
Article Figures & Data
Figures
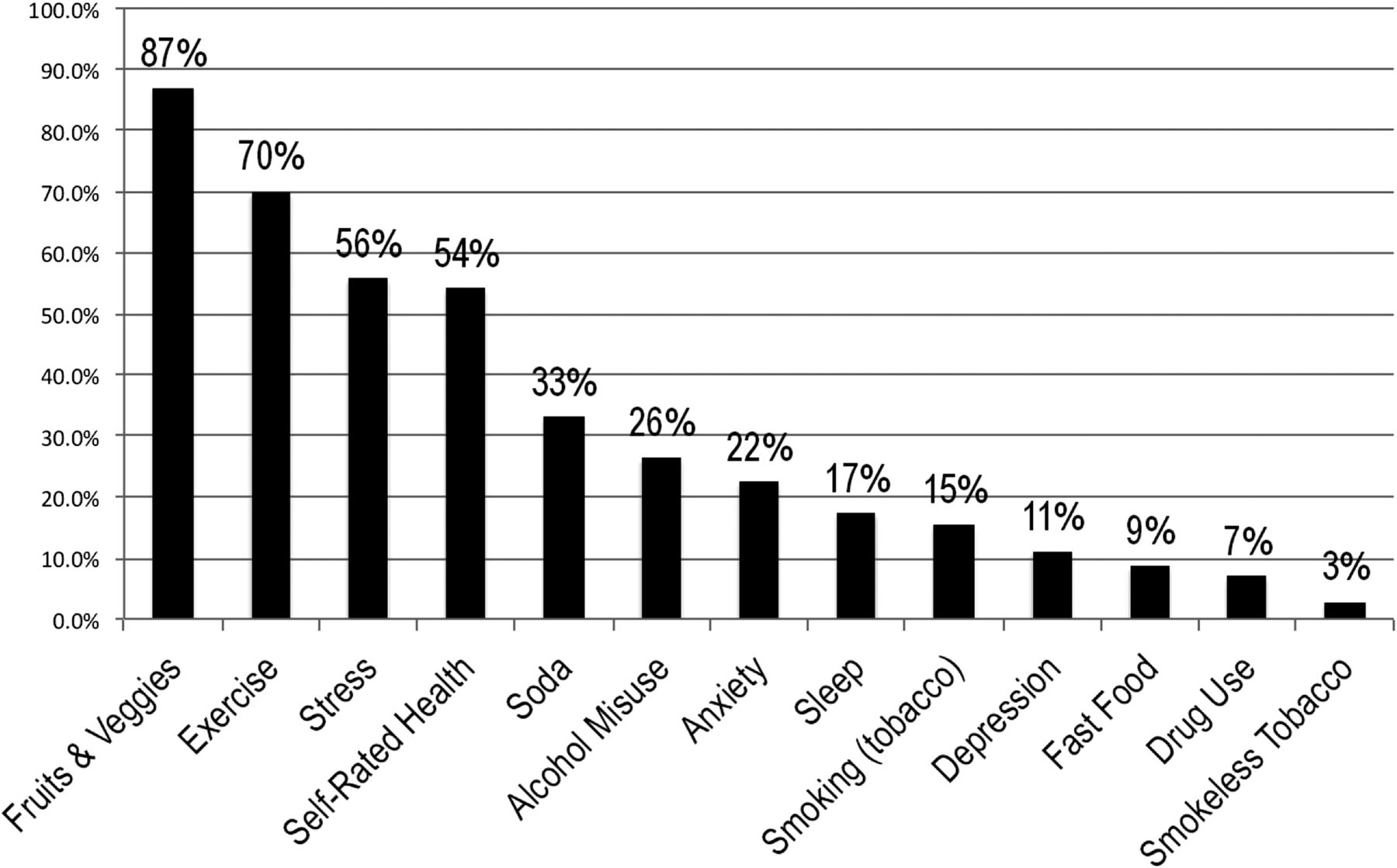
- Figure 1.
Proportion of respondents screening “positive” for intervention for each health behavior and mental health measure

Tables
Practice Site Location Practice Type Primary Patient Demographics History of Implementing Behavioral Health Assessments Electronic Health Record Duration (days) Total Assessments Completed, n (% reach) Patients Providing Feedback (%) A Los Angeles, CA FQHC Low-income, Chinese-American (85%) Registered nurse administered behavioral health assessment during initial intake appointments Yes 6 66 (79)* 94.0 B Santa Ana, CA FQHC Low-income, Mexican-American (76%) Prior use of depression screening (PHQ-9) No 5 59 (74)* 59.3 C Eagle Rock, CA FQHC Low-income, Filipino-American (58%) and Mexican-American (27%) No routine collection of behavioral health data Yes 10 65 (65)* 93.8 D Los Angeles, CA FQHC Low-income, Mexican-Americans (51%) and Central-Americans (31%) No routine collection of behavioral health data Yes 4 93 (85)* 95.7 E Montpelier, VT PBRN Lower-middle income, white (90%) Intermittent use of depression (PHQ-9), anxiety (GAD), and alcohol use (Audit-C) Yes 3 22 (64)* 95.5 F Front Royal, VA PBRN Lower-middle income, white (85%) Routinely assessed multiple health behaviors through personal health record Yes 3 45 (73)† 88.9 G Bon Secours, VA PBRN Lower-middle income, African American (85%) Routinely assessed multiple health behaviors through personal health record Yes 2 20 (88)† 85.0 H Richmond, VA PBRN Lower-middle income, African American (60%) and white (30%) Routinely assessed smoking status but no other behavioral or mental health assessment Yes 4 35 (59)† 100 I Bedford, MA VA Lower-middle income, white veterans (90%) Intermittent collection of behavioral health data but no comprehensive behavioral health assessment in place Yes 4 57 (60)* 91.2 ↵* For 6 practices, reach was calculated using administrative reports (no. of completed surveys / no. number of nonurgent patient visits).
↵† For 4 practices, reach was calculated using tallies by the research team (no. of completed surveys / no. of nonurgent patients offered the survey).
AUDIT-C, Alcohol Use Disorders Identification Test; FQHC, federally qualified health center; GAD, generalized anxiety disorder; PBRN, practice-based research network; PHQ-9, 9-item Patient Health Questionnaire; VA, Veterans Health Administration.
Patient Characteristics Overall (n = 463) FQHCs (n = 284) PBRNs (n = 122) VA (n = 57) P Value Female sex 61.2 70.2 65.3 3.8 < .001 Age, years < .001 <30 5.0 5.4 4.3 3.9 30–39 7.66 7.6 10.3 1.9 40–49 15.8 17.4 15.5 7.7 50–59 32.2 37.7 24.1 21.2 60–69 28.4 26.5 29.3 36.5 70–79 7.4 5.1 11.2 11.5 ≥80 3.6 0.4 5.2 17.3 Education < .001 Less than high school 34.6 50.4 11.2 3.9 High school graduate or GED 25.3 21.7 33.6 25.5 Some college 14.8 11.0 19.0 25.5 Associates degree/technical training 10.7 8.1 12.1 21.6 4-Year college degree or more 14.6 8.8 24.1 23.5 Race/ethnicity < .001 Non-Hispanic white 29.0 6.7 69.6 82.9 Black/African American 7.8 1.9 23.9 9.8 Mexican-American 24.8 36.3 2.2 0.0 Other Hispanic 13.8 19.5 2.2 2.4 Chinese 14.3 21.4 0.0 0.0 Filipino 6.8 10.1 0.0 0.0 Other 3.8 4.1 2.2 4.9 Born in the United States 45.3 14.2 94.6 95.7 < .001 Survey language < .001 English 56.4 28.9 100.0 100.0 Spanish 31.1 50.7 0.0 0.0 Chinese 12.5 20.4 0.0 0.0 English literacy < .001 Very good/good 56.8 31.8 99.1 100.0 Not good 20.9 33.2 0.0 0.0 Not at all 22.3 35.0 0.9 0.0 Needs interpreter < .001 No 64.7 44.8 97.4 100.0 Yes 22.0 34.3 1.8 0.0 Sometimes 13.4 20.9 0.9 0.0 Employment < .01 Full time 21.1 14.4 37.7 19.2 Part time 12.8 18.1 3.5 5.8 Unemployed 16.7 21.0 9.7 9.6 Homemaker 15.3 23.3 3.5 0.0 Disabled 10.1 5.5 18.4 15.4 Other 24.0 17.7 27.2 50.0 Marital status N/S Married 48.5 50.0 49.6 38.5 Single, never married 17.3 16.9 18.3 17.3 Divorced 12.4 10.4 10.4 26.9 Other 21.8 22.7 21.7 17.3 Data are percentages.
FQHC, federally qualified health center; N/S, no statistically significant differences between primary care practice type; PBRN, practice-based research network; VA, Veterans Health Administration.
- Table 3. The Relation of Primary Care Practice Type and Screening Positive, Unadjusted vs. Adjusted Analyses
Health Behavior Measure FQHC (vs PBRN) VA (vs PBRN) Unadjusted OR P Value Adjusted OR P Value Unadjusted OR P Value Adjusted OR P Value Fast food 0.22 < .001 0.16 < .05 0.44 1.06 Fruits/vegetables 0.77 8.8 < .05 0.93 1.26 Soda 0.74 0.76 0.8 1.87 Exercise 1.78 1.14 0.89 0.54 Stress 1.45 < .05 1.25 1.66 2.1 Anxiety/worry 0.86 0.65 1.04 1.46 Depression/interest 1.06 1.18 1.89 1.14 Sleep 0.64 0.82 1.01 1.19 Smoking 0.36 P < .01 0.52 1.7 0.87 Smokeless tobacco 0.31 < .05 47.8 1.64 1.75 Alcohol 1.1 5.01 < .05 1.81 < .05 2.47 Drug use 1.59 0.68 8.44 P < .01 7.34 < .05 Self-rated health 1.69 < .05 1.66 0.77 0.77 Total positive screens* −0.05 0.2 0.37 0.6 P values are compared to practice-based research network (PBRN) practices. The adjusted analyses control for patient sex, age, education, race/ethnicity, nativity, employment status, and marital status. Bold values indicate statistically significant results at P < .05.
↵* Coefficient is interpreted as the odds of primary care practice type [federally qualified health center (FQHC) or Veterans Affairs (VA)] patients screening positive for the measure compared to PBRN patients.
OR, odds ratio.
- Table 4. The Use of the Behavioral Health Assessment during the Clinical Encounter, by Primary Care Practice Type
Overall (n = 408) FQHC (n = 241) PBRN (n = 115) VA (n = 52) P Value* Patient felt comfortable answering the questions 85.6 91.7 76.3 77.5 < .001 Provider showed patients the results of the behavioral health assessment 58.5 53.7 67.7 — < .05 Patients received a copy of results to take home 36.0 28.4 50.0 41.0 < .01 Provider asked patient about their concerns about the results 54.1 46.7 67.0 64.3 < .01 Provider asked which health concerns patient would like to work on 60.2 48.7 81.3 71.4 < .001 Provider helped identify specific steps patient can take to address concerns 72.1 64.6 85.6 81.5 < .01 Patient plans to follow up with provider about health concerns from the behavioral health assessment 83.2 77.5 91.1 93.2 < .01 Data are percentages.
↵* P values indicate the overall differences across primary care practice types.
FQHC, federally qualified health center; PBRN, practice-based research network; VA, Veterans Health Administration.




{kind=link}