
Abstract
Background: Shared decision making (SDM) is an interactive process between clinicians and patients in which both share information, deliberate together, and make clinical decisions. Clinics serving safety net patients face special challenges, including fewer resources and more challenging work environments. The use of SDM within safety net institutions has not been well studied.
Methods: We recruited a convenience sample of 15 safety net primary care clinicians (13 physicians, 2 nurse practitioners). Each answered a 9-item SDM questionnaire and participated in a semistructured interview. From the transcribed interviews and questionnaire data, we identified themes and suggestions for introducing SDM into a safety net environment.
Results: Clinicians reported only partially fulfilling the central components of SDM (sharing information, deliberating, and decision making). Most clinicians expressed interest in SDM by stating that they “selected a treatment option together” with patients (8 of 15 in strong or complete agreement), but only a minority (3 of 15) “thoroughly weighed the different treatment options” together with patients. Clinicians attributed this gap to many barriers, including time pressure, overwhelming visit content, patient preferences, and lack of available resources. All clinicians believed that lack of time made it difficult to practice SDM.
Conclusions: To increase use of SDM in the safety net, efficient SDM interventions designed for this environment, team care, and patient engagement in SDM will need further development. Future studies should focus on adapting SDM to safety net settings and determine whether SDM can reduce health care disparities.
Shared decision making (SDM) occurs when clinicians and patients share information, deliberate jointly, and arrive at decisions that reflect patients' preferences. Clinician barriers to SDM1 may contribute to health disparities. Recent studies of African American patients demonstrate barriers even when patients seek to engage in information sharing.2 Clinics serving minority patients have more hectic workplaces and fewer resources, thus providing challenging settings for SDM.3 We studied perceptions of SDM among clinicians serving the urban poor. We sought to identify perceptions, barriers, and corrective steps to implement SDM in resource-constrained environments.
Methods
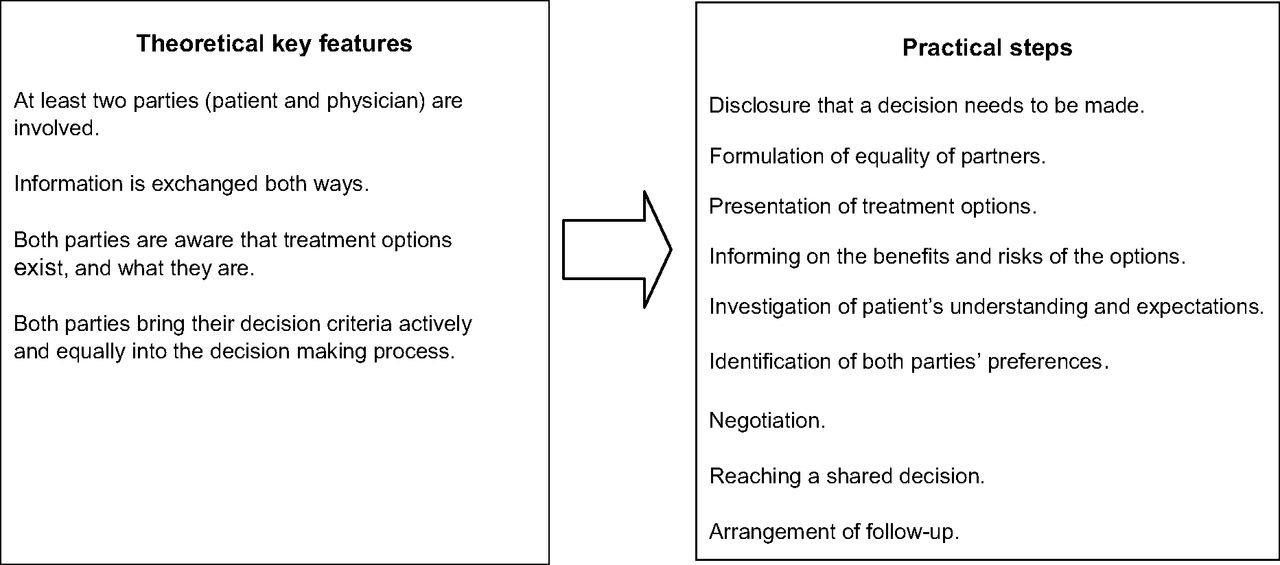
This study was conducted with clinicians enrolled in a randomized trial testing SDM diabetes decision aids. Of 23 eligible clinicians (18 physicians and 5 nurse practitioners and physician assistants), we interviewed a convenience sample of 13 physicians and 2 nurse practitioners at Hennepin County Medical Center (HCMC). One clinician declined to participate. HCMC's patient population is primarily low income, with 65% of patients from communities of color and 25% from immigrant communities. The study took place from March to May 2011 and received local institutional review board approval. A conceptual framework of SDM (Figure 1) from Kriston et al4 structured our approach.

Conceptual model for the shared decision-making process. (From Kriston et al,4 reprinted with permission of the publisher).
The SDM-Q-9 asks about SDM from the patient's perspective.4 We reframed the questions to be from the clinician's perspective. Response options included completely agree, strongly agree, somewhat agree, somewhat disagree, strongly disagree, and completely disagree. We also conducted interviews to explore the feasibility of SDM.
Audiotaped and transcribed interviews were reviewed by the lead author (ABB); a second reviewer assessed approximately 50% of the transcripts. A third reviewer (KT) assessed transcripts after coding was completed and agreed on the coding scheme. Themes were categorized into 3 domains: clinician barriers, patient barriers, and system barriers.
Results
Clinicians often made it clear to patients that a decision needed to be made (67% strong or complete agreement) but less often (33%) helped patients understand information, precisely explained treatment options (33%), or thoroughly weighed treatment options with patients (20%) (Table 1).
Time pressure was noted by all clinicians: “If I did all these steps, I would never get through the day.” Other clinician issues included practice preferences (“I have a clear bias I'm sure comes across [in] the way I present the data”), and visit content (“It's a lot to try to get the patient to absorb in a 15-minute visit…”).
Clinicians also identified patient-related barriers, such as willingness to participate and cultural differences. System barriers included resources and organizational culture (“A place where every point of care is aimed around SDM lets everybody do their job …, but if it feels counter-cultural …, then it's much harder …”).
Discussion
Our safety net primary care clinicians express interest in SDM but do not often practice it. Barriers include time available, personal preferences, knowledge, and training. There are also concerns about patients' willingness to share decisions and system factors, including lack of resources and organizational culture.
Our work adds to that of the systematic review by Légaré et al1 and may be the first to focus on SDM adoption in safety net care. Our results show that physician-identified barriers to SDM may be of similar nature throughout the health care system. What may distinguish barriers in safety net facilities is their magnitude, the importance of the context of the facility and patients, and the efforts needed to overcome them. Results from ongoing trials of SDM implementation at HCMC may offer more insights into the effect these barriers may have on the efficacy of such interventions.
Limitations of our study include the single study site and the limited analysis of qualitative data. Action steps to increase the use of SDM in safety net settings include (1) developing efficient SDM protocols using decision aids; (2) training clinicians in issues related to cultural and context awareness, health literacy, and SDM; (3) promoting patient interest in SDM with health coaches; and (4) developing team cohesion and a culture that supports SDM. As Nowakowski et al5 suggest, we can learn from “exemplary providers who overcome contextual barriers” and actively participate in SDM with their patients.
Notes
This article was externally peer reviewed.
Funding: Support was provided, in part, by a Translating Information on Comparitive Effectiveness into Practice (TRICEP) grant, funded by Agency for Healthcare Research and Quality (AHRQ) grant 5R18HS018339-02 (ML, DHB, SP, NDS, VMM, KT).
Conflict of interest: none declared.
- Received for publication September 3, 2013.
- Revision received December 4, 2013.
- Accepted for publication December 9, 2013.




{kind=link}