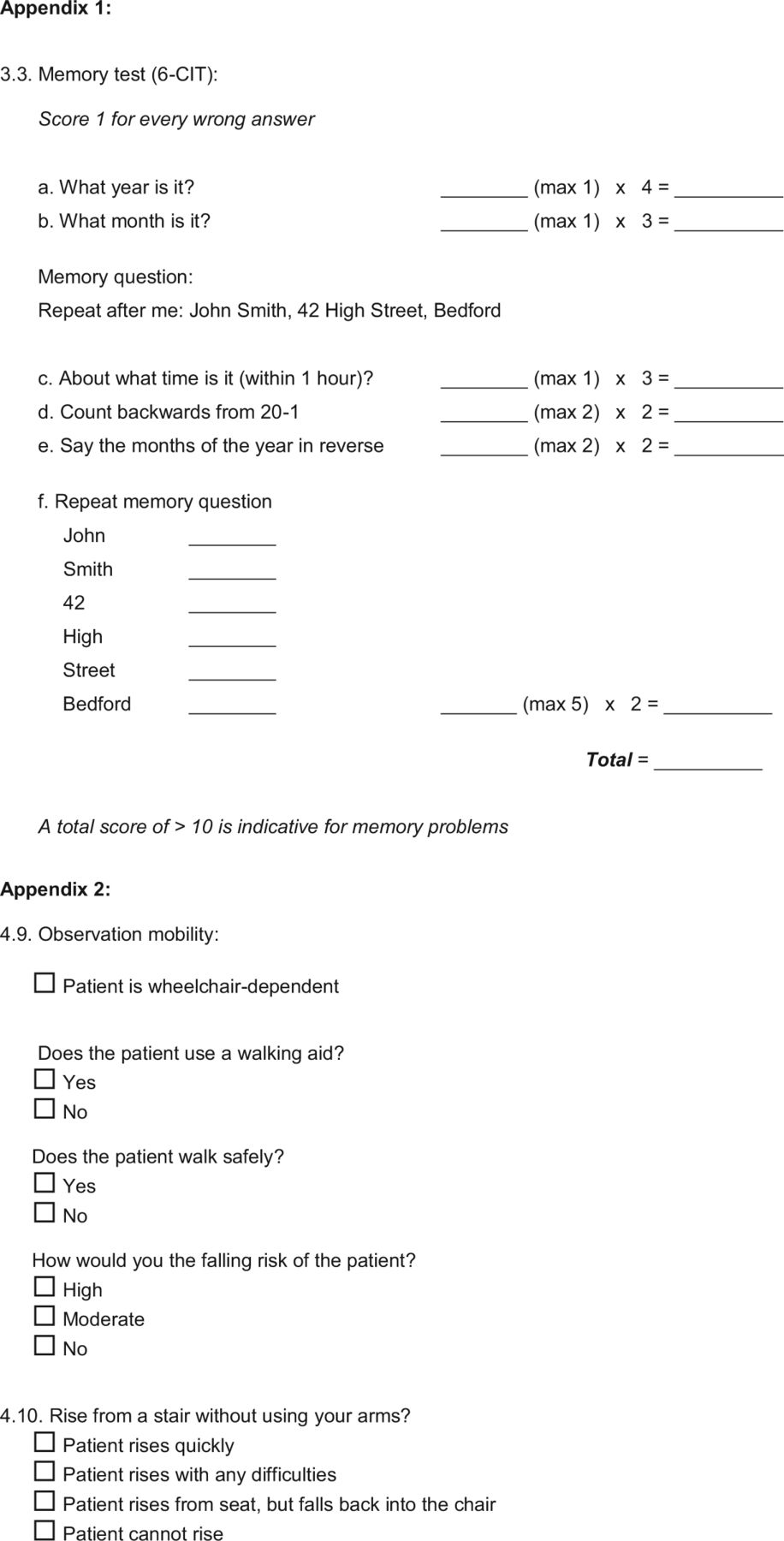
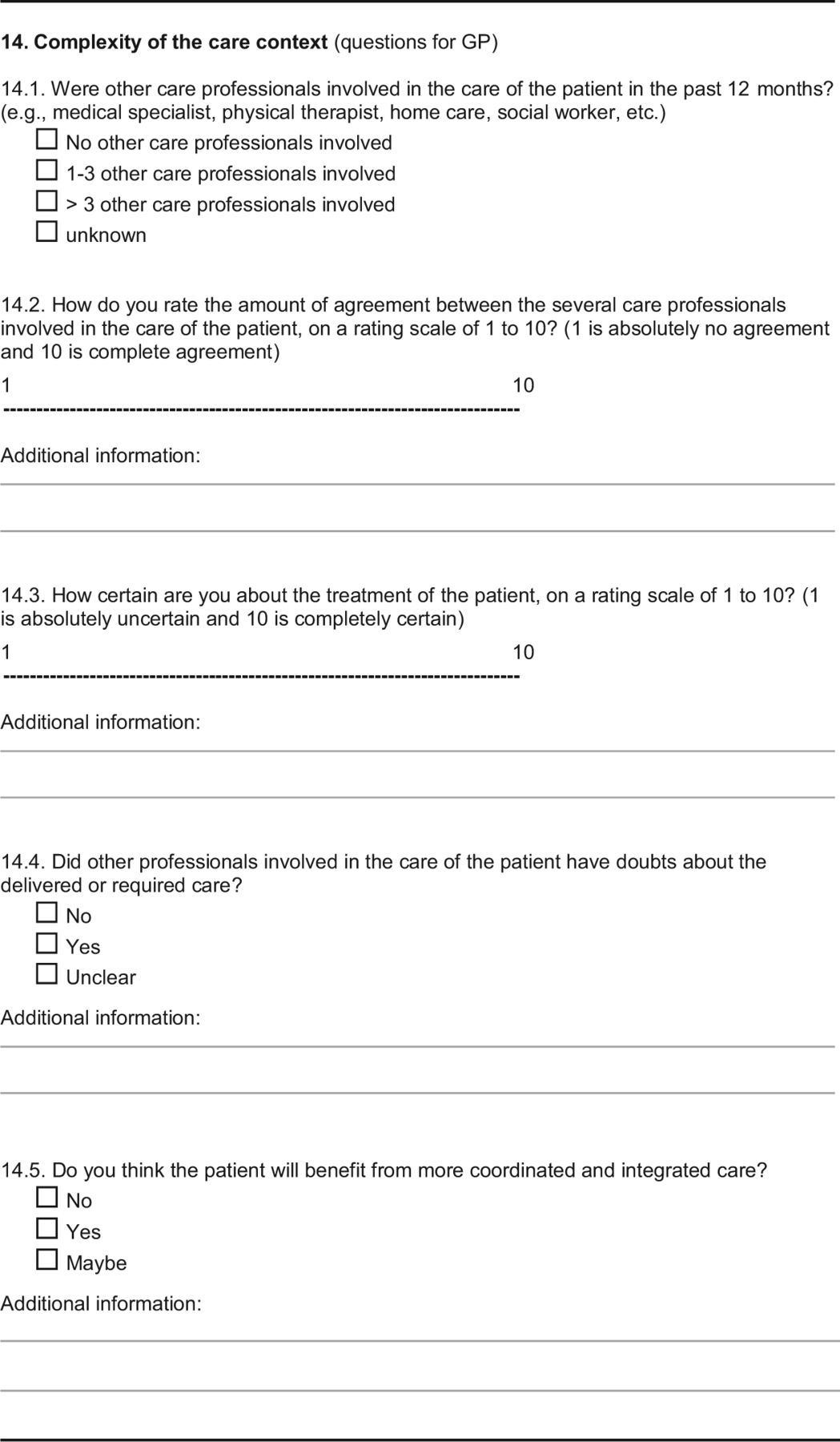
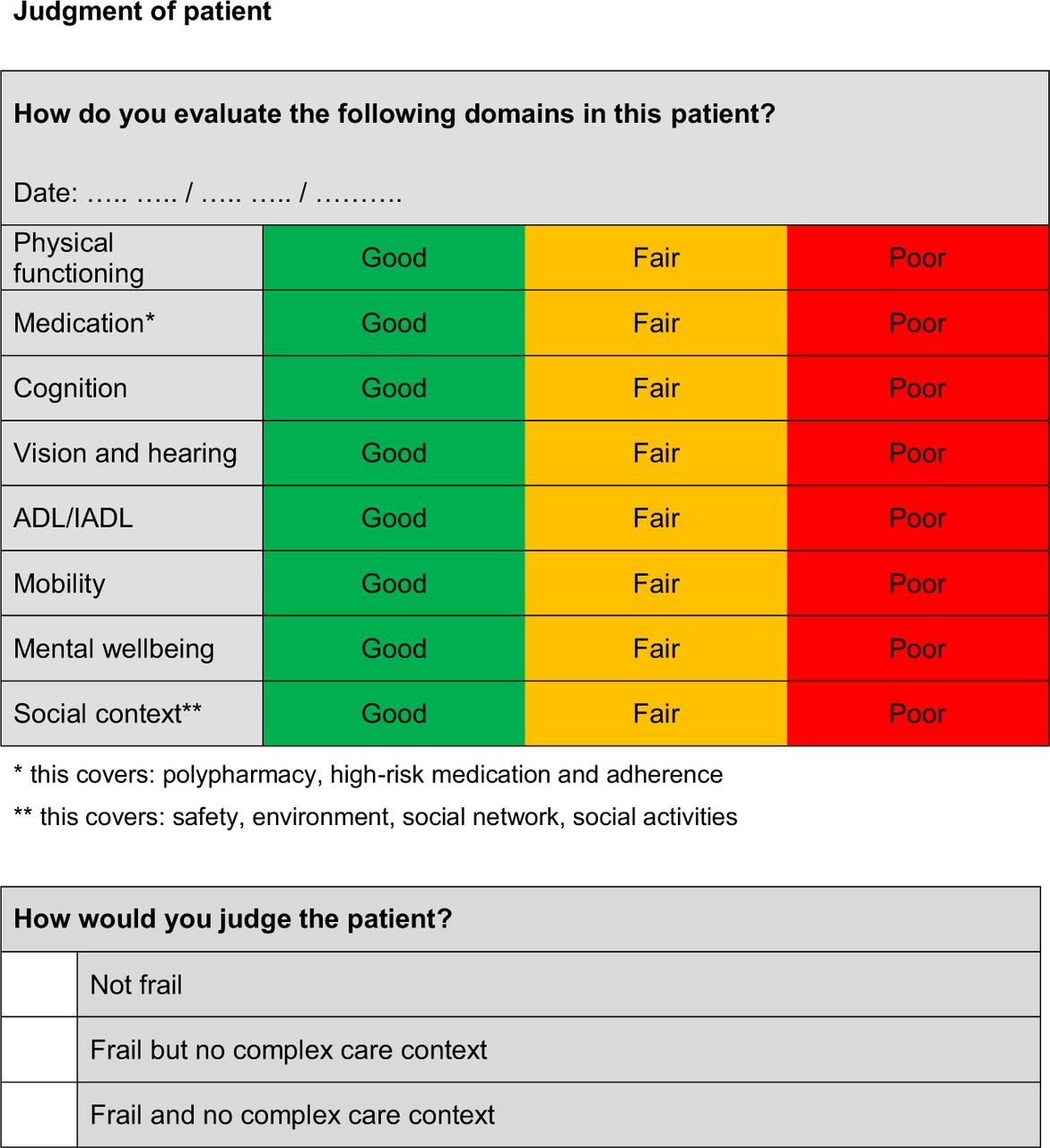
EASY-Care Two-step Older persons Screening (EASY-Care-TOS13; Online Appendix Figure 1) is a 2-step method developed for use in primary care. In the first step, the FP uses already available information, including clinical intuition and knowledge from the patient record, to complete a 14-item checklist (see Online Appendix Document 1). After completion, the FP decides whether the person is frail. This decision is mainly based on clinical reasoning not on a standardized score. If according to the FP, sufficient information is lacking to make the frailty judgment, the case is “unclear,” and the patient proceeds to the second step of EASY-Care-TOS. This comprises a home visit of approximately 1 hour by a primary care nurse, who assesses the person's functioning on physical, psychological, and social domains (see Online Appendix Document 1). After discussing the gathered information with the FP, the FP and nurse will judge the functioning of the person on 8 frailty domains (on a 3-point scale: good-fair-poor): 1) physical, 2) medication (number, use of high-risk medications, and adherence), 3) cognition, 4) sensory, 5) (instrumental) activities of daily living ([I]ADL), 6) mobility, 7) mental, and 8) social. Finally, an overall frailty judgment is made for every person.
For study purposes, all study participants underwent the second step of Easycare-TOS, irrespective of the frailty judgment of the first step.
Comprehensive Geriatric Assessment by Geriatrician
The participants underwent a geriatric assessment at the geriatric outpatient clinic of the Radboud University Medical Center. This assessment consisted of an interview and medical examination by a hospital geriatrician and an interview with the geriatric nurse and additional tests for cognition, mental wellbeing, physical functioning, (I)ADL functioning, and mobility (Cumulative Illness Rating Scale for Geriatrics,16 Mini Mental State Examination,17 Katz-15 (I)ADL scale,18 Short Physical Performance Battery,19 Geriatric Depression Scale,20,21 and Hospital Anxiety and Depression Scale-A22). After this assessment, the geriatrician and geriatric nurse discussed the frailty judgments. They also judged functioning of the patient on the same 8 frailty domains that were used in the FP-CGA and judged the overall frailty status of the patient. They were blinded for the results of the FP-CGA.
Statistics
We determined baseline characteristics of all participants, of the participants who were frail according to the FP, and of the participants who were frail according to the geriatrician.
We used cross tables to compare the frailty judgments (frail vs not frail: for FP the final evaluation after EASY-Care-TOS step 2) and the judgments (good, fair, poor) on the 8 domains between FPs and geriatricians. Next, we determined the proportion of overall agreement between FPs and geriatricians, and calculated Cohen κ. We used the interpretation of κ values of Landis and Koch.23 To further our understanding of the association between the FP and geriatrician frailty judgments in relation to the FPs' and geriatricians' evaluation of the performance on each of the 8 domains, we regressed the frailty judgments first on the profession of the evaluator (geriatrician vs FP) and second on their domain scores (fair/poor vs good) in a logistic mixed model (PROC GLIMMIX, SAS 9.2; SAS Institute, Cary, NC), taking into account the dependence at the participant level with the addition of a random intercept per participant. Because only few participants were rated as “poor” on the domains, we collapsed categories “fair”' and “poor”. In the same manner, we modeled the association between frailty judgments and the number of domains scored as “fair” or “poor” (range, 0–8). We evaluated whether domain scores and the number of domains rated as impaired were differently associated with frailty judgments by the addition of interaction terms between profession and domain scores and the number of domains impaired.
Results
Proportion of Overall Agreement on Frailty Judgments
Agreement on the overall frailty judgment was observed in 76% of patients (Cohen κ, 0.52) (Table 1). Patients were more often judged as frail by geriatricians than by FPs. According to the FPs, 213 (36%) patients were frail, against 294 (50%) according to the geriatricians. Overall physical and psychosocial functioning of patients who were frail according to the geriatrician was slightly better than functioning of the patients who were frail according to the FP (Table 2).
Agreement in Judgments on the Domains
On average, FPs scored fair or poor in 2.0 ± 2.3 standard deviation (SD) of the 8 domains per patient, compared with 3.1 ± 2.6 SD of the 8 domains per patient by geriatricians (Table 2).
Regarding the judgments on the 8 domains (Table 3), we found moderate agreement between FPs and geriatricians in the domains mobility (κ = 0.58), cognition (κ = 0.53), (I)ADL (κ = 0.49), mental (κ = 0.47), and social (κ = 0.42). The lowest agreement was found for the domains physical (κ = 0.36), medication (κ = 0.17), and sensory (κ = 0.29).
The judgments on the domains of the geriatrician were more often fair or poor compared with the judgments of the FP, except for the domains (I)ADL and social. The difference in judgment was most obvious in the domains physical and medication. Geriatricians considered the domain physical in 209 (36%) patients worse than the FP did. Thus, the geriatrician judged the domain as fair or poor and the FP, as good, or the geriatrician judged poor, and the FP, fair. For the domain medication, 260 (44%) patients were considered worse by the geriatrician compared with the FP.
We found complete lack of agreement (good vs poor) between FPs and geriatricians in 41 of 4695 domain judgments (0.9%). In 5 of these 41 judgments, the FP judged the patient's situation on the domain as poor, whereas the geriatrician judged it as good. In the other 36 judgments, the geriatrician judged the domain as poor, whereas the FP judged it as good. The majority of these (25 of 36) were related to the domain medication.
Characteristics of Participants with Concordant and Discordant Frailty Judgments
We divided our participants in 4 group: 2 concordance groups: frail and not frail according to both the FP and geriatrician (F+G+, and F−G−, respectively) and 2 discordance groups (frail according to the FP, not frail according to the geriatrician [F+, G−] and vice versa [F−, G+)]). Comparison of the characteristics of the participants in the 4 different groups (F−G−, F+G+, F−G+, F+G−) showed that the participants who were not frail according to the FP and geriatrician (F−G−) had the least functional problems on physical, mental, and social domains. The patients who were frail according to the FP and geriatrician (F+G+) had most functional problems. Functioning of the patients in the 2 groups without consensus (F−G+ and F+G−) was in between that of the 2 consensus groups (F−G− and F+G+) (see Online Appendix Table 1 for further details).
Does Discordance in Frailty Judgment Relate to Incongruent Evaluation of Domain Functioning?
In the patients who were frail according to the FP and not frail according to the geriatrician (F+G−, n = 30), the agreement on the domains was relatively high and ranged from 60.0% on the domain medication to 90.0% on the domain (I)ADL, with fair κ values (0.28–0.46); thus, incongruence in the evaluation of domain functioning could not immediately be hypothesized to explain the discordance in frailty judgment. In the other group without agreement, F−G+ (n = 111), we saw low agreement on the domains physical (31.5%, κ = 0.04), medication (43.6%, κ = 0.07), and sensory (49.5%, κ = 0.18) and better agreement on the other 5 domains. This finding suggests that perhaps incongruent judgments of the domains physical, medication, and sensory may play a role in the discordant frailty judgment. Online Appendix Table 2 shows the complete comparison of the judgments on the 8 domains of the 4 different groups (F−G−, F+G+, F−G+, F+G−). Generally, the proportion agreement and κ in domain functioning were better in the concordant than in the discordant groups. In agreement with the observation of a higher proportion of participants being judged frail by the geriatrician, regressing the frailty judgment on the profession of the evaluator in a logistic mixed model showed that the evaluator being a geriatrician (as opposed to being FP) had an odds ratio (OR) [95% CI] of 3.1 [2.2–4.4]. Simultaneously modeling the associations of the scores on the domains with the frailty judgments resulted in the following ORs for fair/poor versus good functioning: physical, 7.5 [4.4–12.9]; medication, 2.2 [1.4–3.4]; cognition, 16.9 [8.0–35.9]; sensory, 3.1 [2.0–4.7]; (I)ADL, 7.2 [2.7–18.9]; mobility, 6.8 [3.9–11.9]; mental, 4.9 [2.9–8.2]; and social, 3.8 [2.0–7.2]. One extra domain rated as impaired had an OR of 4.8 [3.7–6.1].
Table 4 shows that if geriatricians rated 1 extra domain as impaired, this was more strongly related to their frailty judgment than in FPs: ORs were 7.7 [5.1–11.5] and 3.8 [2.9–5.0], respectively (P value for interaction “profession*1 extra domain rated as impaired” <.001). The strength of the association (ORs) of separate domains with frailty judgment was comparable across FPs and geriatrician for the domains physical, medication, and social, but being rated as fair/poor had strengthened associations with frailty judgment in geriatricians for the domains cognition, sensory, mobility, and mental as indicated by P values for interaction. In the 2 models reported in Table 4, the independent effect of profession (geriatrician vs FP) had ORs of 0.09 [0.03–0.29] and 0.13 [0.05–0.36], respectively, suggesting that in participants being evaluated with good performance on frailty domains, there are a higher odds of FPs rating a person as frail than of the geriatrician rating a person as frail.
Discussion
In this report, we described how primary care CGA by FPs compared with a CGA by hospital geriatricians. We found 76% agreement between FPs and geriatricians on the overall frailty judgment. Geriatricians more often considered older patients frail than FPs did (50% vs 36%). In the evaluation of the 8 frailty domains, geriatricians more often scored fair or poor compared with the FP, particularly in the domains physical and medication. Complete discordant domain evaluations (good vs poor) were sparse, but discordant domain evaluation on the domains physical, medication, and sensory seemed to be associated with discordant frailty judgment, particularly in the group where the geriatrician rated a person as frail and the FP did not. Mixed multivariable analyses showed that an increasing number of domains rated as impaired related to an increased odds of being evaluated as frail. Typically strong associations with a positive frailty judgment had evaluations of impairment on the domains physical and cognition, but—perhaps with the exception of social—impairments on all domains were associated with frailty judgment. Geriatricians may rely more strongly on the (number of) domains affected in their frailty judgments than do FPs, specifically with impaired domain scores for cognition, sensory, mobility, and mental. FPs seemed more restrained in translating an impaired score on these domains into a positive frailty evaluation. Combining these observations suggests that discordance in frailty judgment may be driven partly by geriatricians being more liberal in evaluating physical health and medication use of participants as problematic and partly by geriatricians more easily than FPs translating the presence of impaired functioning on other domains into a positive frailty judgment. However, if present, FPs' and geriatricians' evaluations of physical and medication had equally strong associations with frailty judgment. Therefore, this cannot explain the discordant frailty judgments.
Striking is the low agreement between the judgments of FPs and geriatricians on the domains physical and medication. If one assumes that both FPs and geriatricians had the same information on the physical health and medications of patients, there must be a difference in what the different professionals take into account in the judgments. We expect that the FPs relate the severity of physical health impairment to other information of functioning of the patient in daily life as well. The geriatricians, on the other hand, may be making the judgment on the basis of the absence or presence of disease only. Evidence for a different approach to evaluating the absence and presence of frailty and its related domains by FPs and geriatricians is also provided by the observation that if no domains were rated as problematic, FPs actually seemed more inclined to rate a person as frail than the geriatricians. Although this rating may be counterintuitive at first, it may offer evidence that FPs use “outside” information—not part of the CGA itself and not showing up in impaired domain ratings—when rating a person's frailty. Moreover, the differences found can partly be explained by differences in the care setting and target population. First, the FP's assessment included an in-home assessment by a nurse, whereas the geriatrician's assessment did not. Second, the FP would be likely to have had a longer term understanding of the patient. Third, the FP worked with ambulatory patients and the geriatrician was hospital-based.
In general, both geriatricians and FPs identify frailty in patients as a marker for the patients who have a higher risk of negative outcomes, but the risk profiles of their patient groups as well as the actual risks these patients face are different in different care settings. Geriatricians generally see patients with a higher a priori chance of diseases who receive more stressful interventions (in hospital) such as surgery. Therefore, they may judge patients with a lower threshold for frailty, in order not to miss anyone. FPs, as coordinators of care, have more prior knowledge of total functioning and the context of the patient. This enables them to make a more accurate judgment of functioning of the patient.24 Hjortdahl25 found that prior knowledge of the patients plays an important role in the clinical decision-making process of FPs. In addition, being used to working with low-risk populations, they are trained to act and judge with more restraint.
Despite these issues being closely linked to the classic work on the ecology of medical care,15 we could find few further empiric reports on this subject to substantiate these assumptions. Kvamme et al26 already showed that knowledge on the differences in decision-making between primary and secondary care is important. They stated that a shared approach seems to be essential for good collaboration and communication. The differences in frailty judgment between FPs and geriatricians found in this report may influence communication and collaboration. Further studies are needed to unravel the differences in (frailty) decision-making between FPs and hospital geriatricians.
This study has some limitations. First, it was performed in a small setting (1 geriatric clinic and 6 FP practices) in the Netherlands, which is a country with a different health care system from, for example, the United States. This may cause generalizability issues. However, the group of participating patients was relatively large. Second, we do not exactly know how FPs and geriatricians made the frailty judgment. How did they weigh the collected information? Did they use information that was not reported? We tried to reveal this information using the quantitative data. However, supplementing qualitative data could have elicited these underlying questions.
In an era in which cross-sector collaboration is ever more important, this is one of a very small number of reports providing some empiric insight into the differences in health care professionals' evaluations of clinical constructs such as risk, function, and disease across different care settings: We call it the same, we implicitly assume we mean the same, but, in fact, we may be speaking about very different things. As an example of this, the relevance of this study into CGA carries beyond geriatric care alone. Because the concept of frailty is increasingly used in both primary care and hospital settings, it is important to realize that these differences in frailty judgment have implications for the communication about frailty between FPs and hospital geriatricians. As is generally accepted for other diagnostic instruments, diagnoses, such as the frailty assessment, have different properties depending on the population and the professionals involved. This 2-stage frailty judgment may be useful and valid in both care settings, but the important question arises whether these differences in frailty judgment are sufficiently taken into account in collaboration between primary and secondary elderly care.
Acknowledgments
The authors thank Hanny Hordijk, Leny Theunisse, Marlies Hoogsteen, Brechtje Lubberink, and Sarah Robben for their help with the data collection.
Appendix








Notes
This article was externally peer reviewed.
Funding: This project was funded by grant 60-61900-98-217 of the Dutch National Care for the Elderly Program, coordinated and sponsored by ZonMw, the Netherlands, organization for health research and development.
Conflict of interest: none declared.
- Received for publication March 3, 2013.
- Revision received November 16, 2014.
- Accepted for publication December 1, 2014.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}