
Abstract
There is often a rich but untold history of events that occur and relationships that form before a practice-based research network (PBRN) is launched. This is particularly the case in PBRNs that are community based and comprise partnerships outside of the health care system. In this article we summarize an organizational “prenatal history” before the birth of a PBRN devoted to people with developmental disabilities. Using a case study approach, this article describes the historic events that preceded and fostered the evolution of this PBRN and contrasts how the processes leading to the creation of this multistakeholder, community-based PBRN differ from those of typical academic/clinical practice PBRNs. We propose potential advantages and complexities inherent to this newest iteration of PBRNs.
- Community-Based Participatory Research
- Developmental Disabilities
- Populations
- Underserved
- Practice-based Research
Since their beginnings in the 1970s, practice-based research networks (PBRNs) in the United States often have been formed by state and national academies of family medicine and by medical school and residency primary care faculty in collaboration with community practices at local, regional, and national levels.1 This article describes an alternative pathway to PBRN development in which the network is formed by multiple stakeholder groups who are invested in the care of a target patient population, including nonclinician stakeholders involved in service, advocacy, and education. The pathway described here may serve as a template for the development of community-engaged PBRNs.
A Historic Context to Health Care and People with Developmental Disabilities
Developmental disabilities (DDs) are defined by federal law as severe chronic disabilities manifesting before age 22 due to a physical and/or mental impairment and resulting in “substantial functional limitations in 3 or more of the following areas of life activity: (1) self-care; (2) receptive and expressive language; (3) learning; (4) mobility; (5) self-direction; (6) capacity for independent living; and (7) economic self –sufficiency.”2 Population estimates for DDs in the United States vary between 1.5% and 2.5%.3 Most people with DDs live in the community, most commonly with family members, with additional support from educational, vocational, and social service programs.4
An emerging literature base is documenting widespread disparities in the health and health care of people with DDs, including both preventive and chronic disease care.5⇓–7 While some individuals with DDs have complex specialty health care needs that assume much of their health care activity, all are in need of primary care. Unfortunately, many primary care physicians report little formal training in the care of this population.8⇓–10
Critical historic events involving the medical community, as well as prevailing societal attitudes, feed a persisting distrust of the health care system by people in the DD community. In the past, physicians routinely advised families to institutionalize children with DDs to avoid “harming” their other children; inaccurate and pessimistic prognoses regarding the health, function, and life expectancy of children with DD were typical.11Unauthorized research conducted on people with DDs ranged from experimental exposure to radioactive substances in food to purposeful infection with viral hepatitis.12⇓⇓⇓–16 Even now, health care professionals counseling expectant parents about prenatal diagnoses of Down syndrome and other genetic conditions tend to present biased views regarding the typical functional status and “quality of life” of children with these conditions, with the assumption that all parents would elect to terminate the pregnancy given the “proper” information.17⇓–19
Health care providers often are unfamiliar with the complexities of their local DD service system, which may or may not include a widely variable and ever-changing range of health, vocational, educational, and residential services provided by county boards of DD, profit and not-for-profit residential service providers, and community-based agencies. Not surprisingly, health care providers make clinically unsupported assumptions about the extent of training and intensity of supports their medically fragile patients with DD receive from community service providers.20,21 Without a proper understanding of the DD service system, even well-intentioned, carefully crafted health care plans are unlikely to yield expected results.
Evolution of the DD-PBRN
The DD-PBRN is a multistakeholder, community-based PBRN established in 2013 with the support of the PBRN Shared Resource at Case Western Reserve University through the National Institutes of Health–funded Cleveland Clinical and Translational Science Collaborative (Figure 1). The mission of the DD-PBRN is to “improve the health and health care of persons with developmental disabilities throughout the lifespan through inquiry and action involving collaborations among the health care, service and disabilities communities.”
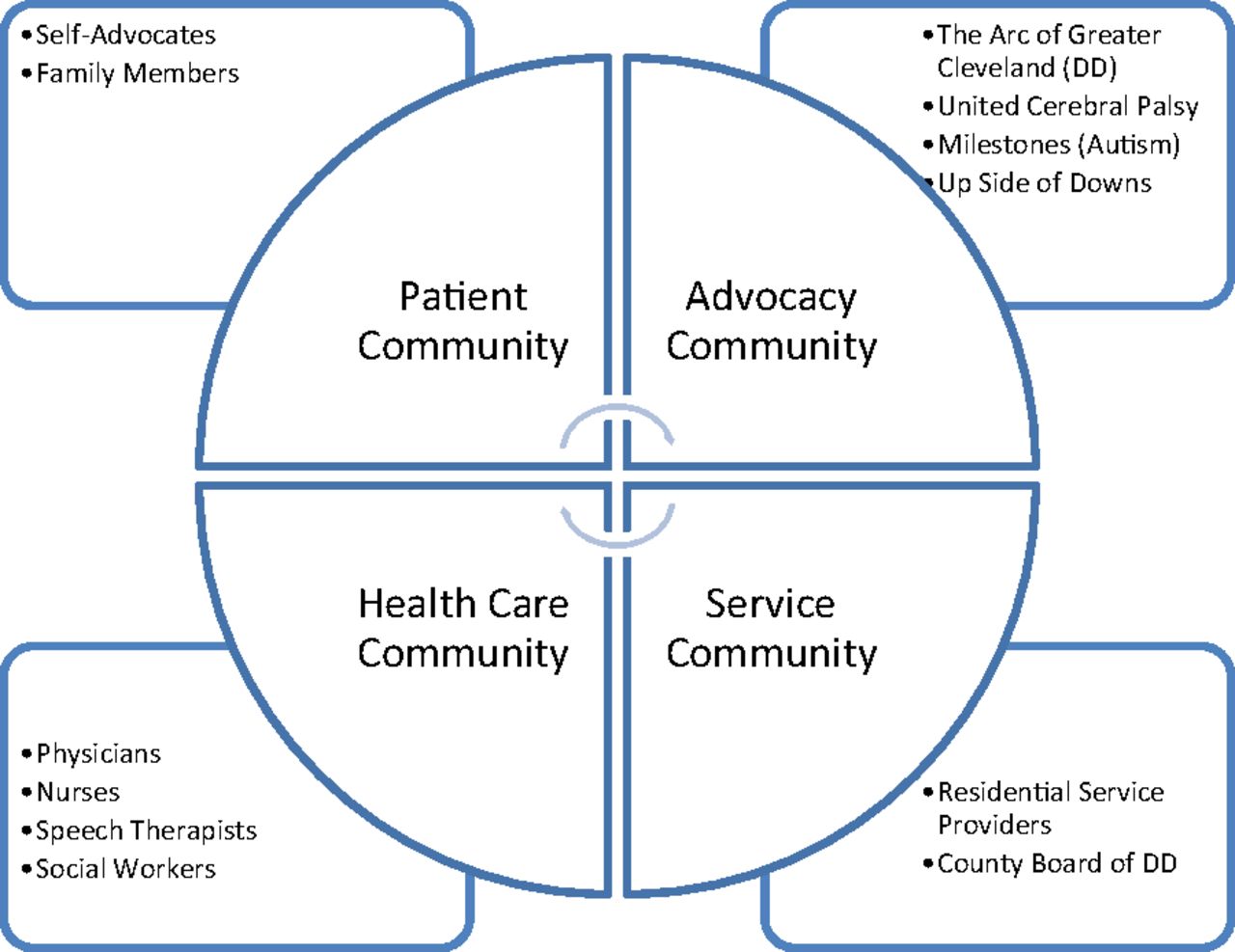
Stakeholders represented in the Developmental Disabilities (DD) Practice-Based Research Network.
Acknowledging this overall historic context, the “prenatal history” of the DD-PBRN can be conceptualized in 3 stepwise phases: (1) affiliation through shared service; (2) emerging mission of advocacy and clinical education; and, finally, (3) expanding the mission to health system change and research. The organizational history and framework presented below were derived from reviews of meeting notes, academic presentations and products, and E-mail communications related to collaborative activities. Drafts of this organizational history were reviewed by participants to ensure their accuracy. A timeline of collaborative activities leading to the establishment of the DD-PBRN are summarized in Table 1. This timeline illustrates the consistent structural core of participating membership, representing the patient, advocacy, service, and health care communities throughout the entire prenatal history of the DD-PBRN.
Phase 1: Affiliation Through Shared Service
Individuals (and their affiliate organizations) who would ultimately establish the DD-PBRN first became acquainted with each other through service provision to shared clients/patients residing within a metropolitan area of northeastern Ohio; the area's total population of nearly 2.1 million residents includes an estimated 30,000 individuals with DD, of whom approximately 13,000 are served by the Cuyahoga County Board of Developmental Disabilities. Over the course of years, members of the disabilities and service communities slowly developed trusting relationships with a small cadre of physicians who demonstrated expertise and commitment to this population. Mutual respect and understanding further developed between members of these 3 communities through collaborative management of complex client situations in which extensive communication and problem-solving between groups were required. Examples of client scenarios requiring high-intensity communication and collaboration included sexual abuse by a neighborhood predator, poor diabetes self-care jeopardizing community residence, recurrent hospitalizations for heart failure, and behavioral health issues.
Phase 2: An Emerging Mission of Advocacy and Clinical Education
A pivotal turning point that shaped the organizational vision for future PBRN members occurred in the context of a Family Medicine Education Consortium conference held locally in 2000. A family medicine residency faculty with a clinical focus in DDs (and the future director of the DD-PBRN) organized a full-day preconference dedicated to primary care and DDs. Most of the presentations were given by invited members of the disabilities and service communities rather than physicians. The presenters included self-advocates, parents, representatives of advocacy organizations, and nonphysician disabilities professionals. In addition to the presenters, the audience comprised approximately 25 family medicine residency faculty, family medicine resident physicians, and medical students from the northeastern United States. For the next decade, the Family Medicine Education Consortium maintained this precedent by hosting an annual full-day preconference devoted to primary care and DDs, with continued participation by members of the disabilities and service communities. Consequently, self-advocates, family members, and service providers began to see a role for themselves as vitally important educators of physicians. Many became involved in ongoing training of resident physicians at their local family medicine residency training programs. They recognized that the education of health professionals was a concrete means of ensuring and advocating for better health care.
In 2008 the Ohio Developmental Disabilities Council called for training grant proposals aiming at improving the primary care of adults with DDS. In response, the future DD-PBRN director gathered representatives of 2 residential service provider organizations (Help Foundation and Welcome House) and a local chapter of a national DD advocacy organization (The Arc of Greater Cleveland) to craft a submission. Previously established relationships between these stakeholder communities allowed the grant proposal to be written within 6 weeks. This group was awarded a 3-year training grant that provided the future PBRN members an opportunity to create enduring training materials to improve the health and health care of adults with DDs.22Working as a united group, the multiple stakeholders wrote the content for a 3-module training DVD and served as the actors for the clinical vignettes embedded within it. Each module addressed a different audience: the self-advocate (an individual with a DD), the direct support professional or family member, and the health care team. The collaborators also wrote a training curriculum for direct support professionals providing care for aging adults with DDs. Finally, they helped create and pilot test a behaviorally anchored videotape review instrument to allow physicians in training to improve their communication skills with people with DDs through structured review of videotaped “live” clinical encounters. These products of the training grant were disseminated by the grant participants to each of their affiliate stakeholder communities.
A shared mission of advocacy was further promoted by the invitation of physicians to serve on boards of advocacy organizations such as The Arc of Greater Cleveland.
Phase 3: Expanding the Mission to Health System Change and Research
The training DVD referenced above was premiered in a “red carpet” gala where participants in the training grant and additional invited members from the stakeholder communities viewed selected portions of the video. Invited guests included administrative officials from the Cleveland Clinic, the sponsoring health care institution. Following the successful completion of the training grant and the positive publicity surrounding it, the future PBRN director requested and received internal support from the Medicine Institute of the Cleveland Clinic to fund a year-long project called the Learning Collaborative in Developmental Medicine. Through this venue, the future PBRN collaborators met 1 half day every other month to examine the health care needs of specific subpopulations of people with DDs, for example, Down syndrome, autism, and cerebral palsy. Meetings included presentations by self-advocates and family members about their personal experiences of health care and the sharing of content knowledge through didactic lectures by collaborative members. Local health system–level data relevant to the specific population under discussion were made available through Explorys (Cleveland, OH), an electronic health record analytic platform company affiliated with the Cleveland Clinic. Clinical resources embedded in the electronic health record were created to enhance care.
In 2013 the PBRN Shared Resource at Case Western Reserve University began supporting the Learning Collaborative' s trajectory as a multifaceted, multistakeholder network. The network is now known as the DD-PBRN. It continues to include the core components of advocacy, clinical education, collaborative learning, and research.
Since its inception in 2013, the DD-PBRN has clarified its organizational mission and vision, hosted regular steering committee meetings, and submitted a grant proposal to the Patient-Centered Outcomes Research Institute. Once its local base is solidified, it plans to network with other disabilities, service, and health care communities throughout the nation.
Reflections on the Organizational History of DD-PBRN
Community Engagement: A Matter of Sequencing
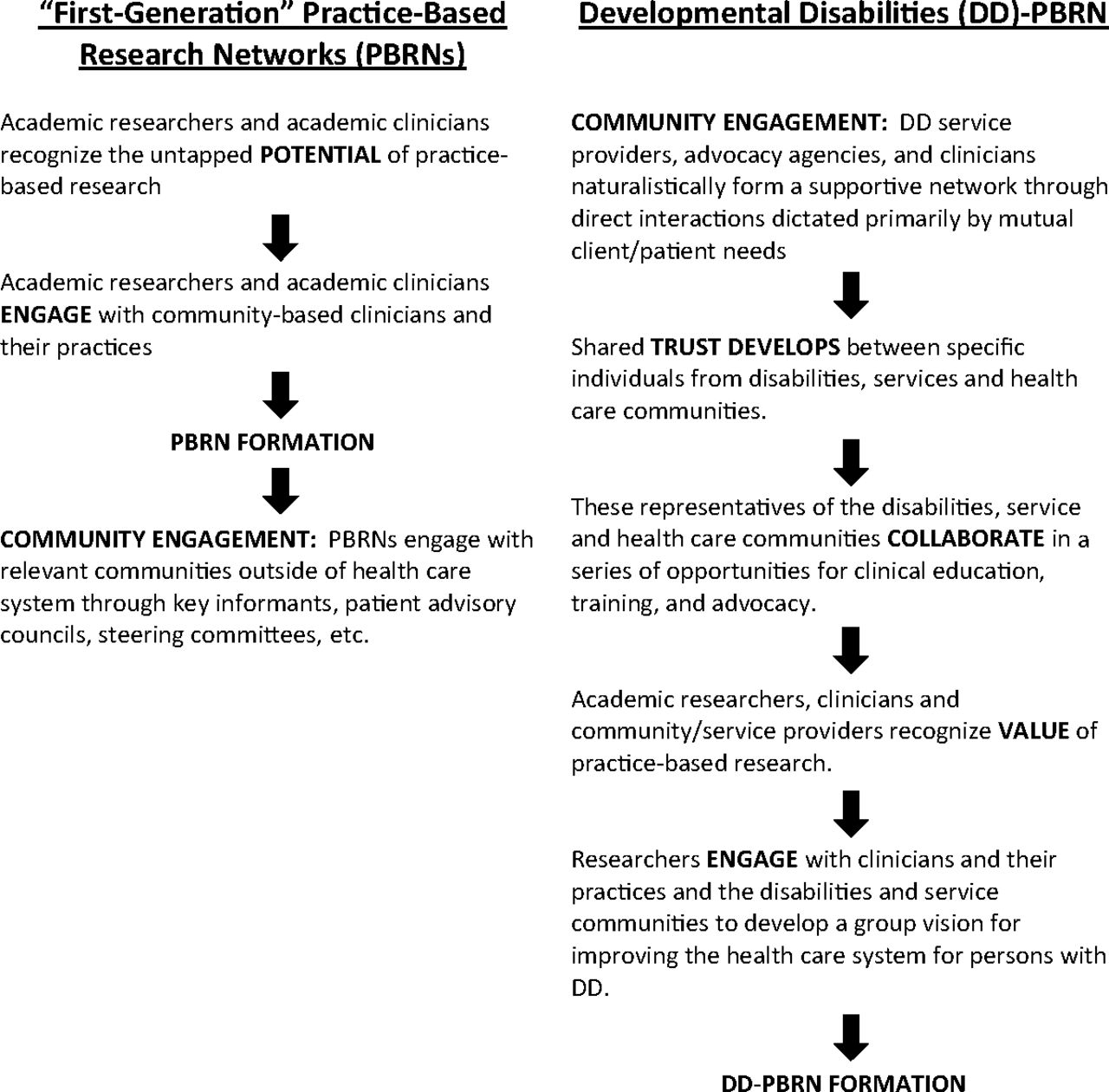
As referenced in Figure 2, early generation PBRNs originally comprised primarily of academic–clinical partnerships, are increasingly, and rightfully, concerned with community engagement with people and organizations outside of the formal health care system.23 Typically, this often occurs organizationally at a stage long after the PBRN was originally established, and it is now maturing and clarifying its mission and focus. In contrast, as illustrated in the case of the DD-PBRN, community engagement occurred as the initial organizing process, linking the health care community with other relevant communities long before the vision of a research mission was even contemplated. We propose that individuals who are involved in a PBRN from its inception–and the stakeholder groups they represent—would have a greater sense of perceived insider status, psychological ownership, and organizational identification than people who are invited as newcomers at a later time.24
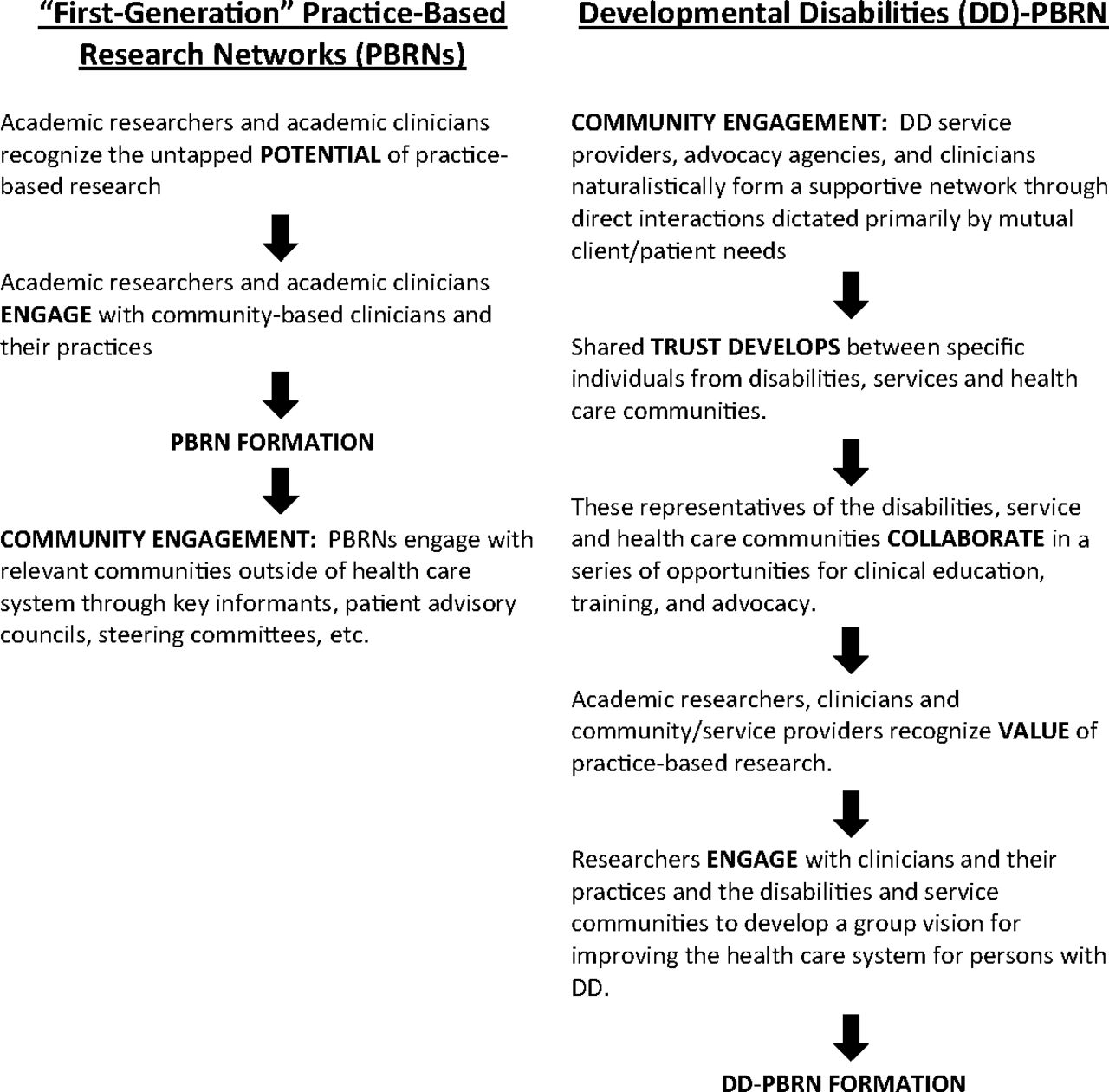
Comparing development of “first-generation” practice-based research networks (PBRNs) with that of the Developmental Disabilities PBRN.
The Role of Advocacy and Education
While some PBRNs addressing health care disparities in underserved populations may become involved with wider advocacy issues,25⇓–27 early generation PBRNs have tended to focus more strictly on research and the dissemination of specific findings. As illustrated by the DD-PBRN, advocacy was one of the core organizing principles for the network and will undoubtedly continue to be so. Community-based PBRNs such as the DD-PBRN are more likely to explicitly engage in advocacy as part of their core mission because they include advocates and advocacy organizations as core stakeholders. One of the challenges of this kind of network is balancing the demands of research with advocacy and other activities.
Similarly, community-based PBRNs, exemplified by LA Net,28⇓⇓⇓–32 are more likely to engage in broader roles of clinical education and community-wide education as part of their core activities. As illustrated in the prenatal history of the DD-PBRN, a shift in organizational dynamics occurred between organizational partners when members of the disabilities and service communities recognized their value as clinical educators to members of the health care system through their involvement as presenters at the Family Medicine Education Consortium annual meetings. The desperate need for basic health information related to DDs both within and outside of the health care community will make education an ongoing activity of the DD-PBRN.5,7,10, 26,33⇓⇓⇓–37
Flexibility Through Diversity
The diversity of membership within the nascent DD-PBRN allows for more expansive projects with a broader reach than what would have been possible if only 1 of the 3 participating communities had been involved. Similarly, we anticipate that more funding opportunities will be available as different support streams generally available to one stakeholder group or another become available to the entire group through their collaborative relationships as part of the DD-PBRN.
Diverse membership also promotes flexibility in potential study designs. For example, to improve the health care of adults with Down syndrome, the DD-PBRN designed a study that intervenes through virtual consultations with the primary care physician; we are now designing a study that intervenes through tailored resources provided to family members and residential service providers.
Hybrids, Chimeras, or a New Species Altogether? The Community-Engaged PBRN
There arises the question of whether to categorize the DD-PBRN as a PBRN at all; rather, is it an academic–community research partnership or some type of community-based research collaboration? Drawing on published literature articulating the core features of “first-generation” PBRNs,38 Table 2 describes how the DD-PBRN builds on but maintains fidelity to the core characteristics of a PBRN.
Critical Resources
The idea of a DD-PBRN slowly emerged following years of affiliation between constituent members. This emergent vision grew from a series of logical next steps, not by following a predetermined road map that was evident from the beginning. It developed in the context of a series of success experiences in which future PBRN members engaged in tasks beyond the scope of their usual daily work, for example, co-creating training and clinical resources and educating health professionals. A stable core of participants and partnering organizations enabled incremental group cohesion, fostered experiential knowledge, and stimulated awakening interest in health care improvement at the health system level. Leadership from the future PBRN director was required to identify, apply for, and coordinate these funded opportunities. The PBRN Shared Resource at Case Western Reserve University provided training to the future PBRN director through a 3-year fellowship in practice-based research design and methodology. The PBRN Shared Resource also provided critical assistance with the transition from learning collaborative to PBRN by providing a PBRN coordinator, educating PBRN members about practice-based research, and providing technical assistance with its first study. The DD-PBRN coordinator is currently supported by the PBRN Shared Resource at Case Western Reserve University, whereas the PBRN director's effort is supported by his sponsoring health care institution, the Cleveland Clinic.
Conclusion
Recollection and reflection about events leading to the creation of both recently and long-established PBRNs may assist others in their own efforts to establish new PBRNs and may provide ideas for ways existing networks might evolve by forging unique partnerships within and outside of the health care system. The DD-PBRN exemplifies a new generation of community-oriented PBRNs, whose complex origins began through shared service affiliations and whose present missions include advocacy and education as well as research.
Acknowledgments
The authors thank Rick Rader MD, Director of Morton J. Kent Habilitation Center at Orange Grove for his assistance with supportive documentation regarding the history of medical experimentation on persons with developmental disabilities. The authors also gratefully acknowledge representatives of the following organizations in the genesis of the DD-PBRN: The Arc of Greater Cleveland, Case Western Reserve University, Cleveland Clinic, Cleveland Clinical and Translational Science Collaborative, Cuyahoga County Board of Developmental Disabilities, HELP Foundation, Northeast Ohio Medical University, Welcome House, United Cerebral Palsy of Greater Cleveland, The Mentor Network, Koinonia, Via Quest, and Up Side of Downs. The authors thank Jennifer Solivas-Maluyao, MD; Linda Council, MSN, RN; and Michelle Abraham, MSSA, LISW, for their thoughtful review of this manuscript and Kathy Gaughan, BA, for her secretarial assistance. Finally, the authors gratefully acknowledge the personal support and institutional funding for the Learning Collaborative in Developmental Medicine provided by David Longworth, MD, Medicine Institute Chair, Cleveland Clinic.
Notes
This article was externally peer reviewed.
Funding: This publication was made possible through the PBRN Shared Resource of the Clinical and Translational Science Collaborative of Cleveland; grant UL1TR000439 from the National Center for Advancing Translational Sciences (NCATS) component of the National Institutes of Health (NIH) and NIH Roadmap for Medical Research; and the Case Comprehensive Cancer Center Support Grant 2P30CA043703–23 of the National Cancer Institute (NCI), NIH.
Disclaimer: The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of the NIH.
Conflict of interest: none declared.
- Received for publication January 16, 2014.
- Revision received August 6, 2014.
- Accepted for publication August 11, 2014.




{kind=link}
{kind=link}