
Abstract
Background: There is increased interest nationally in multicenter clinical trials to answer questions about clinical effectiveness, comparative effectiveness, and safety in real-world community settings. Primary care practice-based research networks (PBRNs), comprising community- and/or academically affiliated practices committed to improving medical care for a range of health problems, offer ideal settings for these trials, especially pragmatic clinical trials. However, many researchers are not familiar with working with PBRNs.
Methods: Experts in practice-based research identified solutions to challenges that researchers and PBRN personnel experience when collaborating on clinical trials in PBRNs. These were organized as frequently asked questions in a draft document presented at a 2013 Agency for Health care Research and Quality PBRN conference workshop, revised based on participant feedback, then shared with additional experts from the DARTNet Institute, Clinical Translational Science Award PBRN, and North American Primary Care Research Group PBRN workgroups for further input and modification.
Results: The “Toolkit for Developing and Conducting Multi-site Clinical Trials in Practice-Based Research Networks” offers guidance in the areas of recruiting and engaging practices, budgeting, project management, and communication, as well as templates and examples of tools important in developing and conducting clinical trials.
Conclusion: Ensuring the successful development and conduct of clinical trials in PBRNs requires a highly collaborative approach between academic research and PBRN teams.
There is increased interest nationally in multicenter clinical trials, especially pragmatic clinical trials (PCTs), to answer questions about clinical effectiveness, comparative effectiveness, and safety in real-world community settings. PCTs measure the effectiveness that a community-, clinical-, or system-level intervention produces in routine clinical settings.1 Primary care practice-based research networks (PBRNs) are an ideal setting for these PCTs.
PBRNs are composed of community- and/or academically affiliated practices that are committed to improving medical care for a range of health problems by conducting primary care research, engaging understudied populations, and accelerating the adoption of new knowledge and best practices. More than 100 PBRNs are registered with the Agency for Health care Research and Quality.2 A number of PBRNs have conducted PCTs in community-based primary care practices to evaluate treatment effectiveness and behavioral interventions for chronic conditions.3⇓–5However, many investigators have not had experience working with PBRNs.
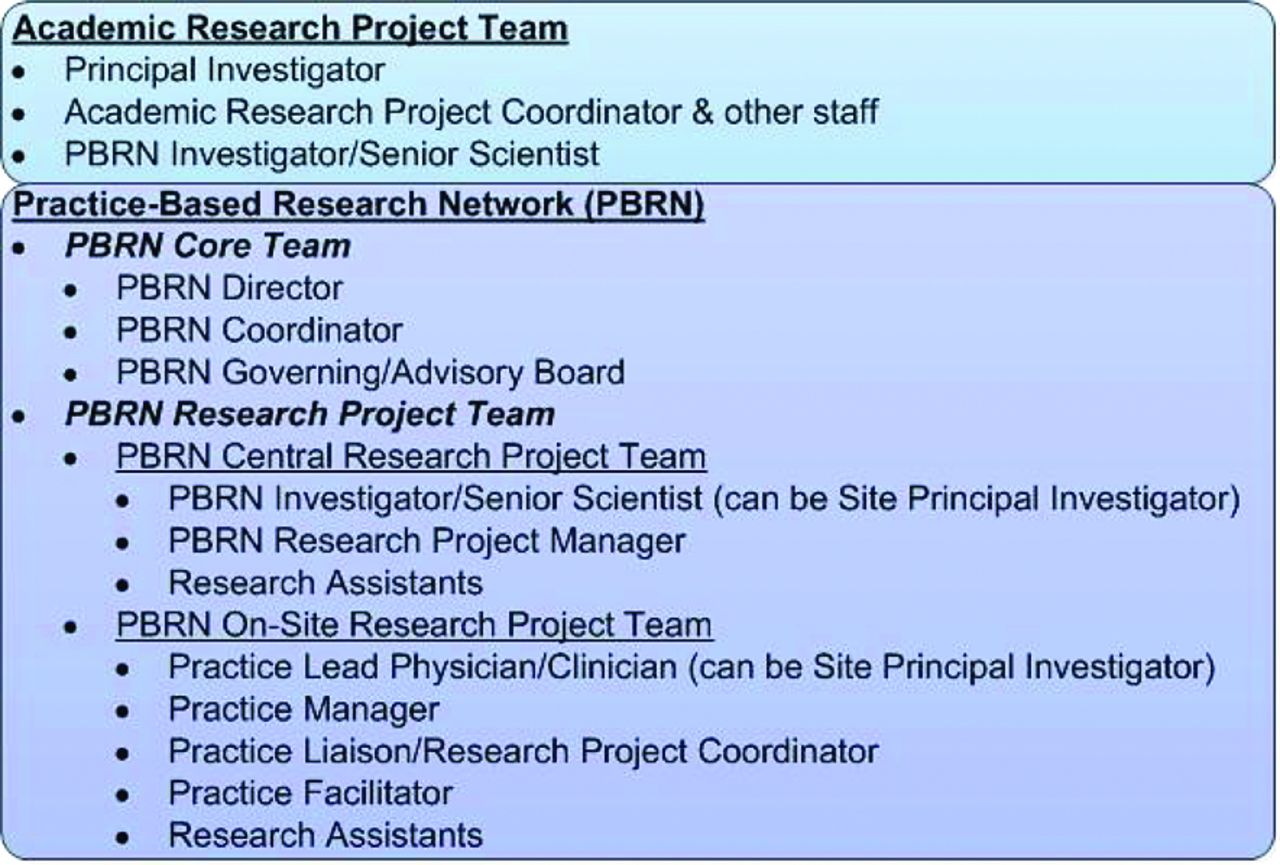
Through extensive involvement with clinical trials, PBRN leaders have found that the projects are most successful when the PBRN team (Figure 1) is engaged to assist with trial design, procedures, and budgeting (during the proposal submission phase); practice recruitment, participant recruitment, and communications (during the enrollment phase); management of the trial (during the trial conduct phase); and interpretation and dissemination of trial results, manuscripts, and presentations (during the close-out and dissemination phase). We created a toolkit consisting of a set of frequently asked questions (FAQs), templates, and examples of tools to guide researchers who are interested in conducting a clinical trial in a PBRN setting. In addition, these FAQs will assist PBRN directors and their teams in communicating with researchers about the project-specific needs of their PBRN.

Academic and practice-based research network (PBRN) teams and personnel.
Methods
Experts in practice-based research who are members of 2 workgroups—the DARTNet Institute (DI) Research Steering Committee and the Clinical Translational Science Award (CTSA) Community Engagement PBRN workgroup—identified the need to better communicate solutions to the challenges that researchers and PBRN personnel experience when collaborating while developing and conducting clinical trials in PBRNs. Five topic areas for development were originally proposed by these workgroups: (1) practice recruitment and engagement, (2) budgeting, (3) project management, (4) engaging and maintaining study teams, and (5) communication.
Each section was written in an FAQ format with advice relevant to different phases of a clinical trial: trial development, conduct, close out, and dissemination. A draft of the 5 sets of FAQs was presented at the 2013 North American Primary Care Research Group PBRN conference in Bethesda, Maryland, in a workshop format with small-group breakouts to discuss and refine each section. Based on feedback from the workshop participants, 2 sections (project management and engaging and maintaining study teams) were merged into 1 section entitled project management, and the resulting 4 FAQ documents were revised based on participant feedback. A revised draft of the FAQs and an introduction to these documents were sent to the DI Research Steering Committee, the CTSA Community Engagement PBRN, and North American Primary Care Research Group Committee for the Advancement of Science in Family Medicine PBRN workgroups for further input and modification.
The FAQ documents have been combined with templates and examples of tools important to clinical trial development and conduct, as well as with a glossary of terms (see Table 1 and Appendix 1) to create a web-based toolkit entitled “Toolkit for Developing and Conducting Multi-site Clinical Trials in Practice Based Research Networks.” This toolkit is available on the DARTNet Institute website at www.dartnet.info/clinicaltrialsPBRNtoolkit.htm.
Results
Summaries of the key recommendations from the FAQs are presented in the following sections.
Recruiting and Engaging Practices
Including a PBRN core team member (eg, PBRN director, PBRN investigator, PBRN coordinator) on the clinical trial research team is critical to facilitate practice recruitment. PBRNs have established relationships and garnered the trust of the practices and know or can determine the research capacities and suitability of the practices specific to a clinical trial. A short, 1-page information sheet that emphasizes the value of the trial to the practices and outlines the work required is ideal for recruiting purposes. There are a variety of different venues (eg, PBRN meetings, regular practice meetings) and communication tools (eg, newsletters, E-mails) that may be used to attract practices to participate in a trial. The PBRN team can help to determine the most effective venues and tools for a particular clinical trial and/or practice.
Strategies to keep practices engaged include minimizing the amount of work required by the practices, working with practices to implement the intervention(s) into their existing workflow, adequately compensating practices for their participation, providing additional training as needed throughout the trial, and frequently soliciting feedback from the practices. Keeping practices engaged can also be facilitated by identifying a practice lead physician/clinician who can provide leadership for the trial at the practice. Good communication is critical to keeping practices engaged and excited about a project. Table 2 summarizes the key points regarding recruiting and engaging practices.
Budgeting
As with other areas of a clinical trial, engagement of PBRN core team members as early as possible in the development of the budget is crucial. Ideally, a clearly designated scientific lead and administrative lead, including representation from the PBRN, should be involved in the budget process from the beginning. The PBRN core team will be able to advise on the overall structure of the budget as well as particular costs unique to a PBRN-based clinical trial (eg, PBRN infrastructure costs, practice honoraria, dissemination of findings to practices). Because of the multiple collaborators, following a strict timeline for completion of a grant proposal's budget, including a draft budget completed at least 6 weeks before the grant proposal due date and a final budget at least 3 weeks before the due date, is important. Discussion of any changes to the budget by all research team leaders and clear communication of these changes to participating entities is critical. Table 3 summarizes the key points related to the budgeting process.
Project Management
Practice-based research is distinctive because PBRN and practice representatives (eg, PBRN investigators, practice lead physicians/clinicians) are essential members of the research project team. Their roles are critical in all stages of a clinical trial. Early engagement of these team members is essential for the appropriate design and implementation of the trial protocol.6 With their knowledge of the capacity of the participating practices, the PBRN director and PBRN coordinator are able to offer critical feedback on the effort required by the PBRN central research project team and the participating practices to implement the clinical trial. Given its established research relationships with the practices, the PBRN central research project team also plays a key role in the ongoing conduct of the clinical trial.
Because responsibilities differ for each clinical trial, determining before the start of the trial which tasks will be performed by the academic research project team, the PBRN central research project team, and the PBRN on-site research project team is imperative. For most studies, a PBRN research project manager will be assigned to coordinate clinical trial implementation with the academic research project team. The PBRN research project manager and PBRN central research project team may manage the trial directly or they may work closely with an on-site practice liaison/research project coordinator who manages on-site trial implementation.
Given the different personnel and organizations involved, a PBRN-based clinical trial will run more smoothly with a formal manual of protocol procedures that outlines all trial procedures and is accessible to all project personnel; the manual should include flow charts or summaries that address any workflow questions. This helps to ensure fidelity to the intervention and the collection of high-quality data. In addition the PBRN should maintain a regulatory binder, which contains the study protocol, consent form, institutional review board (IRB) approval/correspondence, regulatory documents (such as the US Food and Drug Administration Statement of Investigator 1572 form, drug accountability form, if applicable), curriculum vitae and training documents of the principal investigator and key personnel, and other site-related documents. Managing the quality of the trial also requires documenting trial progress in detail and maintaining organized trial files. Communication is key to keeping all members of the PBRN on-site research project team engaged. Finally, keeping the participating practices and patients informed by providing updates on trial results and publications through letters, E-mail, or newsletters is important. Table 4 summarizes the key points regarding project management.
Communication
Good communication ensures that the clinical trial runs smoothly and that patient care is enhanced and not compromised. Clinical trials conducted in collaboration with a PBRN often have a number of diverse collaborators. Given these many diverse collaborators, establishing clear lines of communication is especially important. To be effective, communication should be multidirectional, allowing all the collaborators the ability to share ideas, ask questions, or voice concerns. Good communication depends on the recognition that each collaborator brings particular skills and expertise that are important to the success of the trial. Good communication is designed to keep all collaborators updated on issues such as trial progress, issues or concerns that have arisen, and changes in the clinical trial protocol. Toward the end of the trial, ensuring that the participating practices receive trial results and have a chance to help interpret research findings is particularly important. These “observations from the field” help to explain research results and inform the discussion of the findings. Table 5 summarizes the key points regarding communication.
Discussion
PBRNs provide an ideal setting in which to conduct clinical trials, especially PCTs. However, many academic researchers have not worked with PBRNs and may not be aware of the many elements specific to designing and implementing an effective clinical trial with PBRN partners. We have developed the “Toolkit for Developing and Conducting Multi-site Clinical Trials in Practice Based Research Networks” to offer guidance to investigators interested in conducting clinical trials with PBRNs with the hope of facilitating collaborations between investigators and PBRN teams and promoting the success of clinical trials. To reach as broad an audience as possible, this toolkit will be hosted on the DARTNet Institute website with links to the CTSA/National Center for Advancing Translational Sciences, Community Campus Partnerships for Health, and research toolkit web sites, among others.
As an example, the Translating Research into Primary Care Practice for Postpartum Depression (TRIPPD) study funded by the Agency for Health care Research and Quality assessed the effectiveness of postpartum depression screening and management in 28 practices in a single PBRN, the American Academy of Family Physicians National Research Network. During the grant submission phase, the project principal investigator, co-investigators, and PBRN director were involved in writing the proposal and developing the budget. Together they modified the research plan (eg, recruitment and study procedures) to fit a busy clinical environment and calculated the personnel time and practice reimbursement required during the course of a project. The PBRN director served as the principal investigator for the PBRN subcontract. When the grant was awarded, the PBRN central research team was instrumental in recruiting practices using established communication venues (practice meetings, teleconferencing) and materials (research summary with copies of recruitment materials and consent) that were collaboratively developed by the academic research project team and the PBRN core team. The practice personnel received study-specific training, IRB training, regulatory document support, and a manual of protocol procedures was created to ensure implementation fidelity. After IRB approval, recruitment commenced and the academic research project and PBRN core teams collaboratively monitored enrollment metrics and retention rates. Regular communication between the academic research project team, the PBRN central research and core teams, and the participating practices was established through weekly team (academic project research team and PBRN core team) conference calls, weekly project calls between PBRN central research team members and practice staff, weekly study E-newsletters called “FAQs,” and monthly calls between academic study investigators, the PBRN principal investigator, and practice lead clinicians. The academic research project team and the PBRN core team met face to face at least once a year to discuss data analysis, interim results, dissemination of results, and publications. The budget included personnel effort for the PBRN director, PBRN associate director, PBRN research assistant, and PBRN system analyst. Practice lead clinicians and practice research project coordinators were compensated for time spent on training. Participating practices were provided an annual stipend based on completing milestones. A 2-day face-to-face study kickoff meeting with 2 attendees from each practice site, as well as annual meetings for the academic research project team and PBRN central research project team during the life of the grant, were budgeted. All practice staff were invited to periodic events funded by the academic research project team, such as pizza parties, to encourage practice-wide involvement in the trial. Indirect costs for the PBRN were included.5,7
A listing of documents such as those used for practice recruitment, participant recruitment, and site communication is included in Appendix 1. The full resources are available as links or downloads on the DARTNet website (www.dartnet.info/clinicaltrialsPBRNToolkit.htm). Many were developed for projects we conducted and were determined to be good examples to list as resources.
Conclusion
Ensuring the successful development and conduct of clinical trials in PBRNs requires a highly collaborative approach between academic research and PBRN teams—collaboration that we hope is facilitated by our “Toolkit for Developing and Conducting Multi-site Clinical Trials in Practice Based Research Networks.”
Acknowledgments
The DARTNet Institute Research Steering Committee, CTSA Community Engagement PBRN workgroup members, the North American Primary Care Research Group (NAPCRG) Committee on Advancing the Science of Family Medicine PBRN workgroup, workshop participants at the NAPCRG PBRN 2013 conference, Kim Kimminau, PhD, and Wilson D. Pace, MD, FAAFP, all contributed to the development of the “Toolkit for Developing and Conducting Multi-site Clinical Trials in Practice Based Research Networks.”
Appendix 1
Toolkit Resources
Notes
This article was externally peer reviewed.
Funding: This work was supported in part by the National Center For Advancing Translational Sciences of the National Institutes of Health under Award Numbers UL1TR000423 and UL1TR001117.
Conflict of interest: none declared.
Disclaimer: The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
- Received for publication June 5, 2014.
- Revision received July 31, 2014.
- Accepted for publication August 6, 2014.




{kind=link}