
Article Figures & Data
Figures
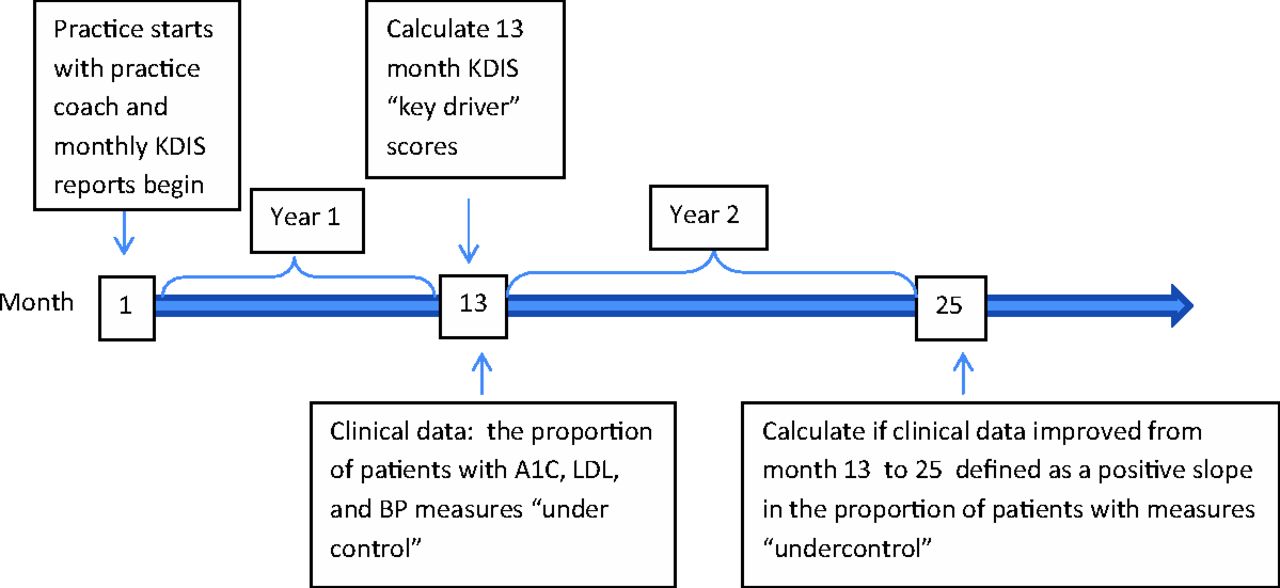
- Figure 1.
Data collection timeline. BP, blood pressure; KDIS, Key Drivers Implementation Scale; LDL, low-density lipoprotein.
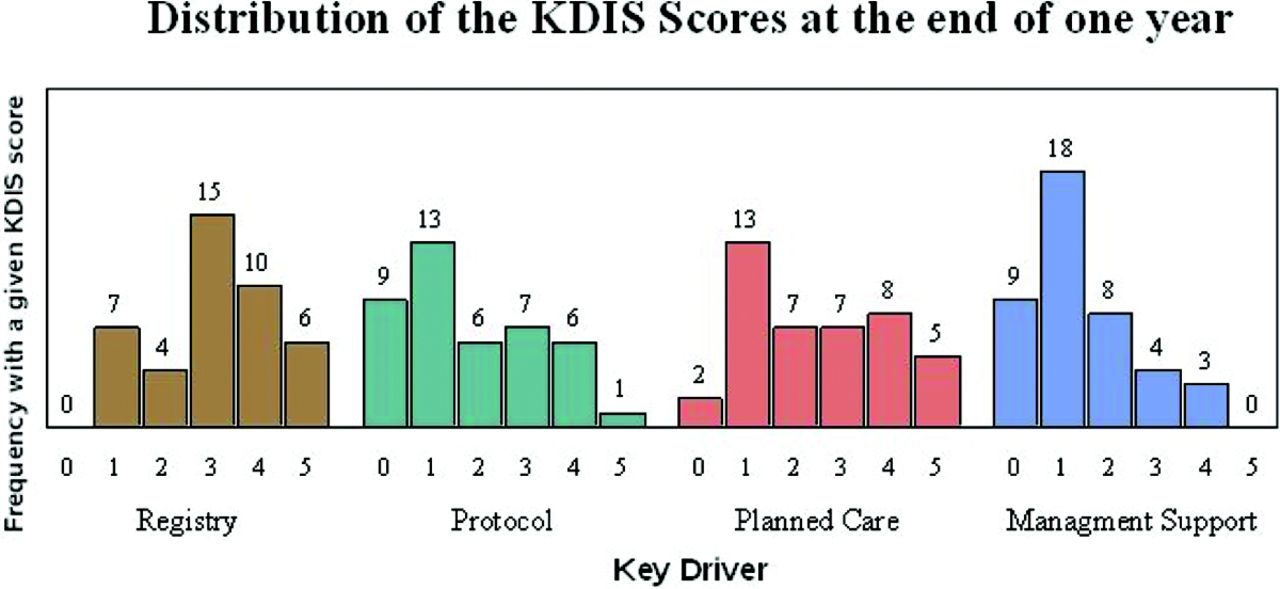
- Figure 2.
Frequency distribution of Key Drivers Implementation Scale (KIDS) scores attained at 1 year (with averages across months 10, 11, and 12) after coaching commenced by key driver.


Tables
- Table 1. Sample of Registry Item of the Practice Assessment Scales/Key Driver Implementation Scale* in Improving Performance in Practice
Item No. Item Title Description 0 No activity There has been no activity on registry adoption or use. 1 Selected The practice has chosen a registry but has not yet begun using it. 2 Installed The practice has a registry installed on a computer and has set up a template, and entered demographic data on patients of interest (e.g., diabetes) or has outlined a process to systematically enter the data. 3 Testing workflow The practice is testing the process for entering clinical data into the registry but is not yet using the registry to help with the daily care of patients. 4 Patient management All clinical data is entered into the registry and the practice is using the registry daily to plan patient care and is able to produce consistent reports on population performance. 5 Full integration Registry is kept up to date with a consistent and reliable process. The practice checks on and monitors the registry processes and uses the registry to manage the entire patient population. For the full scale see http://forces4quality.org/sites/default/files/tool6.1ipippractice%20assessment%20template.pdf.
↵* The Key Driver Implementation Scale term is that used by the investigators of the Transforming Primary Care Practice in North Carolina (AHRQ R18 HS019131).
Characteristic Practices* Service area Rural 26 (62) Urban 16 (38) Mean provider count (n) 8.4 Providers (n) ≤3 18 (43) 4–6 13 (31) ≥7 11 (26) Practice specialty Family medicine 31 (73) Internal medicine 9 (21) Mixed (internal/family medicine) 2 (5) Practice type Nonacademic 37 (74) Academic 5 (12) Insurance† (mean %) Medicaid (n = 35) (23) Uninsured (n = 33) (18) Practice visits per day (n = 37), n (range) 73.6 (10–345) Uses electronic health record system 22 (52) Study practices with baseline clinical data that reached NCQA Diabetes Recognition Program performance thresholds LDL levels‡ <100 mg/dL 23 (37) Systolic blood pressure 31 (36) Hemoglobin A1C 17 (27) Study practices that reached IPIP goals (n) LDL levels‡ <100 mg/dL 1 Systolic blood pressure 1 Hemoglobin A1C 4 Data are n (%) unless otherwise indicated.
↵* Percentages listed may reflect rounding.
↵† Insurance and practice visit data for several practices are missing.
↵‡ One practice did not have data for low-density lipoprotein (LDL) levels.
NCQA, National Committee for Quality Assurance; IPIP, Improving Performance in Practice.
- Table 3. Change in the Proportion of Patients* Meeting the Low-Density Lipoprotein Goal as a Function of Key Drivers Implementation Scale (KDIS) Score at Year 1†
KDIS Score Key Drivers‡ Registry Protocol Planned Care Template Self-Management Support All 4 Drivers§ 0 0.89 (0.68–1.16) 0.74 (0.60–0.91) 1.20 (0.91–1.59) 1.15 (0.94–1.40) 0.78 (0.59–1.03) 1 0.97 (0.78–1.20) 0.88 (0.75–1.03) 1.13 (0.91–1.40) 1.10 (0.93–1.30) 0.91 (0.74–1.11) 2 1.05 (0.89–1.25) 1.05 (0.89–1.25) 1.05 (0.89–1.25) 1.05 (0.89–1.25) 1.05 (0.89–1.25) 3 1.14 (0.99–1.33) 1.26 (0.98–1.61) 0.98 (0.84–1.15) 1.01 (0.82–1.23) 1.22 (0.99–1.50) 4 1.24 (1.07–1.44) 1.50 (1.07–2.11) 0.92 (0.77–1.10) 0.96 (0.75–1.24) 1.42 (1.07–1.89) 5 1.35 (1.13–1.61) 1.80 (1.16–2.80) 0.86 (0.68–1.08) 0.92 (0.67–1.26) 1.65 (1.13–2.41) Values are presented as odds ratio (95% confidence intervals). An odds ratio greater than 1 indicates improvement between years 1 and 2. Bold values indicate statistically significant results at P < .05.
↵* Proportion at the end of 2 years participation compared to 1 year.
↵† Only 41 practices are included in this analysis because 1 practice did not have low-density lipoprotein data for months 10, 11, or 12; the 1-year time interval actually comprises 13 months of data reporting.
↵‡ Estimates for individual key drivers are calculated holding the other 3 key driver scores at a value of 2.
↵§ Indicates model estimates when all key drivers receive the same score (ie, all 3s, all 4s, etc.).
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Successful Trial of Practice Facilitation for Plan, Do, Study, Act Quality Improvement
- Strategies and Factors Associated With Top Performance in Primary Care for Diabetes: Insights From a Mixed Methods Study
- Quality Improvement Teams: Moving from the Passionate Few to the Mandated Many
- Organizational Leadership and Adaptive Reserve in Blood Pressure Control: The Heart Health NOW Study
- The Cost to Successfully Apply for Level 3 Medical Home Recognition
- Patient Care Outcomes of a Tobacco Use Registry in an Academic Family Practice
- Family Physicians are Complex Care Physicians and Quality of Care Advancement Experts