
Article Figures & Data
Figures
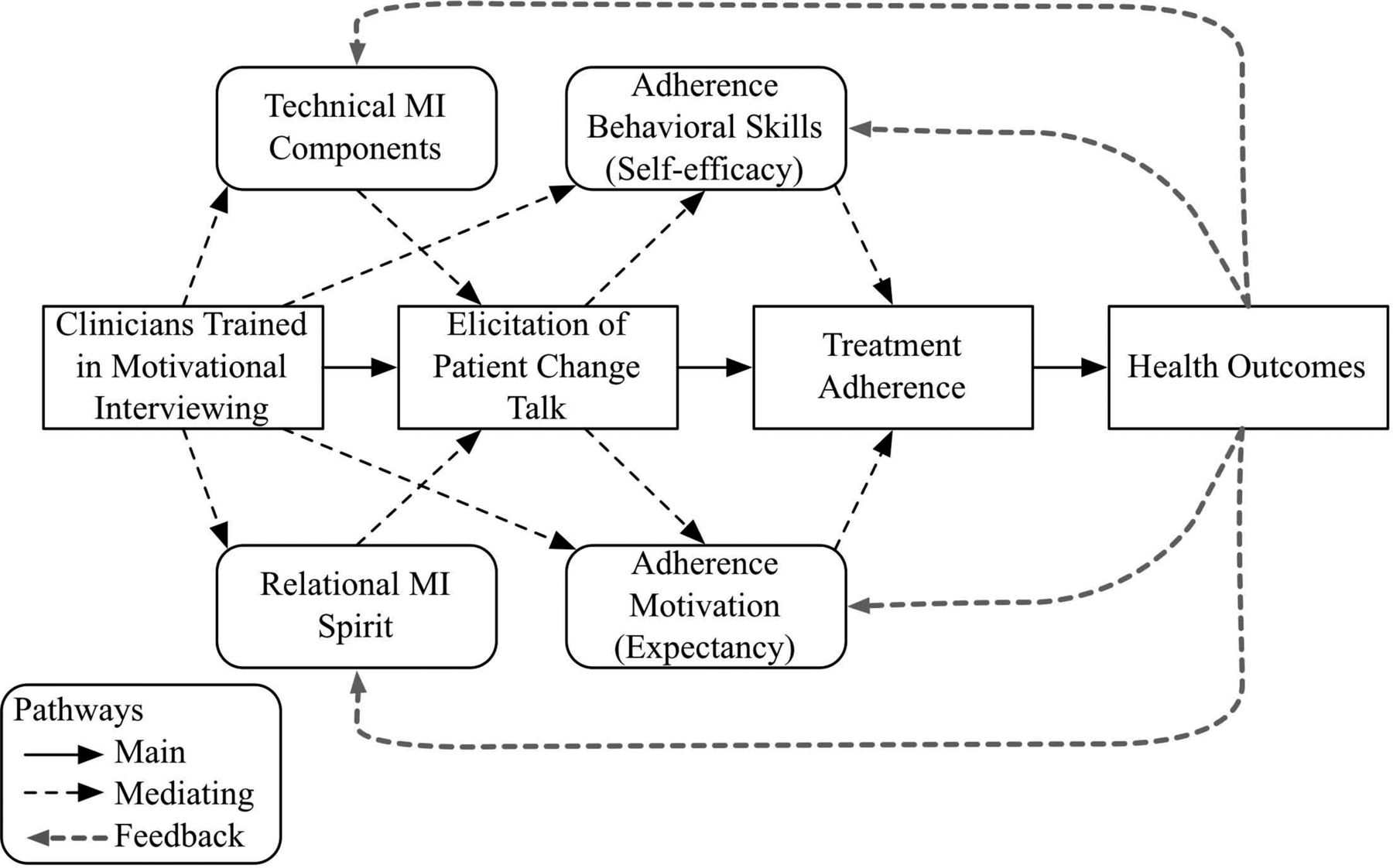
- Figure 1.
Theoretical model of how motivational interviewing (MI) training influences patient treatment and health outcomes.
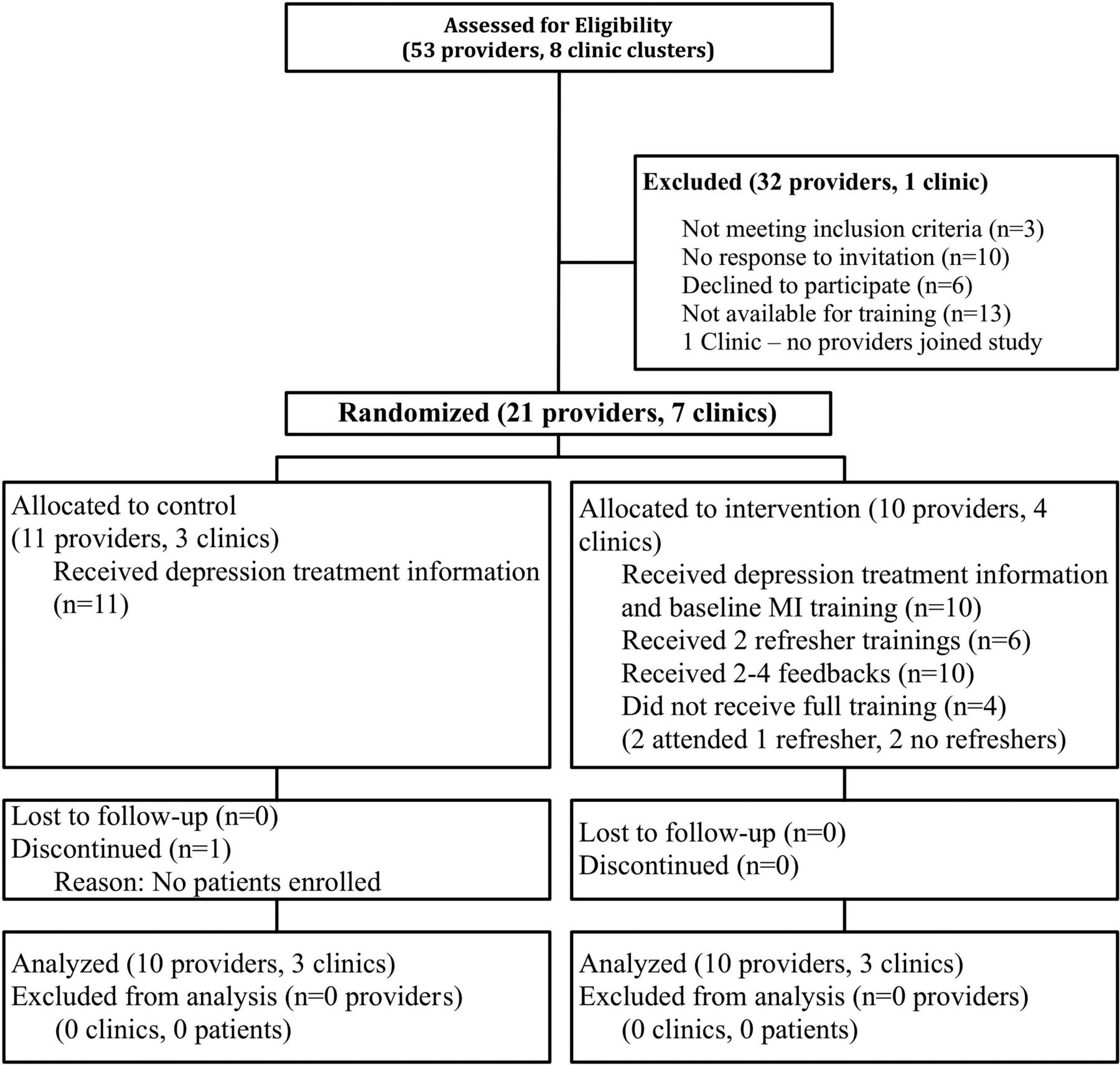
- Figure 2.
Flow diagram of primary care provider progress through the phases of the randomized trial. MI, motivational interviewing.

Tables
Baseline visit goals: Follow-up visit goals: Enhance treatment adherence with “rulers”***
Explore other relevant behavioral targets
Foster behavioral activation and problem solving
↵* OARS: Open questions, Affirmations, Reflections, Summary statements.
↵** Elicit-Provide-Elicit: A method of asking about current knowledge, providing information with permission, and asking patient to reflect on the new information. Goal is to elicit change talk.
↵*** Rulers: 10 point scale of patient's confidence in and perceived importance of behavior change.
Characteristics* Intervention† Control‡ Providers n = 10 n = 11 Age, years 49.2 (7.6) 47.4 (8.6) Female sex (n) 6 8 Ethnicity (n) White 8 10 Hispanic 1 2 Specialty (n) Internal medicine 3 2 Family medicine 4 6 Nurse practitioner 2 2 Physician's assistant 1 1 Years in practice 16.8 (8.6) 17.5 (8.8) Previous MI training (hours) 1.1 (3.3) 0.5 (0.8) Patients§ n = 85 n = 86 Clusters (n) 10 11 Age, years 51.5 (7.9) 45.3 (7.3) Female sex, % 62.0 (31.1) 67.8 (24.5) Race/ethnicity, % Non-Hispanic white 17.6 (13.7) 26.0 (14.6) Non-Hispanic black 32.6 (34.8) 43.2 (23.9) Hispanic 38.2 (31.4) 25.2 (26.4) Other 11.7 (9.8) 5.6 (7.7) Insurance, % Uninsured 34.5 (20.3) 46.4 (24.6) Private 2.9 (7.1) 2.7 (4.3) Public 62.5 (21.9) 49.8 (22.1) Household income <$10,000, % 48.0 (20.7) 51.7 (23.5) Employed 39.9 (23.9) 47.6 (14.1) Body mass index (kg/m2) 31.5 (3.9) 32.9 (3.3) Physical comorbidities‖ 2.3 (0.8) 2.1 (1.0) PHQ-9 score 15.6 (2.4) 15.9 (1.8) Data are mean (standard deviation) of participants unless stated otherwise.
↵* The number of participating primary care physicians (PCPs) was distributed as follows: 2 clinics with 1 PCP, 1 with 2 PCPs, 3 with 4 PCPs, and 1 with 5 PCPs.
↵† Motivational interviewing with standard management of depression training.
↵‡ Standard management of depression training alone.
↵§ Patient characteristics were analyzed by cluster. Data provided are per cluster.
↵‖ Comorbid categories were derived from abstracting the electronic medical record of up to 8 common chronic diseases in the patient problem list, including arthritis, asthma, chronic pain, congestive heart failure, chronic obstructive pulmonary disease, coronary heart disease, diabetes, and obesity (body mass index ≥30 kg/m2).
PHQ-9, 9-item Patient Health Questionnaire.
- Table 3. Comparison of Mean Scores for Provider- and Patient-level Outcomes by Randomization Arm
Provider- and Patient-Level Measures Intervention* Mean or Proportion (SD) n = 85 Control† Mean or Proportion (SD) (n = 86) P Value Adjusted Odds Ratio or Cohen's d** (95% CI) Summary MI performance Rate of MI-consistent statements‡ 8.80 (4.16) 6.98 (4.14) .005 d = 0.44 (0.13–0.74) Summary global rating Beginning spirit in MI Spirit (≥3.5) 0.37 (1.01) 0.15 (0.59) .083 3.28 (0.83–12.90) Provider treatment advice Recommendation for physical activity 0.34 (0.54) 0.19 (0.43) .053 2.21 (0.99–4.95) Prescription for antidepressant medication 0.42 (0.53) 0.38 (0.51) .66 1.17 (0.59–2.30) Frequency of patient change talk Rate of all depression treatment-related‖ change talk‡ 0.90 (0.91) 0.44 (0.90) .001 d = 0.51 (0.21–0.82) Rate of change talk specific to physical activity 0.30 (0.51) 0.10 (0.51) .01 d = 0.39 (0.09–0.70) Rate of change talk specific to antidepressant medication 0.25 (0.47) 0.15 (0.46) .17 d = 0.21 (−0.09 to 0.51) Treatment adherence Days physically active in past week,§ n¶ 3.05 (2.83) 1.84 (2.75) .007 d = 0.42 (0.11–0.72) Filled prescription, % 0.62 (0.17) 0.56 (0.17) .63 1.27 (0.48–3.34) Data are number (%) of participants unless stated otherwise.
↵* Motivational interviewing (MI) with standard management of depression training.
↵† Standard management of depression training alone.
↵‡ Mean rate of open questions, reflective statements, or MI-adherent statements per 10 minutes of the clinical encounter.
↵§ Physical activity was ascertained on average 5.4 days (standard deviation, 3.3 days) after the index encounter.
↵‖ Includes change talk regarding physical activity, antidepressant medication, specialty mental health counseling, and nonharmful behaviors the patient suggests might alleviate depressive symptoms.
↵¶ Days in the previous week during which patient engaged in at least 30 minutes of physical activity.
↵** Clinical effect sizes based on Cohen d values: 0.2, small; 0.5, medium; 0.8, large. Clinical effect sizes based on odds ratio (OR): 1.29, small; 1.88, medium; 2.79, large.44
- Table 4. Provider Motivational Interviewing Treatment Integrity Technical and Relational Measures by Randomization Arm
Mean (SD) by Treatment Arm P Value Intervention* (n = 85) Control† (n = 86) Visit time (seconds) 1571 (480) 1447 (545) .056 MI treatment integrity instrument component measure‡ MI-adherent statements 3.49 (3.29) 2.01 (3.3) .004 Asking permission§‖ 0.75 (0.92) 0.13 (0.92) <.0001 Affirmations§‖ 1.07 (1.65) 0.39 (1.64) .007 Emphasizing control‖ 0.31 (0.76) 0.42 (0.76) .34 Support‖ 1.35 (1.91) 1.08 (1.91) .36 MI nonadherent statements† 3.14 (7.11) 3.62 (7.05) .66 Advising 1.24 (2.81) 1.48 (2.79) .58 Confronting 1.10 (3.23) 1.30 (3.20) .68 Directing 0.75 (1.80) 0.84 (1.80) .76 Percent MI-Adherent 56.04 (63.41) 37.69 (61.62) .07 Beginning proficiency for Percent MI-Adherent (n/N)¶ 0/10 0/10 — Questions Closed 29.85 (20.76) 25.93 (20.65) .22 Open§‖ 5.87 (3.87) 4.5 (3.87) .02 Open questions (%)¶ 16.97 (10.59) 15.37 (10.58) .32 Beginning proficiency for open questions (n/N) 0/10 0/10 — Reflections Simple‖ 6.73 (6.60) 6.48 (6.57) .80 Complex§‖ 2.91 (3.38) 1.74 (3.38) .03 Complex reflection (%)¶ 28.92 (33.96) 19.41 (33.62) .07 Beginning proficiency for complex reflections (n/N) 2/10 0/10 .47 Reflection-to-question ratio¶ Giving information 20.16 (11.78) 20.86 (11.75) .70 Global ratings Evocation 3.00 (2.08) 2.52 (2.07) .127 Evocation: beginning proficiency¶ 3/10 0/10 .21 Collaboration 3.13 (2.23) 2.74 (2.21) .25 Collaboration: beginning proficiency¶ 3/10 2/10 1.00 Autonomy support 3.21 (1.75) 2.79 (1.74) .11 Autonomy support: beginning proficiency 1/10 3/10 .58 Direction 4.40 (1.28) 3.97 (1.28) .03 Direction: beginning proficiency‡ 10/10 8/10 .47 Empathy 3.22 (2.03) 2.82 (2.01) .20 Empathy: beginning proficiency 3/10 2/10 1.00 Data are number (%) of participants unless stated otherwise.
↵* Motivational interviewing (MI) with standard management of depression training.
↵† Standard management of depression training alone.
↵‡ Language counts, frequencies, and global scores are derived from clustered analyses. For standardization purposes the language counts are adjusted for encounter length (seconds).
↵§ Motivational Interviewing Treatment Integrity (MITI) component was a focus in >1 MI classroom training.
↵‖ MITI component included in composite frequency of MI-consistent language measure.
↵¶ MITI ratio definitions: percentage adherent to MI = MI-adherent statements/(MI-adherent statements + MI-nonadherent statements); percentage of OC = open questions/(open questions + closed questions); percentage of complex reflections = complex reflections/(complex reflections + simple reflections); reflection-to-question ratio = (simple + complex reflections) / (closed + open questions).
- Table 5. Association between Motivational Interviewing (MI) Trainings Attended and MI Performance and Global Rating
MI Measure Training Sessions 3 Sessions (n = 47) 2 Sessions (n = 21) 1 Session (n = 17) Control (n = 86) MI performance score MI-consistent statement rate (per 10 minutes of the encounter) (95% CI) 9.59 (8.5–10.7) 8.55 (7.0–10.2) 6.92 (5.1–8.7) 6.96 (6.2–7.8) 3 MI training sessions vs comparator, Cohen d (95% CI), P value 0.28 (−0.21 to 0.77), .290 0.72 (0.21–1.24), .012 0.71 (0.36–1.06), <.001 Global Rating Beginning Spirit in MI Spirit (3.5 or higher) (95% CI) 0.49 (0.22–0.77) 0.25 (0.04–0.72) 0.18 (0.02–0.67) 0.15 (0.06–0.32) 3 MI training sessions vs comparator, OR (95% CI), P value 2.89 (0.27–31.21), .380 4.27 (0.34–53.37), .26 5.6 (1.13–27.89), .036 Clinical effect sizes with Cohen's d: 0.2, small; 0.5, medium; 0.8, large. Clinical effect sizes with odds ratio (OR): 1.29, small; 1.88, medium; 2.79, large.44
Components1,2 Definition Examples/Rating Scheme Relational domain MI Spirit MI spirit is exemplified by collaboration in all areas of MI practice; eliciting and respecting the client's ideas, perceptions, and opinions; eliciting and reinforcing the client's autonomy and choices; and accepting the client's decisions.
The spirit of MI has 3 foundations:Collaboration: Collaboration between the primary care provider and the patient or “client” builds a trusting relationship.
Evocation:- Helping the client to voice their own ideas and reasons for change.
Autonomy/support: The provider supports the patient as the agent of change, and the patient is responsible for following through or not. The provider is supportive of the patient regardless of whether and how they decide to change.
Average of global scores of evocation, collaboration, and autonomy/support (scales of 1 to 5; percentage highest; average, 3); providers score high on collaboration when they negotiate with the client, respect the client's ideas about how change can occur, avoid persuasion, and focus on supporting the client's own concerns and ideas. Confrontational, authoritative, and rigid providers score low on collaboration.
Higher scores on evocation result when the provider draws out the client's ideas as opposed to instilling knowledge, insights, and advice. Lower scores are ascribed to providers who show little interest in the client's perspective or display cynicism about prospects for change.
Higher scores for autonomy/support occur when the provider readily accepts the client's decisions not to change at that particular moment. This provider recognizes that critical factors predicting change reside within the client. Low autonomy/support is typified by an urgency to change and lack of acceptance of the client's capability to decide to change or not; client freedom of choice and self-determination is not recognized in this instance.Empathy Expressing empathy includes expressing understanding of the patient's lived experience or seeing, feeling, and experiencing the world through the patient's eyes. Range 1 to 5 (higher is better; average, 3); high empathy is characterized by the provider showing active interest in the client's perspectives, including situation, meaning, perceptions, and feelings. Low empathy is characterized by a lack of interest in the client's perspectives and experiences. Probing for factual information and pursuing an agenda are examples of low empathy. Technical domain MI-adherent statements This category is used to capture particular interviewer behaviors that are consistent with a motivational interviewing approach.
Affirmation: The provider says something positive or complementary to the client; may be in the form of appreciation, confidence, or reinforcement. The provider comments on the client's strengths or efforts.
Emphasize autonomy: The provider recognizes the client's freedom of choice, autonomy, and ability to decide.
Asking permission before giving advice or permission: Asking what the client already knows or has already been told about a topic before giving advice or information.
Support: The provider makes a statement that takes on a compassionate, sympathetic, supportive, or agreeing quality.“It takes courage to come in and talk about depression.” (Affirm)
“You've got a point there.” (Emphasizing the client's control)
“May I share some information about antidepressant medications?” (Ask permission)
“Well, there is really a lot going on for you right now.” (Support)Open-ended questions An open question is coded when the interviewer asks a question that allows a wide range of possible answers. The question may seek information, invite the client's perspective, or encourage self-exploration. The open question allows the option of surprise for the questioner.
“Tell me more” statements are coded as open questions unless the tone and context clearly indicate a direct or confront code.“What is your take on that?” (Open question) Reflective statements (simple and complex) This category is meant to capture reflective listening statements made by the provider in response to client statements. A reflection may introduce new meaning or material, but it essentially captures and returns to clients something about what they have just said.
Simple: Simple reflections typically convey understanding or facilitate client/provider exchanges. These reflections add little or no meaning (or emphasis) to what clients have said.
Complex: Complex reflections typically add substantial meaning or emphasis to what the client has said. These reflections serve the purpose of conveying a deeper or more complex picture of what the client has said. Sometimes the provider may choose to emphasize a particular part of what the client has said to make a point or take the conversation in a different direction.“You are determined to start an antidepressant medication.” (Simple reflection)
“On the one hand you perceive potential benefit from the medicine, and on the other hand you are terrified of getting addicted.” (Complex reflection)MI-consistent language MI adherent statements + reflections + open questions Rulers The confidence and importance rulers invite the client to rate their confidence or importance on a 0 to 10 scale regarding making a target behavior change. The provider may implement the rulers to evoke client “change talk,” or language toward making a specific behavior change. When the client provides a number, eg, “5,” the provider can ask, “Why did you say ‘5’ and not ‘2’?” which evokes reasons for change. Alternatively, the provider might say, “What would it take to raise the ‘5’ to an ‘8’?,” which also evokes change talk. The process involves 2 open questions. Ask–provide–ask or elicit–provide–elicit The ask—provide–ask tool is an MI-consistent approach to sharing information. First, the provider asks permission to share information, then with permission shares information, and follows by asking the client what they think or how they are reacting to the information. A variant is the elicit–provide–elicit approach for garnering learning about a client's thoughts or perspectives, sharing information or one's perspectives with permission, then eliciting more of the client's perspectives and change talk. The provider firsts asks permission to share information by asking, for example, “Would you be interested in hearing more about possible treatment options for depression?” If the patient assents, the provider can then provide information, then ask about or elicit the client's thoughts, eg, by asking “What do you think about those options?” Elaborate, affirm, reflect, summarize When a provider recognizes change talk, the goal is to reinforce the change talk. The provider then asks the patient to elaborate on what they meant using evocative questions, affirms the patient's statements toward positive change, and reflects the change talk. This approach often elicits more change talk. The provider then summarizes the patient's change talk, any plans to change, and strengths. Giving information If the provider gives information, educates, provides feedback, or discloses personal information, it is considered “giving information.” An example would be feedback from a depressive symptom scale. “You scored a 19 on the depressive symptoms scale, which is consistent with moderately severe depressive symptoms.” Closed questions Closed questions can be answered with a “yes” or “no.” “Have you been taking your antidepressant medication as prescribed?” MI-nonadherent statements Advising, directing, confronting
Advising without permission involves uninvited advice, suggestions, or a solution.
Direct- involves a command, direction, or order.
A confrontation involves expert-like responses that have a particular negative/parental quality, an uneven power relationship accompanied by disapproval, disagreement, or negativity.
The provider may directly disagree, argue, correct, shame, blame, seek to persuade, criticize, judge, label, moralize, ridicule, or question the client's honesty.“I'd recommend that you start an antidepressant medication.” (Advising)
“At this point, you really need to get some therapy.” (Direct)
“It's evident to me that you are not taking your medicine.” (Confrontation)Measure ICC fMICO (rate) 0.74 MI spirit 0.54 MI-adherent statements, % 0.61 Open questions, % 0.70 Complex reflections, % 0.45 Giving information (adjusted for time) 0.79 Change talk pertaining to ways to handle depression (rate) 0.83 Change talk around medications for depression (rate) 0.85 Change talk around physical activity (rate) 0.76 fMICO, frequency of MI-consistent language; MI, motivational interviewing.
Measure By Provider Rate of MI-consistent language 0.009 MI spirit (1–5) 0.48 Beginning proficiency in MI spirit (≥3.5) 0.22 Prescription for antidepressant provided 0.00 Recommendation of physical activity 0.0005 Change talk regarding depression treatment frequency 0.021 Change talk specific to antidepressant medication frequency 0.010 Change talk specific to physical activity frequency 0.0036 Physical activity 0.014 Filled antidepressant medication 0.056 ↵* Coefficients of intracluster correlation are considered small (<0.05), medium (<0.15), or large (>0.15).43
MI, motivational interviewing.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Cluster randomised trial of a health system strengthening approach applying person-centred communication for the prevention of female genital mutilation in Guinea, Kenya and Somalia
- Does education of primary care professionals promote patient self-management and improve outcomes in chronic disease? An updated systematic review
- Better Doctor-Patient Relationships Are Associated with Men Choosing More Active Depression Treatment
- This Issue: Important Clinical Studies with New Useful Information on Problems Encountered Daily by Family Physicians